Back to Journals » Drug Design, Development and Therapy » Volume 19
Application of Loading Dose Warfarin in Postpartum Women with Pulmonary Embolism – a Prospective, Randomized, Double-Blind Trial
Authors Huang W, Sun H ![]() , Zhou L, Chen Y, Huo Y
, Zhou L, Chen Y, Huo Y
Received 9 June 2025
Accepted for publication 30 October 2025
Published 24 November 2025 Volume 2025:19 Pages 10437—10448
DOI https://doi.org/10.2147/DDDT.S537351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Weifeng Huang,1,* Huiqin Sun,2,* Lu Zhou,3 Yan Chen,4 Yan Huo5
1Department of Critical Care Medicine, Shanghai Xuhui Central Hospital, Zhongshan-Xuhui Hospital, Fudan University, Shanghai, People’s Republic of China; 2Department of Anesthesiology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 3Department of Epidemiology, Ministry of Education Key Laboratory of Public Health Safety, School of Public Health, Fudan University, Shanghai, People’s Republic of China; 4Department of Pharmacy, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 5Department of Pharmacy, Yangpu Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Chen, Department of Pharmacy, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China, Email [email protected] Yan Huo, Department of Pharmacy, Yangpu Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China, Email [email protected]
Purpose: Warfarin is usually used in a fixed loading dose regimen, which may increase the risk of bleeding or prolong the time to reach standard dose. The aim of the study is to compare the efficacy and safety of loading dose versus maintenance dose of warfarin therapy in postpartum women with pulmonary embolism (PE) under the guidance of clinical pharmacogenetic information.
Patients and Methods: A total of 64 postpartum women with PE were recruited from September 2022 to August 2023. Participants were randomly divided 1:1 into two groups using a random-number table patients in the experimental group received a regimen combining the initial 1 to 3 days loading dose with the International Warfarin Pharmacogenetics Consortium (IWPC) model. Patients in the control group only received a regimen guided by the IWPC model for the initial 1 to 3 days. Starting from day 4, the warfarin dose was adjusted according to the international normalized ratio (INR). The primary outcome was first time to therapeutic INR (2.0– 3.0).
Results: The study found that the median time to first reach the therapeutic INR was 5.5 days in the experimental group compared to 7 days in the control group (p=0.002). The median time within therapeutic range (TTR) was 97.24% in the experimental group compared to 95.50% in the control group (p=0.001). The difference in adverse events showed no statistical significance between the two groups (P > 0.05).
Conclusion: The study could provide ideas for the precise treatment of warfarin in postpartum women with PE. The integration of warfarin loading doses guided by pharmacogenetics into clinical practice can enhance decision-making, optimize patient outcomes, and reduce adverse events.
Keywords: warfarin, loading dose, maintenance dose, IWPC, postpartum women
Introduction
Postpartum women face a significantly increased risk of pulmonary embolism (PE) during pregnancy and the puerperium compared to non-pregnancy, and it is a direct cause of in-hospital mortality in postpartum women.1,2 Warfarin is the only oral anticoagulant recommended by the American College of Obstetricians and Gynecologists in women who are breastfeeding weeks postpartum.3,4 Warfarin is recommended because it has not been detected in breastmilk and is unlikely to be excreted into breastmilk due to being nonlipophilic, polar, and highly protein bound.5 A number of factors could influence the therapeutic dose of warfarin, and there is individual variability, making it challenging to determine the appropriate initial and maintenance dose.6 In 2007, the Food and Drug Administration added pharmacogenetic information to the warfarin product label.7 In 2010, they recommend using genotype stratification tables for estimating the precise dose of warfarin, including two genes—cytochrome P450, family 2, subfamily C, polypeptide 9 (CYP2C9), and vitamin K epoxide reductase complex, subunit 1 (VKORC1).7 CYP2C9 and VKORC1 gene polymorphisms explained approximately 40% of the individual variation in warfarin dose in terms of pharmacokinetics and pharmacodynamics, respectively.8 Furthermore, it has been suggested that interactions between warfarin and breastfeeding may also lead to an increased need for warfarin.9
A large number of randomized controlled trials have demonstrated that the stable dose of warfarin predicted by gene-directed prediction models is more closely related to the actual stable dose, but the selection of the initial dose remains controversial.10,11 The American College of Chest Physicians recommends that starting warfarin therapy at a fixed loading dose of 10 mg per day for the first 2 days rather than starting at a dose predicted by pharmacogenetic information.12 The American Heart Association/American Stroke Association recommends that the initial dose of warfarin should be guided by pharmacogenetic information (CYP2C9 and VKORC1 genotypes).13 In contrast, the European Pharmacogenetics in Anticoagulation Therapy consortium study showed that the modified IWPC dosing algorithm tended to underestimate the actual dose.14 Warfarin dosing has remained largely empirical in China, whereby patients are initiated on fixed doses and titrated based on INR measurements during the first few weeks of therapy.15 A meta-analysis has revealed that VKORC1-1639 GG, GA, and G carriers required a 101% (53.0–149.0%), 40% (36.0–45.0%) and 38% (35.0–42.0%) higher mean daily warfarin dosage, respectively, than VKORC1-1639 AA carriers. Approximately 90% of the Chinese population carries VKORC1 variant alleles.16 There are few prospective studies on the pharmacogenetic information about warfarin in postpartum women, and even fewer clinical studies on the development of loading doses. Therefore, how to quickly and accurately determine the starting dose of warfarin, shorten the dosage adjustment cycle, and make the patient’s international normalized ratio (INR) quickly reach the standard level with security is the primary problem for clinicians. The aim of this study is to evaluate the safety and efficacy of initiating warfarin therapy in postpartum women with PE by pharmacogenetic-guided loading dose compared to pharmacogenetic-guided maintenance dose. This will provide reference for the precise dosage of warfarin.
Materials and Methods
Study Design
Ethical approval for this prospective, randomized, double-blind study was obtained from the Ethics Committee of Shanghai Sixth People’s Hospital (approval number: 2021–220-(1)) and registered in the Chinese Clinical Trial Registry (ChiCTR2200063325). This trial was performed in accordance with the Declaration of Helsinki, and written informed consent was obtained from all subjects before they participated in the study. The flowchart of the study design is shown in Figure 1. The study included 64 postpartum women with PE from the Critical Care Maternity Center. All participants were ≥18 years old and had confirmed PE by computed tomography pulmonary angiography. Patients meeting the criteria were randomly divided 1:1 into experimental (pharmacogenetic-guided loading dose group) and control (pharmacogenetic-guided maintenance dose group) groups to receive physician-guided warfarin dosing to obtain a target INR window between 2.0 and 3.0. The trial protocol was blinded to patients, investigators who assessed treatment endpoints and analyzed data, and was unblinded to the primary care physician.
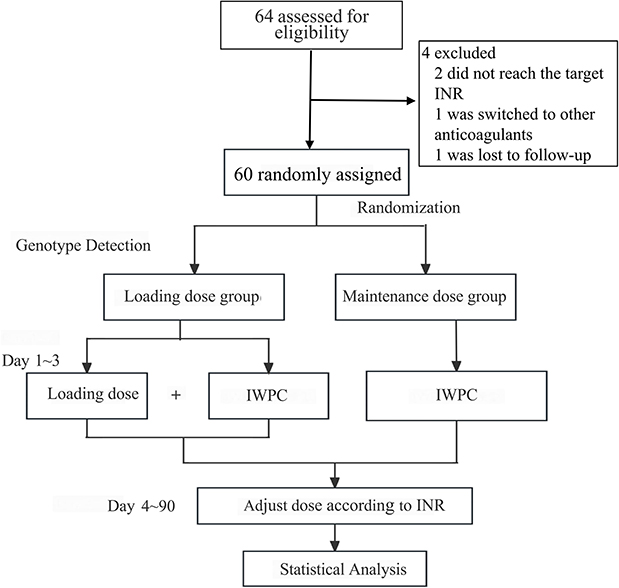 |
Figure 1 Flow chart of study design. Abbreviation: IWPC, International Warfarin Pharmacogenetics Consortium. |
Study Participants
Sample size: The participants of the study were post-partum patients with PE who were treated at the Shanghai Sixth People’s Hospital from September 2022 to August 2023, which is a critical care center for postpartum women and affiliated with six different hospitals. PE happened within 3 days after the delivery and the patient was admitted to the hospital within 24 hours. Patients’ demographics, laboratory data, clinical characteristics etc. were collected right away. All participants breastfed normally after giving birth. Referring to previous literature and combining the results of the pre-trial with small samples, the time to reach therapeutic INR in the experimental group was at least 5 days lower than that in the control group. In accordance with the principles of superiority trial design, a superiority cut-off value of 3 days was set based on the results of previous studies.11 Using the Superiority by a Margin Tests for the Difference Between Two Means process through PASS 15.0 software, the time to reach the therapeutic INR for the two groups was set at 2.5, α= 0.05, and the degree of certainty = 0.9, and 28 cases were calculated for each group. Considering a 10% lost to follow-up, a total sample size of 62 cases was required finally.
Inclusion criteria: 1) age ≥18 years, no history of smoking or drinking; 2) puerperium; 3) diagnosis of PE confirmed by computed tomography pulmonary angiography within 1–3 days after delivery, and all postpartum women with PE were admitted to the hospital within 24h from onset of the disease, and clinical data were complete; 4) oral warfarin anticoagulation was initiated during the hospitalization period, and the anticoagulant therapy of warfarin exceeded 3 months, and maintained a stable dose (Consistent with the same oral dose for at least 2 outpatient follow-up visits and with an interval of ≥ 7 days); 5) written informed consent signed by both patients and their family members.
Exclusion criteria: 1) past history of warfarin application; 2) with active bleeding; 3) with comorbid hematologic or coagulation abnormalities; 4) with severe infections, malignant tumors, severe hepatic or renal insufficiency, and chronic cardiorespiratory diseases; 5) taking medications such as aspirin, amiodarone, or rifampicin, which can affect warfarin’s pharmacodynamics or pharmacokinetics, as well as other anticoagulant medications; 6) with a baseline INR ≥ 1.5; 7) INR consistently not reached target value during hospitalization and follow-up, with target INR value defined as 2.0–3.0; 8) poor adherence, and for various reasons patient is unable to continue the clinical trial.
Genotype Detection
Sample preparation: A disposable vacuum blood collection tube was used to collect 2–3 mL of peripheral venous blood upon admission from both groups of subjects, and the samples were anticoagulated with EDTA. Genotype testing for CYP2C9 and VKORC1 was performed within 24h.
Testing procedure: The sample (200 µL) was transferred to a 1.5-mL centrifuge tube, and 1.2 mL of the 1X NH4Cl pre-treatment solution was subsequently added. The tube was then gently inverted 10 times and incubated at room temperature for 5 minutes until the liquid turned into a clear red color. The tube was subsequently centrifuged at 3000 rpm (approximately 500–700 × g) for 5 minutes. The supernatant, consisting of a clear red liquid, was carefully removed, and 1 mL of 1 × NH4Cl solution was added to fully resuspend the leukocytes that had settled at the bottom of the tube. After centrifugation at 3000 rpm (or 500–700 xg) for 5 minutes, the supernatant was carefully removed, and 30–50 µL of nucleic acid purification reagent (Yaojinbao, Beijing Huaxia Times Gene Technology Co., Ltd., China) was added to the tube. The contents were then mixed thoroughly by repeated pipetting. The tube was maintained at room temperature for a duration of 30 minutes, during which it was shaken and mixed twice. Then, 4 µL of the prepared sample was added to the Sequencing Reaction Universal Kit for gene testing (Beijing Huaxia Times Gene Technology Co., Ltd). The mixture was thoroughly combined and subsequently analyzed using a micro-fluorescence detector (Fluotec 48E, Tianlong Technology).
Procedures
The warfarin dose was calculated in reference to the International Warfarin Pharmacogenetics Consortium (IWPC) warfarin prediction model formula (http://www.warfarindosing.org).17 This formula involved CYP2C9*3 (1075A>C) and VKORC1 (1639G>A) genotypes, as well as clinical factors such as age, height, and weight. Patients in the experimental group received a regimen combining the initial 1 to 3 day loading dose with IWPC dose prediction model. Based on pre-experiments and previous literature, the loading dose was defined as 1.5 times the predicted dose of IWPC.18 Patients in the control group only received a regimen guided by the IWPC dose prediction model for the initial 1 to 3 days. Starting on day 4, INR value was monitored at 8 a.m. daily, and the dose of warfarin was adjusted according to INR values at 1 p.m. daily. INR values were rechecked every 1 to 3 days in postpartum women with PE during hospitalization. After a therapeutic INR has been achieved on 2 consecutive occasions, the measurement interval was extended; if there was a significant abnormality of INR, additional measurements should be taken promptly. Patients in both groups were enrolled and injected with LMWH (Sanofi Aventis Pharmaceuticals Ltd., Beijing, China) subcutaneously twice a day (6000 IU) at the same time. Patients could discontinue low molecular weight heparin after they reached therapeutic INR for the first time. Patients were counseled on warfarin medication at discharge. Instruct the patient to try to avoid foods rich in vitamin K such as spinach, egg yolks, tomatoes and mangoes. Patients were followed up for 3 months and INR values, daily dose of warfarin, and adverse events (INR>4 and bleeding events) were recorded.
Outcome Measures
Primary outcome: 1) Time to reach therapeutic INR for the first time.
Secondary outcomes: 1) Stable dose of warfarin and time to reach stable dose; 2) INR percentage of time within therapeutic range (TTR); and 3) INR >4 or adverse events such as bleeding. Severe bleeding was defined as that which resulted in a decreased hemoglobin of 2 g/d L, the need for a 2U red blood cell transfusion, or bleeding from vital organs or fatal bleeding (eg, intracranial hemorrhage, subdural hemorrhage, retro-peritoneal hemorrhage, joint hemorrhage, and intrapericardial hemorrhage). Minor bleeding was defined as bleeding from other sites such as nosebleeds, gum bleeding, skin bleeding, hematuria, etc. (Once bleeding occurs, immediately discontinue warfarin, vitamin K1, and coagulation factor replacement therapy, and provide blood transfusion support. Monitor INR every 4 to 6 hours until stable. If the bleeding is non-life-threatening and anticoagulation is necessary, therapy may be cautiously restarted several days to weeks after bleeding has stopped, initially using low molecular weight heparin as a bridge).19
Statistical Analysis
Data were analyzed by SPSS v26.0 (IBM, Armonk, NY, USA), Prism v8.0 (GraphPad, San Diego, CA, USA) and HKU AF CAL software. Continuous variables are summarised as mean±SD or median (IQR) according to distribution. Comparisons of descriptive statistics between groups for continuous variables were analyzed using the independent samples t-test and the Mann–Whitney U-test (when data were not normally distributed). We performed Shapiro–Wilk normality tests on data and visualized the results using Q-Q plots and histograms. Based on the test results and visual inspection, we selected either parametric test method or nonparametric test method for analysis. The Levene test yielded non-significant results (p > 0.05), and the residual plot showed no evident pattern of heteroscedasticity, indicating that the assumption of homogeneity of variances was satisfied. A χ2 test or Fisher’s exact test was used to analyze categorical data, described as frequencies (percentages). Results of event occurrence over time were shown by Kaplan–Meier curves, and a Log rank test was performed to compare survival curves. The degree of association is expressed as odds ratio (OR) and its 95% confidence interval (95% CI), with a test level typically considered to be 0.05. P < 0.05 (two-sided) indicates statistically significant differences.
Results
Study Subjects
There were 4 cases excluded from the analysis among the 64 patients who met the inclusion criteria. There were 2 cases that consistently failed to achieve the target INR during hospitalization, 1 case that switched to another anticoagulant midway, and 1 case that was lost to follow-up. A total of 60 patients were included in the final analysis, 30 cases in the experimental group and 30 cases in the control group. A Hardy–Weinberg equilibrium test was performed for the genotype distribution of CYP2C9*3 (1075A>C) and VKORC1 (1639G>A). Both CYP2C9*3 (1075A>C) and VKORC1 (1639G>A) were tested for Hardy-Weinberg equilibrium (χ2 = 0, P = 1; χ2 = 0.12, P = 0.94), and the samples were representative. The genotype distributions of two groups in this study were similar to those described in the previous literature,20,21 as shown in Figure 2.
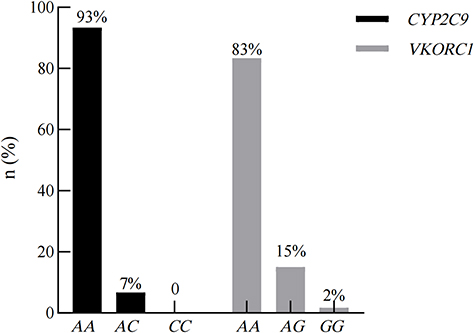 |
Figure 2 Frequency of CYP2C9*3 (1075A>C) and VKORC1 (1639G>A) genotype distribution. |
The demographic information, clinical baseline characteristics, and genotype distribution of the patients are shown in Table 1, and the baselines of postpartum women in both groups were essentially equal.
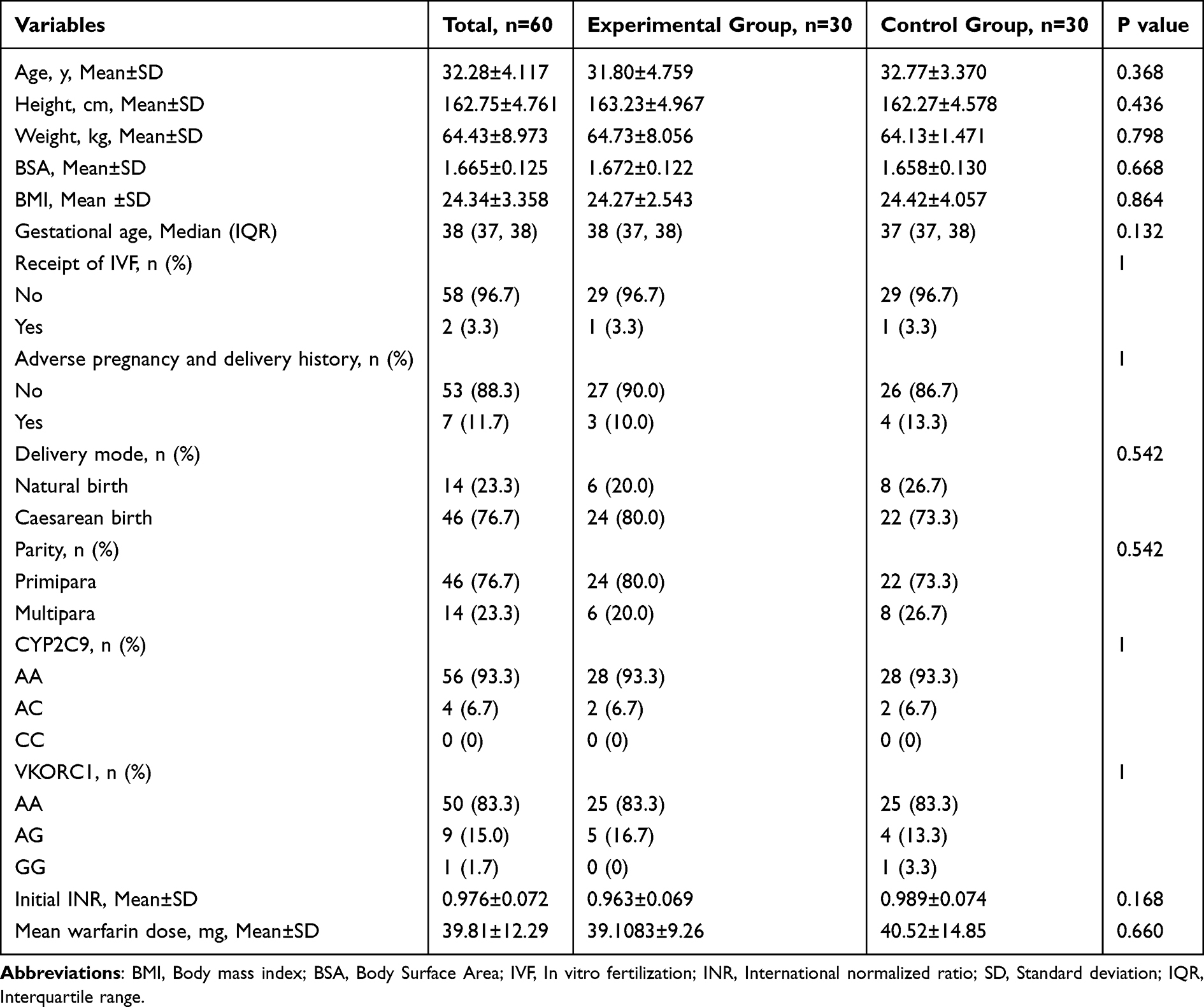 |
Table 1 Demographic and Baseline Clinical Characteristics of the Study Patients |
Primary Outcome
In the treatment analysis, the median time to first reach therapeutic INR was 5.5 days in the experimental group and 7 days in the control group, and the difference was statistically significant (P=0.002), as shown in Figure 3A. The postpartum women in the experimental group reached the stable dose faster than the control group (P=0.005), as shown in Figure 3B. The trend of mean INR was similar in both groups, which increased rapidly in the first 10 days and then declined slowly to remain within the target range, as in Figure 4A. For the two groups, the difference between the mean INR was greatest at D5-D10 after the initiation of anticoagulation therapy, and became gradually non-significant during the follow-up period, as shown in Figure 4A.
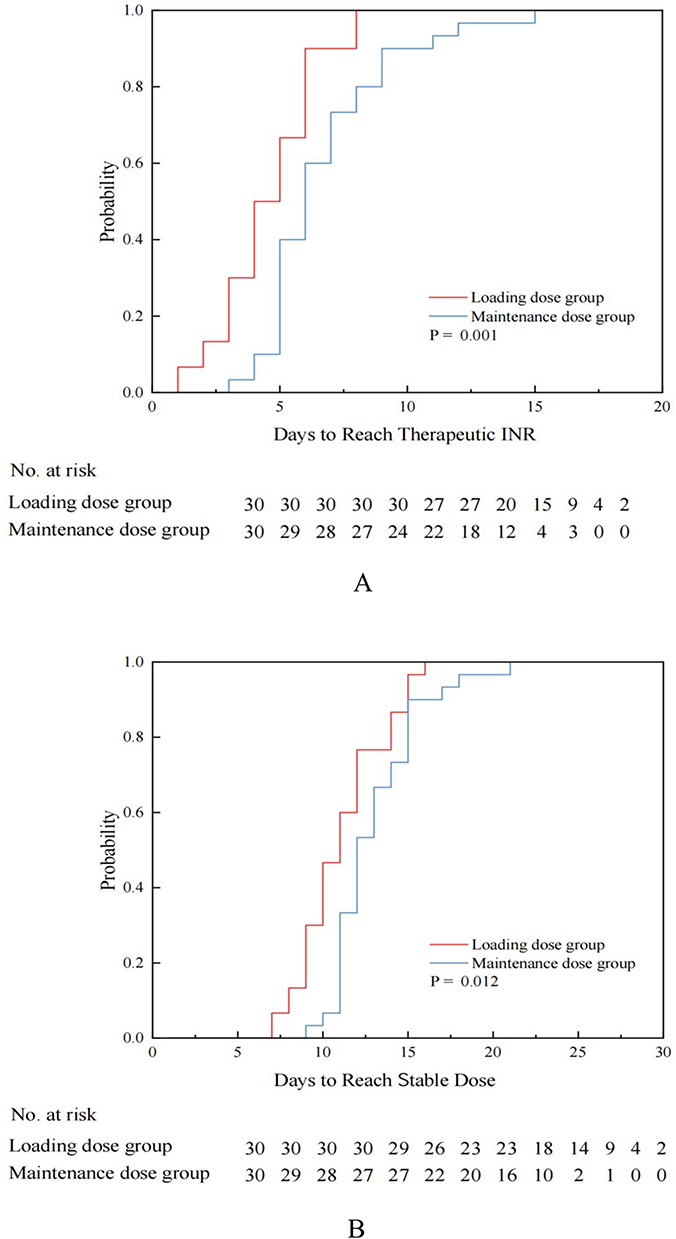 |
Figure 3 (A) Kaplan–Meier Plots of the Time to Reach a Therapeutic INR. (B) Kaplan–Meier Plots of the Time to Reach a Stable Warfarin Dose. |
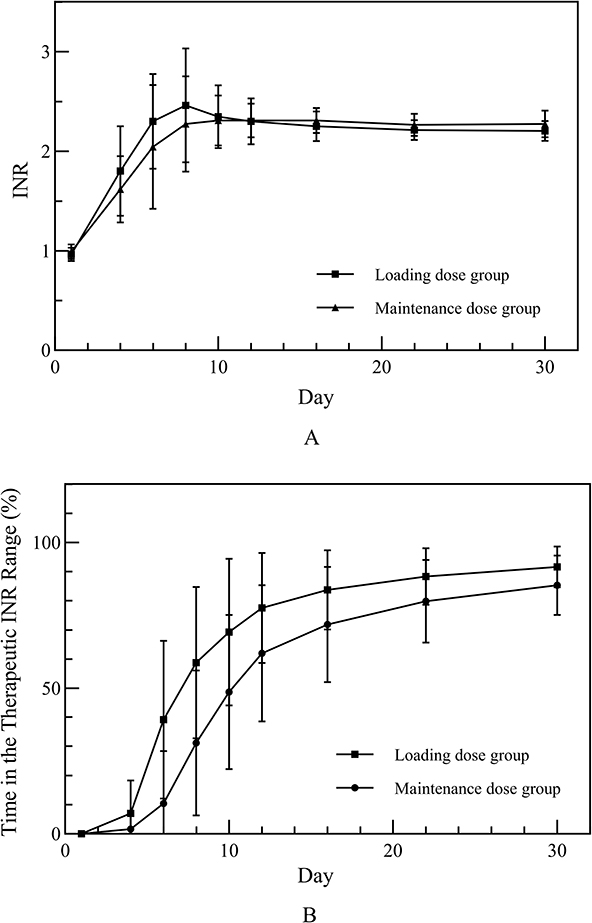 |
Figure 4 (A) Mean International Normalized Ratio (INR). (B) Percentage of Time in the Therapeutic INR Range. |
Secondary Outcome
It was shown that TTR increased as time passed in both experimental and control groups. Starting from D4, the difference in TTR of two groups began to become significant (P=0.028). During the 3-month follow-up period, the TTR of the experimental group was consistently higher than that of the control group, and the difference was statistically significant (P=0.001), as shown in Table 2, Figure 4B. In addition, the postpartum women in the experimental group reached the stable dose faster than the control group (P=0.005), and the median of daily stable dose in both groups was 4.375 mg, as shown in Table 3, Figure 3B. The hospitalization time and hospitalization cost of the two groups are shown in Table 3, and there is no statistically significant difference (P>0.05); however, compared with the control group, the experimental group can shorten the hospitalization time and hospitalization cost in some degree. A total of 3 bleeding events (2 cases in the experimental group and 1 case in the control group) were identified throughout the study. Among them, there were 2 cases of mild bleeding events (1 case in the experimental group and 1 case in the control group), and 1 case of severe bleeding events (1 case in the experimental group, with an unexplained decrease in hemoglobin of 2 g/d L). The differences in bleeding events and adverse events such as INR > 4 between the two groups were not statistically significant (P > 0.05).
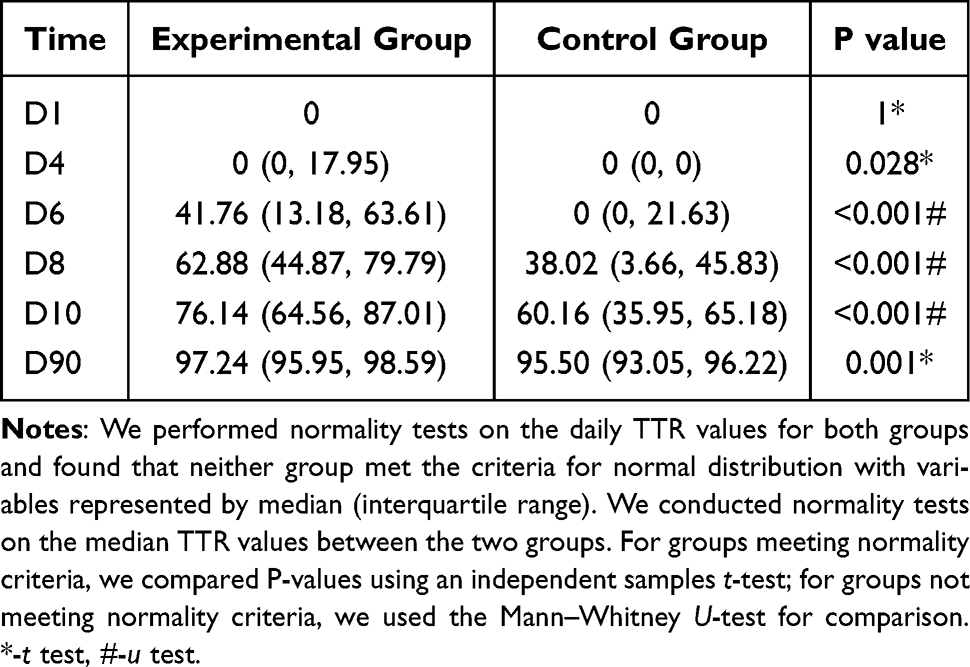 |
Table 2 Changes of TTR in Experimental and Control Groups |
 |
Table 3 Primary and Secondary Outcomes |
Discussion
Different from previous studies, the present study compared a pharmacogenetic-guided loading dose (1.5 times of the maintenance dose) combined with maintenance dose regimen versus a pharmacogenetic-guided maintenance dose regimen for the first time in postpartum women. The study found that gene-guided loading doses when starting warfarin therapy significantly shortened the time to first reach therapeutic INR and the time to reach stable dose and did not increase the risk of over-anticoagulation (INR≥4.0) and clinically relevant bleeding at an early stage. This suggests that using loading dose combined with maintenance dose regimen based on pharmacogenetic guidance is not only safe but also leads to achieve anticoagulant stability more quickly.
Previous studies have shown that the mutant type of CYP2C9*3 accounts for 1% to 4% and the wild type of VKORC1 accounts for about 82% of the Asian population, and the genotype distributions of two groups in this study were similar to those described in the previous literature.20,21
The study showed that the median time to reach the therapeutic INR for the first time was 5.5 and 7 days in the experimental and control groups, respectively. It is similar to the results of Ruzickova’s study (5.24 days versus 7.3 days), which suggests that pharmacogenetic-guided loading dose at the initiation of warfarin therapy significantly shortens the time to reach therapeutic INR for the first time.22 The greatest difference in mean INR values between two groups was observed in the early trial period (Figure 4A). The result is consistent with previous studies showing that the effect of pharmacogenetic-guided dosing is greatest in the early stages of warfarin.23
The calculation of TTR based on the INR value and the time of measurement during anticoagulation therapy is the most common way to assess the efficacy of anticoagulation therapy. Our study showed that the mean TTR value was 96.47±0.54 in the experimental group compared to 93.88±0.78 in the control group at 90 days of follow-up using HKU AF CAL software, and the difference was statistically significant (P=0.001). The study of EU-PACT showed TTR of the modified IWPC algorithm was 67.4 at 90 days follow-up period, which was lower than that of 96.47 in the present study. This may be due to the fact that the loading dose in EU-PACT’s study was decreasing day by day, and the loading dose in the present study was 1.5 times the maintenance dose, which drove the patients to achieve target INR more quickly. On the other hand, the average age of subjects in our study was younger with higher adherence. In addition, confounding factors such as the number of dose adjustments and the frequency of INR monitoring may also affect the results.11 As shown in the literature, TTR% ≥65% is considered effective for anticoagulation therapy. About 73.33% patients in the experimental group were treated effectively at D10, when the mean TTR in the experimental group was 69.27 ± 4.60 and in the control group was 48.65 ± 4.83, which is a statistically significant difference (p < 0.001). It is consistent with Gong’s study (WRAPID algorithm).24
Previous studies have shown that the stable dose of warfarin in China ranges from 2.28 to 3.59 mg/d.16,25,26 However, the stable dose of warfarin in the present study was higher than this range, which may be due to the following reasons: The average age of patients was young, with a small proportion of elderly patients.27 Most domestic clinical studies on warfarin are cardiac disease (eg, atrial fibrillation, postoperative heart valves) which suggests an INR target of 1.5–2.5. It is lower than the target INR of 2.0–3.0 in this study. Some scholars have found that warfarin therapy guided by genetic testing can shorten the time required to achieve the target INR range and reach a stable dose more quickly, which is similar to the results of our study (13 days versus 14 days).28 An algorithm guided by pharmacogenetic and clinical factors improved the accuracy and efficiency of warfarin dose initiation.
This study compared the occurrence of anticoagulation complications during hospitalization and follow-up in two groups as indicators of the safety of warfarin clinical therapy. Previous studies have shown that initiation of warfarin therapy with a fixed 10 mg loading dose at 1 to 3 days lead to reach the therapeutic range more quickly. However, this may result in 30% of patients suffering from a higher INR of 3 in the early stages.29,30 In the study, the loading dose was given referring to the pharmacogenetic information, and only 10% of the patients showed higher INR than the therapeutic range in the early stages, suggesting that gene-guided loading dose is superior to fixed loading dose. In Huang’s study, the incidence of adverse reactions by pharmacogenetic-guided dose was 11.5%, which was higher than the 6.7% in the experimental group and 3.3% in the control group of this study.31 In addition, only 3 patients experienced bleeding complications during the follow-up period (2 cases in the experimental group and 1 case in the control group), and the difference was not statistically significant (p > 0.05). It suggests that pharmacogenetic-guided loading dose combined with maintenance dose is safe compared to direct maintenance dose regimen.
Limitations
Our study also has some limitations. First, the sample size was small. The low prevalence of PE in postpartum women requires consideration when expanding the sample size, which may extend the study duration. Second, considering that the pharmacogenetic-guided group has been proved to be superior to the clinical fixed-dose group, we did not set up a clinical fixed-dose control group.11,32 Finally, there is uncertainty in extrapolating to other races as the study was limited to Asian postpartum women.
Conclusion
Based on the above results, compared to pharmacogenetic-guided maintenance dose, pharmacogenetic-guided loading dose (1.5 times of estimated maintenance dose) combined with maintenance dose regimen shortens the time to first reach target INR of warfarin and improves the efficacy of warfarin without increasing the risk of adverse events among the postpartum women with PE. This could serve as a basis for developing evidence-based guidance for optimal warfarin dosing in China.
The Ethics Ratify
This study was approved by the Ethics Committee of Shanghai Sixth People’s Hospital, with ethical approval number: 2021-220-(1).
Data Sharing Statement
The data that support the findings of the study are available on request from the corresponding author. The date is not publicly available due to privacy or ethical restrictions.
Acknowledgments
The authors thank the study volunteers and the study staff for their participation. We also thank the assistance of Obstetrics and Gynaecology teams.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was funded by the Clinical Pharmacy Innovation Research Institute of Shanghai Jiao Tong University School of Medicine (2018–2020) (grant number CXYJY2019MS005) and Development Center for Medical Science&Technology, National Health Commission of the People’s Republic of China (grant number WKZX2024DN0131).
Disclosure
Weifeng Huang and Huiqin Sun are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Collier AY, Molina RL. Maternal mortality in the United States: updates on trends, causes, and solutions. Neoreviews. 2019;20:e561–e74.
2. Sun H, Zhou L, Lu Y, Li Y, Huo Y, Huang W. A nomogram model containing genetic polymorphisms to predict risk of pulmonary embolism in pregnant women. Int J Womens Health. 2024;16:1505–1516. doi:10.2147/IJWH.S470644
3. Bates SM, Rajasekhar A, Middeldorp S, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: venous thromboembolism in the context of pregnancy. Blood Adv. 2018;2:3317–3359. doi:10.1182/bloodadvances.2018024802
4. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 196: thromboembolism in pregnancy. Obstet Gynecol. 2018;132:e1–e17. doi:10.1097/AOG.0000000000002706
5. Clark SL, Porter TF, West FG. Coumarin derivatives and breast-feeding. Obstet Gynecol. 2000;95:938–940. doi:10.1016/s0029-7844(00)00809-7
6. Hirsh J, Fuster V, Ansell J, Halperin JL. American Heart Association/American College of Cardiology Foundation guide to warfarin therapy. J Am Coll Cardiol. 2003;41:1633–1652. doi:10.1016/S0735-1097(03)00416-9
7. Gage BF, Lesko LJ. Pharmacogenetics of warfarin: regulatory, scientific, and clinical issues. J Thrombosis Thrombolysis. 2008;25:45–51. doi:10.1007/s11239-007-0104-y
8. Wang L, McLeod HL, Weinshilboum RM. Genomics and drug response. N Engl J Med. 2011;364:1144–1153. doi:10.1056/NEJMra1010600
9. Uppuluri E, Idrees N, Shapiro N. Warfarin dosage in a postpartum woman while breastfeeding: a case report. Pharmacother J Human Pharmacol Drug Ther. 2024;44:343–347. doi:10.1002/phar.2917
10. Kimmel SE, French B, Kasner SE, et al. A pharmacogenetic versus a clinical algorithm for warfarin dosing. N Engl J Med. 2013;369:2283–2293.
11. Pirmohamed M, Burnside G, Eriksson N, et al. A randomized trial of genotype-guided dosing of warfarin. N Engl J Med. 2013;369:2294–2303. doi:10.1056/NEJMoa1311386
12. Holbrook A, Schulman S, Witt DM, et al. Evidence-based management of anticoagulant therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest physicians evidence-based clinical practice guidelines. Chest. 2012;141:e152S–e84S. doi:10.1378/chest.11-2295
13. Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:2160–2236. doi:10.1161/STR.0000000000000024
14. Avery PJ, Jorgensen A, Hamberg AK, et al. A proposal for an individualized pharmacogenetics-based Warfarin initiation dose regimen for patients commencing anticoagulation therapy. Clin Pharmacol Ther. 2011;90:701–706. doi:10.1038/clpt.2011.186
15. Jahmunah V, Chen S, Oh SL, Acharya UR, Chowbay B. Automated warfarin dose prediction for Asian, American, and Caucasian populations using a deep neural network. Comput Biol Med. 2023;153:106548. doi:10.1016/j.compbiomed.2023.106548
16. Ren Y, Yang C, Chen H, et al. Pharmacogenetic-guided algorithm to improve daily dose of Warfarin in Elder Han-Chinese population. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.01014
17. Finkelman BS, Gage BF, Johnson JA, Brensinger CM, Kimmel SE. Genetic Warfarin dosing: tables versus algorithms. J Am Coll Cardiol. 2011;57:612–618. doi:10.1016/j.jacc.2010.08.643
18. Bungard TJ, Mutch J, Ritchie B. A randomized trial of restarting warfarin at maintenance versus loading doses following an elective procedure. J Thromb Thrombolysis. 2017;44:507–515. doi:10.1007/s11239-017-1553-6
19. Witt DM, Nieuwlaat R, Clark NP, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: optimal management of anticoagulation therapy. Blood Adv. 2018;2:3257–3291. doi:10.1182/bloodadvances.2018024893
20. Jorgensen AL, FitzGerald RJ, Oyee J, Pirmohamed M, Williamson PR. Influence of CYP2C9 and VKORC1 on patient response to Warfarin: a systematic review and meta-analysis. PLoS One. 2012;7:e44064. doi:10.1371/journal.pone.0044064
21. Geisen C, Watzka M, Sittinger K, et al. VKORC1 haplotypes and their impact on the inter-individual and inter-ethnical variability of oral anticoagulation. Thromb Haemost. 2005;94(10):773–779. doi:10.1160/TH05-04-0290
22. Ruzickova T, Sramek M, Kaplan V, et al. Warfarin loading dose guided by pharmacogenetics is effective and safe in cardioembolic stroke patients - a randomized, prospective study. Pharmacogenomics J. 2019;19:446–454. doi:10.1038/s41397-019-0066-4
23. Horne BD, Lenzini PA, Wadelius M, et al. Pharmacogenetic warfarin dose refinements remain significantly influenced by genetic factors after one week of therapy. Thromb Haemost. 2012;107:232–240. doi:10.1160/TH11-06-0388
24. Gong IY, Tirona RG, Schwarz UI, et al. Prospective evaluation of a pharmacogenetics-guided warfarin loading and maintenance dose regimen for initiation of therapy. Blood. 2011;118:3163–3171. doi:10.1182/blood-2011-03-345173
25. Tao H, Li Q, Zhou Q, et al. A prediction study of warfarin individual stable dose after mechanical heart valve replacement: adaptive neural-fuzzy inference system prediction. BMC Surg. 2018;18:10. doi:10.1186/s12893-018-0343-1
26. Zhu Y, Xu C, Liu J. Randomized controlled trial of genotype-guided warfarin anticoagulation in Chinese elderly patients with nonvalvular atrial fibrillation. J Clin Pharm Therap. 2020;45:1466–1473. doi:10.1111/jcpt.13218
27. Klein TE, Altman RB, Eriksson N, et al. Estimation of the warfarin dose with clinical and pharmacogenetic data. N Engl J Med. 2009;360:753–764.
28. Anderson JL, Horne BD, Stevens SM, et al. Randomized trial of genotype-guided versus standard warfarin dosing in patients initiating oral anticoagulation. Circulation. 2007;116:2563–2570. doi:10.1161/CIRCULATIONAHA.107.737312
29. Harrison L, Johnston M, Massicotte MP, Crowther M, Moffat K, Hirsh J. Comparison of 5-mg and 10-mg loading doses in initiation of warfarin therapy. Ann Intern Med. 1997;126:133–136. doi:10.7326/0003-4819-126-2-199701150-00006
30. Crowther MA, Ginsberg JB, Kearon C, et al. A randomized trial comparing 5-mg and 10-mg warfarin loading doses. Arch Intern Med. 1999;159:46–48. doi:10.1001/archinte.159.1.46
31. Huang SW, Chen HS, Wang XQ, et al. Validation of VKORC1 and CYP2C9 genotypes on interindividual warfarin maintenance dose: a prospective study in Chinese patients. Pharmacogenet Genomics. 2009;19:226–234. doi:10.1097/FPC.0b013e328326e0c7
32. Wang X, Tang B, Zhou M, et al. Efficacy and safety of genotype-guided warfarin dosing versus non-genotype-guided warfarin dosing strategies: a systematic review and meta-analysis of 27 randomized controlled trials. Thrombosis Res. 2022;210:42–52. doi:10.1016/j.thromres.2021.12.023
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.