Back to Journals » International Journal of Women's Health » Volume 18
Application of High-Throughput Sequencing Technology in Fetal Growth Restriction and Analysis of Pregnancy Outcomes
Authors Qin Y ![]() , Mei Y, Liu B, Wang S
, Mei Y, Liu B, Wang S
Received 11 September 2025
Accepted for publication 16 December 2025
Published 10 January 2026 Volume 2026:18 566566
DOI https://doi.org/10.2147/IJWH.S566566
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Yanfeng Qin,1 Yan Mei,2 Bailing Liu,2 Sumei Wang1
1Department of Obstetrics, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China; 2Department of Obstetrics, Liuzhou Maternal and Child Health Hospital, Liuzhou, Guangxi Zhuang Autonomous Region, People’s Republic of China
Correspondence: Sumei Wang, Department of Obstetrics, The First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi Zhuang Autonomous Region, People’s Republic of China, Email [email protected]
Background: Fetal growth restriction (FGR) is a significant cause of perinatal morbidity and mortality. This study aimed to verify whether high-throughput sequencing technologies (Copy Number Variation Sequencing, CNV-seq; Trio Whole Exome Sequencing, Trio-WES) can overcome the limitations of traditional karyotype analysis and improve the detection rate of genetic etiologies in FGR fetuses, and to analyze associated pregnancy outcomes.
Methods: A retrospective analysis was conducted on 235 fetuses who underwent invasive prenatal diagnosis following ultrasound-diagnosed fetal growth restriction (FGR) at Liuzhou Maternal and Child Health Hospital between January 2019 and March 2025. All cases underwent concurrent chromosomal karyotyping and genome-wide copy number variation sequencing (CNV-seq). Among these, 19 cases with normal results from both karyotyping and CNV-seq were further analyzed using trio-whole exome sequencing (Trio-WES). For karyotyping and CNV-seq, genomic DNA was extracted from amniotic fluid or umbilical cord blood samples. For Trio-WES, genomic DNA was obtained from fetal amniotic fluid or umbilical cord blood, along with peripheral blood samples from both parents as controls.
Results: Among the 235 FGR specimens, chromosomal abnormalities were detected in 9 cases (3.8%, 9/235) by karyotype analysis of chromosomes, and 26 cases (11.1%,26/235) by CNV-seq technology.Among FGR cases with normal karyotypes, CNV-seq detected an additional 17 abnormalities (7.5%, 17/226). When comparing the two techniques, the abnormal detection rate of CNV-seq technology was higher than that of karyotype analysis, and the difference was statistically significant (P < 0.05). Among the 19 cases negative for both karyotype and CNV-seq, Trio-WES detected 6 abnormalities (31.6%, 6/19), including 3 pathogenic variants, 1 likely pathogenic variant, and 2 variants of uncertain significance (VOUS). A total of 32 cases (13.6%, 32/235) of abnormal variations were detected by the combination of karyotype analysis and high-throughput sequencing. Pregnancy outcomes included: all 9 karyotype-abnormal cases chose termination of pregnancy (TOP); of the 17 CNV-seq-abnormal cases (karyotype-normal), 10 underwent TOP (3 with combined organ malformations) and 7 had live births (6 with normal follow-up to 2 years, 1 with developmental delay and hypertonia at 2-year follow-up); of the 6 Trio-WES-abnormal cases, 5underwent TOP and1 had live births (1 with normal follow-up).
Conclusion: Compared with traditional karyotype analysis (3.8% detection rate), high-throughput sequencing technologies (CNV-seq and Trio-WES) significantly improve the detection rate of genetic abnormalities in FGR fetuses to 13.6%. The “karyotype analysis + CNV-seq + Trio-WES” stepwise detection protocol provides critical support for prenatal genetic counseling and clinical decision-making,and contributes to optimizing pregnancy management and outcomes.
Keywords: fetal growth restriction, high-throughput sequencing, karyotype analysis of chromosomes, prenatal diagnosis, pregnancy outcome
Introduction
Fetal growth restriction (FGR) refers to a condition where fetal growth fails to reach its inherent genetic potential, with an incidence rate of 5%–10%.1 It is a significant contributing factor to perinatal morbidity and mortality. According to global perinatal health reports, FGR accounts for 15%–20% of total perinatal deaths, and the missed diagnosis rate of FGR etiologies is higher in low-income regions due to limited diagnostic technologies.The pathophysiological process of FGR is multifactorial, involving genetic susceptibility, maternal underlying diseases, placental insufficiency, and other factors. Among these, fetal genetic etiology is one of the important causes of FGR, accounting for 5%–20% of all FGR cases.2 Over the past decade, the application of molecular genetic detection technologies, particularly chromosomal microarray analysis (CMA) and high-throughput sequencing technology, has provided strong technical support for identifying disease-related genomic loci and genes and genotype-phenotype associations. However, traditional chromosomal karyotype analysis can only detect large-fragment chromosomal abnormalities (resolution: 5–10 Mb) and cannot identify microdeletions/microduplications (eg, 15q11.2q13.1 deletion), resulting in a high missed diagnosis rate.
This study aimed to address three core questions: (1) Whether CNV-seq has significant advantages over traditional karyotype analysis in detecting genetic etiologies of FGR? (2) Whether Trio-WES has supplementary diagnostic value for FGR cases negative for karyotype/CNV-seq? (3) Whether there are differences in genetic abnormality distribution and pregnancy outcomes among FGR cases diagnosed at different gestational ages? Its unique contributions lie in: ① Verifying the effectiveness of the “karyotype + CNV-seq + Trio-WES” stepwise protocol in the FGR population in Southwest China for the first time; ② Discovering that the Trio-WES detection rate is significantly higher in FGR cases diagnosed before 28 weeks than in late pregnancy, providing a basis for gestational age-stratified testing.
In this study, high-throughput sequencing technology was used to perform chromosomal karyotype analysis and CNV-seq detection on fetuses with FGR indicated by prenatal ultrasound. Additionally, Trio-WES analysis was conducted on FGR cases with negative results in both karyotype analysis and CNV-seq. The aim was to explore the application value of high-throughput sequencing technology in prenatal genetic diagnosis of FGR, thereby providing a theoretical basis for improving the etiological diagnosis rate of FGR and optimizing pregnancy outcomes.
Materials and Methods
General Information
A retrospective analysis was performed on 235 fetuses who underwent invasive prenatal diagnosis in Liuzhou Maternal and Child Health Hospital due to prenatal ultrasound-diagnosed fetal growth restriction (FGR) from January 2019 to March 2025. The diagnostic criteria for FGR were defined as follows: ultrasound-estimated fetal weight (EFW, calculated using the Hadlock C formula) or abdominal circumference (AC) < the 10th percentile for the same gestational age.3 All FGR cases underwent Doppler ultrasound of the fetal umbilical artery and middle cerebral artery to exclude FGR caused by simple placental blood flow abnormalities. Gestational age was determined by first-trimester ultrasound measurements.
Exclusion criteria included hypertensive disorders in pregnancy, maternal infections, intrauterine infections, abnormal nutritional factors, and multiple pregnancies. The sample size was estimated based on preliminary pilot results (3.5% abnormal detection rate by karyotype analysis, 10.8% by CNV-seq), with α = 0.05 and β = 0.2. Using PASS software, the minimum required sample size was calculated to be 210 cases. Considering a 10% follow-up loss rate, 235 cases were finally included.
A total of 235 pregnant women were enrolled in this study, with a mean age of (30.2±5.3) years. The gestational age at FGR diagnosis was (28.4±3.5) weeks, and the gestational age at invasive prenatal diagnosis was (28.1±3.2) weeks. All cases underwent both G-banding karyotype analysis and CNV-seq, among which 19 FGR cases with negative results in both karyotype analysis and CNV-seq were further subjected to Trio-WES.4 All pregnant women received prenatal genetic counseling and were fully informed of the indications, limitations, and risks of the tests. After signing the informed consent form, appropriate invasive puncture procedures were selected based on the gestational age at the time of consultation. All operations were strictly performed in accordance with relevant diagnostic and therapeutic specifications.
The protocol for this retrospective study was reviewed and approved by the Institutional Review Board (IRB)/Ethics Committee of Liuzhou Maternal and Child Health Hospital, Guangxi, China (Approval No.: 2023–171). The IRB granted a waiver of individual informed consent for the access and use of patient medical records. This waiver was justified on the grounds that the study was retrospective in nature, involved no more than minimal risk to the subjects, and the research could not practicably be carried out without the waiver. Furthermore, all data utilized were fully anonymized prior to analysis; all personal identifiers were permanently deleted and replaced with non-identifiable codes. Throughout the study, stringent measures were implemented to protect data confidentiality, including storage on encrypted servers and limiting access to the research team. This study was conducted in accordance with the ethical standards outlined in the Declaration of Helsinki.
Detection Methods
Chromosomal Karyotype Analysis: The test object was the fetus, with samples sourced from fetal amniotic fluid or umbilical cord blood. Amniotic fluid samples were centrifuged at 2000 rpm for 10 minutes to remove upper maternal blood cells (to avoid maternal blood contamination); umbilical cord blood samples were used directly without prior maternal blood removal. Samples were subjected to cell culture using medium supplemented with GIBCO fetal bovine serum, followed by chromosome specimen preparation using G-banding technology (with C-banding or N-banding if necessary). In accordance with the International System for Human Cytogenomic Nomenclature (ISCN, 2020), 20 well-spread metaphase spreads of moderate length were analyzed under an oil immersion microscope for each specimen. If karyotypic abnormalities were identified, the number of spreads analyzed was increased to 100.
Low-Coverage Copy Number Variation Sequencing (CNV-Seq)
(1) Genomic DNA extraction: Genomic DNA was extracted from fetal amniotic fluid/umbilical cord blood using a magnetic bead-based method; (2) DNA library construction: Libraries were constructed via fragmentation, end repair, adapter ligation, and PCR amplification; (3) Sequencing platform: High-throughput sequencing was performed on the Illumina NovaSeq 6000 platform, with a sequencing depth of 0.1×–0.3×; (4) Bioinformatics analysis: Sequencing data were aligned to the human reference genome (hg19), and CNVs were analyzed using Copy Number Variation Analyzer v3.0 software (threshold: CNV fragment length ≥ 100 kb and copy number ≥ 3 or ≤ 1). The clinical significance of CNVs was determined by searching databases such as UCSC, DECIPHER, OMIM, ClinVar, DGV, and PubMed. In this study, CNV-seq abnormalities were defined as numerical chromosomal abnormalities, structural chromosomal abnormalities including pathogenic and likely pathogenic CNVs, and VOUS.
Whole Exome Sequencing (WES)
(1) Genomic DNA extraction: Genomic DNA was extracted from fetal amniotic fluid/umbilical cord blood and parental peripheral blood (as control samples) using a magnetic bead-based method; (2) Target gene capture and high-throughput sequencing: The exome region was captured using the Agilent SureSelect Human All Exon V6 kit, and sequencing was performed on the Illumina NovaSeq 6000 platform with an average sequencing depth ≥ 100×; (3) Data filtering and bioinformatics analysis: Low-quality reads (Q30 < 80%) were filtered out, and the remaining data were aligned to the human reference genome (hg19). Single nucleotide variants (SNVs) and insertions/deletions (InDels) were detected using GATK v4.2.0 software, and rare variants were screened using databases such as ExAC and gnomAD; (4) Sanger sequencing verification: Suspected pathogenic variants were verified by Sanger sequencing to trace their origin in the fetus and parents. All samples were verified by Short Tandem Repeat (STR) genotyping (16 STR loci) to confirm fetal origin and exclude maternal blood contamination; no maternal blood contamination had been detected in this study.
Genetic Counseling and Follow-Up of Pregnancy Outcomes
All cases received genetic counseling after the detection reports were available. Follow-up of pregnancy outcomes for all cases was conducted via telephone or the Guangxi Maternal and Child Health System, with a follow-up period ranging from diagnosis to 2 years postnatally. Monitoring indicators included: (1) Fetal growth curve during pregnancy (EFW assessed by ultrasound every 2 weeks); (2) Gestational age and birth weight at delivery; (3) Postnatal growth (height/weight at 1 and 2 years, compared with age-matched growth standards); (4) Neurodevelopmental assessment (using the Denver Developmental Screening Test, DDST).Specific pregnancy outcomes were defined as: (1) Termination of pregnancy (TOP, with recorded gestational age and reason); (2) Live birth (distinguished into preterm birth < 37 weeks and term birth ≥ 37 weeks, with recorded birth weight and whether it was low birth weight < 2500 g); (3) Stillbirth (with recorded gestational age).
Statistical Methods
Data analysis was performed using SPSS 26.0 software. Count data were presented as numbers (n) and percentages (%). The chi-square (χ2) test was used to compare differences between groups. A P value < 0.05 was considered statistically significant.
Results
Abnormal Results Detected by Chromosomal Karyotype Analysis and CNV-Seq, and Pregnancy Outcomes
Among the 235 FGR cases, karyotype analysis identified 9 cases of chromosomal abnormalities (3.8%, 9/235), including 3 cases of numerical abnormalities (2 cases of trisomy 18, 1 case of trisomy 13), 3 cases of chimerism, and 3 cases of structural abnormalities (2 cases of deletions, 1 case of derivative chromosome). All these cases underwent termination of pregnancy (cases numbered 1–9).In cases with normal chromosomal karyotype results, CNV-seq detected 17 abnormalities (7.5%, 17/226), including 14 pathogenic CNVs and 3 CNVs of uncertain clinical significance. Among these 17 cases, 10 underwent termination of pregnancy (cases numbered 10, 11, 12, 15, 16, 17, 18, 19, 23, and 24 in Table 1), 3 of which were complicated with structural abnormalities of organs. The remaining 7 cases had live births (cases numbered 13, 14, 20, 22, 25, 26, and 21). Among these 7, 6 showed no abnormalities during postnatal follow-up until 2 years of age. One case (case 21, with a de novo pathogenic variant) was delivered by cesarean section at 35 weeks of gestation due to fetal distress, with a birth weight of 1.4 kg; postnatal follow-up until 2 years of age revealed clinical manifestations of developmental delay and hypertonia.
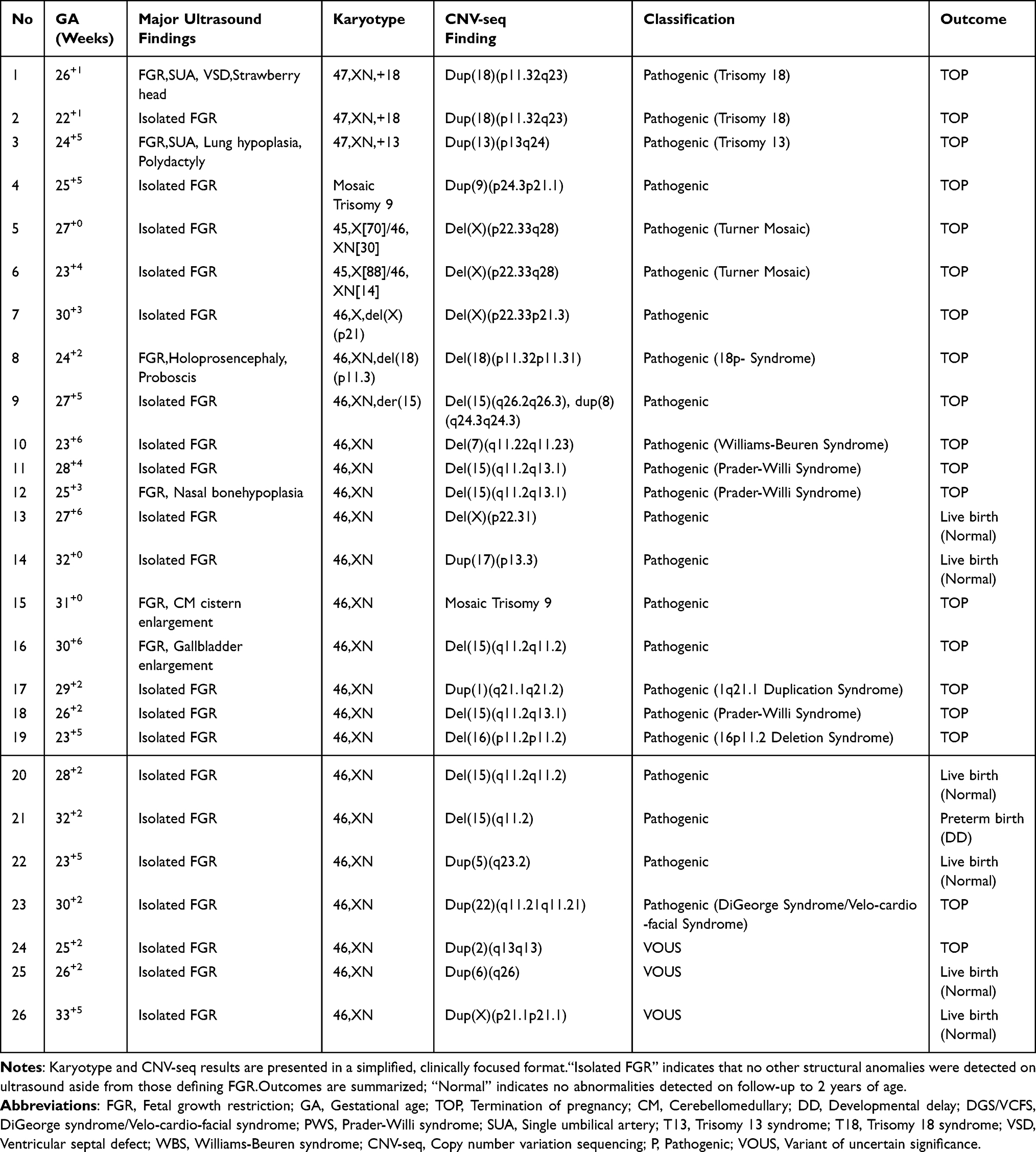 |
Table 1 Chromosomal Abnormalities and Pregnancy Outcomes in 26 FGR Fetuses |
Abnormal Results Detected by Trio-WES and Pregnancy Outcomes
Among the cases with negative karyotype and CNV-seq results, 19 underwent Trio-WES, which detected 3 pathogenic variants and 1 likely pathogenic variant; all these 4 cases underwent termination of pregnancy (TOP). Two additional VOUS were identified: one was of paternal origin and resulted in a live birth with normal follow-up to 2 years of age; the other was a de novo variant, and the pregnancy was terminated.Detailed information on the genetic variants, inheritance patterns, associated diseases, and pregnancy outcomes of these 6 FGR fetuses is shown in Table 2.
 |
Table 2 Genetic Variants and Pregnancy Outcomes Identified by Trio-WES in 6 FGR Fetuses |
Comparison of Chromosomal Karyotype Analysis, CNV-Seq, and Trio-WES Techniques in the Detection of Genetic Etiologies of FGR
Among the 235 FGR specimens, G-banded karyotype analysis detected 9 abnormal cases (3.8%, 9/235), CNV-seq detected 26 abnormal cases (11.1%, 26/235), and the difference in abnormal detection rate between the two techniques was statistically significant (χ2 = 8.76, P = 0.003 < 0.05). Among the cases negative for both karyotype and CNV-seq, Trio-WES detected an additional 6 abnormal cases (31.6%, 6/19), with a higher detection rate in cases diagnosed before 28 weeks (42.9%, 3/7) than in late pregnancy (15.4%, 3/19), suggesting that early-pregnancy FGR may be more prone to monogenic variants. In total, 32 abnormal cases (13.6%, 32/235) were detected by the combination of karyotype analysis and high-throughput sequencing. See Figure 1.
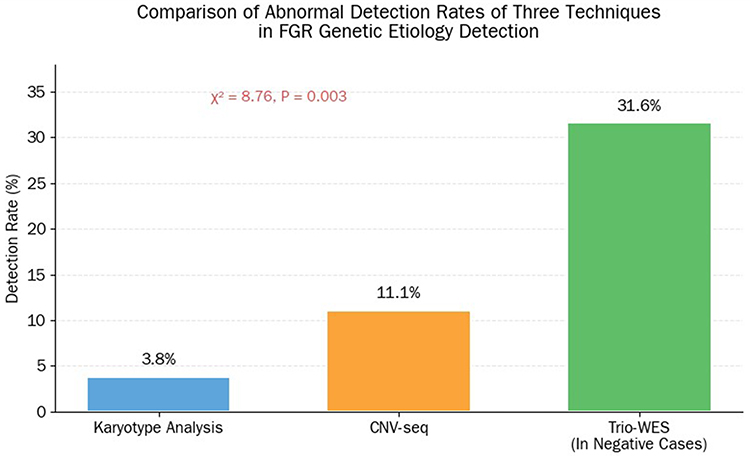 |
Figure 1 Comparison of Abnormal Detection Rates of Three Techniques in FGR Genetic Etiology Detection. Notes: A bar chart showing the detection rates of the three techniques: karyotype analysis (3.8%), CNV-seq (11.1%), and Trio-WES (31.6% in karyotype/CNV-seq negative cases). The vertical axis represents the detection rate (%), and the horizontal axis represents the detection technique. |
Analysis of Genetic Detection Results and Pregnancy Outcomes of FGR in Different Gestational Age Groups Stratified by the Gestational Age at First Diagnosis of FGR
FGR cases were divided into three groups based on the gestational age at first diagnosis: <28 weeks (n=105), 28–31+6 weeks (n=76), and ≥32 weeks (n=54).
The average gestational age at delivery was (36.6±4.95) weeks in the <28 weeks group, (38.4±4.99) weeks in the 28–31+6 weeks group, and (38.4±4.91) weeks in the ≥32 weeks group. The average neonatal birth weight was (2.59±0.82) kg, (2.52±0.83) kg, and (2.53±0.82) kg in the three groups, respectively.
The TOP rate (29.5%, 31/105) and low birth weight rate (48.6%, 36/74; denominator: number of live births in the group) in the <28 weeks group were significantly higher than those in the other two groups (P < 0.05). There were no statistically significant differences in the genetic abnormality detection rate (18.1% vs 10.5% vs 9.3%), stillbirth rate (0.1% vs 1.3% vs 1.9%), preterm birth rate (15.2% vs 11.8% vs 16.7%), or term birth rate (54.3% vs 71.1% vs 70.4%) among the three groups (P > 0.05).See Table 3.
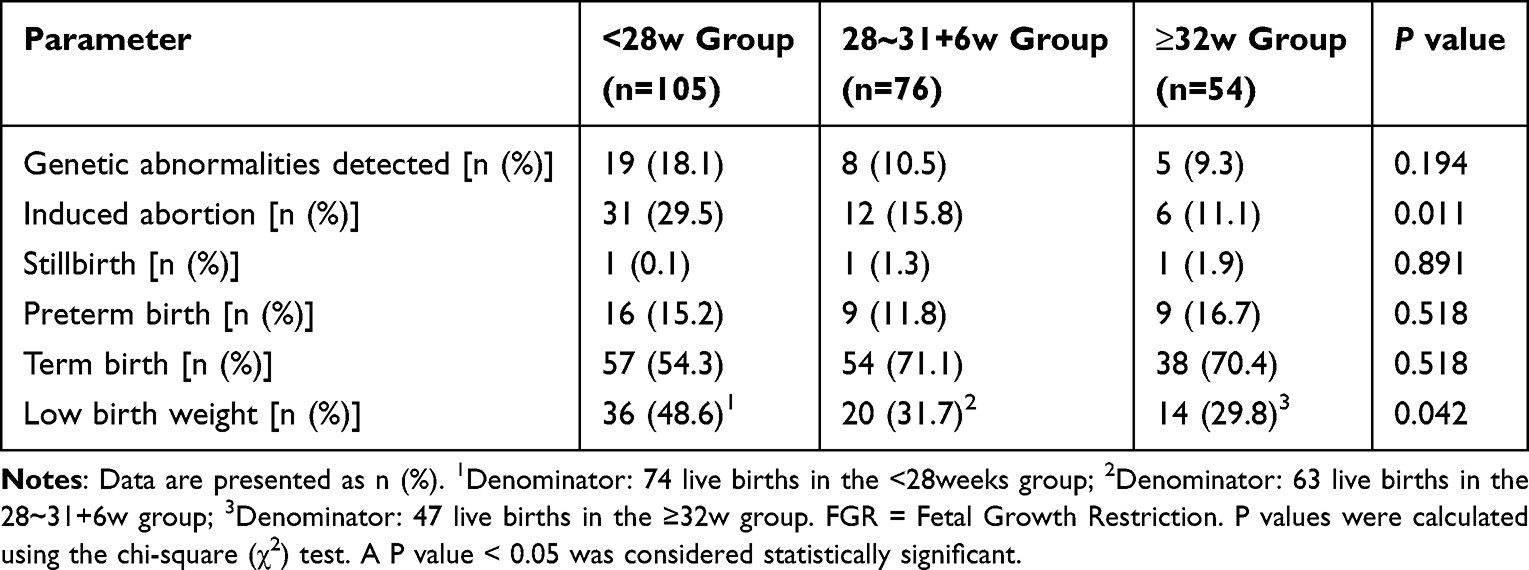 |
Table 3 Analysis of Genetic Detection Results and Pregnancy Outcomes of FGR in Different Gestational Age Groups |
Discussion
Advantages of High-Throughput Sequencing in the Genetic Diagnosis of FGR
The genetic etiology of fetal growth restriction (FGR) is complex, with previous studies indicating that approximately 5%–20% of FGR cases are attributable to fetal genetic abnormalities.5 In a study by Tong et al6 involving 120 FGR cases subjected to karyotyping and chromosomal microarray analysis (CMA), a total of 14 abnormalities (11.7%) were detected. Notably, CMA identified an additional 4%–10% of copy number variations (CNVs) in cases with a normal karyotype. Similarly, Chen et al7 reported in a cohort of 149 FGR pregnancies that the detection rate of chromosomal abnormalities by CMA (13.42%) was 8.05% higher than that by karyotyping, underscoring the significant value of CMA in the etiological diagnosis of FGR and supporting its use as a first-line testing strategy.
In the present study, CNV-seq detected abnormalities in 26 cases (11.1%), which was 7.3 percentage points higher than the yield of karyotyping (3.8%). Furthermore, CNV-seq identified additional abnormalities in 7.5% of karyotypically normal cases. These findings are largely consistent with the literature cited above and validate the advantages of CNV-seq,8 including its higher resolution (enabling detection of CNVs larger than 100 kb), ability to identify microdeletions/duplications that are challenging for karyotyping (such as deletions in 7q11.22q11.23 and 15q11.2q13.1), shorter turnaround time (1–2 weeks), and consequent greater suitability for rapid prenatal diagnosis.
For FGR cases with normal results from both karyotyping and CNV-seq, Trio-WES can further improve the diagnostic yield. A meta-analysis by Pauta et al9 of 8 studies involving 146 fetuses with isolated FGR demonstrated that Trio-WES detected an additional 12% of pathogenic variants, particularly in cases with gestational age < 32 weeks. Similarly, Lena S et al10 performed Trio-WES on 190 FGR cases with normal karyotype/CMA and no structural anomalies, identifying clinically significant variants in 15.2% of cases.
In our study, Trio-WES was performed on 19 karyotypically and CNV-seq normal cases, revealing abnormalities in 6 cases (31.6%). Although this diagnostic rate is higher than those reported in the literature, the discrepancy may be attributed to our relatively small sample size (n=19) and potential selection bias, as all included cases had undergone invasive diagnostic procedures and may therefore represent a subgroup at higher genetic risk. Nevertheless, our results support the utility of Trio-WES as a complementary diagnostic tool for FGR, particularly in cases where a monogenic disorder (such as osteogenesis imperfecta or neurodevelopmental disorders) is suspected.
Clinical Significance of FGR-Related Genetic Abnormalities and Association with Pregnancy Outcomes
This study detected several genetic abnormalities associated with specific syndromes, with significant differences in prognosis: (1) Microdeletion/microduplication syndromes (eg, Williams-Beuren syndrome, Prader-Willi syndrome): These syndromes are often accompanied by moderate to severe intellectual disability and multi-organ malformations. For example, 15q11.2q13.1 deletion (Prader-Willi syndrome) silences imprinted genes such as SNRPN, disrupting growth regulatory pathways, leading to FGR in the fetal period and obesity/intellectual disability postnatally; all such cases in this study chose TOP. (2) Monogenic diseases (eg, G6PD deficiency, primary microcephaly): These can cause severe neonatal complications (eg, hemolysis, neurodevelopmental delay), and all affected cases underwent TOP. (3) VOUS: Among 5 VOUS cases (3 from CNV-seq, 2 from Trio-WES), 2 had normal live births, indicating that clinical decisions for VOUS may pose difficulties for genetic counseling and clinical decision-making,11 we should integrate “variant origin (paternal/maternal/de novo)”, “ultrasound findings (isolated/combined malformations)”, and dynamic monitoring to avoid excessive TOP.
Consistent with literature reports12,13 that “the earlier the onset of FGR, the poorer the pregnancy outcome”, this study found that the <28 weeks group had a significantly higher TOP rate (29.5%) and low birth weight rate (48.6%) than the late-pregnancy groups (P < 0.05), suggesting that early-pregnancy FGR is more likely to be associated with severe genetic abnormalities or placental insufficiency, requiring more active genetic evaluation and monitoring.
Study Limitations and Clinical Recommendations
This study has several limitations: (1)Single-center retrospective design, which may introduce selection bias (eg, only FGR cases undergoing invasive diagnostic procedures were included, while mild FGR cases were not enrolled). (2) Small sample size for Trio-WES (19 cases), which may overestimate the detection rate; large-sample studies are needed for verification. (3) Follow-up loss in some cases (due to uncontrollable factors such as lost contact with parents) led to incomplete data on neonatal complications, making it difficult to fully evaluate long-term prognosis. (4) Furthermore, the influence of non-genetic factors such as maternal thyroid dysfunction and placental vascular pathology on FGR was not completely ruled out; subsequent multicenter prospective studies are needed to further control for confounding factors. (5) Cases with FGR caused by simple placental blood flow abnormalities were excluded, which may underestimate the impact of non-genetic factors. (6) WES did not detect non-coding region variants, potentially missing FGR caused by regulatory region variants. (7) Follow-up duration was only 2 years, failing to assess long-term neurodevelopmental outcomes (eg, school-age cognitive function).
Based on the study results and supporting Shi et al14 conclusion that “WES has supplementary diagnostic value for isolated FGR with normal CMA/CNV-seq”, the following clinical recommendations are proposed: (1) Optimize the detection protocol: After ultrasound diagnosis of FGR, “karyotype analysis + CNV-seq” is recommended as the first-line prenatal genetic diagnosis protocol, replacing traditional single karyotype analysis. (2) Indications for Supplemental Testing: For patients with negative karyotype and CNV-seq results, trio-based whole-exome sequencing (Trio-WES) is recommended when either of the following conditions is present:
a) Diagnosis of fetal growth restriction (FGR) before 28 weeks of gestation;
b) Coexistence of unexplained sonographic soft markers (eg, ventriculomegaly, microcephaly) or structural anomalies. (3) Genetic counseling strategy: For VOUS cases, individualized counseling should be provided based on parental variant tracing, database comparison, and dynamic ultrasound monitoring; long-term follow-up and regular re-evaluation are necessary for continued pregnancies. (4) Long-term follow-up management: Live-born FGR neonates should be followed up to at least 2 years, with monitoring of growth and neurodevelopment; prenatal genetic data should be re-evaluated postnatally based on clinical manifestations if necessary.15 (5) For future research, efforts should focus on elucidating the mechanisms of monogenic variants in early-onset FGR and exploring the genotype-phenotype correlations. Concurrently, establishing a multicenter genetic database for FGR is recommended to provide data support for developing personalized diagnostic workflows.
Conclusion
This study confirms that high-throughput sequencing technologies (CNV-seq and Trio-WES) significantly improve the detection rate of genetic abnormalities in FGR fetuses: compared with traditional karyotype analysis (3.8%), the combined detection rate of “karyotype + CNV-seq + Trio-WES” reaches 13.6%. CNV-seq compensates for the insufficient resolution of traditional karyotype analysis, while Trio-WES serves as an effective supplement for cases negative for karyotype/CNV-seq. FGR cases diagnosed before 28 weeks have higher TOP rates and Trio-WES detection rates, requiring more active prenatal monitoring and genetic evaluation.16
Despite the limitation of a relatively small sample size for Trio-WES (n=19), which warrants validation in larger cohorts, the stepwise diagnostic protocol established in this study provides a practical and efficient framework for the prenatal genetic diagnosis of FGR. This model can be adapted to various clinical settings and resource availability, thereby offering a foundation for future guideline development and contributing to improved perinatal outcomes through precise genetic diagnosis.
In clinical practice, the “karyotype analysis + CNV-seq” protocol is recommended as the first-line option for prenatal genetic diagnosis of FGR, with Trio-WES added when necessary. Combined with genetic counseling and long-term follow-up, this approach provides precise support for FGR pregnancy management and ultimately improves perinatal outcomes, laying a foundation for the development of future FGR prenatal diagnosis guidelines.
Acknowledgments
We would like to express our sincere gratitude to all the patients and their families who participated in this study. We are deeply indebted to Dr. Sumei Wang for her invaluable guidance and supervision throughout the research process. Additionally, we would like to acknowledge the clinicians, sonographers, and laboratory technicians at the Prenatal Diagnosis Center of Liuzhou Maternal and Child Health Hospital, Guangxi Zhuang Autonomous Region, for their precious assistance in sample collection, clinical data management, and technical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Guangxi Key Research and Development Program [Grant No. Guike AB24010063], the Guangxi Health Commission [Grant No. S2023067], and the Self-Funded Research Project of Guangxi Health Commission [Grant No. Z-B20231517].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wu JJ, Chen JH, Wang DG. Research progress on the genetic causes of fetal growth restriction. Obstet Gynecol Genet. 2023;13(2):40–10.
2. Zhu H, Lin SB, Huang LH, et al. Analysis of chromosomal microarray results in fetuses with growth restriction. Chin J Prenatal Diagn. 2016;8(2):16–18.
3. McCowan L, Figueras F, Anderson N. Evidence-based national guidelines for the management of suspected fetal growth restriction: comparison, consensus, and controversy. Am J Obstet Gynecol. 2018;218(2):S855–S868. doi:10.1016/j.ajog.2017.12.004
4. Monaghan KG, Leach NT, Pekarek D, et al. The use of fetal exome sequencing in prenatal diagnosis: a points to consider document of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2020;22(4):675–680. doi:10.1038/s41436-019-0731-7
5. Fetal Medicine Group, Perinatal Medicine Branch, Chinese Medical Association. Expert consensus on fetal growth restriction (2019 edition). Chin J Perinat Med. 2019;22(6):361–380.
6. Tong YL, Pan H, Yu L, et al. Application of chromosomal microarray analysis in prenatal diagnosis of fetal growth restriction. Chin J Perinat Med, Mar. 2025;28:3.203–210.
7. Chen Y, Xie YJ, Jiang YY, et al. The genetic etiology diagnosis of fetal growth restriction using single-nucleotide polymorphism-based chromosomal microarray analysis. Front Pediatr. 2021;9:743639. doi:10.3389/fped.2021.743639
8. Luo XJ, Guo YY, Huang HM, et al. Diagnostic value of whole-genome copy number variation sequencing in detecting chromosomal abnormalities in fetal growth restriction. Chin J Clin Lab Sci. 2020;38(12):921–925.
9. Pauta M, Martinez-Portilla RJ, Meler E, et al. Diagnostic yield of exome sequencing in fetal growth restriction: systematic review and meta-analysis. Prenat Diagn. 2023;43(5):596–604. doi:10.1002/pd.6339
10. Reissig LS, et al. Diagnostic yield of exome sequencing in fetal growth restriction without structural malformations. Genet Med. 2022. doi:10.1016/j.gim.2022.01.018
11. Wang SX, Ma JM. Clinical pathway selection based on chromosomal microarray analysis in prenatal diagnosis. Chin J Perinat Med. 2019;22(1):26–29.
12. Shah DK, Pereira S, et al. Long-term neurologic consequences following fetal growth restriction: the impact on brain reserve. Dev Neurosci. 2025;47(2):139–146. doi:10.1159/000539266
13. Juan J, Yang HX. Impact of fetal growth restriction on perinatal outcomes and long-term health. Chin J Pract Gynecol Obstet. 2020;36(8):710–713.
14. Shi XM, Huang YL, Ding H, et al. Utility of whole exome sequencing in the evaluation of isolated fetal growth restriction in normal chromosomal microarray analysis. Ann Med. 2025;57(1):2476038. doi:10.1080/07853890.2025.2476038
15. Yue F, Hao MZ, Jiang DD, Liu RZ, Zhang HG. Prenatal phenotypes and pregnancy outcomes of fetuses with 16p11.2 microdeletion/microduplication. BMC Pregnancy Childbirth. 2024;24(1):494. doi:10.1186/s12884-024-06702-w
16. Paz Y, Miño MF, Pauta M, et al. Postnatal genetic and neurodevelopmental assessment in infants born at term with severely low birth weight of non-placental origin[J]. Obstet Gynecol Surv. 2024;79(3):141–143. doi:10.1097/01.ogx.0001010420.53414.ec
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.