Back to Journals » Open Access Emergency Medicine » Volume 14
Application of Automated External Defibrillators in Motorcycle Ambulances in Thailand’s Emergency Medical Services
Authors Apiratwarakul K ![]() , Tiamkao S
, Tiamkao S ![]() , Cheung LW
, Cheung LW ![]() , Celebi I
, Celebi I ![]() , Suzuki T, Ienghong K
, Suzuki T, Ienghong K ![]()
Received 11 February 2022
Accepted for publication 6 April 2022
Published 12 April 2022 Volume 2022:14 Pages 141—146
DOI https://doi.org/10.2147/OAEM.S361335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Korakot Apiratwarakul,1 Somsak Tiamkao,2 Lap Woon Cheung,3,4 Ismet Celebi,5 Takaaki Suzuki,6 Kamonwon Ienghong1
1Department of Emergency Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Department of Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 3Department of Accident and Emergency, Princess Margaret Hospital, Kowloon, Hong Kong; 4Emergency Medicine Unit, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Pokfulam, Hong Kong; 5Department of Paramedic, Gazi University, Ankara, Turkey; 6Department of Emergency and Critical Care Medicine, University of Tsukuba Hospital, Tsukuba, Japan
Correspondence: Kamonwon Ienghong, Department of Emergency Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, 40002, Thailand, Tel +66 043 366 869, Email [email protected]
Background: Access time to emergency patients is a critical factor that affects the outcomes of life-or-death situations, especially in the cases of out-of-hospital cardiac arrests (OHCA). This study focused on developing a new model of emergency medical services (EMS) using a motorcycle-based ambulance (motorlance) with an automated external defibrillator (AED). There are currently no studies regarding access time for this vehicle. This study aimed at utilization of an AED in conjunction with motorlance and comparing the response time between a traditional ambulance and a motorlance.
Methods: This was a prospective study conducted in the EMS department of Srinagarind Hospital, located in Khon Kaen, Thailand, over a five-month period, from September 2021 to January 2022. Data were recorded employing a national standard of operations record form used for Thailand EMS departments nationwide.
Results: The 891 cases were divided into two groups which were motorlance and ambulance. The activation times for motorlance and ambulance were 0.44 minutes and 1.42 minutes, respectively (p < 0.001) and the response time in the motorlance group was 7.20 minutes compared with 9.25 minutes in the ambulance group. In OHCA, the motorlance with AED arrived at patients location and assisted to continue resuscitation at the hospital 88.9% of the time.
Conclusion: AED used in conjunction with motorcycle ambulances had shorter periods of both activation time and response time compared to ambulances. The use of AEDs clearly increases the number of continuous resuscitations in out-of-hospital cardiac arrest patients.
Keywords: ambulance, cardiac arrest, emergency care, prehospital emergency care, response time
Introduction
Out of hospital cardiac arrest (OHCA) is the most urgent condition in emergency medical services (EMS).1,2 Quick access to patients for assessment and treatment is vital and increases the chances of survival for the patient.3,4 In the first stage of the chain of necessary treatment, OHCA patients will need chest compression and defibrillation with an automated external defibrillator (AED) as soon as possible to improve their chances of survival.5–7 In Thailand, AEDs in public areas are still fairly uncommon and especially in provinces outside of Bangkok (the capital city of Thailand), installing an AED is almost impossible due to their rural nature. Therefore, the management of OHCA is almost solely the duty of emergency medical operations who must bring equipment and personnel for quick and efficient treatment.8,9
Reaching OHCA patients in time is of the utmost importance. A study found that every one-minute delay with chest compressions and defibrillation decreases survival by 7–10%, and even with prompt treatment, only ten percent of OHCA survivors were found to make it.10,11 In Thailand, there is considerable traffic congestion, especially in large cities. The development of the use of motorcycle ambulances (motorlance) was done primarily with an aim to reduce response time. Motorlances take significantly less time to reach patients, resulting in rapid patient access, reduced waiting times, and increased response to expectations in emergency situations. The model of AED used with a motorlance was established to solve problems and promote sustainable development in Thailand’s EMS.
The rapid access is the key for EMS, motorcycle model was established to resolve delay response time in major cities that have traffic congestion. The advantage of this vehicle can travel in confined space with decreased response time than traditional ambulance. In mass casualty incidence, the motorlance was used to be a vehicle to support medical director to access the situation.
This study aimed at the utilization of an AED in conjunction with motorlances and comparing the response time between a traditional ambulance and a motorlance.
Materials and Methods
Study Design and Population
This was a prospective study conducted in the EMS department of Srinagarind Hospital, a major university hospital located in Khon Kaen, Thailand. The EMS serviced an average of 2000 cases per year in tertiary care from September 2021 to January 2022.
All cases of EMS operations in the period of the study were enrolled with both motorlance and traditional ambulance delivery to access patients. Cases with incomplete data and days of operation under poor weather conditions were excluded from this study.
This study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines. The Khon Kaen University Ethics Committee for Human Research approved the study (HE641417). The informed consent was waived due to the fact that this study was based on the routine operation of EMS since patient confidentiality protection had been guaranteed. The patient identification could not be identified by using study number.
Operating Definitions
Activation time was defined as times starting from initial dispatch to vehicle of (motorlance and traditional ambulance) being en route. Response time was defined as times from the 1669 emergency call-center call receipt to arrival on scene.
The motorlances were developed from a factory stock Honda New Forza 300 (Honda Motor Company, Ltd.; Tokyo, Japan) models (Figures 1 and 2). Three gadget boxes were then attached to the rear of the motorlance. The box connected to the side of the motorlance and clearly marked so as to provide easy access to the AED equipment.
 |
Figure 1 Motorlance model, side view. |
 |
Figure 2 Motorlance model, front view. |
Primary Outcome and Statistical Analysis
Data was recorded employing the national standard of operation recording form for Thailand EMS consisting of demographic information of patients including age and gender, operation time, type of patient, time of AED accessed, and status of patients when the emergency vehicle arrived. This information was then recorded in the EMS database of Srinagarind Hospital.
The two data collectors were well-trained emergency room physicians who verified the information from the EMS database. After that, a double data entry method was performed. In cases of non-matched information, the senior collectors checked and collected the data.
The time (response time and activation time) utilized for this study was decided by one synchronized clock which was found within the dispatch center. The dispatcher observed EMS operations by means of telemedicine. The time of each operation handled is recorded by computer into the EMS database.
The Khon Kaen University’s license for IBM SPSS for Windows version 27.0 (IBM Corp.; Armonk, New York, USA) was used for statistical analysis. Categorical data were presented as percentages and continuous data were presented using means and standard deviations. Univariate analysis was performed using a Wilcoxon rank sum tests for numerical data and a Chi-square test for comparing data between the groups.
Results
In the five-month period of study, a total of 901 cases of EMS operation were examined. The ten cases which were excluded from the study were the result of having incomplete data or taking place during poor weather conditions. The remaining 891 cases were divided into two groups (motorlance and ambulance). The characteristics of the services and subjects are shown in Table 1. The mean age of the patients in the motorlance group was 49.5±8.2 years, and 56.7% (n = 182) were male. The activation times for motorlance and ambulance were 0.44 minutes and 1.42 minutes, respectively (p < 0.001), and the response time in the motorlance group was 7.20 minutes as compared with 9.25 minutes in the ambulance group. Both groups of the study operated primarily in the daytime with non-trauma patients.
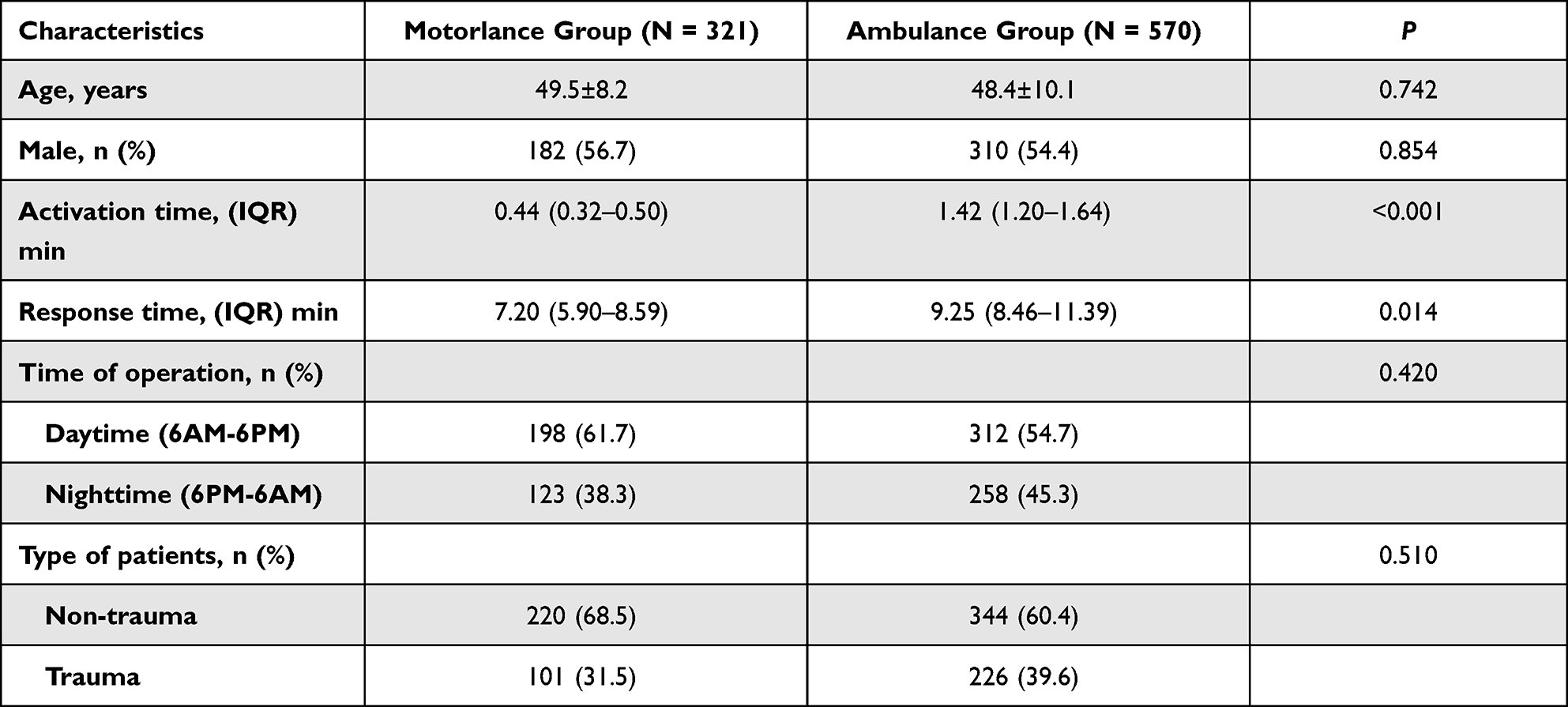 |
Table 1 Baseline Characteristics of the EMS Patients (N = 891) |
The motorlance equipped with an AED operated in cases with telephone triage of collapse or in cases of unresponsiveness from patients with 46 cases analyzed in Table 2. Cardiac arrest was the most common primary diagnosis at the scene with 39.1%, followed by syncope (26.1%) and hypoglycemia (15.2%). In cardiac arrest patients, shockable rhythm was performed in 55.6% of cases and response time in cases of the no pulse at the scene group was 6.44 minutes.
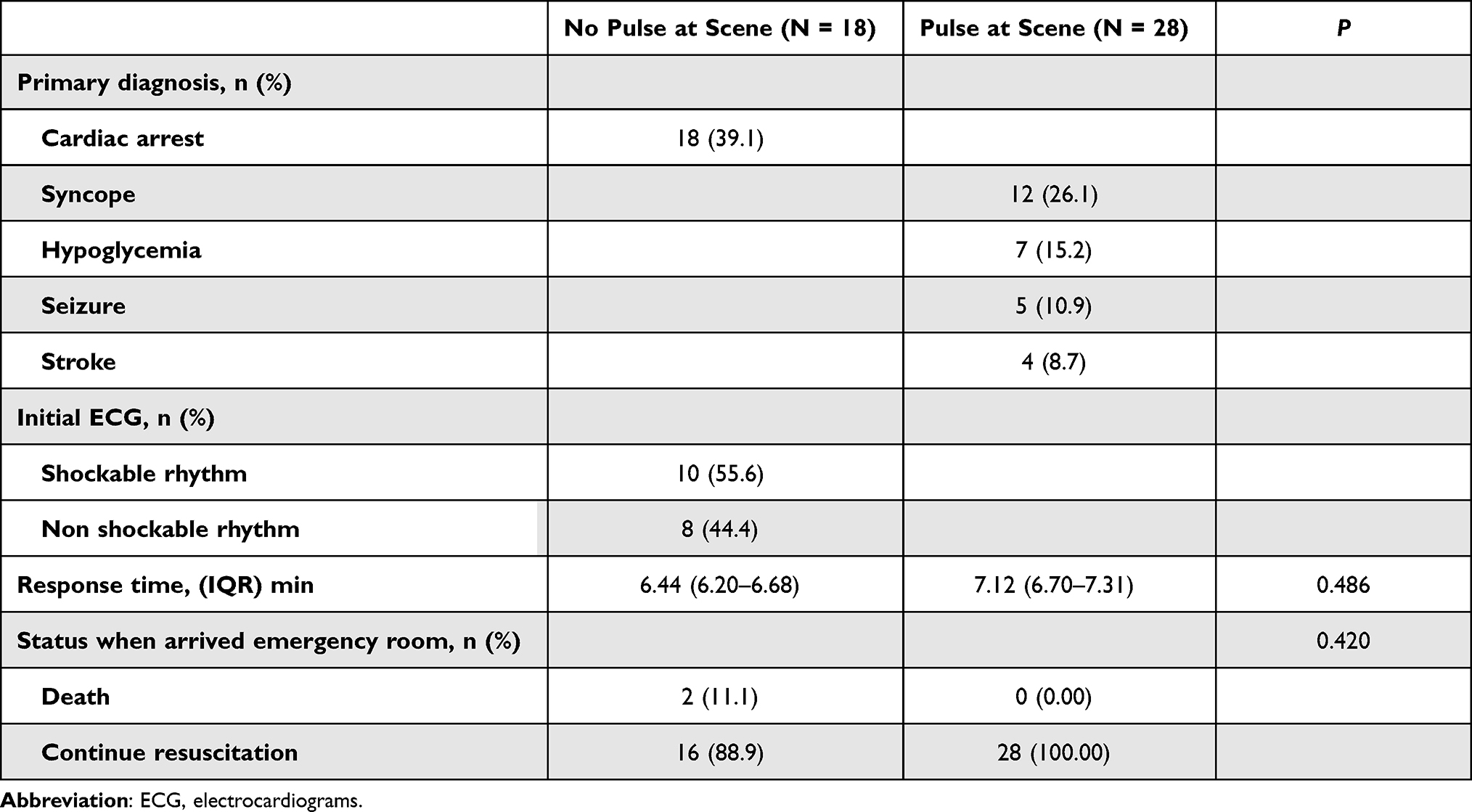 |
Table 2 The Services of a Motorlance Equipped with an AED (N = 46) |
Discussion
This study creates a new method of emergency patient access with the model using an emergency motorcycle base ambulance equipped with an AED. The objective is to compare the interval of access to emergency patients in a motorlance compared to that of a traditional ambulance, this includes studying the characteristics of the patients who used the AED installed in an emergency motorlance. The data of this study was gathered from the EMS database at Srinagarind Hospital in Khon Kaen, Thailand. The exclusion criteria did not include operations in rainy weather or weather resulting in poor driving conditions. This is because the operation poses a risk of danger to the motorlance as well as directly affects the length of time to reach emergency patients.
The time from dispatch to vehicle being en route (activation time) in the motorlance group took less time than that of an ambulance which was consistent with previous studies.8,9,12 The main reason is that the number of members operating with a motorlance team were fewer. The motorlance uses only one to two members for each operation, less than an ambulance that requires three to five members according to the standards of Thailand’s operations.13,14 Therefore, it takes less time from receiving a notification of an operation to a vehicle moving out of the hospital when the team is on a motorcycle.
We also found that the response time by the motorlance was shorter than an ambulance. This is consistent with previous studies which found that the motorlance is much more maneuverable in confined spaces or in traffic congestion than a typical ambulance in the form of a van.15,16 In addition, in Thailand there is still a serious problem of traffic giving way for ambulances en route to emergency scenes.17 Therefore, the use of motorcycles has become a new form of EMS operations in large cities where there is a higher likelihood of traffic jams or there are regularly many vehicles on the road as an adjustment of the hospital’s service units to fit the social context.18,19
In terms of the use of AEDs in conjunction with a motorlance, we found that throughout the five-month study period, there were forty-six cases of unresponsive or patients who had collapsed which meets the standard operating criteria to reaching the patient with an AED as quickly as possible.8,9,13,14 In this study there were eighteen cases with out-of-hospital cardiac arrest and ten cases whereof electrocardiograms were required for defibrillation as there were no AEDs in public areas. Therefore, the use of a motorlance equipped with AEDs increases the chances of survival for the patients with out-of-hospital cardiac arrest dramatically.8,9 In addition, the benefit of a motorlance equipped with an AED effectively addresses two common problems; access delays and the problem of AED storage in the public.
Unconscious patients were found in both groups (with and without pulse) that required the fastest access possible in conjunction with the use of AED at the scene. Therefore, EMS members use the time to reach such patients quickly until when assessing the symptoms of the patient at the scene, it was found that there were groups that had to use the AED device and those who did not need equipment.
In terms of continuous resuscitation, it was found that a motorlance equipped with an AED can provide continuous resuscitation at the emergency room for almost ninety percent of patients. This is an answer to an important problem for patients with out-of-hospital cardiac arrest outcomes.20–23
However, the study had limitations, the data from only one hospital where the population’s characteristics may differ from those in other areas as well as traffic conditions of the area of study is one of the provinces of Thailand where there may be different traffic conditions from other areas. In addition, there were limitations of the motorcycle model as it cannot operate under heavy rain or other severe weather conditions. This could not only be unsafe for the operator, but also damage the installed medical equipment.
In future study, we recommend to study the use of motorlance during COVID-19 pandemic. The motorlance used only two EMS members for each operation, which may decrease the risk of infection to health-care providers.
Conclusions
Motorcycle ambulances equipped with an AED had shorter periods of activation time and response time when compared to traditional ambulances. The use of AEDs can greatly increase the number of continuous resuscitations in out-of-hospital cardiac arrest patients.
Acknowledgments
The authors would like to express their sincere gratitude to Josh Macknick for acting as an English consultant. This study was funded by the Young Researcher Development Project of Khon Kaen University Year 2022.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Park JH, Song KJ, Shin SD, et al. Does second EMS unit response time affect outcomes of OHCA in multi-tiered systems? A nationwide observational study. Am J Emerg Med. 2021;42:161–167. doi:10.1016/j.ajem.2020.02.018
2. Ornato JP, Peberdy MA, Siegel CR, et al. Delay to initiation of out-of-hospital cardiac arrest EMS treatments. Am J Emerg Med. 2021;41:60–65. doi:10.1016/j.ajem.2020.12.024
3. Kashef MA, Lotfi AS. Evidence-based approach to out-of-hospital cardiac arrest. Curr Treat Options Cardiovasc Med. 2021;23(6):43. doi:10.1007/s11936-021-00924-3
4. Dicker B, Govender K, Howie G, et al. Positive association between ambulance double-crewing and OHCA outcomes: a New Zealand observational study. Resusc Plus. 2021;8:100187. doi:10.1016/j.resplu.2021.100187
5. Stoesser CE, Boutilier JJ, Sun CLF, et al. Moderating effects of out-of-hospital cardiac arrest characteristics on the association between EMS response time and survival. Resuscitation. 2021;169:31–38. doi:10.1016/j.resuscitation.2021.10.014
6. Banerjee P, Ganti L, Stead TG, et al. Every one-minute delay in EMS on-scene resuscitation after out-of-hospital pediatric cardiac arrest lowers ROSC by 5. Resusc Plus. 2020;5:100062. doi:10.1016/j.resplu.2020.100062
7. Sirikul W, Piankusol C, Wittayachamnankul B, et al. A retrospective multi-centre cohort study: pre-hospital survival factors of out-of-hospital cardiac arrest (OHCA) patients in Thailand. Resusc Plus. 2022;9:100196. doi:10.1016/j.resplu.2021.100196
8. Apiratwarakul K, Ienghong K, Mitsungnern T, et al. Use of a motorlance to deliver emergency medical services; a Prospective Cross Sectional Study. Arch Acad Emerg Med. 2019;7:e48.
9. Apiratwarakul K, Ienghong K, Gaysonsiri D, et al. Role of motorcycle-based ambulance (Motorlance) in major sporting events. J Med Assoc Thai. 2020;103:15–17.
10. Bateman RM, Sharpe MD, Jagger JE, et al. 36th International Symposium on Intensive Care and Emergency Medicine: Brussels, Belgium. Crit Care. 2016;20:94.
11. Hardeland C, Skåre C, Kramer-Johansen J, et al. Targeted simulation and education to improve cardiac arrest recognition and telephone assisted CPR in an emergency medical communication centre. Resuscitation. 2017;114:21–26. doi:10.1016/j.resuscitation.2017.02.013
12. Apiratwarakul K, Ienghong K, Bhudhisawasdi V, et al. Response times of motorcycle ambulances during the COVID-19 Pandemic. Open Access Maced J Med Sci. 2020;8:526–529. doi:10.3889/oamjms.2020.5527
13. Pochaisan O, Pattanarattanamolee R, Pongphuttha W, et al. Development of an emergency medical services system in Thailand: roles of the universal health coverage and the national lead agency. Emerg Med Australas. 2021;33(4):756–758. doi:10.1111/1742-6723.13794
14. Pattanarattanamolee R, Sanglun RY, Nakahara S. Community-based first responder network in rural Thailand: a case study of out-of-hospital cardiac arrest. Prehosp Disaster Med. 2021;36:234–236. doi:10.1017/S1049023X20001545
15. van der Pols H, Mencl F, de Vos R. The impact of an emergency motorcycle response vehicle on prehospital care in an urban area. Eur J Emerg Med. 2011;18:328–333. doi:10.1097/MEJ.0b013e32834624e8
16. Mongbo V, Ouendo EM, De Brouwere V, et al. Quality of caesarean delivery: a cross-sectional study in 12 hospitals in Benin. Rev Epidemiol Sante Publique. 2016;64:281–293. doi:10.1016/j.respe.2016.02.009
17. Shaikh S, Hashmi I, Baig LA, et al. Assessment of a mass media campaign on giving way to ambulances in five cities of Pakistan. J Pak Med Assoc. 2020;70:1510–1515. doi:10.5455/JPMA.18906
18. Brown TP, Booth S, Hawkes CA, et al. Characteristics of neighbourhoods with high incidence of out-of-hospital cardiac arrest and low bystander cardiopulmonary resuscitation rates in England. Eur Heart J Qual Care Clin Outcomes. 2019;5:51–62. doi:10.1093/ehjqcco/qcy026
19. Vollmer MAC, Radhakrishnan S, Kont MD, et al. The impact of the COVID-19 pandemic on patterns of attendance at emergency departments in two large London hospitals: an observational study. BMC Health Serv Res. 2021;21:1008. doi:10.1186/s12913-021-07008-9
20. Rees N, Howitt J, Breyley N, et al. A simulation study of drone delivery of Automated External Defibrillator (AED) in out of hospital cardiac arrest (OHCA) in the UK. PLoS One. 2021;16:e0259555. doi:10.1371/journal.pone.0259555
21. Leung KHB, Brooks SC, Clegg GR, et al. Socioeconomically equitable public defibrillator placement using mathematical optimization. Resuscitation. 2021;166:14–20. doi:10.1016/j.resuscitation.2021.07.002
22. Johnson AM, Cunningham CJ, Zégre-Hemsey JK, et al. Out-of-hospital cardiac arrest bystander defibrillator search time and experience with and without directional assistance: a randomized simulation trial in a community setting. Simul Healthc. 2022;17:22–28. doi:10.1097/SIH.0000000000000582
23. Alsofayan YM, Althunayyan SM, Mohamed MA, et al. Out of hospital cardiac arrest: Saudi red crescent experience throughout COVID-19 era. Open Access Emerg Med. 2021;13:431–438. doi:10.2147/OAEM.S334808
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.