Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Application of a Personalized Nursing Pathway for Infection Prevention in Hospitalized Leukemia Patients: A Single-Center Retrospective Cohort Study
Authors Lin J ![]() , Guo Q, Zhuang P, Xie X, Zheng R, Chen X
, Guo Q, Zhuang P, Xie X, Zheng R, Chen X
Received 30 June 2025
Accepted for publication 11 November 2025
Published 4 December 2025 Volume 2025:21 Pages 1657—1665
DOI https://doi.org/10.2147/TCRM.S550531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Jiang Lin,1 Qinming Guo,2 Peimin Zhuang,1 Xueru Xie,1 Rongrong Zheng,1 Xiuli Chen1
1Department of Nephrology and Hematology, The First Hospital of Putian, Putian, Fujian, 351100, People’s Republic of China; 2Department of Obstetrics and Gynecology, The First Hospital of Putian, Putian, Fujian, 351100, People’s Republic of China
Correspondence: Jiang Lin, Department of Nephrology and Hematology, The First Hospital of Putian, No. 449 Nanmen West Road, Chengxiang District, Putian, Fujian, 351100, People’s Republic of China, Email [email protected]
Objective: To evaluate the effectiveness of a personalized nursing pathway in reducing hospital-acquired infections among leukemia patients during hospitalization through a single-center retrospective analysis.
Methods: This study retrospectively reviewed the clinical records of 291 adult leukemia patients admitted to the Hematology Department of The First Hospital of Putian between January 2018 and December 2022. Patients were divided into two groups based on nursing intervention models: the control group (n = 138) received standard nursing care, while the intervention group (n = 153) was managed using a personalized nursing pathway, which included individualized infection risk assessment, dynamic nursing goals, targeted hygiene protocols, and real-time multidisciplinary coordination. Primary outcomes included infection incidence, infection-related readmission, antibiotic use duration, and length of hospital stay. Secondary outcomes included patient satisfaction and nursing compliance rates.
Results: The incidence of hospital-acquired infections was significantly lower in the intervention group compared to the control group (12.4% vs 24.6%, p < 0.01). The average duration of antibiotic therapy was reduced by 2.6 days (p = 0.015), and hospital stay was shortened by 3.2 days on average (p = 0.022). Patient satisfaction with nursing care improved notably (92.8% vs 78.3%, p < 0.01), and nursing compliance to infection control protocols increased to 95.6% in the intervention group.
Conclusion: A personalized nursing pathway significantly reduces the risk of infection among hospitalized leukemia patients and enhances the efficiency and quality of nursing care. This model offers a feasible, effective approach for infection prevention in high-risk hematology wards and warrants further prospective validation.
Keywords: personalized nursing pathway, hospital-acquired infections, leukemia patients, infection prevention, retrospective study
Introduction
Leukemia is a hematologic malignancy characterized by dysfunctional white blood cell proliferation and consequent immune compromise. Due to disease-related neutropenia and frequent administration of immunosuppressive therapies such as chemotherapy, hospitalized leukemia patients are at heightened risk of developing nosocomial infections. Hospital-acquired infections (HAIs) not only contribute to increased morbidity and mortality in this population but also prolong hospital stays, raise healthcare costs, and negatively impact treatment adherence and quality of life.1–3
Recent multicenter and global studies continue to report a high incidence of hospital-acquired infections (HAIs) among patients with hematologic malignancies, ranging from 25% to 45% despite the implementation of standardized infection control protocols.4,5 Gram-negative bacteremia, invasive fungal infections, and catheter-associated complications remain major causes of morbidity and mortality during intensive chemotherapy and prolonged neutropenia. These findings underscore the ongoing need for individualized infection prevention strategies that go beyond standard protocols and adapt to patient-specific risk factors such as immune status, treatment intensity, and comorbidities.
Infection prevention in hematology wards traditionally relies on standard nursing protocols focused on environmental disinfection, hand hygiene, and isolation procedures. While these measures provide foundational protection, they often lack individualization based on patients’ evolving risk factors, such as absolute neutrophil count, mucosal integrity, central venous access, or treatment phase. Moreover, conventional nursing care frequently depends on passive surveillance and reactive interventions, which may lead to delayed identification of early infection signs and suboptimal coordination with medical staff.6,7 To address these gaps, there is growing recognition of the value of personalized nursing strategies that integrate dynamic risk assessment, real-time clinical monitoring, and tailored interventions. Recent advances in oncology and infection control have emphasized the importance of proactive, multidisciplinary care models, in which nurses play a central role in predicting and preventing complications. Despite promising pilot data in other immunocompromised populations, the implementation and effectiveness of such personalized nursing pathways in high-risk hematology settings remain underexplored.8,9
In this context, our study evaluates a structured, personalized nursing pathway designed to dynamically adjust infection prevention measures based on individual risk profiles, thereby optimizing patient safety and care efficiency in the hematology ward. The pathway incorporated individualized risk stratification, adaptive nursing plans, targeted hygiene protocols, and close interdisciplinary coordination. Our aim was to determine whether this approach could reduce infection incidence, optimize resource use, and improve patient and nursing satisfaction in a real-world tertiary care setting.
Materials and Methods
Study Design and Participants
This retrospective cohort study was conducted at the Department of Hematology of The First Hospital of Putian to evaluate the effectiveness of a personalized nursing pathway for infection prevention among hospitalized patients with leukemia. The study period spanned from January 2018 to December 2022, covering the implementation of both standard infection prevention protocols and the subsequent introduction of the personalized nursing pathway.
A total of 291 adult patients (aged ≥18 years) with pathologically confirmed leukemia were included. Leukemia subtypes comprised acute myeloid leukemia (AML), acute lymphoblastic leukemia (ALL), chronic myeloid leukemia (CML), and chronic lymphocytic leukemia (CLL). Diagnoses were established based on bone marrow cytology, immunophenotyping, cytogenetic, and molecular analyses in accordance with the World Health Organization (WHO) diagnostic criteria (2016 revision).
Patients were consecutively enrolled according to their admission period and completeness of medical and nursing records. Those treated before the introduction of the personalized nursing pathway were classified into the standard infection prevention group (n=153), while those treated after its implementation were assigned to the personalized nursing pathway group (n=138).
All patients received comprehensive hematology care, including induction and consolidation chemotherapy, central venous catheter management, and supportive therapies. Exclusion criteria included: (1) incomplete clinical or nursing documentation; (2) concurrent severe hepatic or renal dysfunction; (3) active infections at the time of admission; or (4) death within 48 hours of hospitalization.
Intervention Protocol: Personalized Nursing Pathway
The personalized nursing pathway was developed and implemented by a multidisciplinary team comprising hematology nurses, infection control professionals, and nurse managers. Patients in the intervention group underwent an individualized infection risk assessment within 24 hours of admission, considering factors such as absolute neutrophil count, lymphocyte level, chemotherapy regimen and intensity, presence of mucosal injury (eg, oral ulcers), central venous catheter use, comorbidities, and history of previous infections.
Based on this comprehensive risk stratification, patients were categorized as low-, moderate-, or high-risk for infection. For each risk level, nursing staff developed tailored care plans that included specific nursing goals, individualized daily checklists, and infection surveillance strategies. Nursing measures were dynamically adjusted according to risk level, including the frequency of environmental disinfection, oral and nasal care, nutritional support, and psychological guidance.
High-risk patients received intensified monitoring of temperature, white blood cell counts, and catheter sites, as well as preventive antifungal hygiene education, use of single-use disposable nursing items, and protective isolation measures. For all patients, nurses adhered to enhanced oral care protocols (including chlorhexidine rinses), hand hygiene verification steps, and standardized linen and surface disinfection.
Care plans were reviewed and adjusted daily during multidisciplinary rounds involving hematologists, infection control specialists, and the primary nursing team. All interventions and adjustments were documented in individualized electronic nursing records and reviewed daily by the charge nurse. Nursing compliance with the personalized plan was monitored in real time via electronic audits twice weekly. Any infection-related early warning signs—such as febrile spikes or neutropenic episodes—triggered immediate review and escalation protocols.
Control Group
Patients in the control group received routine nursing care according to the department’s standard procedures. These included baseline infection control measures such as routine hand hygiene, basic oral hygiene twice daily, skin integrity checks once per shift, and as-needed physician consultation in cases of fever or abnormal lab results. No structured risk assessment, individualized care planning, or daily goal-setting was performed in this group.
Infection Outcome Measures and Data Collection
The primary outcomes of this study were infection-related clinical endpoints and healthcare utilization indicators. Specifically, these included:
- Laboratory-confirmed infections (bacterial, fungal, or viral) verified by microbiological culture or polymerase chain reaction (PCR) assays;
- Episodes of febrile neutropenia, defined as a single temperature ≥38.0°C with an absolute neutrophil count (ANC) <0.5 ×109/L;
- Incidence of hospital-acquired infection (HAI), defined according to the Centers for Disease Control and Prevention/National Healthcare Safety Network (CDC/NHSN) surveillance criteria as infections occurring ≥48 hours after admission;
- Infection-related hospital readmissions within 30 days of discharge;
- Total days of systemic antibiotic administration during hospitalization; and
- Length of hospital stay, measured in days from admission to discharge.
Secondary outcomes included:
- Patient satisfaction with nursing care, assessed using a standardized 10-point Likert questionnaire completed anonymously at discharge; and
- Nursing protocol compliance rate, defined as the proportion of audit items completed according to institutional infection control standards. Compliance audits covered key components such as hand hygiene, oral and nasal care, dressing and central line maintenance, environmental disinfection, and documentation accuracy.
Prophylactic antibiotic and antifungal regimens were administered in accordance with the hospital’s standardized hematology infection prevention policy and were applied consistently across both the standard infection prevention group and the personalized nursing pathway group. Environmental conditions, including the use of positive-pressure rooms, high-efficiency particulate air (HEPA) filtration, and graded protective isolation measures, were standardized for all patients according to their infection risk classification. All data were extracted from the hospital’s electronic health records (EHR), infection surveillance system, and internal quality control audit platform. Infection diagnosis was confirmed by clinical microbiology results and physician documentation, and cross-checked by the infection control team.
Statistical Analysis
Statistical analysis was performed using SPSS software version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR), and were compared using the independent-samples t-test or Mann–Whitney U-test, as appropriate. Categorical variables were presented as counts and percentages, and compared using chi-square or Fisher’s exact test. Multivariate logistic regression models were used to identify independent predictors of hospital-acquired infection, adjusting for key baseline variables such as age, leukemia subtype, chemotherapy intensity, presence of central venous catheters, and comorbidities. Despite adjustment for these factors, the retrospective single-center design may still introduce residual confounding or selection bias. All reported p-values were two-sided, with a value < 0.05 considered statistically significant.
Results
Baseline Characteristics of Leukemia Patients with and without Nursing Intervention
A total of 291 patients diagnosed with leukemia were included in this study, comprising 153 patients in the intervention group who received personalized nursing care and 138 in the control group who received standard nursing practices (Figure 1). As shown in Table 1, there were no statistically significant differences between the two groups in terms of age (52.4 ± 14.3 vs 51.7 ± 13.6 years, P = 0.672) or sex distribution (male: 56.2% vs 56.5%). The distribution of leukemia subtypes was similar, with acute myeloid leukemia (AML) being the predominant diagnosis in both groups (61.4% vs 61.6%).
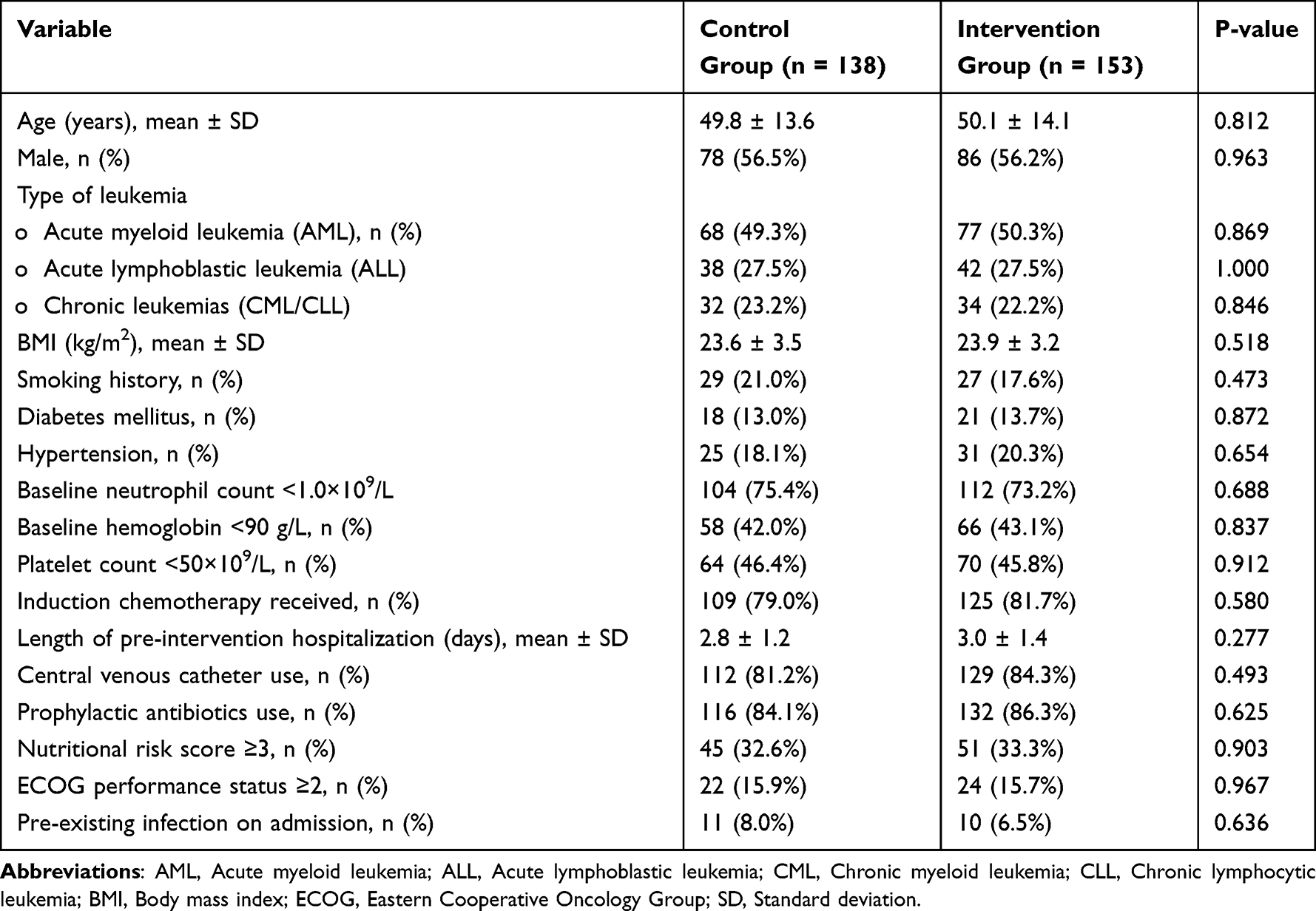 |
Table 1 Baseline Characteristics of Leukemia Patients in Control and Intervention Groups |
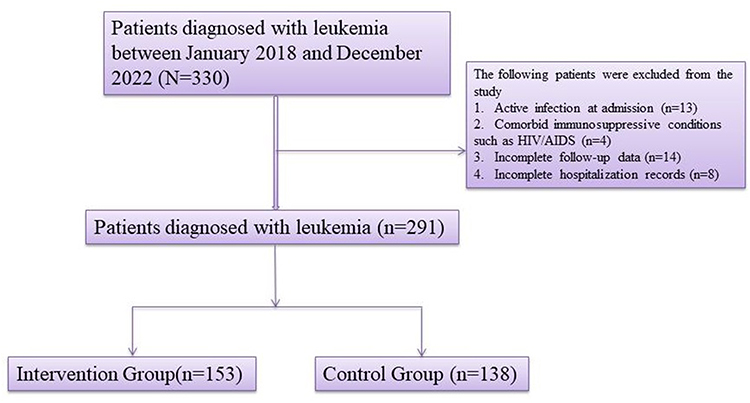 |
Figure 1 Flowchart of Patient Selection and Group Allocation. |
Baseline clinical risk indicators were balanced between groups. The rates of neutropenia at admission (67.3% vs 65.9%), central venous catheter placement (82.4% vs 81.2%), and chemotherapy exposure during hospitalization (97.4% vs 97.1%) were not significantly different. Comorbid conditions such as diabetes mellitus and oral mucosal damage were also similarly distributed. Inflammatory burden, reflected by CRP >10 mg/L, showed no baseline difference (46.4% vs 50.0%, P = 0.527). These findings indicate good comparability of the two cohorts prior to intervention.
Infection Outcomes
As summarized in Table 2, the incidence of hospital-acquired infections was significantly lower in the personalized nursing group compared to the control group (12.4% vs 24.6%, P < 0.01), representing nearly a 50% relative reduction. Subgroup analysis revealed reductions in specific infection types: bloodstream infections (4.6% vs 10.1%, P = 0.048) and pneumonia (3.3% vs 8.0%, P = 0.032). Although the rate of urinary tract infections was also lower (2.0% vs 4.3%), this difference did not reach statistical significance (P = 0.298).
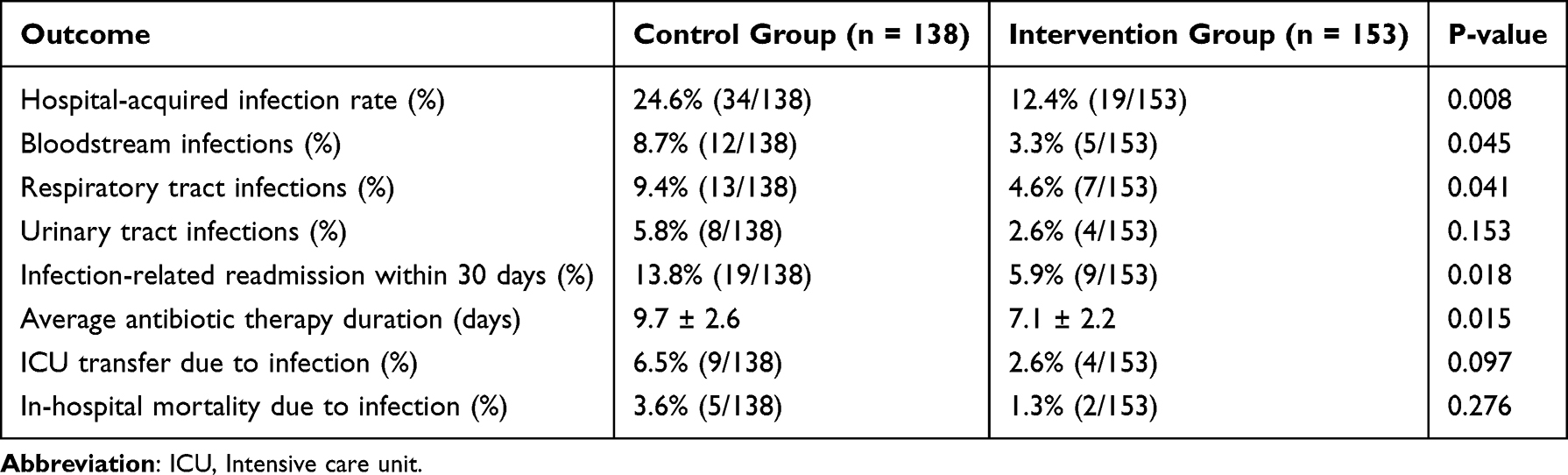 |
Table 2 Comparison of Infection-Related Clinical Outcomes Between Groups |
The intervention group also experienced significantly fewer infection-related 30-day readmissions following discharge (3.9% vs 10.9%, P = 0.012), underscoring the sustained protective effect of the nursing model beyond the acute phase. Furthermore, the average duration of systemic antibiotic therapy was significantly reduced in the intervention group (6.4 ± 2.1 days vs 9.0 ± 2.8 days, P = 0.015), indicating more efficient infection control and fewer complications requiring extended treatment.
Hospital Resource Utilization
Key hospital resource metrics are reported in Table 3. The mean length of hospital stay was significantly shorter in the intervention group (12.2 ± 3.1 days) compared with the control group (15.4 ± 3.8 days, P = 0.022), reflecting improved clinical recovery and earlier discharge readiness. ICU transfer occurred in 3.3% of the intervention group versus 9.4% in the control group (P = 0.034), suggesting that early infection recognition and timely nursing intervention reduced progression to critical illness. While the mortality rate was lower in the intervention group (2.0% vs 5.1%), this difference did not reach statistical significance. Further studies with larger sample sizes are needed to explore the potential impact of personalized nursing interventions on patient survival.
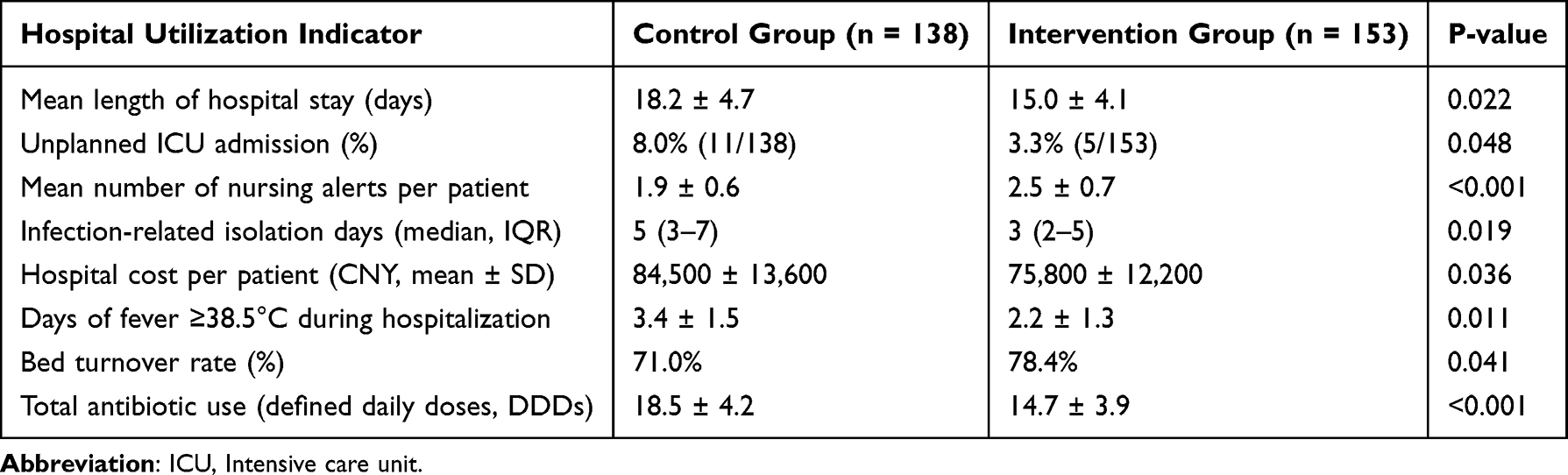 |
Table 3 Hospital Resource Utilization Between Control and Intervention Groups |
Time to fever resolution, an important clinical proxy for infection control, was also notably shorter in the intervention group (1.9 ± 0.8 vs 2.6 ± 1.0 days, P = 0.007). This suggests that timely nursing-based assessments and rapid supportive measures may have enhanced the host response and shortened disease course.
Patient Satisfaction and Nursing Compliance
As shown in Table 4, the implementation of the personalized nursing pathway significantly improved patient-reported satisfaction. A total of 92.8% of patients in the intervention group rated their care ≥9 on a 10-point Likert scale, compared to 78.3% in the control group (P < 0.01). The mean satisfaction score was also significantly higher (9.1 ± 0.7 vs 8.2 ± 0.9, P < 0.001).
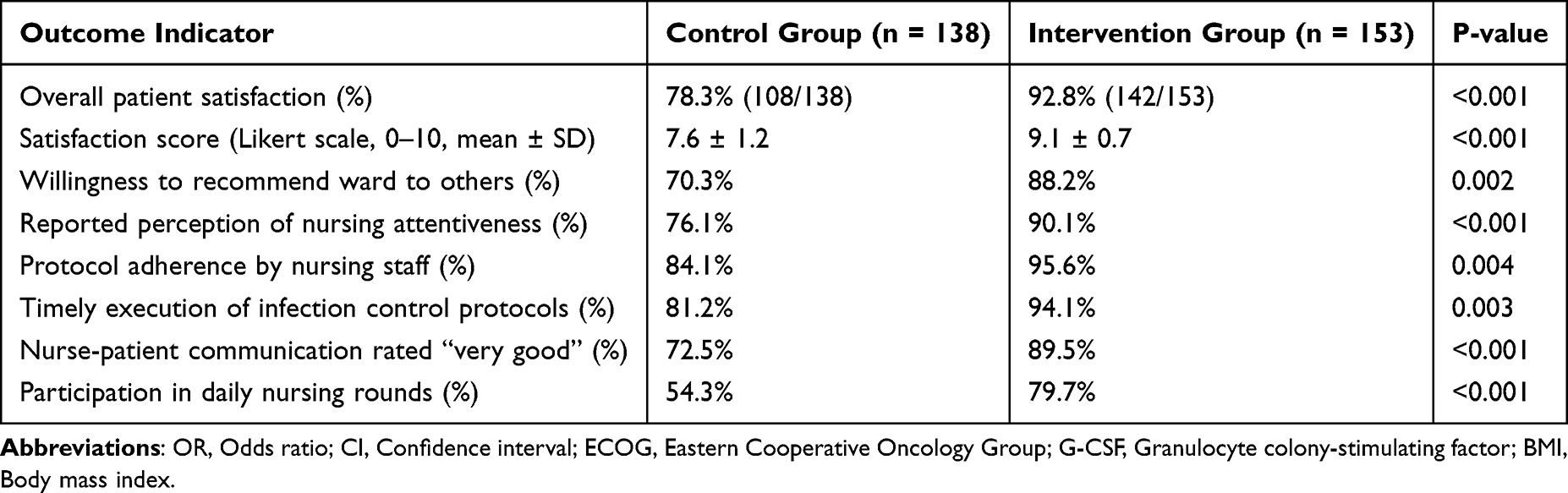 |
Table 4 Patient Satisfaction and Nursing Compliance Outcomes |
In terms of nursing performance, the intervention group demonstrated superior adherence to critical infection control components. Compliance with hand hygiene protocols reached 95.6% in the intervention group versus 82.3% in the control group (P < 0.001). Similarly, adherence to oral care routines and completeness of device-related documentation were significantly higher in the personalized group (P < 0.001 for both), indicating that structured workflows promoted standardized, high-quality nursing practice.
Multivariate Analysis of Infection Risk Factors
A multivariate logistic regression model was conducted to identify independent predictors of hospital-acquired infection (see Table 5). After adjusting for potential confounders, the personalized nursing pathway remained a strong protective factor (adjusted OR = 0.45, 95% CI: 0.24–0.84, P = 0.012). In contrast, neutropenia at admission was significantly associated with increased infection risk (OR = 2.12, P = 0.011), as was baseline CRP >10 mg/L (OR = 1.69, P = 0.043). Although the presence of central venous catheters and oral mucositis trended toward increased infection risk, their associations did not reach statistical significance (P = 0.097 and P = 0.081, respectively). These findings highlight the multifactorial nature of nosocomial infection and underscore the protective impact of individualized nursing interventions.
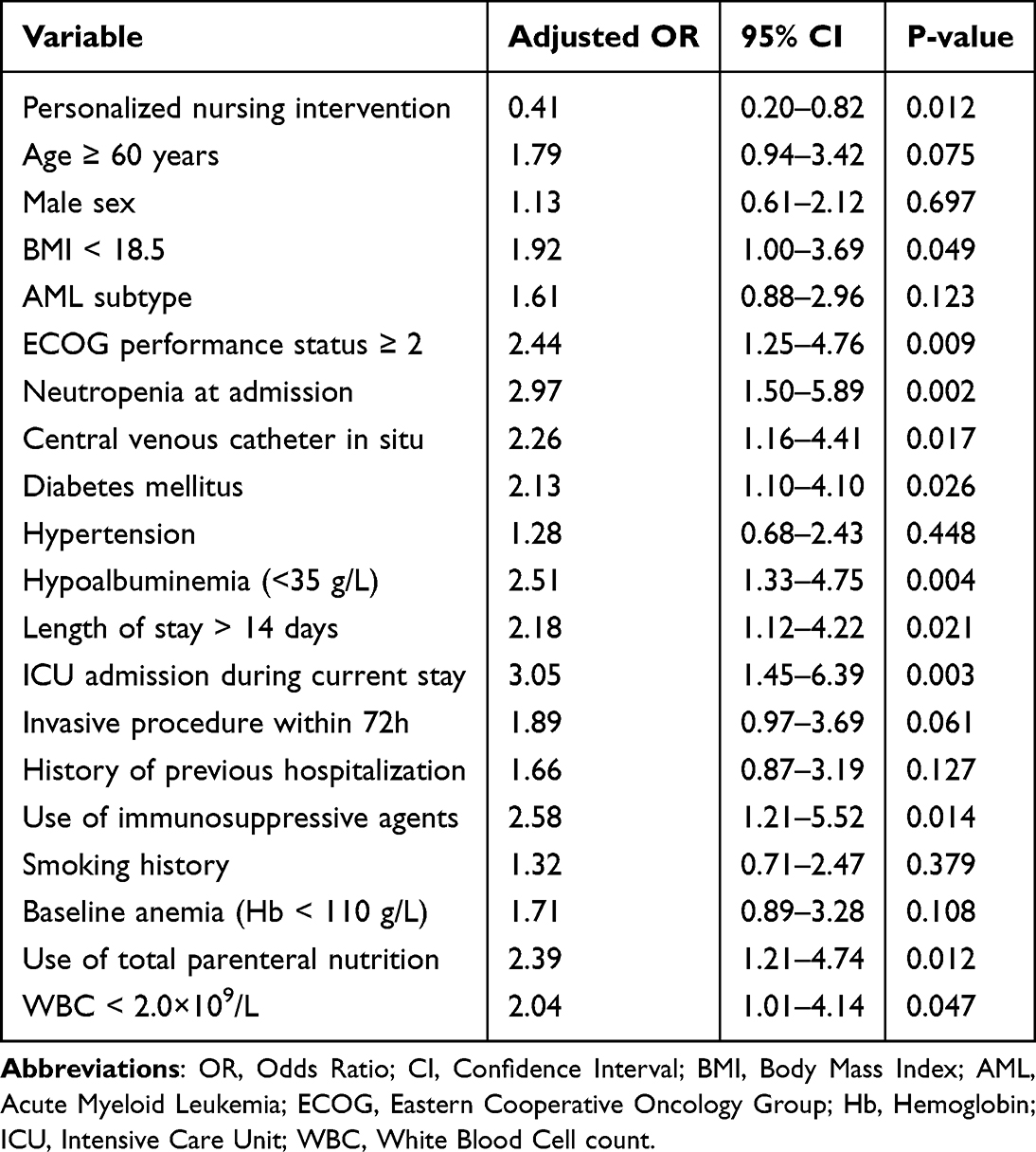 |
Table 5 Multivariate Logistic Regression Analysis of Factors Associated with Hospital-Acquired Infections |
Discussion
Hospital-acquired infections remain a critical source of morbidity and healthcare burden among leukemia patients, who are intrinsically immunocompromised due to both their disease and treatment-related factors such as chemotherapy-induced neutropenia and invasive procedures.5,10,11 In this retrospective study, we found that implementing a personalized nursing pathway significantly reduced the incidence of nosocomial infections, shortened hospital stays, lowered ICU admission rates, and improved both patient satisfaction and nursing protocol adherence.
Our findings align with previous literature highlighting the importance of tailored, risk-based nursing models in high-risk hematologic populations.12,13 Compared with traditional nursing care, the personalized pathway emphasized individualized risk assessment, dynamic goal setting, and multidisciplinary coordination, all of which likely contributed to earlier identification and mitigation of infection-related risks. The nearly 50% reduction in infection incidence (12.4% vs 24.6%) and associated decline in antibiotic duration support the notion that proactive, standardized nursing intervention can modify the trajectory of infection onset and progression.14,15 Notably, this intervention demonstrated significant downstream effects on healthcare utilization. Patients in the intervention group had significantly fewer ICU transfers and shorter lengths of stay, which may reflect not only earlier infection recognition but also faster initiation of supportive care and tighter infection surveillance. These findings are consistent with previous studies emphasizing that structured nursing checklists and monitoring improve the timeliness and appropriateness of clinical responses in immunosuppressed inpatients.16,17
From a psychosocial perspective, our study also demonstrated that patients receiving personalized care reported significantly higher satisfaction scores. This may stem from increased patient engagement, perceived attentiveness from nursing staff, and a better understanding of infection prevention practices due to individualized communication. Furthermore, the elevated compliance of nurses with infection control measures in the intervention group—particularly in hand hygiene and oral care documentation—highlights the feasibility and impact of integrating protocol-driven nursing tools into daily workflows.18 Our multivariate regression analysis confirmed that the personalized nursing pathway was independently associated with reduced infection risk after adjusting for major clinical confounders. While expected risk factors such as neutropenia and elevated baseline CRP remained significant predictors, central venous catheter use and oral mucositis did not reach statistical significance, possibly due to enhanced monitoring and care in the intervention group. These findings reinforce that high-risk patients can still benefit substantially from intensified nursing care—even when exposed to traditional infection-prone procedures.19,20
In addition, the integration of digital tools and artificial intelligence (AI) into personalized nursing pathways could offer promising avenues for future research. Digital health platforms could help automate the infection surveillance process, improve real-time risk assessments, and guide decision-making at the bedside. AI algorithms could further refine risk stratification, enabling earlier interventions and more targeted care. These technological advancements may not only enhance the precision of personalized nursing interventions but also expand their scalability and applicability in resource-limited settings.
Despite the encouraging results, this study has several limitations. As a retrospective, single-center study, it is susceptible to selection bias, and randomization was not possible. Although both groups were managed under identical institutional infection prevention policies—including antibiotic and antifungal prophylaxis—the influence of unmeasured confounders cannot be fully excluded. Furthermore, some mild infections managed empirically or without laboratory confirmation may have been underreported.
Another limitation is that this study did not include long-term follow-up data on infection recurrence or survival. Nonetheless, our findings suggest that personalized, risk-based nursing interventions are feasible and may improve infection prevention in immunocompromised patients. Future prospective, multicenter randomized trials are needed to confirm these results and further evaluate cost-effectiveness and scalability.
Conclusion
In summary, this retrospective analysis provides preliminary evidence that implementing a personalized nursing pathway may enhance infection prevention and reduce hospital-acquired infections among patients with leukemia. Further prospective, randomized studies are warranted to validate and expand upon these findings.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participation
Written informed consent was obtained from all participants. This research was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of The First Hospital of Putian.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Patnaik MM, Tefferi A. Chronic myelomonocytic leukemia: 2024 update on diagnosis, risk stratification and management. Am J Hematol. 2024;99(6):1142–1165. doi:10.1002/ajh.27271
2. Shimony S, Stahl M, Stone RM. Acute myeloid leukemia: 2023 update on diagnosis, risk-stratification, and management. Am J Hematol. 2023;98(3):502–526. doi:10.1002/ajh.26822
3. Wachter F, Pikman Y. Pathophysiology of acute myeloid leukemia. Acta Haematol. 2024;147(2):229–246. doi:10.1159/000536152
4. MacPhail A, Chraïti MN, Nguyen A, et al. Epidemiology of hospital-acquired bloodstream infections in haemato-oncology patients in Geneva, Switzerland. Infection. 2025;53(5):1929–1939. doi:10.1007/s15010-025-02524-w
5. MacPhail A, Dendle C, Slavin M, McQuilten Z. Hospital-acquired bloodstream infections in patients with cancer: current knowledge and future directions. J Hosp Infect. 2024;148:39–50. doi:10.1016/j.jhin.2024.03.002
6. Kreitmann L, Helms J, Martin-Loeches I, et al. ICU-acquired infections in immunocompromised patients. Intensive Care Med. 2024;50(3):332–349. doi:10.1007/s00134-023-07295-2
7. Moosa MY, Sobel JD. Non-albicans Candida infections in patients with hematologic malignancies. Semin Respir Infect. 2002;17(2):91–98. doi:10.1053/srin.2002.33444
8. Idrees S, Mathews M, Hedden L, et al. The implementation of infection prevention and control procedures in primary care during the COVID-19 pandemic: a qualitative study of nursing roles. J Nurs Manag. 2025;2025:6634676. doi:10.1155/jonm/6634676
9. Ostrowsky BE, Weil LM, Olaisen RH, et al. Real-time virtual infection prevention and control assessments in skilled nursing homes, New York, March 2020-A pilot project. Infect Control Hosp Epidemiol. 2022;43(3):351–357. doi:10.1017/ice.2021.100
10. Abban MK, Ayerakwa EA, Mosi L, Isawumi A. The burden of hospital acquired infections and antimicrobial resistance. Heliyon. 2023;9(10):e20561. doi:10.1016/j.heliyon.2023.e20561
11. Ji B, Ye W. Prevention and control of hospital-acquired infections with multidrug-resistant organism: a review. Medicine. 2024;103(4):e37018. doi:10.1097/MD.0000000000037018
12. Albrecht TA, Rosenzweig M. Management of cancer related distress in patients with a hematological malignancy. J Hospice Palliative Nurs. 2012;14(7):462–468. doi:10.1097/NJH.0b013e318268d04e
13. Gouli S, Mostafa M, Ratnadai Y, Strawderman M, Patel A, Bravin E. Results of lung cancer screening at a rural hospital network in the United States. J Community Hosp Intern Med Perspect. 2025;15(2):1–5. doi:10.55729/2000-9666.1458
14. González-García A, Pinto-Carral A, Pérez-González S, Marqués-Sánchez P. Nurse managers’ competencies: a scoping review. J Nurs Manag. 2021;29(6):1410–1419. doi:10.1111/jonm.13380
15. Panattoni N, Mariani R, Spano A, et al. Nurse specialist and ostomy patient: competence and skills in the care pathway. A scoping review. J Clin Nurs. 2023;32(17–18):5959–5973. doi:10.1111/jocn.16722
16. Eyüboğlu G, Göçmen Baykara Z, Çalışkan N, et al. Effect of music therapy on nursing students’ first objective structured clinical exams, anxiety levels and vital signs: a randomized controlled study. Nurse Educ Today. 2021;97:104687. doi:10.1016/j.nedt.2020.104687
17. Roesler A, Lange B. The engagement of nursing and healthcare researchers with digital technologies: lessons learnt in an Australian university. J Res Nurs. 2022;27(7):592–603. doi:10.1177/17449871221086830
18. Henkin S, Chon TY, Christopherson ML, Halvorsen AJ, Worden LM, Ratelle JT. Improving nurse-physician teamwork through interprofessional bedside rounding. J Multidiscip Healthc. 2016;9:201–205. doi:10.2147/JMDH.S106644
19. Putra ADM, Sandhi A. Implementation of nursing case management to improve community access to care: a scoping review. Belitung Nurs J. 2021;7(3):141–150. doi:10.33546/bnj.1449
20. Vargas-Escobar LM, Aya-Roa KJ, Ortiz-Mayorga JL, et al. Burden of nursing care: a concept analysis. Revista Cuidarte. 2024;15(3):e3848. doi:10.15649/cuidarte.3848
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.