Back to Journals » International Medical Case Reports Journal » Volume 14
Appendiceal Agenesis: A Very Rare Intraoperative Diagnosis – A Case Report
Authors Yohannes B ![]() , Abebe K
, Abebe K
Received 2 March 2021
Accepted for publication 20 March 2021
Published 9 April 2021 Volume 2021:14 Pages 233—236
DOI https://doi.org/10.2147/IMCRJ.S309192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Binyam Yohannes, Kirubel Abebe
Department of Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Kirubel Abebe
Department of Surgery, St. Paul’s Hospital Millennium Medical College, P.O. Box 1271, Addis Ababa, Ethiopia
Tel +251 921143772
Email [email protected]
Background: Appendiceal agenesis is a rare intraoperative diagnosis which occurs in 0.001% of laparotomies done for presumed acute appendicitis. To our knowledge, this is the first report of appendiceal agenesis in our country and the second in Africa.
Case Presentation: A 19 year old Ethiopian female student came with clinical and imaging findings of acute appendicitis. No history of previous abdominal surgery and similar illness. The vermiform appendix could not be identified following laparotomy performed for the assumption of acute appendicitis. The surgical exploration also revealed no cause for the abdominal pain. Then appendiceal agenesis was declared with an additional diagnosis of nonspecific abdominal pain (NSAD). The postoperative follow-up was uneventful.
Conclusion: Appendiceal agenesis is a rare malformation which demands a careful examination and meticulous laparotomic/laparoscopic exploration for diagnosis.
Keywords: appendiceal agenesis, appendiceal anomalies, acute appendicitis, Ethiopia
Introduction
Appendiceal agenesis is a developmental arrest resulting in total absence of the vermiform appendix.1 Morgagni, in 1719, reported the first case of appendiceal agenesis.2 It is a very rare congenital anomaly which occur in 0.001% of laparotomies done for the assumption of acute appendicitis.1,3–9 Diagnosis of this rare condition is made intraoperatively after a thorough laparotomic or laparoscopic exploration.8,10
Acute appendicitis is the commonest reason for emergency surgery and diagnosis is predominately based on clinical examination. The diagnosis can be challenging if the presentation is atypical and this may result in treatment delay.4,11,12
In this paper, we present a young female patient who came to our hospital with a clinical and sonographic features of acute appendicitis. However, the laparotomic exploration revealed an absent vermiform appendix and no cause for the abdominal pain.
To the best of our knowledge, this is the first report of appendiceal agenesis in our country and the second in Africa following a report by SN Anyanwu in 1994.13
Case Presentation
A 19-years-old female Ethiopian student came with a one-day history of colicky abdominal pain which was initially periumbilical later shifted to the right lower quadrant. The pain was associated with anorexia, nausea and two episodes of non-bilious vomiting. She had no fever, no bowel or urinary compliant. Her menstrual cycle was regular with the last one being 7 days ago. She had no history of similar illness, no previous abdominal surgery or trauma. She also stated the absence of chronic medical diseases.
On examination, her vital signs were within the normal range. No abdominal surgical scar. Tenderness was appreciated over the right lower quadrant and psoas sign was positive.
The Laboratory blood test showed a normal level of white blood cells (10,000/µL with 60% neutrophil). Urinary analysis was non revealing and negative for HCG. Since the Alvarado score was 6, abdominopelvic ultrasound (US) was done and reported evidences of acute appendicitis (increased diameter of the appendix and periappendiceal fluid).
With a presumptive diagnosis of acute appendicitis, the patient was prepared and the peritoneal cavity was entered through Lanz incision. The appendix was looked at the usual location but could not be identified. A thorough search was made after the cecum was delivered to the wound, the taenia coli were followed to the site where they coalesce (Figure 1). The incision was further extended and the cecum and proximal part of the ascending colon were mobilized. Careful and meticulous exploration in the ileo- and retrocecal regions, sub hepatic space, right retro peritoneum, sub serosa of the cecum and ascending colon was made.
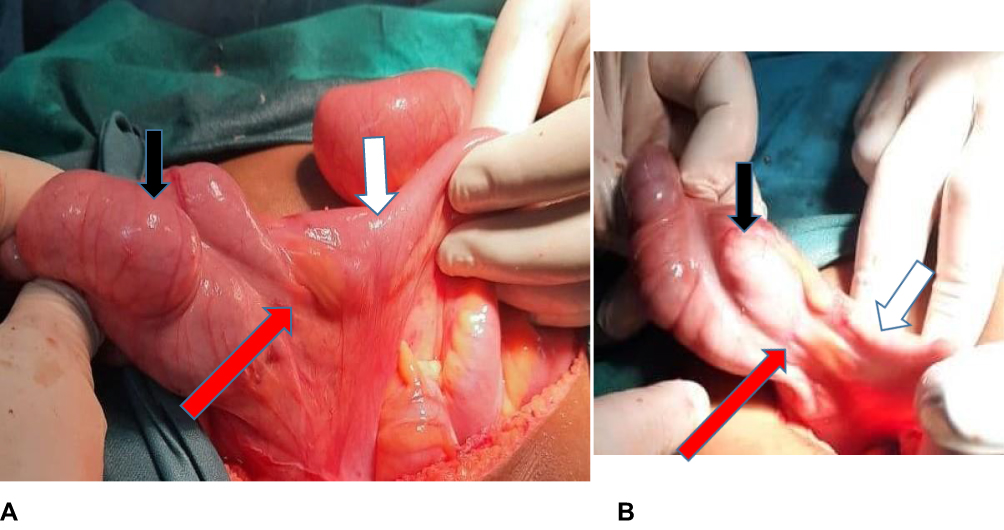 |
Figure 1 An intraoperative view of the ileocecal and retrocecal regions (A and B) showing the cecum (dark arrow), the distal ileum (white arrow) and the site where the taenia coli converge (red arrow) with absent appendix. |
The abdomen was also explored for other possible abdominal conditions like mesenteric lymphadenopathy, Meckel’s diverticulum but none could be found. Furthermore, the fallopian tubes and ovaries were examined and found to be grossly normal. Finally, appendiceal agenesis was declared with the additional diagnosis of nonspecific abdominal pain (NSAP).
Postoperatively, the patient started on antibiotics and analgesics. She was discharged on the 4th postoperative day after an uneventful course. The patient was followed for three months and no complications or recurrence of the pain was noted. Abdominopelvic ultrasound was unremarkable at the last visit.
Discussion
At the 8th week of fetal development, the appendix appears as a diverticulum at the distal end of the embryonic cecum. It develops more slowly than the growth of the remaining cecum and becomes an elongated tubular structure with a blind end. A fully developed appendix is visible at 10 weeks of gestational age.3,5,6,8,9 The base of the appendix has a constant position located 2–5 cm below the ileocecal valve on the posteromedial aspect of the cecum at the junction of the three taenia. Therefore, the appendix can be traced following this land mark, taenia coli. Unlike the base, the position of the appendicular tip varies. Most Authors reported retrocecal as the commonest position.3–5,9
Various forms of appendiceal anomalies could occur if the developmental event is interrupted. In general, Anomalies of the vermiform appendix are very rare and have a wide range of manifestations such as agenesis, atresia, duplication, and the so-called giant appendix. The most common forms are agenesis and duplication which has 0.004% of incidence.1,6–8
In 1719, Morgagni described the first case of appendiceal agenesis.2 This rare anomaly occurs one in 100,000 laparotomies performed for suspected appendicitis.1,4,6–9 Appendiceal agenesis can be isolated or part of cecoappendiceal malformation. Collins addressed this issue and classified it as Type I – absence of appendix and cecum; Type II – rudimentary cecum and absence of appendix; Type III – normal cecum and absence of appendix; Type IV – normal cecum and rudimentary appendix; Type V – giant cecum and absence of appendix.14 Even if authors reported type II as the commonest form, our case and a review done by Vieira et al found Type III malformation.4,15 Intestinal malformations, dextrocardia, hexadactylism and congenital cataract are also mentioned as associated conditions, which are absent in our patient.4,5,8
The etiology of the appendicular agenesis is not well known, however, it is presumed to be a result of intrauterine vascular accident.3–5,9 Furthermore, intrauterine Thalidomide exposure is also reported as a cause of this rare anomaly.6,8 Autoamputation of the appendix due to appendiceal torsion, intrabdominal infection and removal in previous surgery should be ruled out and carefully investigated before declaring agenesis.5,10 We did not detect any of these conditions in the current case.
Preoperative diagnosis of appendiceal agenesis is difficult and inaccurate due to lack of specific symptoms, serum markers and physical findings. Preoperative imaging such as abdominal CT scan may be considered and helpful in some patients.5,9 Laparotomic or laparoscopic exploration should be done for accurate diagnosis of appendiceal agenesis. If a surgeon fails to detect the appendix, the first step should be to follow the taenia coli till the convergence. If this does not help, the cecum and the ascending colon should be mobilized to explore the entire ileocecal and retrocecal areas. If these maneuvers still could not identify the appendix, cecum should be palpated carefully to exclude appendiceal invagination or intussusception.1,5,9 In our patient, we performed all the intraoperative maneuvers and steps to declare the diagnosis of appendiceal agenesis.
As it is well known, acute appendicitis is the commonest reason for emergency surgery and diagnosis predominately relay on clinical examination. The diagnosis can be challenging if the presentation is atypical and this may result in treatment delay.4,11,12 Alvarado score is the most widely used scoring system in the clinical diagnosis of this condition. A systematic review done by Ohle et al reported Alvarado score as an accurate diagnostic “rule out” score at a cut point 5 for all patients.16 For a score of 7 or greater surgery is indicated. There will be a diagnostic dilemma, if the score is equivocal 5 to 6. This may warrant the use of imaging such as an abdominal ultrasound or contrast CT.12,16 In the current case, abdominal ultrasound was done provided that the Alvarado score is 6 and to rule out gynecologic emergencies.
Despite the advance of modern investigative modalities, the world wide mean negative appendectomy rate may reach up to 25%.3,11,12 Ultrasound has sensitivity and specificity of 75% to 90% and 86% to95% respectively.11 In the discussed case, US reported features of acute appendicitis like increased appendiceal diameter and periappendiceal fluid. However, laparotomy confirmed appendiceal agenesis. This could be explained by the fact that ultrasound is operator dependent and in our case it was done by a medical radiology technologist (not a radiologist). In Ethiopia, such professions are trained and assigned in hospitals to overcome the low number of radiologists.
Nonspecific abdominal pain (NSAP) is an acute abdominal pain less than 7 days and the cause is not known despite examination and baseline investigation. Literature reported NSAP as the commonest cause of emergency surgical admission with observed incidence of 13% to 40%. Our patient clinical examination and laparotomic exploration revealed no identifiable cause for the abdominal pain.3,17
Conclusion
Appendiceal agenesis is a very rare condition and diagnosis is made after thorough clinical and laparotomic/laparoscopic exploration. Extensive and Meticulous surgical exploration of the ileocecal and retrocecal regions is mandatory before declaring this rare anomaly. Surgeons should keep in mind that appendiceal agenesis could be found in patients presenting with the sign and symptoms suggestive of acute appendicitis.
Ethics and Consent
Written informed consent was provided by the patient to use the information and accompanying images for publication. Ethical approval from the institutional review board is not required given it is a case report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Nissler V, Fleischmann J, Hümmer HP, Knorr C. Agenesis of the vermiform appendix. J Pediatr Surg. 2012;47(6):1302–1303. doi:10.1016/j.jpedsurg.2012.03.050
2. Morgagni GB. Adversaria anatomica all things (1-V1) of which the latter three are now for the first time will be betrayed. Patavic J Cominus. 1719;3:64.
3. Shah TA. A 25-year-old male with appendicular agenesis: a case report and literature review. J Taibah Univ Med Sci. 2017;12(1):75–77. doi:10.1016/j.jtumed.2016.02.003
4. Vieira ED, Bonato LM, Silva GG, Gurgel JL. Congenital abnormalities and anatomical variations of the vermiform appendix and mesoappendix. J Coloproctol. 2019;39(3):279–287. doi:10.1016/j.jcol.2019.04.003
5. Gok M, Sozuer E, Topal U, et al. A rare developmental anomaly associated with right colon cancer: appendix vermiformis agenesis. Ann Ital Chir. 2020;9:S2239253X2003090X.
6. Beger B, Kızılyıldız BS. Ileocecal stenosis with agenesis of vermiform appendix: a rare cause of congenital bowel obstruction. J Anat Soc India. 2018;67:S48–S50. doi:10.1016/j.jasi.2018.09.002
7. Vincent MV, Doyle A, Bernstein S, Jackman S. Absence of the appendix discovered during childhood. Springerplus. 2014;3(1):1–4. doi:10.1186/2193-1801-3-522
8. Martínez DG, Sánchez AW, Rivera FV, Romano RC, Torreblanca CB. Appendicular agenesis. Acta Médica Grupo Ángeles. 2010;8(3):167–171.
9. Tripathy BB. Congenital absence of appendix: a Surgeon’s dilemma during surgery for acute appendicitis. J Indian Assoc Pediatr Surg. 2016;21(4):199. doi:10.4103/0971-9261.186555
10. Maitra TK, Roy S, Mondal SK, Mahjabin S. Absent appendix. Bangladesh Crit Care J. 2013;1(2):109–110. doi:10.3329/bccj.v1i2.17207
11. Petroianu A. Diagnosis of acute appendicitis. Int J Surg. 2012;10(3):115–119. doi:10.1016/j.ijsu.2012.02.006
12. Chandrasekaran TV, Johnson N. Acute appendicitis. Surgery. 2014;32(8):413–417. doi:10.1016/j.mpsur.2014.06.004
13. Anyanwu SN. Agenesis of the appendix–case report. West Afr J Med. 1994;13(1):66.
14. Collins DC. Agenesis of the vermiform appendix. Am J Surg. 1951;82(6):689–696. doi:10.1016/0002-9610(51)90391-1
15. Arsenio TD, Brito CH, Perez LA, Andrade LA, Ramos JA. A very rare association: acute apendagitis and appendicular agenesis, case report. MOJ Clin Med Case Rep. 2016;4(4):00095.
16. Ohle R, O’Reilly F, O’Brien KK, Fahey T, Dimitrov BD. The Alvarado score for predicting acute appendicitis: a systematic review. BMC Med. 2011;9(1):1–3. doi:10.1186/1741-7015-9-139
17. Morino M, Pellegrino L, Castagna E, Farinella E, Mao P. Acute nonspecific abdominal pain: a randomized, controlled trial comparing early laparoscopy versus clinical observation. Ann Surg. 2006;244(6):881. doi:10.1097/01.sla.0000246886.80424.ad
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.