Back to Archived Journals » Reports in Medical Imaging » Volume 15
Aortic Knob Diameter in Chest Radiographs of Healthy Adults in Uganda
Authors Magera S, Sereke SG ![]() , Okello E, Ameda F, Erem G
, Okello E, Ameda F, Erem G
Received 11 January 2022
Accepted for publication 12 March 2022
Published 24 March 2022 Volume 2022:15 Pages 21—29
DOI https://doi.org/10.2147/RMI.S356443
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tarik Massoud
Steven Magera,1 Senai Goitom Sereke,1 Emmy Okello,2 Faith Ameda,1 Geoffrey Erem1
1Department of Radiology and Radiotherapy, College of Health Sciences, Makerere University, Kampala, Uganda; 2Department of Cardiology, Uganda Heart Institute, Kampala, Uganda
Correspondence: Steven Magera; Senai Goitom Sereke, Email [email protected]; [email protected]
Background: The burden of cardiovascular diseases, such as aortic and degenerative diseases, grows in the aging population. Chest radiograph still plays an important role in the diagnosis of cardiovascular diseases. Aortic knob diameter in chest radiographs can be used to evaluate early changes of the aortic structure and together with clinical and laboratory findings. This study was aimed at determining the mean values of aortic knob diameter among healthy adults in Uganda.
Methods: We conducted a descriptive cross-sectional study in three selected hospitals in Kampala Uganda. All participants had normal chest radiographs without radiological evidence of cardiovascular disease. Chest radiograph findings extracted included aortic knob diameter, aortic arch diameter, transverse heart diameter, and transverse thoracic diameter. All films were independently examined by two experienced radiologists.
Results: We analyzed chest radiograph findings of 294 participants, of which 204 (69.4%) were male. Aortic knob diameter increased with age (p – 0.000). The mean aortic knob diameter of males was higher than for females (3.14± 0.34cm versus 2.77± 0.37cm, p – 0.000). The mean aortic knob diameter on the digital screen was higher than plain films (3.03± 0.393cm versus 2.96± 0.392cm, p – 0.000). Aortic knob diameter positively correlated with age (p – 0.000) and aortic arch diameter (p – 0.000). Aortic knob diameter also correlated positively with a transverse thoracic diameter (p – 0.05), transverse heart diameter (p – 0.05), and cardiothoracic ratios (p – 0.05).
Conclusion: The aortic knob diameter was higher in males and there was a positive correlation with age, aortic arch diameter, transverse heart diameter, and transverse thoracic diameter. Aortic knob diameter measurements should be done on digital rather than printed x-ray films.
Keywords: aortic knob, diameter, chest radiograph, cardiovascular, Uganda
Background
Cardiovascular disease accounts for three-quarters of all global estimated deaths in low- and middle-income countries.1 Chest radiograph remains an important tool for the investigation of cardiovascular conditions despite the advent of newer and more sophisticated imaging modalities such as echocardiography, computerized tomography (CT), and magnetic resonance imaging (MRI) in the world.2 This is mainly due to the more readily available and comparatively cheaper costs of performing a chest radiograph and still provides valuable clues to the diagnosis of cardiovascular pathology.3 Moreover, the reproducibility of aortic and heart measurements on chest radiographs has been described in the literature.4,5
The aorta is a major vascular supply of the human body and plays an important role in controlling systemic vascular resistance and heart rate. This control is done via pressure-responsive receptors located in the ascending aorta and aortic arch.6 An increase and decrease in aortic pressure results in a decrease in heart rate and systemic vascular resistance and an increase in heart rate and systemic vascular resistance, respectively.7
The Aortic knob is an important structure that refers to the hump-shaped contour of the aorta seen in a frontal chest radiograph on the left mediastinal silhouette.8 Abnormal aortic knuckle shape, enlargement, and aortic nipple may give cardiovascular disease the first clue.9 The aortic knob can be enlarged due to increased pressure or flow in the aorta, increased volume, or changes in the elasticity of its wall. In adults, aortic knob enlargement can be seen in systemic hypertension, valvular insufficiency, aortic dissection, traumatic aortic injury, thoracic aortic aneurysm, and atherosclerosis.10
Aortic knob diameter (AKD) is a good predictor of target organ damage with a sensitivity ranging between 70% to 90% for hypertension-related cardiovascular conditions, even in early disease.11 These include hypertensive heart disease, subclinical atherosclerosis, aneurysms, and aortic dissection.12 Moreover, aortic knob width is positively correlated with both systolic and diastolic blood pressures.12–14
Uganda is a low-income country and yet is experiencing a shift in major causes of death with coronary artery disease and other forms of heart failure on the rise.15 And the normal AKD in the literature was taken from studies done among Caucasians,16 Americans,12 South Koreans, Indians, and West Africans. These studies showed that variations exist amongst different populations, age groups, and between sexes.17 In the current practice, more advanced imaging modalities are recommended to measure the AKD,18 however, this is not always feasible in low-income settings like Uganda due to the availability of the modalities and cost-effectiveness. In this study, therefore, we sought to determine the normal AKD amongst healthy adults in Uganda.
Methods
Study Design and Setting
This was a descriptive cross-sectional study conducted in three selected tertiary hospitals in Kampala, Uganda from January 2020 to June 2020. Hospital A is a private tertiary referral hospital with a capacity of 361 beds and approximately 450 chest radiographs were performed per month. Hospital B is also a tertiary public hospital where chest radiographs were performed as part of ongoing recruitment in government agencies like police, the army, and local governments. Hospital C is a private, tertiary hospital and around 100 chest radiographs were performed per month.
Study Population
Study participants included asymptomatic participants referred for chest radiograph examination for pre-employment and pre-travel medical check-ups and were recruited in this study. Participants with a normal chest radiograph (Posterior anterior view, erect), and age between 18–90 years, with no thoracic skeletal deformity, no known cardiovascular disease, and normal blood pressure for age (blood pressure chart) were included in the study. Participants whose chest radiographs had significant rotation (>0.5cm) or artifacts were excluded from the study.
Sample Size
A sample size of 294 participants was used using the formula proposed by Rosner B. 201519 as summarized below.
N = (Zα/2+Zβ)2 *2*σ2/d2
Where N = sample size required. Zα/2 =is the critical value of the Normal distribution at α/2 (eg for a confidence level of 95%, α is 0.05 and the critical value is 1.96), Zβ =is the critical value of the Normal distribution at β (eg for a power of 80%, β is 0.2 and the critical value is 0.84), σ2= is the population variance, d = desired level of precision/marginal error.1 Based on a cross-sectional study done by Ray et al 2014 in the Indian population20 where the mean and standard deviation of the aortic diameter was 3.04±4.1 among the male and female population, population variance was taken as 4.1.
N = (1.96+0.84)2 *2*(4.1)2/(1)2. N=264. Non-response of 10% was 30. Hence the sample size was 294.
Study Procedure
Study participants who gave their consent were physically examined and enrolled in the study. A total of 294 participants’ posteroanterior (PA) chest radiographs were obtained. The PA chest radiograph of all the candidates was taken in the erect position with a film focus distance of 1.8m. The exposures were made at normal arrested inspiration. Participants’ names, sex, age, height, and medical history were recorded. A normal chest radiograph was confirmed by two independent radiologists. Parameters such as AKD, transverse thoracic diameter (TTD), and transverse heart diameter (THD) were evaluated for each patient (Figure 1). The AKD was measured as the maximum transverse diameter from the lateral border of the air in the trachea to the lateral border of the aortic knob.16 The measurements were done on both the printed films and screens independently for all study participants. The Aortic arch diameter (AAD) was measured as the most lateral extension to the right and left of the midline at the level of the aortic knob. TTD was measured as the maximum horizontal distance between the internal margins of the chest wall at the level of the right hemidiaphragm.21,22 THD was measured as the sum of the maximum projection to the right and left heart borders from the midline.21,22 The measurements were done using a standard metric ruler of 30 cm long for the measurements that were taken from printed films and a DICOM viewer inbuilt measurement ruler for the measurements that were taken from screens.
 |
Figure 1 Chest x-ray measurements, aortic knob diameter denoted AKD, aortic arch diameter denoted by AAD, transverse heart diameter denoted by THD (summation of the upper and the lower measurements), and transverse thoracic diameter denoted by TTD. |
Data Analysis
A structured data collection tool was used to collect bio-demographics and relevant history (Appendix 1). Data were analyzed using STATA version 16. Descriptive statistics for continuous variables were presented as mean and standard deviation. Spear man rank correlation was used to test for the correlation between the aortic diameter measurements with continuous independent variables. In addition, a Student’s t-test was performed to test for the mean difference of AKD between groups. A p < 0.05 was considered statistically significant.
Results
A total of 294 participants, of whom 204 (69.4%) were male and the age range between 18–89 years were recruited in the study. Overall, 196 (66.7%) participants were attending the hospital for a pre-employment medical exam, 92 (31.3%) came for annual medical checkup exams, and 6 (2%) pre-travel exams. The mean age of the participants was 35.3±10.5. Sex distribution in the different age ranges is shown in Table 1.
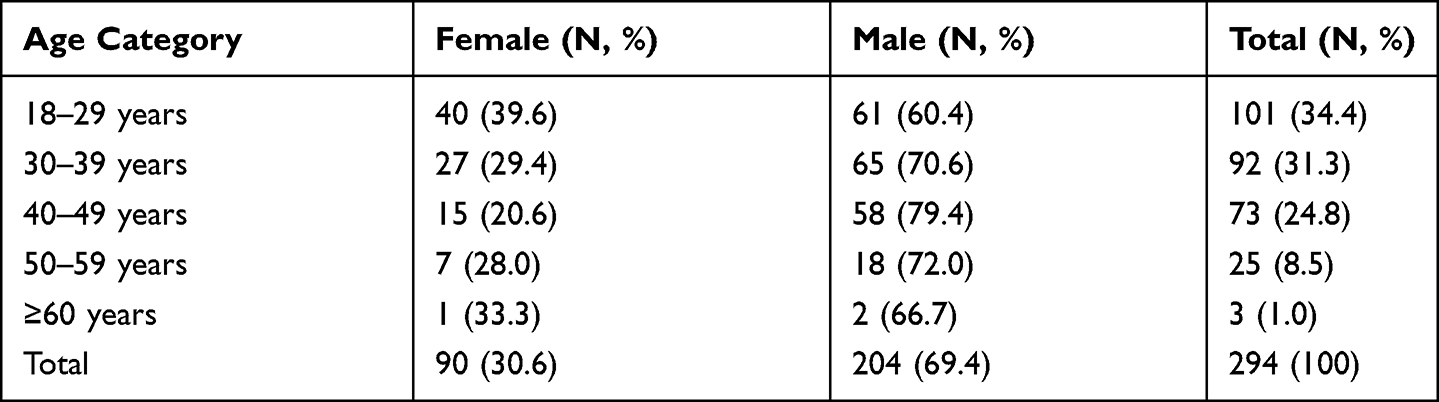 |
Table 1 Age Distribution of the Participants |
Male participants had significantly higher mean AKD compared to their female counterparts (3.14±0.34 cm versus 2.77±0.37cm, p - 0.000). Those in the age group of 50–59 years had significantly higher means than younger people in the age group of 18–29 years (Table 2). Females aged 18–29 years have lower mean AKD compared to men in the same age groups. Overall, male patients had higher AKD when compared with females of all age categories (Figure 2).
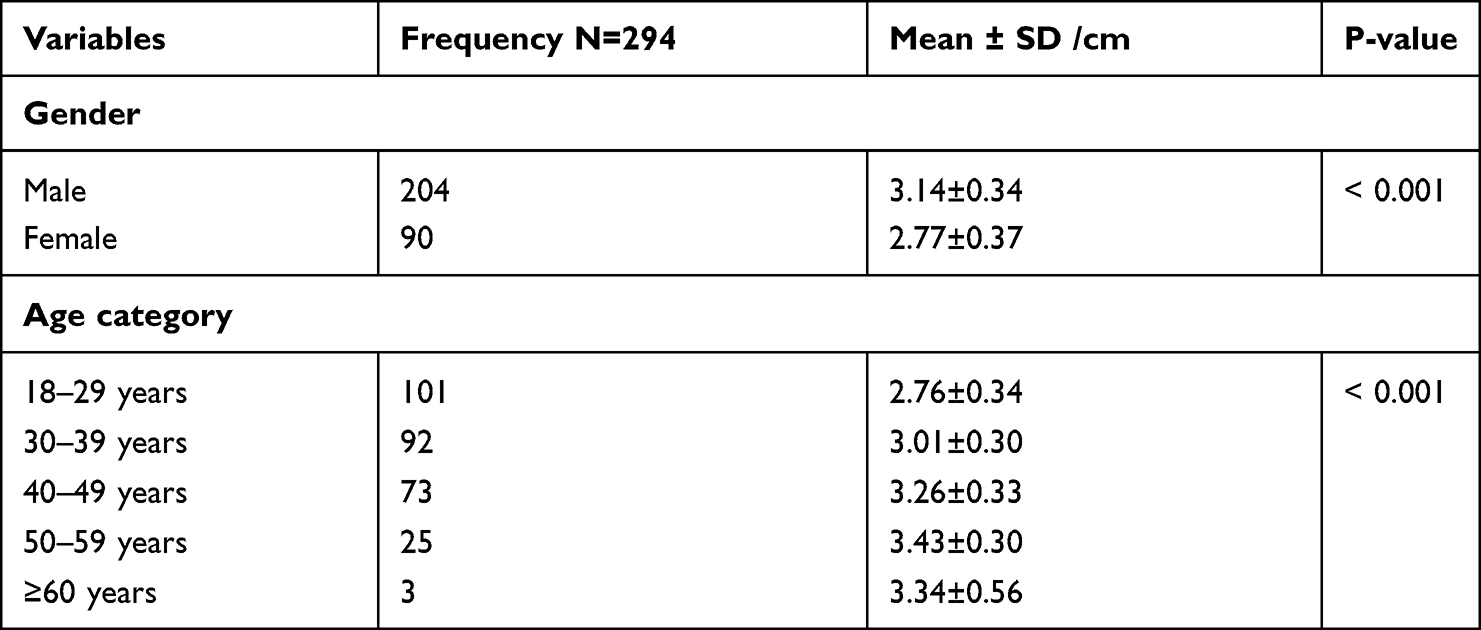 |
Table 2 The Mean Aortic Knob Diameter of 294 Participants |
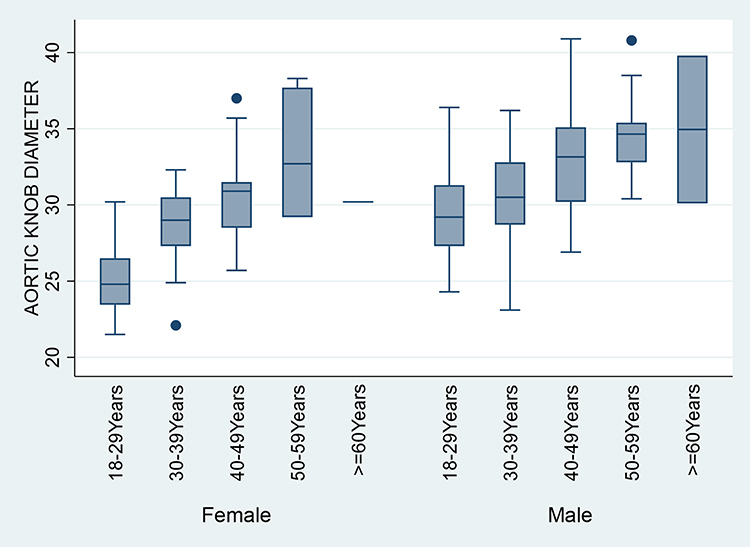 |
Figure 2 Box and whisker plot showing participants’ age-group and gender-specific aortic knob diameters. |
Multivariate regression analysis among different age groups demonstrated increased AKD in older participants compared to the younger participant (p- <0.001). Moreover, males had larger AKD than their female counterparts (p<0.001). But no difference among the different hospitals was seen (Table 3).
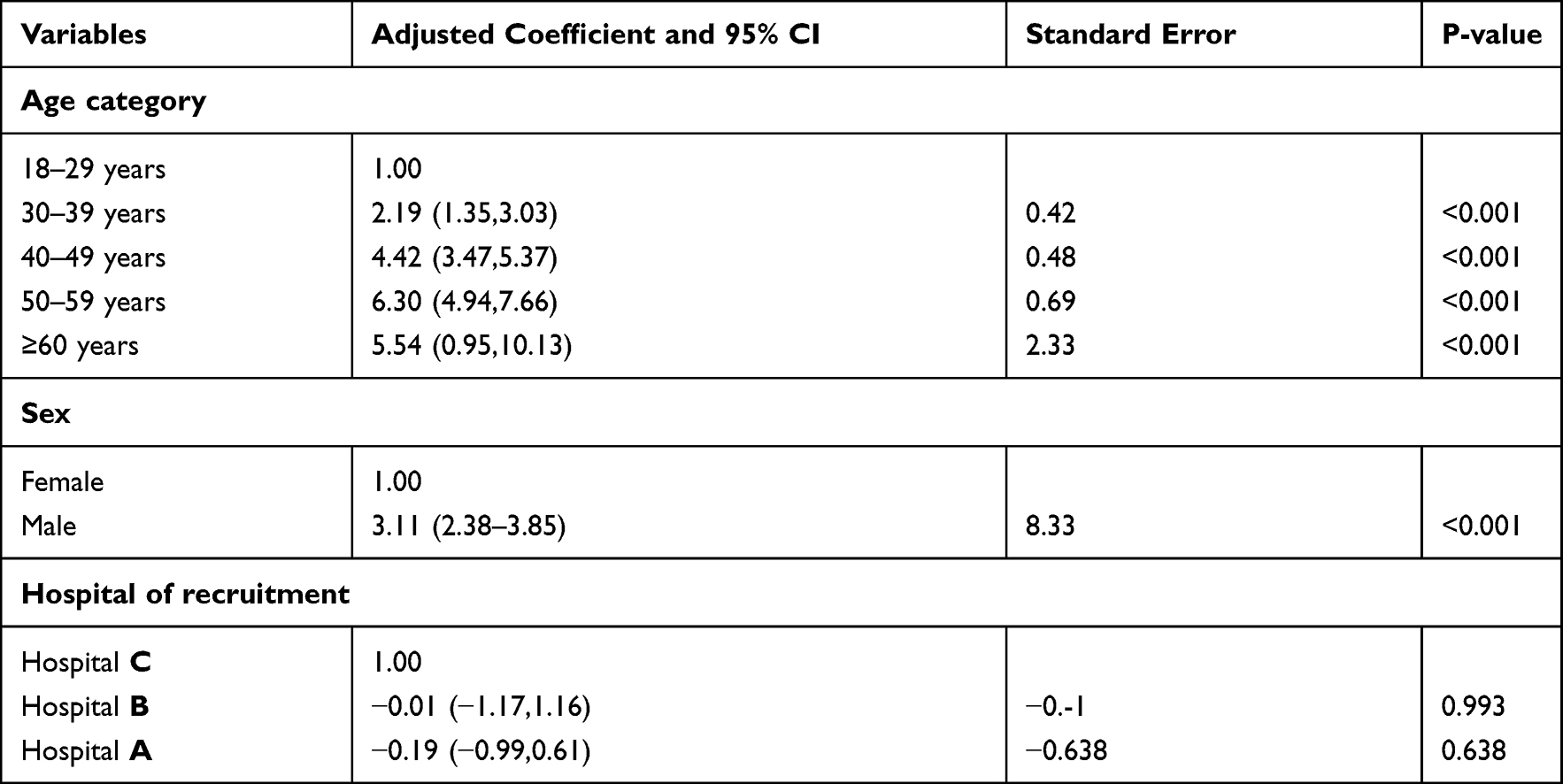 |
Table 3 Multivariate Regression Analysis for the Association Between the Aortic Knob Diameters and Other Parameters |
The average AKD of the sample population was 3.03±0.39cm, the smallest was 2.2cm and the largest was 4.1 cm. The mean AAD of the study population was 5.63±0.64cm and the average cardiothoracic ratio is 0.446±0.037 with the highest being 0.522cm and the lowest 0.366cm (Table 4).
 |
Table 4 Other Cardiovascular Parameters on Chest X-Ray for 294 Participants |
Weight and height were weakly correlated though positively associated with the aortic knob diameter across both genders. However, it was all higher among the female counterpart and the relationships were not statistically significant at a 95% confidence level (Table 5).
 |
Table 5 Correlation of the Aortic Knob Diameter with Aortic Arch Diameter, the Transverse Diameter of the Chest, and Heart Diameter for Male and Female Population (Spearman Correlation and Pearson’s Correlation) |
AKD was strongly and more positively correlated with age among the females than in males, the coefficient was higher among the females and the relationship was statistically significant at 95% confidence level r=0.7411 p-value <0.001 for females vs r=0.5191 p-value <0.001 for males. A strong positive correlation was also observed between the AKD and AAD for both males and females. However, AKD was weakly correlated with THD, TTD, and cardiothoracic ratio respectively (Table 5).
The mean AKD was higher when the measurement was done on a digital screen than on the chest radiograph film (3.03±0.393 cm versus 2.96±0.392cm, p - 0.000). However, the males still had significantly higher AKD compared to females and a unit increase in age would also increase the AKD (Table 6).
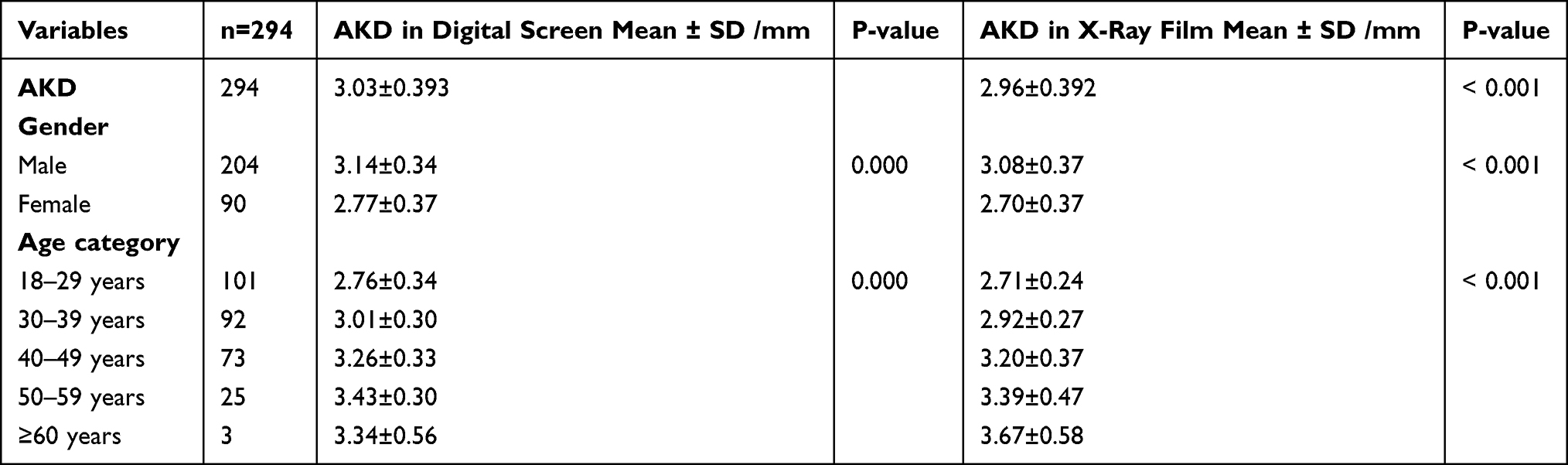 |
Table 6 The Aortic Knob Diameter Measurement on Digital Screen and X-Ray by Gender and Age Groups of 294 Participants |
Discussion
The best way to measure aortic knob diameter is using cross-sectional imaging.18 However, the easy accessibility and comparatively cheaper cost of acquiring chest radiography and higher cost, and lack of easy access to cross-sectional imaging in our setting make it harder to use the latter. Therefore, this study sought to determine the aortic knob diameter in chest radiographs of healthy adults in Uganda. The results of our study showed that AKD increases with age in both sexes. This can be explained by geometric and functional alterations seen with aging.23,24 Studies in India, Nigeria, Zambia, the United States, and South Korea also showed similar results.12,13,20,25,26
AKD was higher in males than in females. Among males, the mean average diameter of the aortic knob was 3.14±0.34 cm. A population-based large cohort study in the Netherlands showed that men had higher mean thoracic aorta diameter than women but provided no explanation as to why.27 Mean AKD findings in the Indian population20 and South Korean population13 were comparable with our findings (3.10 cm±0.334 cm and 3.42±0.478 respectively). The mean aortic knob diameter among females was 2.77±0.37. This value was smaller in comparison to the value obtained in the Indian20 study of 3.076 cm±0.39 cm and the south Korean13 study of 3.00±0.498 (Table 7).
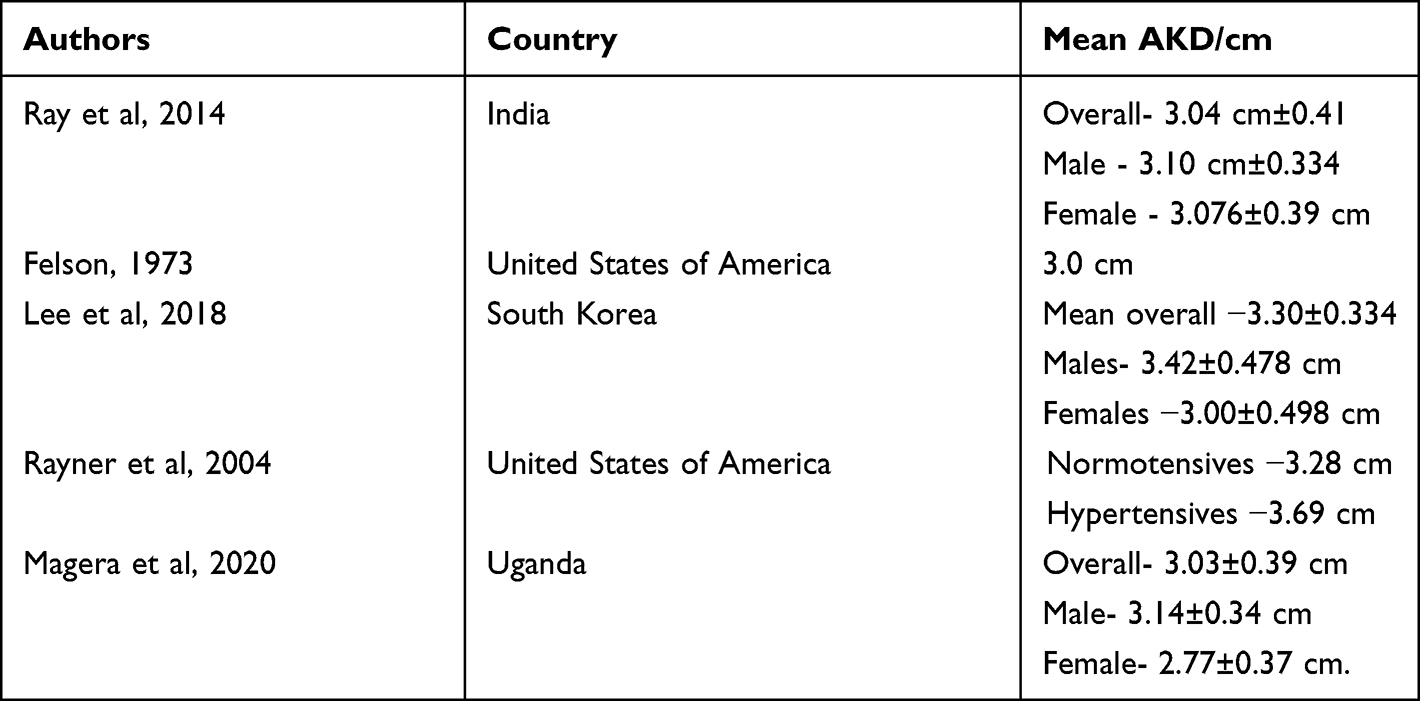 |
Table 7 Comparison of Aortic Knob Diameters in Different Populations |
The mean aortic knob and arch diameters were higher in males than females which is consistent with the findings of Ikeme et al28 and Ray et al.20 On the contrary, a study done in Jamaica reported a higher aortic arch size in females than males.29 These findings were attributed to the higher blood pressures in females than males.29
Kim and Choi observed that an aortic knob diameter (AKD) width of more than 4 cm occurred more frequently in patients with the thoracic aortic disorder as compared to normal subjects.30 In this study, there was no female with an AKD > 4cm but there were 2 males whose AKD was slightly above 4cm measured on the digital screen. These were healthy males with no cardiovascular disease and normal blood pressure for age.
The AAD is another measurement for evaluation of the size of the aorta on chest radiograph.31 In this study, the mean of the AAD was 5.6 ±0.64cm. This value is comparable to other values in different studies by Yousef and colleagues in Sudan32 5.3±0.6, and 5.3 by Umerah in Zambia.26 Anyanwu and Agwuna measured the width of the aortic shadow as the sum of the maximum extension of the aortic shadow to the right and left of the midline and found the mean of AAD varied between 4.7±0.5 cm in the Nigerian population.33
The mean THD and mean TTD were 12.9±12.6 cm and 29.07±2.78cm respectively. This was comparable to 11.9 ± 9 cm of mean THD and 27.8± 7cm of mean TTD in the Sudanese population.32 This means, our study population had a higher mean of transverse heart and thoracic diameters. In Sudanese and Nigerian studies, aortic knob diameter correlated positively with chest and heart diameters.25,32
In this study, we found that there was a slightly higher mean AKD when measurements were done on a digital screen than on the x-ray films and the difference was statistically significant. This can be explained by the fact that digital measurements on screens are correct to the nearest millimeter, which may be difficult to achieve on plain films due to approximation. Hence, in practice, measurements should be done on a digital screen rather than x-ray films. This study also demonstrated that weight and height did not significantly affect the size of the aortic knob.
The strengths of our study include being a prospective study with a relatively large sample size and its multi-centric nature. The limitation of the study was that it was a hospital-based study which could introduce selection bias. Moreover, the number of female participants was much smaller than the number of male counterparts.
Conclusions and Recommendations
The aortic knob diameter was higher in males and there was a positive correlation with age, aortic arch diameter, transverse heart diameter, and transverse thoracic diameter. We recommend aortic knob diameter measurements should be done on a digital screen than printed x-ray films and sex-specific aortic knob diameters should be utilized in clinical practice.
Abbreviations
AAD, aortic arch diameter; AKD, aortic knob diameter; THD, transverse heart diameter; PA, postero-anterior; TTD, transverse thoracic diameter.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Written informed consent was obtained from all participants to participate in the study. Ethical approval was obtained from the Makerere University School of Medicine Research and Ethics committee and administrative clearance was sought from the three hospitals. The study complies with the Declaration of Helsinki.
Acknowledgments
We would like to acknowledge all the lecturers and residents at the Department of Radiology and Radiotherapy, College of Health Sciences, Makerere University for their valuable technical assistance. We also thank Mr. Okello Bonny for his immense help in the analysis.
Author Contributions
All authors made a significant contribution to the study by participating in its conception, study design, execution, acquisition of data, analysis, and interpretation of the study results. The further all participated in the drafting, revising, and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World Health Organization. Cardiovascular diseases (CVDs) [Internet]; 2021 [cited February 22, 2022]. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
2. Stokes MB, Roberts-Thomson R. The role of cardiac imaging in clinical practice. Aust Prescr. 2017;40(4):151–155. doi:10.18773/austprescr.2017.045
3. Puddy E, Hill C. Interpretation of the chest radiograph. Cont Educ Anaesth Crit Care Pain. 2007;7(3):71–75. doi:10.1093/bjaceaccp/mkm014
4. Lai V, Tsang WK, Chan WC, Yeung TW. Diagnostic accuracy of mediastinal width measurement on posteroanterior and anteroposterior chest radiographs in the depiction of acute nontraumatic thoracic aortic dissection. Emerg Radiol. 2012;19(4):309–315. doi:10.1007/s10140-012-1034-3
5. Truszkiewicz K, Poręba R, Gać P. Radiological cardiothoracic ratio in evidence-based medicine. J Clin Med. 2021;10(9):2016. doi:10.3390/jcm10092016
6. Armstrong M, Kerndt CC, Moore RA. Physiology, Baroreceptors. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 [cited September 18, 2021]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK538172/.
7. Mayet J, Hughes A. Cardiac and vascular pathophysiology in hypertension. Heart. 2003;89(9):1104–1109. doi:10.1136/heart.89.9.1104
8. Xue Z, Long R, Jaeger S, Folio L, George Thoma R. Extraction of aortic knuckle contour in chest radiographs using deep learning. In:
9. Jain D, Dietz HC, Oswald GL, Maleszewski JJ, Halushka MK. Causes and histopathology of ascending aortic disease in children and young adults. Cardiovasc Pathol. 2011;20(1):15–25. doi:10.1016/j.carpath.2009.09.008
10. Goldstein SA, Evangelista A, Abbara S, et al. Multimodality imaging of diseases of the thoracic aorta in adults: from the American Society of Echocardiography and the European Association of Cardiovascular Imaging: Endorsed by the Society of Cardiovascular Computed Tomography and Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr. 2015;28(2):119–182. doi:10.1016/j.echo.2014.11.015
11. Halilu S, Aiyekomogbon J. The usefulness of aortic arch width measurements on chest radiographs of adult patients with systemic hypertension and hypertensive heart disease. New Niger J Clin Res. 2018;7(12):51.
12. Rayner BL, Goodman H, Opie LH. The chest radiograph. A useful investigation in the evaluation of hypertensive patients. Am J Hypertens. 2004;17(6):507–510. doi:10.1016/j.amjhyper.2004.02.012
13. Lee E-J, Han J-H, Kwon K-Y, et al. The relationship between aortic knob width and metabolic syndrome. Korean J Fam Med. 2018;39(4):253–259. doi:10.4082/kjfm.17.0038
14. Erkan H, Korkmaz L, Ağaç MT, et al. Relation between carotid intima-media thickness and aortic knob width in patients with essential hypertension. Blood Press Monit. 2011;16(6):282–284. doi:10.1097/MBP.0b013e32834e3d5c
15. Musinguzi G, Wanyenze RK, Ndejjo R, et al. An implementation science study to enhance cardiovascular disease prevention in Mukono and Buikwe districts in Uganda: a stepped-wedge design. BMC Health Serv Res. 2019;19(1):253. doi:10.1186/s12913-019-4095-0
16. Felson B. A review of over 30,000 normal chest roentgenograms. In: Chest Roentgenology. Philadelphia: Saunders; 1973:494–495.
17. Afsar B, Saglam M, Yuceturk C, Agca E. The relationship between aortic knob width and various demographic, clinical, and laboratory parameters in stable hemodialysis patients. Saudi J Kidney Dis Transpl. 2014;25(6):1178–1185. doi:10.4103/1319-2442.144250
18. van Hout MJ, Scholte AJ, Juffermans JF, et al. How to measure the aorta using MRI: a practical guide. J Magn Reson Imaging. 2020;52(4):971–977. doi:10.1002/jmri.27183
19. Rosner B. Fundamentals of Biostatistics. Cengage learning; 2015.
20. Ray A, Mandal D, Kundu P, Manna S, Mandal S. Aortic knob diameter in chest X-ray and its relation with age, heart diameter and transverse diameter of thorax in a population of Bankura district of West Bengal, India: a cross sectional study. J Evol Med Dent Sci. 2014;3(31):8595–8601.
21. Kabala JE, Wilde P. The measurement of heart size in the antero-posterior chest radiograph. Br J Radiol. 1987;60(718):981–986. doi:10.1259/0007-1285-60-718-981
22. Ungerleider HE, Gubner RS. Evaluation of heart size measurements. Am Heart J. 1942;24:494–510. doi:10.1016/S0002-8703(42)90966-9
23. Mitchell JRA, Schwartz CJ. Arterial Disease. Blackwell Scientific Publications; 1965.
24. Redheuil A, Yu W-C, Mousseaux E, et al. Age-related changes in aortic arch geometry: relationship with proximal aortic function and left ventricular mass and remodeling. J Am Coll Cardiol. 2011;58(12):1262–1270. doi:10.1016/j.jacc.2011.06.012
25. Obikili EN, Okoye IJ. Aortic arch diameter in frontal chest radiographs of a normal Nigerian population. Niger J Med. 2004;13(2):171–174.
26. Umerah BC. Unfolding of the aorta (aortitis) associated with pulmonary tuberculosis. Br J Radiol. 1982;55(651):201–203. doi:10.1259/0007-1285-55-651-201
27. Bons LR, Rueda-Ochoa OL, El Ghoul K, et al. Sex-specific distributions and determinants of thoracic aortic diameters in the elderly. Heart. 2020;106(2):133–139. doi:10.1136/heartjnl-2019-315320
28. Ikeme AC, Ogakwu MA, Nwakonobi FA. The significance of the enlargement of the aortic shadow in adult Nigerians. Afr J Med Med Sci. 1976;5(3):195–199.
29. Stuart KL, Miall WE, Tulloch JA, Christian DE. Dilatation and unfolding of the aorta in a Jamaican population. Br Heart J. 1962;24:455–463. doi:10.1136/hrt.24.4.455
30. Kim K-T, Choi Y-H. Nontraumatic disorders in mediastinum and thoracic aorta: chest radiographic findings. J Korean Soc Emerg Med. 2000;72–82. Available from: https://pesquisa.bvsalud.org/portal/resource/pt/wpr-123741.
31. McComb BL, Munden RF, Duan F, Jain AA, Tuite C, Chiles C. Normative reference values of thoracic aortic diameter in American College of Radiology Imaging Network (ACRIN 6654) arm of national lung screening trial. Clin Imaging. 2016;40(5):936–943. doi:10.1016/j.clinimag.2016.04.013
32. Yousef M, Gameraddin M, Ali A, Ahmed B. Aortic and heart dimensions of adults in Sudanese’s population using chest X-ray. Kärntner Botanikzentrum. 2014;21(4):122–3.
33. Anyanwu GE, Agwuna KK. Aortic arch diameter and its significance in the clinical evaluation of cardiac and aortic enlargements. Niger J Clin Pract. 2009;12(4):453–456.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.