Back to Journals » Journal of Experimental Pharmacology » Volume 17
Antidiabetic Activity of Moringa oleifera Aqueous Leaf Extract on Prediabetic Wistar Male Rats
Authors Nurhayati T, Tarawan VM, Delia H, Faisal F, Goenawan H ![]() , Setiawan S
, Setiawan S
Received 17 August 2024
Accepted for publication 20 November 2025
Published 21 December 2025 Volume 2025:17 Pages 861—872
DOI https://doi.org/10.2147/JEP.S490839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Abdelwahab Omri
Titing Nurhayati,1 Vita Murniati Tarawan,1 Happy Delia,2 Faisal Faisal,3 Hanna Goenawan,1 Setiawan Setiawan1
1Departement of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Jatinangor, Indonesia; 2Faculty of Medicine, Universitas Padjadjaran, Jatinangor, Indonesia; 3Departement of Pediatrics, Rumah Sakit Hasan Sadikin, Bandung, Indonesia
Correspondence: Titing Nurhayati, Department of Biomedical Sciences, Faculty of Medicine, Universitas Padjadjaran, Jl. Raya Bandung Sumedang KM.21, Hegarmanah, Kec, Jatinangor, Kabupaten Sumedang, Jawa Barat, 45363, Indonesia, Email [email protected]
Purpose: Diabetes mellitus is a chronic metabolic disorder linked to sedentary lifestyles, which reduces insulin sensitivity and increases hyperglycemia risk. Standard treatments include lifestyle changes and medications. Recently, herbal remedies like Moringa oleifera leaves have gained attention due to bioactive compounds—polyphenols and flavonoids—believed to have antihyperglycemic effects. However, research on their impact on prediabetic conditions remains limited. This study aimed to investigate the effect of Moringa leaf extract on blood glucose levels in sedentary male Wistar rats to explore its potential as a natural antihyperglycemic agent.
Patients and Methods: Thirty sedentary male Wistar rats, representing a lifestyle-induced prediabetic model, were acclimatized for two weeks and randomized into five groups: Control (K), Metformin (M), and three treatment groups receiving Moringa oleifera leaf extract at doses of 200 mg/kgBW (D200), 400 mg/kgBW (D400), and 800 mg/kgBW (D800). The intervention lasted for 12 weeks. Blood glucose levels—including fasting, postprandial, and time-based measurements—were assessed using an Accutrend Plus device. Data were analyzed with the Shapiro–Wilk, Levene, Kruskal–Wallis, and Mann–Whitney tests (p < 0.05).
Results: Moringa leaf extract demonstrated a dose-dependent reduction in blood glucose levels. In the FBG test, all treatment groups showed significantly lower glucose levels compared to the control (K: 122.8 mg/dL; D200: 85.6 mg/dL; D400: 82.6 mg/dL; D800: 95.4 mg/dL; P=0.015). Similarly, TBG levels were lower in D200 (197.8 mg/dL) and D400 (186.8 mg/dL) compared to K (231 mg/dL; P=0.022). Although the PPBG decreased over time, especially in D200, the differences were not statistically significant (P> 0.05).
Conclusion: Administration of Moringa leaf powder has been shown to significantly reduce fasting blood glucose levels, but not postprandial or intermittent blood glucose levels.
Keywords: Moringa oleifera, Moringa leaves, blood glucose, antihyperglycemic, sedentary lifestyle, metabolic syndrome
Introduction
Diabetes, a chronic metabolic disorder characterized by increased blood glucose levels, was included in the top 10 causes of death globally in 2019.1,2 In 2021, the death toll from diabetes reached 6.7 million, with 537 million cases in adults aged 20–79 years which is equivalent to one in ten people in the world.3 The prevalence of diabetes mellitus in Indonesia increased from 1.5% in 2013 to 2% in 2018, affecting all provinces including West Java, where the percentage reached 1.7.4 The increase in the incidence of diabetes is influenced by two types of risk factors, namely those that can be modified and those that cannot be modified.5
One risk factor that can be modified is physical activity which refers to the condition of not doing enough physical activity for 150 minutes per week or not doing high-intensity physical activity for 75 minutes or a combination thereof per week.6 On the other hand, there is the term sedentary lifestyle which describes awake behavior with energy expenditure ≤1.5 metabolic equivalents (METs).7 These two terms are thought to be related, although the sedentary lifestyle is independent and perhaps even more so than physical inactivity.6 The results of the meta-analysis show that there is no significant difference between people who are very physically active (>35.5 METs-d/week) and individuals who spend less than 4 hours/day sedentary or even do no physical activity for more than 8 hours/day. However, watching television for more than 3 hours/day, even ≥5 hours/day can increase the risk of death, including diabetes mellitus.6,8–10
Diabetes mellitus is caused by metabolic dysfunction, such as increased plasma triglycerides, high-density lipoprotein (HDL) cholesterol, and insulin resistance.8,9,11,12 Insulin, an important hormone in metabolism and glucose regulation, is disrupted in cases of diabetes mellitus increasing blood glucose levels.13,14
High blood glucose levels can be overcome with a healthy lifestyle such as a balanced diet and physical activity. However, to achieve adequate glycemia in the long term, pharmacological modifications are necessary, including the use of metformin as first-line therapy.15,16 Metformin reduces glucose production in the liver by inhibiting the mitochondrial respiratory chain which causes AMPK to be activated, insulin sensitivity to increase, and cAMP to decrease so that the expression of gluconeogenic enzymes decreases.17
In addition, insulin sensitivity in type 2 diabetes sufferers can also be increased by using herbal medicine.18,19 About a quarter of modern medicines are thought to originate from natural products.20 One of them is the Moringa plant (Moringa oleifera), a herbal plant that grows in subtropical and tropical areas such as Indonesia. This herbal plant is known as Miracle’s Tree and Mother’s Best Friend because of its rich nutrition and pharmacological effects, such as antidiabetic.18,19,21 The antidiabetic content in Moringa leaves, such as polyphenols and flavonoids, affects glucose intake in the small intestinal mucosa so that absorption of blood glucose takes more time and reduces increases in blood glucose levels.22 Previous research also showed that mice given Moringa oleifera leaf extract had lower fasting blood glucose levels than the control group, namely 5.78 ± 0.74 mmol/L (Moringa leaf extract treatment group) and 7.91 ± 0.52 mmol /L (control group).23
However, research regarding the nutritional potential and antihyperglycemic properties of Moringa leaf extract in prediabetic mice is still limited and has not reached definite conclusions. Apart from that, the optimal dose of Moringa leaf extract in treating diabetes has not been identified. Therefore, this prompted the author to research the effect of administering Moringa oleifera leaf extract on blood sugar levels in male Wistar rats. This study offers a novel approach by evaluating the antihyperglycemic effects of Moringa oleifera in a lifestyle-induced prediabetic model rather than a chemically induced diabetic model. This provides new insights into its potential preventive role in early glucose dysregulation.
Materials and Methods
Study Design
This research used data obtained from laboratory experiments with blood samples from male Wistar rats. This research used semi-quantitative analytical methods and was conducted from December 2023 to January 2024 at the Faculty of Medicine, Padjadjaran University. The prediabetic state was developed through a sedentary lifestyle model without using chemical induction agents such as Alloxan or Streptozotocin (STZ). This approach was chosen to model early-stage glucose dysregulation associated with physical inactivity, rather than chemically induced diabetes.
Study Samples
A total of 30 male Wistar rats were used as research samples with the following inclusion criteria: male, 9–10 weeks old, body weight 250–275 grams, and healthy. Meanwhile, the exclusion criteria were mice that had been treated, mice with changes in behavior, injuries, or illness, changes in hair structure, loose feces, and mice that experienced >10% weight loss during the adaptation period. Mice that die either during the adaptation period or the treatment period are criteria for mice that will be removed or dropped out. After going through the adaptation process, the mice were then randomized into 5 groups – control, metformin, and three treatment groups, and the experimental period was 12 weeks. Rats in the control group were rats that were given standard food and drink, while rats in the metformin group were given 200 mg/kgBW/day of metformin and standard feed. Both groups did not receive Moringa oleifera leaf extract at all during the treatment period. This is different from the three other treatment groups which were given Moringa oleifera extract for 12 weeks, namely at a dose of 200 mg/kgBW/day, 400 mg/kgBW/day, or 800 mg/kgBW/day. Determination of the dose of Moringa leaf water extract in this study refers to previous research conducted by Adedapo et al, (2009) which concluded that the safety of Moringa leaf water extract given orally for 21 days (subacute) to mice was at a dose of 400, 800 mg/kg body weight, and toxicity test studies conducted by Awodele et al (2012) which stated that the safety of Moringa leaf water extract for 60 days (subchronic) given at a dose of 200–1500 mg/KgBW.20,21 So research was carried out using Moringa leaf powder suspended with water compounds at doses of 200, 400, and 800 mg/KgBW for 90 days (sub-chronic) to determine the optimum dose of giving Moringa leaves to rats for long-term use long.24,25
The independent variable in this research is the fine form of Moringa leaf extract obtained from PT. Indonesian Organic Moringa (MOI) has been certified by the Indonesian Food and Drug Supervisory Agency with distribution permit number: BPOM RI MD 619111001777. First, the Moringa leaf extract is dissolved in a water solvent. After that, the extract solution was given orally using a gastric probe once/day every 08.00 WIB during the treatment period with the number of doses mentioned previously. The author chose to use Moringa leaf powder from PT. The MOI for this research is because the company applies strict standards in the production of Moringa leaf extract and guarantees that all production stages are carried out in a structured manner. These products are the best representation of the quality of Moringa leaves in Indonesia.
The dependent variable observed in this study was blood glucose levels, which consisted of fasting blood glucose, postprandial blood glucose, and random blood glucose. Blood glucose levels were measured by taking blood samples through the rat’s tail vein and using the Accutrend Plus device. The three blood glucose levels are differentiated based on the time of blood sampling. Before termination, Time Blood Glucose sampling (TBG) is carried out. The normal value for TBG levels is 3.95 ± 1.31 mmol/L to 7.5 mmol/L or the equivalent of 71 to 135 mg/dl. Fasting Blood Glucose (FBG) was measured after the mice had been fasted for ± 10 hours, followed by sampling at 08.00 WIB. After that, the mice will receive treatment according to their group and continue with taking Postprandial Blood Glucose (PPBG) samples at the 15th, 30th, 60th, and 120th minutes. Normal rat PPBG levels are 5.65 ± 1.63 mmol/L to 10 mmol/L or the same as 102 to 80 mg/dl.26
Data Collection and Analysis
After undergoing an adaptation period of 2 weeks, the mice were ready to enter the experimental period for 12 weeks. First, the animal is anesthetized to reduce nerve activity to eliminate pain during the surgical process.25 After anesthesia, blood samples were taken via the rat’s tail vein and then dripped onto a glucose strip on the Accutrend Plus to measure the rat’s blood glucose levels. The blood glucose levels obtained were the variables observed in this study.
Analysis of research results was carried out by presenting data using the IBM SPSS Statistics version 28.0.1.1 program. All data was tested using the Shapiro–Wilk normality test and Levene’s homogeneity test. Because one of the basic requirements for using One Way ANNOVA is not met, namely the normality test, a nonparametric test needs to be carried out, namely Kruskall Wallis. After that, if there are significant differences, further tests are carried out to see significant differences between treatment groups using Mann–Whitney. Statistical analysis showed significant differences if the P value <0.05 was met. These findings will be described and discussed further in the following chapters.
Ethical Consideration
All laboratory procedures involving animals were conducted in strict accordance with internationally recognized ethical standards for animal research, particularly the 3Rs principles (Replacement, Reduction, and Refinement) and the Five Freedoms (freedom from hunger and thirst; discomfort; pain, injury, or disease; freedom to express normal behavior; and freedom from fear and distress). These guidelines were rigorously applied throughout all experimental stages involving mice to ensure humane handling and welfare of the animals. The ethical framework of this study was based on The Principles of Humane Experimental Technique (Russell and Burch, 1959). Ethical clearance for the study was granted by the Padjadjaran University Research Ethics Committee (Approval No. 1390/UN6.KEP/EC/2023).
Results
Of the 30 mice involved, the final sample size in the study was 25 mice. This happened because mice in the negative group (K4) and the treatment group (M16 and M35) died during the treatment. Therefore, each treatment group uses 5 data to calculate the same mean. Rat death can be caused by several factors, such as environmental factors, stress, or infection. However, this event did not affect the research results because it was included in the dropout criteria.
After receiving the experimental data, an analysis of blood glucose levels in the five types of treatment groups was carried out. Based on the normality, homogeneity and mean difference tests carried out, all dependent variables were proven to have significant differences, except for postprandial blood glucose as seen in Table 1.
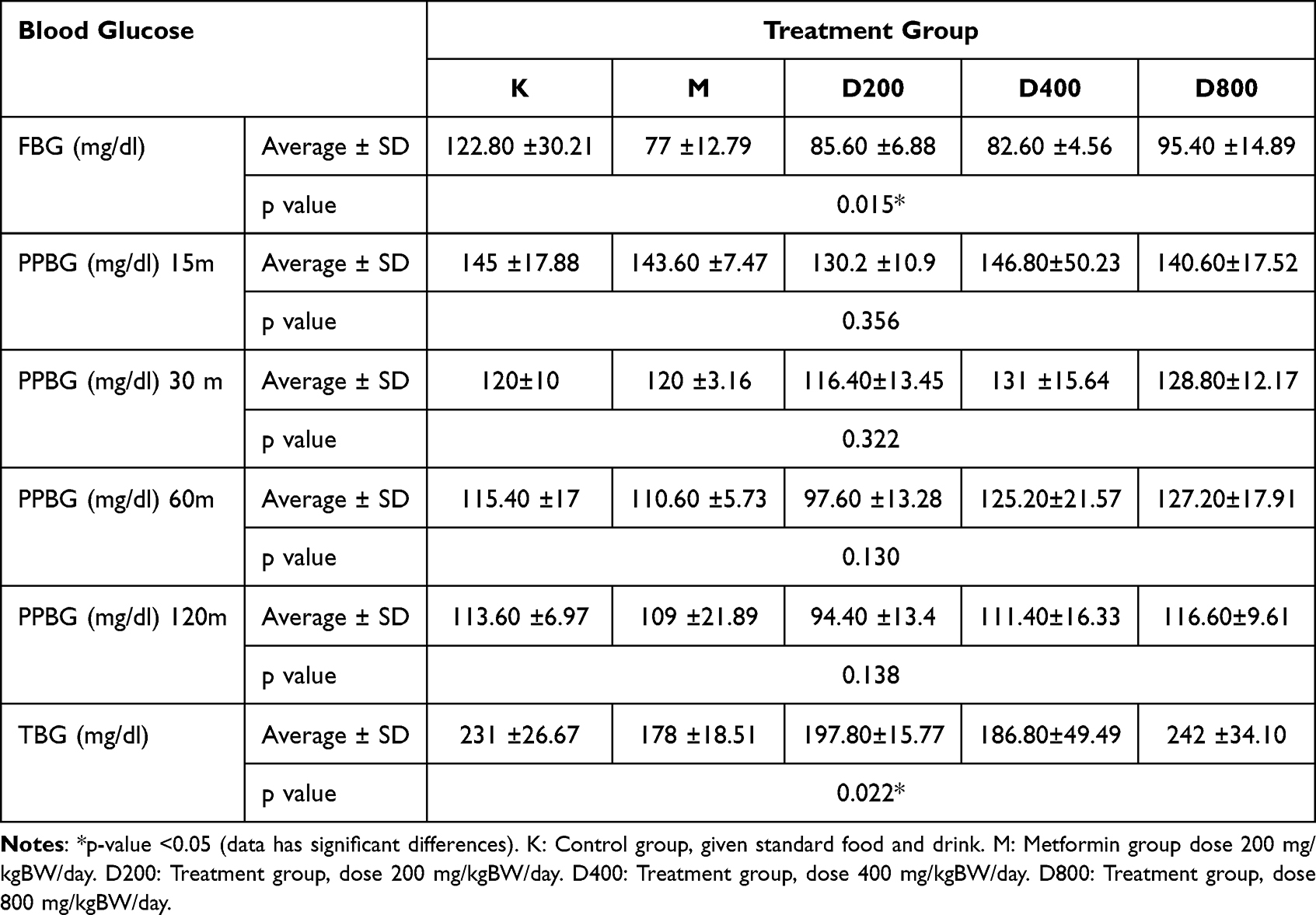 |
Table 1 Kruskall-Wallis Mean Difference Test Results |
Fasting blood glucose levels in the group of mice given Moringa leaf extract were lower compared to the control group. A comparison of the average fasting blood glucose levels in each treatment group can be seen in Figure 1.
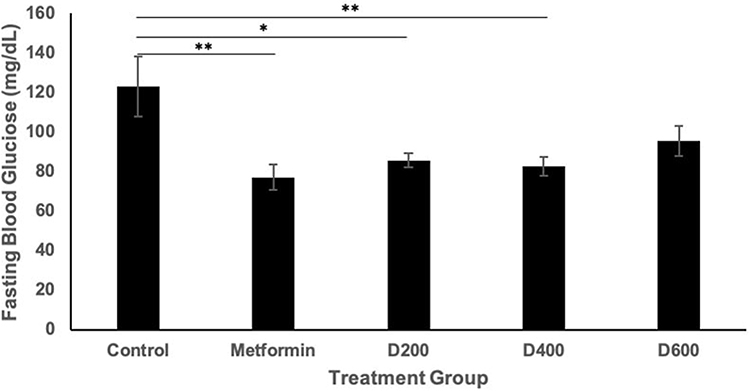 |
Figure 1 Graph of Average Fasting Blood Glucose. *p-value <0.05 (data has significant differences). **p-value <0.005 (data has very significant differences). |
Based on Figure 1, the FBG levels obtained in group K were 122.8 mg/dl, group M was 77 mg/dl, group D200 was 85.6 mg/dl, group D400 was 82.6 mg/dl, and group D800 amounting to 95.4 mg/dl. In general, all doses were able to reduce fasting blood glucose levels because they gave lower results compared to the negative control. Then, compared to the positive control group (M), FBG levels were higher in mice given Moringa leaf extract.
Next, to see which groups experienced statistically significant differences, a pairwise comparisons test was carried out, namely, the Mann–Whitney test on the FBG variable as seen in Table 2.
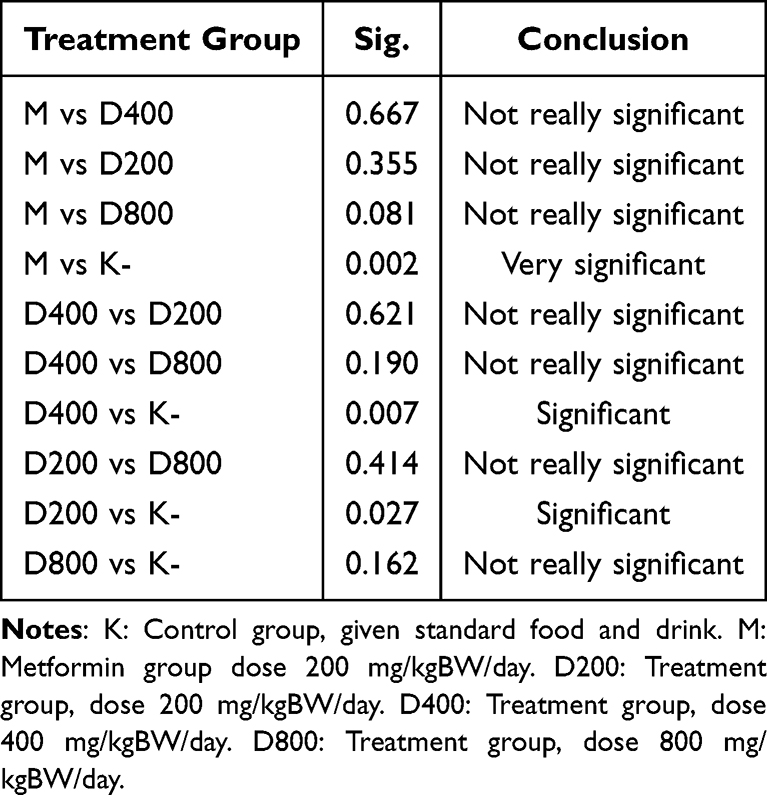 |
Table 2 Mann–Whitney Test Results for FBG Variables |
Based on Table 2 above, the results of the Mann–Whitney test show that there are significant differences regarding the FBG variable profile between groups of experimental animals. Real differences were seen in group M and group K, group K and group D400, and group K with administration of D200.
Along with that, the blood glucose in the group of mice given Moringa leaf extract also showed lower results than the control group (Figure 2). From these results, it can be seen that each dose of Moringa leaf powder shows varying changes in blood glucose levels over time. A decrease in blood glucose levels occurred in the D200 (197.8 mg/dl) and D400 (186.8 mg/dl) groups. In addition, TBG levels were higher in the D800 group (242 mg/dl) compared to the K group (231 mg/dl).
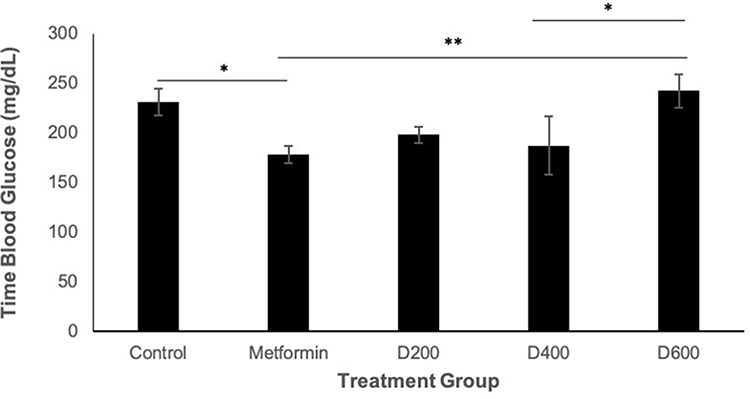 |
Figure 2 Graph of Average Time Blood Glucose. *p-value <0.05 (data has significant differences). **p-value <0.005 (data has very significant differences). |
Furthermore, to determine statistically significant differences between groups, the Mann–Whitney test was also carried out on the FBG variable, which can be observed in Table 3.
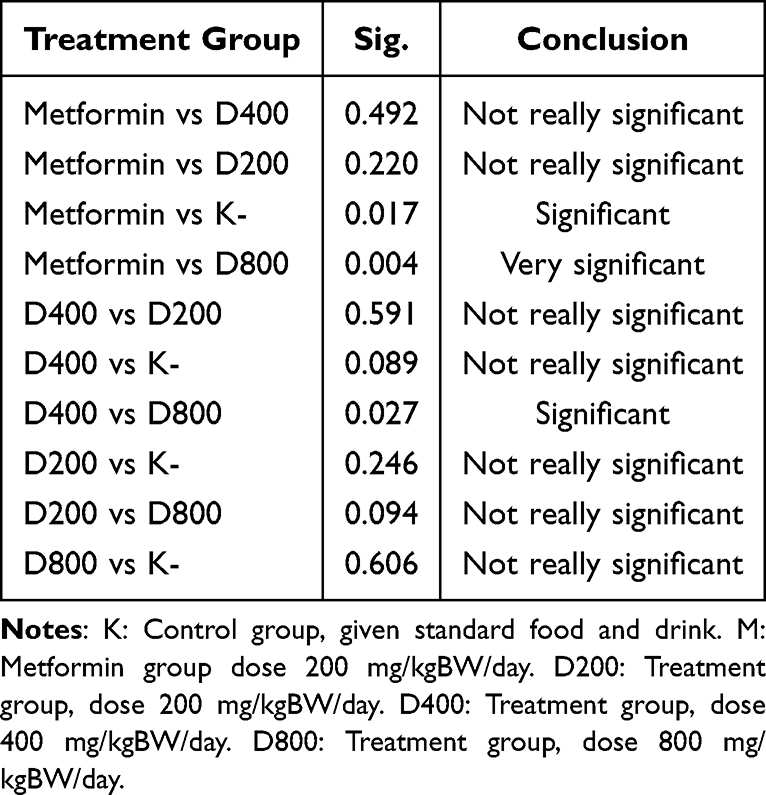 |
Table 3 Mann–Whitney Test Results for TBG Variables |
Based on Table 3, significant differences occurred between group M and group K, group M and group D800, and group D400 and group D800.
Meanwhile, although not statistically significant, in Figures 3–6 there is a tendency that postprandial blood glucose levels in the control group tended to be higher than in the group of mice given Moringa leaf extract. This pattern was only observed in the D200 group, while D400 and D800 showed higher levels compared to the control group.
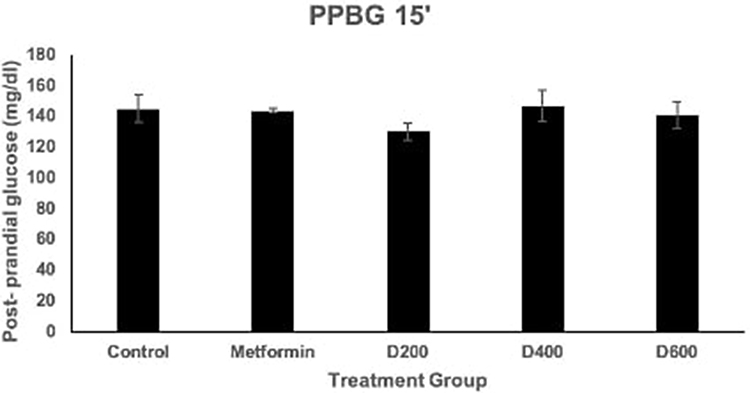 |
Figure 3 Graph of Average Postprandial Blood Glucose at 15 minutes. |
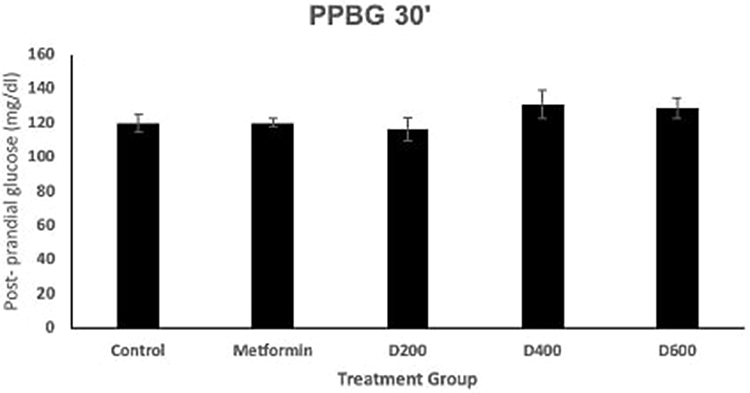 |
Figure 4 Graph of Average Postprandial Blood Glucose at 30 minutes. |
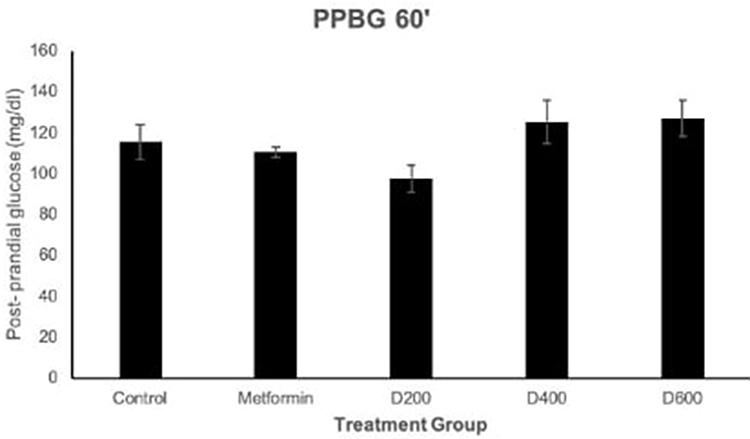 |
Figure 5 Graph of Average Postprandial Blood Glucose at 60 minutes. |
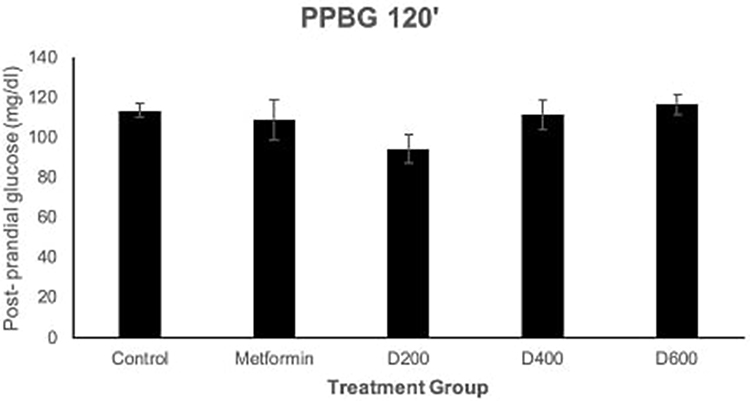 |
Figure 6 Graph of Average Postprandial Blood Glucose at 120 minutes. |
If observed from the other side, postprandial blood glucose levels decreased over time in all treatment groups. This can be observed in Figures 7–11.
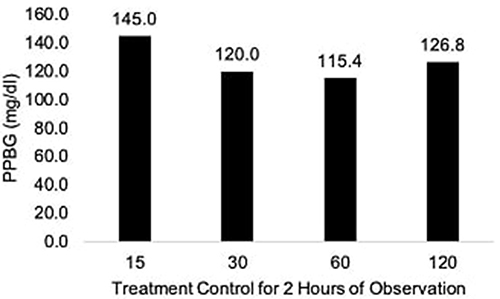 |
Figure 7 PPBG Changes in the Control Group Over a 2-Hour Observation Period. |
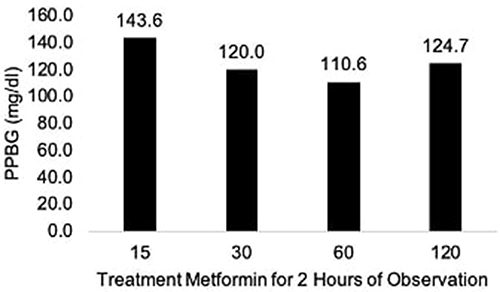 |
Figure 8 PPBG Changes in the Metformin Group Over a 2-Hour Observation Period. |
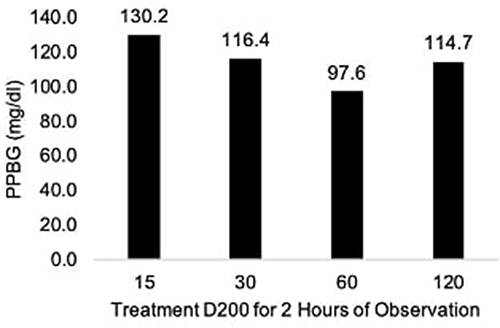 |
Figure 9 PPBG Changes in the D200 Group Over a 2-Hour Observation Period. |
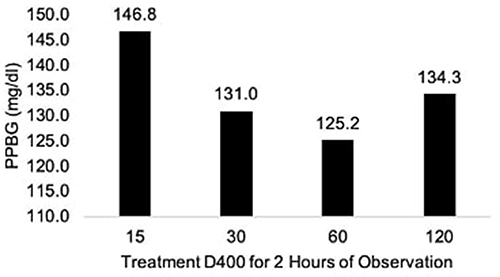 |
Figure 10 PPBG Changes in the D400 Group Over a 2-Hour Observation Period. |
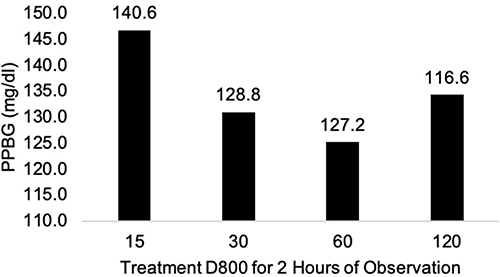 |
Figure 11 PPBG Changes in the D800 Group Over a 2-Hour Observation Period.jpg. |
Discussion
Based on the results of research that has been carried out, the FBG variables D200, D400, and D800 show lower glucose levels compared to the control group. Group K showed a value of 122.8 mg/dl, while group D200 reached 85.6 mg/dl, group D400 82.6 mg/dl, and group D800 reached 95.4 mg/dl. Meanwhile, the D400 group provided an effect that was quite equivalent to the M group which resulted in a reduction in blood glucose of 77 mg/dl. Based on the Mann–Whitney test, the D200 and D400 groups were also proven to have significant differences when compared with the K group. However, D800 did not show any real differences when compared with group K. This research is in line with Marisa et al 2018 in Mexico which evaluated the preventive effect of Moringa oleifera on metabolic syndrome in male Wistar rats. After induction of metabolic syndrome, rat FBG levels were higher in the control group (103 ± 3.8 mg/dl) compared to the prevention group that received Moringa oleífera before induction. (80.09 ± 5.5 mg/dl). At the end of the experiment, FBG levels also showed higher results in the control group compared to the treatment group, but the difference was not significant.27 Other findings were also confirmed by Shidiq et al 2019 which used doses of Moringa leaf flour of 125 mg/kgBW/day, 250 mg/kgBW/day, and 500 mg/kgBW/day on alloxan-induced male rats. The study showed a decrease in fasting blood glucose levels in the Moringa leaf flour group with 500 mg/kgBW/day, an effect equivalent to glibenclamide.28 The results of this study provide differences in the number of doses, dosage form, and duration of administration of Moringa oliefera.
Meanwhile, in the timeblood glucose variable, it was also seen that there was a decrease in the treatment group, but the D800 was higher than the control (243 mg/dl > 231 mg/dl). This shows that there is a toxic effect from administering Moringa leaf extract at a dose of 800 mg/kgBW on timeblood glucose. In addition, previous research by Yasaroh et al 2021 stated that giving Moringa leaf extract treatment with dose variants of 200 mg/KgBW, 400 mg/KgBW and 600 mg/KgBW was able to reduce blood glucose levels compared to the control treatment induced by alloxan.29 However, based on the Mann–Whitney test, the real difference between the control group and the Moringa leaf powder treatment was not proven to be real.
Changes in the average PPBG profile 15’, 30’, 60’, and 120’ have not provided statistically significant results. The results obtained are in line with previous research by Leone et al 2018 in his research which reported the results of evaluating postprandial glucose responses in 2 criteria for mice, namely healthy mice and diabetic mice. In healthy subjects, male Wistar rats did not show significant results after being observed at several postprandial time points. Meanwhile, diabetic mice gave a lower average glycemic response after being given Moringa leaf powder compared to controls, with results that were statistically significant.30 Differences in results may arise due to variations in dose used, duration of treatment, methods and examination parameters used.
In general, Moringa leaves have been reported to have benefits for several chronic diseases including cardiovascular conditions, liver disease, cancer, insulin resistance, and diabetes. For example, cardioprotective effects have been attributed to the presence of quercetin, chlorogenic acid, alkaloids, tannins, ITC, and B-sitosterol.31 Meanwhile. Anudeep et al 2016 in his research reported that Moringa oleifera contains soluble fiber which improves glucose levels, lymphocyte proliferation and induces nitric oxide from macrophages.
In DM, the capacity of the small intestine to absorb glucose is increased, due to increased expression of GLUT2 and SGLT1. This creates an additional burden on patients suffering from DM, which is further complicated by the fact that most antidiabetic drugs, such as sulfonylureas, biguanides, or thiazolidinediones, have their primary targets in organs other than the intestine.32 One proposed mechanism involves quercetin, as this substance may act as an apical inhibitor of GLUT2, although it does not affect GLUT5 or SGLT1. Quercetin has also been shown to activate adenosine monophosphate-activated protein kinase (AMPK), increase glucose absorption through stimulation of GLUT4 in skeletal muscle, and decrease glucose production through downregulation of phosphoenolpyruvate carboxykinase (PEPCK) and glucose-6. -phosphatase (G6Pase) in the liver.
The mechanism for reducing blood glucose levels can be influenced by the content of bioactive compounds contained in Moringa leaves. The antidiabetic content in Moringa leaves includes various polyphenols and flavonoids which can influence glucose intake in the small intestinal mucosa so that glucose absorption in the blood takes longer and ultimately lowers blood sugar levels. Apart from that, Moringa leaf extract also provides anti-hyperglycemic effects by inhibiting the α-glucosidase enzyme in the brush border of the small intestine. By inhibiting the α-glucosidase enzyme, the rate of carbohydrate digestion becomes slower and ultimately reduces postprandial hyperglycemia.22
In DM, the capacity of the small intestine to absorb glucose is increased, due to increased expression of GLUT2 and SGLT1. This creates an additional burden on patients suffering from DM, which is further complicated by the fact that most antidiabetic drugs, such as sulfonylureas, biguanides, or thiazolidinediones, have their primary targets in organs other than the intestine.32 One proposed mechanism involves quercetin, as this substance may act as an apical inhibitor of GLUT2, although it does not affect GLUT5 or SGLT1. Quercetin has also been shown to activate adenosine monophosphate-activated protein kinase (AMPK), increase glucose absorption through stimulation of GLUT4 in skeletal muscle, and decrease glucose production through downregulation of phosphoenolpyruvate carboxykinase (PEPCK) and glucose-6. -phosphatase (G6Pase) in the liver.33
Inhibitory activity of α-glucosidase, pancreatic α-amylase, and intestinal sucrose, contributes to antihyperglycemic properties. The inhibitory effect is believed to be due to the action of phenolic compounds, flavonoids, and tannins found in Moringa. Slow carbohydrate digestibility, also caused by inhibition of these enzymes, causes a decrease in post-prandial hyperglycemia and hemoglobin A1C (HbA1C). In addition, this compound has protective and regenerative properties on pancreatic beta cells and can increase insulin production and release. These findings suggest that Moringa oleifera may serve as a potential complementary approach for early intervention in prediabetic conditions. Further studies are needed to determine the optimal dosage and to evaluate potential side effects at higher doses. This study demonstrates the preventive potential of Moringa oleifera in a lifestyle-induced prediabetic model, though limited by its animal-based design.34
Conclusion
In conclusion, Moringa oleifera leaf powder demonstrated a significant reduction in fasting blood glucose levels in a lifestyle-induced prediabetic model, suggesting its potential as a complementary natural agent for early glycemic control in prediabetic conditions. However, further studies are warranted to isolate its active components, verify dose-dependent effects, and confirm long-term safety.
Acknowledgments
Authors thank the following for their support during the process of this study: APC (Article Processing Charge) – DRPM Universitas Padjadjaran.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. World Health Organization. Diabetes. 2023. Available from: https://www.who.int/health-topics/diabetes.
2. World Health Organization. The top 10 causes of death. 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
3. International Diabetes Federation. IDF diabetes atlas 10th edition. 2021. Available from: https://diabetesatlas.org/idfawp/resource-files/2021/07/IDF_Atlas_10th_Edition_2021.pdf.
4. Riskesdas. Hasil Utama Riskesdas 2018. 2018. Available from: https://kesmas.kemkes.go.id/assets/upload/dir_519d41d8cd98f00/files/Hasil-riskesdas-2018_1274.pdf.
5. Kemenkes. Infodatin Tetap Produktif, Cegah, dan Atasi Diabetes Melitus. 2020. Available from: https://www.kemkes.go.id/downloads/resources/download/pusdatin/infodatin/Infodatin%202020%20Diabetes%20Melitus.pdf.
6. Panahi S, Tremblay A. Sedentariness and health: is sedentary behavior more than just physical inactivity? Front Public Health. 2018;6(258). doi:10.3389/fpubh.2018.00258
7. Tremblay MS, Aubert S, Barnes JD, et al. Sedentary behavior research network (SBRN) – terminology consensus project process and outcome. Int J Behav Nutrition Phys Activity Home About Articles Submission Guidelines. 2017:75.
8. Park JH, Moon JH, Kim HJ, Kong MH, Oh YH. Sedentary lifestyle: overview of updated evidence of potential health risks. Korean J Fam Med. 2020;41(6):365–373. doi:10.4082/kjfm.20.0165
9. Patterson R, McNamara E, Tainio M, et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur J Epidemiol. 2018;33(9):811–829. doi:10.1007/s10654-018-0380-1
10. Saunders TJ, McIsaac T, Douillette K, et al. Sedentary behaviour and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S197–217. doi:10.1139/apnm-2020-0272
11. Li DD, Yang Y, Gao ZY, et al. Sedentary lifestyle and body composition in type 2 diabetes. Diabetol Metab Syndr. 2022;14(1):8. doi:10.1186/s13098-021-00778-6
12. Joseph JJ, Echouffo-Tcheugui JB, Golden SH, et al. Physical activity, sedentary behaviors and the incidence of type 2 diabetes mellitus: the multi-ethnic study of atherosclerosis (Mesa). BMJ Open Diabetes Res Care. 2016;4(1):e000185. doi:10.1136/bmjdrc-2015-000185
13. Hamilton MT, Hamilton DG, Zderic TW. Sedentary behavior as a mediator of type 2 diabetes. Med Sport Sci. 2014;60:11–26.
14. Rahman MS, Hossain KS, Das S, et al. Role of insulin in health and disease: an update. Int J Mol Sci. 2021;22(12):6403. doi:10.3390/ijms22126403
15. Feingold K. Oral and injectable (Non-Insulin) pharmacological agents for the treatment of type 2 diabetes. Endotext. 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279141/.
16. Goyal R, Jialal I. Type 2 diabetes. StatPearls. 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513253/.
17. Rena G, Hardie DG, Pearson ER. The mechanisms of action of metformin. Diabetologia. 2017;60(9):1577–1585. doi:10.1007/s00125-017-4342-z
18. Syamra A, Indrawati A, Warsyidah AA. Pemberian rebusan daun kelor terhadap penurunan kadar glukosa darah pada pasien penderita diabetes mellitus (DM). Vol. 8. Jurnal Media Laboran; 2018. Available from: http://farmingschool.blogspo.
19. Pareek A, Pant M, Gupta MM, et al. Moringa oleifera: an updated comprehensive review of its pharmacological activities, ethnomedicinal, phytopharmaceutical formulation, clinical, phytochemical, and toxicological aspects. Int J Mol Sci. 2023;24(3):2098. doi:10.3390/ijms24032098
20. Yuan H, Ma Q, Ye L, Piao G. The traditional medicine and modern medicine from natural products. Molecules. 2016;21(5):559. doi:10.3390/molecules21050559
21. Gopalakrishnan L, Doriya K, Kumar DS. Moringa oleifera: a review on nutritive importance and its medicinal application. Food Sci Human Wellness. 2016;5(2):49–56. doi:10.1016/j.fshw.2016.04.001
22. Alethea T, Ramadhian DMR, Antidiabetik E, Kelor D, Ramadhian MR. Efek antidiabetik pada daun kelor. Majority. 2015;4:118–122.
23. Zhao C, Zhu JZ, Song CR, et al. Effects of moringa oleifera leaf extract plus rosiglitazone on serum leptin and glucose and lipid metabolism in type 2 diabetic rats. Altern Ther Health Med. 2023;29(8):650–655.
24. Awodele O, Oreagba IA, Odoma S, Teixeira da Silva JA, Osunkalu VO. Toxicological evaluation of the aqueous leaf extract of Moringa oleifera Lam. J Ethnopharmacol. 2012;139(2):330–336. doi:10.1016/j.jep.2011.10.008
25. Adedapo AA, Mogbojuri OM, Emikpe BO. Safety evaluations of the aqueous extract of the leaves of Moringa oleifera in rats. J Med Plants Res. 2009;3:586–591.
26. Wang Z, Yang Y, Xiang X, Zhu Y, Men J, He M. Estimation of the normal range of blood glucose in rats. Wei Sheng Yan Jiu. 2010;39(2):133–7,142.
27. López M, Ríos-Silva M, Huerta M, et al. Effects of Moringa oleifera leaf powder on metabolic syndrome induced in male Wistar rats: a preliminary study. J Int Med Res. 2018;46(8):3327–3336. doi:10.1177/0300060518781726
28. Shidiq MRH. Efektivitas Tepung Daun Kelor (Moringa Oleifera) Terhadap Kadar Glukosa Darah Tikus Jantan Galur Wistar Yang Diinduksi Aloksan. UPN Veteran Jakarta. 2019.
29. Yasaroh S, Christijanti W, Lisdiana L, Iswari RS. Efek ekstrak daun kelor (Moringa oleifera) terhadap kadar glukosa darah tikus diabetes induksi aloksan. In: Prosiding Semnas Biologi ke-9 Tahun 2021. 2021:224–229.
30. Leone A, Bertoli S, Di Lello S, et al. Effect of Moringa oleifera leaf powder on postprandial blood glucose response: in vivo study on saharawi people living in refugee camps. Nutrients. 2018;10(10):1494. doi:10.3390/nu10101494
31. Vergara-Jimenez M, Almatrafi M, Fernandez M. Bioactive components in Moringa oleifera leaves protect against chronic disease. Antioxidants. 2017;6(4):91. doi:10.3390/antiox6040091
32. Meneses M, Silva B, Sousa M, Sá R, Oliveira P, Alves M. Antidiabetic drugs: mechanisms of action and potential outcomes on cellular metabolism. Curr Pharm Des. 2015;21(25):3606–3620. doi:10.2174/1381612821666150710145753
33. Eid H, Nachar A, Thong F, Sweeney G, Haddad P. The molecular basis of the antidiabetic action of quercetin in cultured skeletal muscle cells and hepatocytes. Pharmacogn Mag. 2015;11(41):74. doi:10.4103/0973-1296.149708
34. Abd El Latif A, El Bialy BES, Mahboub HD, Abd Eldaim MA. Moringa oleifera leaf extract ameliorates alloxan-induced diabetes in rats by regeneration of β cells and reduction of pyruvate carboxylase expression. Biochem Cell Biol. 2014;92(5):413–419. doi:10.1139/bcb-2014-0081
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.