Back to Journals » International Medical Case Reports Journal » Volume 18
Anterior Uveitis From Retained Perfluorocarbon Liquid in the Anterior Chamber, A Case Report
Authors Gomide GA ![]() , Zukerman R, Chen RW
, Zukerman R, Chen RW
Received 16 January 2025
Accepted for publication 6 March 2025
Published 28 March 2025 Volume 2025:18 Pages 439—443
DOI https://doi.org/10.2147/IMCRJ.S517908
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gabriel A Gomide,1 Ryan Zukerman,2 Royce WS Chen1
1Department of Ophthalmology, Edward S. Harkness Eye Institute, Columbia University Irving Medical Center, New York-Presbyterian Hospital, New York, NY, USA; 2Department of Ophthalmology, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA
Correspondence: Royce WS Chen, Edward S. Harkness Eye Institute, Columbia University Medical Center, New York Presbyterian Hospital, 622 W. 168th Street, 18th Floor, New York, NY, 10032, USA, Tel +1-212-305-9535, Email [email protected]
Purpose: Perfluorocarbon liquids (PFCL) are routinely used in vitreoretinal surgery to flatten the retina and push subretinal fluid. Perfluorocarbon liquid retention is a common complication of vitreoretinal surgery. While retention in the posterior chamber can lead to an inflammatory response, PFCL in the anterior chamber has been shown to be generally well tolerated.
Patients and Methods: This report summarizes the findings and treatment of a patient with pathologic myopia and a history of retinal detachment in the left eye repaired with pars plana vitrectomy presenting with one week of blurry vision in the left eye. He was found to have an initial intraocular pressure of 54 mmHg in the left eye along with 1+ conjunctival injection, fine and medium-sized keratic precipitates on the cornea, and 30 cells per high power field. Additionally, there was a retained perfluorocarbon liquid bubble in the anterior chamber from his original retinal detachment repair surgery.
Results: After being started on topical steroids and pressure lowering medications, the patient had persistent inflammation and elevated intraocular pressures. The patient’s anterior uveitis and elevated intraocular pressure resolved with removal of the perfluorocarbon liquid bubble by anterior chamber tap.
Conclusion: Retained PFCL in the anterior chamber can cause anterior uveitis and can be promptly treated by removal.
Keywords: anterior uveitis, PFO, PFCL, retained PFCL
Introduction
Perfluorocarbon liquids (PFCL) are commonly used as an adjunct for vitreoretinal surgery. Developed in the 1980s, PFCLs present many advantages in posterior segment surgery given its high specific gravity. For example, with a specific gravity of between 1.7 and 2.3 g/cm – a higher density than water – PFCLs can flatten the retina and anteriorly push subretinal fluid, significantly reducing the need for posterior drainage retinotomy.1 Similarly, PFCL use offers low viscosity and the most visible optical interface, allowing for easy surgical manipulation and its complete removal at the end of surgery.2 Still, despite these surgical advantages, post-operative retention of PFCL is a common complication of vitreoretinal surgery.2,3
Retained PFCL has been extensively studied. In animal models, intravitreal placement of PFCL for 48 hours produced no adverse effects, and 6-month follow-up showed no adverse histologic changes related to small amounts of residual PFCL.4 In the posterior segment, clinical and histopathologic findings in patients with retained PFCL has demonstrated an inflammatory response – particularly in younger patients with considerable residual vitreous – though this inflammatory response resolves upon removal of PFCL.5 Meanwhile, anterior retention of PFCL in the anterior chamber has been shown to be well-tolerated without adverse effects for periods as long as nine years after surgery.2
Here we report one case of a patient with anterior uveitis in the setting of retained PFCL in the anterior chamber after retinal detachment repair. The presence of the PFCL in the angle, combined with prompt resolution of uveitis following removal of the bubble, strongly suggests that the PFCL incited the inflammation. Although previous reports demonstrated no adverse effects of PFCL in the anterior chamber, we hypothesize in this case that impurities in the PFCL may have contributed to the uveitis.
Case Presentation
A 43-year-old man with a history of pathologic myopia presented to the ophthalmology clinic for evaluation of blurry vision. Seven years prior he had had a retinal detachment in his left eye while living in China that was repaired with a pars plana vitrectomy and silicone oil. Shortly after the primary repair, his retina re-detached and was reattached using gas tamponade. He reported that his repair was complicated by two to three weeks of elevated intraocular pressure (IOP) that required a hospital stay and was treated with drops and an anterior chamber paracentesis. He experienced no further episodes of elevated intraocular pressure, blurry vision, or inflammation prior to presenting to the clinic.
On presentation, he described one week of episodes of blurry vision in his left eye that lasted about an hour. After the initial episode, he was evaluated by an outside ophthalmologist, at which point his IOP was 54 mm Hg in his left eye. At that time, the episodes of blurry vision were thought to be secondary to high intraocular pressures and he was started on latanoprost 0.005% once nightly, brimonidine 0.2% three times daily, dorzolamide 2%/timolol 0.5% twice daily, and oral acetazolamide 250mg four times daily for two days. He was then referred to our clinic for evaluation.
On exam, best-corrected Snellen visual acuity was counting fingers at three feet in the right eye and 20/50 +1 in the left eye, and intraocular pressures were 13 mm Hg and 17 mm Hg respectively. Extraocular movements were full, and pupils were equal, round, and reactive to light and accommodation. Examination of the right eye revealed a 3+ opalescent central nuclear sclerosis cataract. Examination of the left eye revealed 1+ conjunctival injection, fine and medium-sized keratic precipitates on the cornea, 30 cells per high power field, and a well-positioned posterior chamber intraocular lens without prominent lens particles. There was no focal corneal haze. Posterior examination of left eye was notable for a staphylomatous appearance and pigmentary changes consistent with myopic degeneration and prior retinal detachment surgery with no vitreous haze or cells. Gonioscopy of the left eye revealed a PFCL bubble in the inferior angle and peripheral anterior synechiae in the temporal angle (Figure 1). He was then started on prednisolone acetate 1% eye drops every hour in the left eye with planned follow-up in one week.
 |
Figure 1 Slit lamp photo with gonioscopy of the patient’s anterior chamber demonstrating a retained PFCL bubble (black arrow) in the angle. |
At the following visit ten days later, his intraocular pressure in the left eye was 14 mm Hg. Corneal sensation tested at that time was normal. His inflammation was decreasing, with few keratic precipitates on the left cornea, and 10–15 cells per high power field and a PFCL bubble still in the anterior chamber. He was transitioned to prednisolone eye drops six times daily in the left eye for two weeks and then tapered to four times daily for two weeks.
One month later, the patient’s intraocular pressure in the left eye was 15 mm Hg. On examination he still had 5–10 cells per high power field, with a PFCL bubble in the anterior chamber. Given the persistent inflammation, an anterior chamber tap was performed to remove the PFCL bubble in case it may be inciting the uveitis. The PFCL bubble was successfully removed, and he was continued on prednisolone drops four times daily in the left eye with a four-week taper.
At the subsequent visit one month later, the patient had self-discontinued his prednisolone drops after two weeks because of symptom improvement. On examination, his inflammation was markedly decreased, with 2–5 cells per high power field in the anterior chamber and no keratic precipitates on the cornea (Figure 2). Gonioscopy revealed no residual PFCL in the angle or in the anterior chamber. Since that visit approximately 2 years ago, the patient’s inflammatory status has been quiet on all subsequent visits, he is off all anti-inflammatory and pressure drops, and he feels that his eye has returned to its baseline status. He has also now undergone cataract extraction and intraocular lens placement in the right eye.
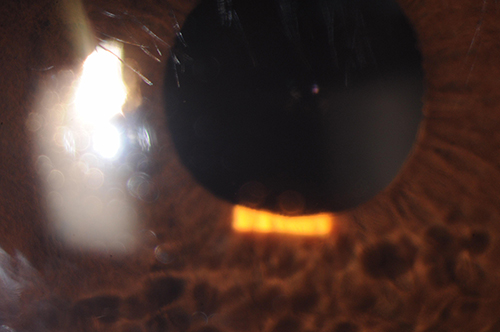 |
Figure 2 Slit lamp photo of the patients anterior chamber demonstrating no anterior chamber cell or flare and resolved keratic precipitates on the cornea. |
Discussion
PFCLs are industrially produced compounds that are not found in nature. While in the United States and North America perfluoro-n-octane (PFO) is the most commonly used PFCL, a wide variety of PFCLs have been used in ophthalmology, including perfluorodecalin (PFD), perfluorotributylamide (PFTB), and perfluorooctylbromide (PFOB), among others. Rates of retention of PFCLs in the anterior chamber after complex retinal detachment surgery vary amongst the different PFCLs, resulting in varying rates of corneal abnormality and elevated IOP.6
While we are not able to fully confirm which specific PFCL was found retained in this patient, we presume it to be the cause of the anterior uveitis given the prompt resolution of inflammation after its removal. Persistent inflammation has not been seen with other cases of retained PFCL in the anterior chamber, suggesting that there may be another component contributing to his presentation.7 Importantly, PFCL-induced ocular inflammation has been tied closely to the purification and chemical stability of PFCLs. As impure formulations of both PFD and PFOB have been shown to cause severe retinal inflammation and detachment, we hypothesize that impurities in the retained PFCL may have contributed to the anterior uveitis.8 Another possible element to this presentation, is the presence of breakdown products of the PFCL. Given the long interval between the patient’s inflammation and the original surgery, the gradual accumulation of breakdown products of PFCL could be responsible, as suggested in other studies with late onset inflammation due to retained PFCL.9 We also surmise that the PFCL bubble may have migrated to the anterior chamber relatively recently before presentation, accounting for the acuity of symptoms.
While the presentation of anterior uveitis with elevated intraocular pressures is often associated with viral etiologies, we believe his clear cornea with normal corneal sensation, resolution of symptoms without antiviral agents, and lack of recurrence for more than two years make this less likely. Medication-induced etiologies for the inflammation are a possible etiology, although less likely as this would not explain the elevated intraocular pressure or vision changes prior to his first presentation. A glaucomatocyclitic crisis is another possible etiology to explain both the elevated pressures and inflammation but would not typically present with a granulomatous uveitis. Auto-immune causes such as HLA-B27 are unlikely due to the lack of recurrence and elevated intraocular pressure. With these considerations in mind, and the prompt resolution of symptoms with the removal of the PFCL bubble, this patient was diagnosed with an acute anterior uveitis due to retained PFCL in the anterior chamber angle.
Abbreviations
PFCL, perfluorocarbon liquids; IOP, intraocular pressure; PFD, perfluorodecalin; PFO, perfluoro-n-octane; PFOB, perfluorooctylbromide.
Data Sharing Statement
The data supporting the findings of this case report are available within the article. However, to protect patient confidentiality, additional data, including clinical images and detailed patient information, are not publicly available. Access to de-identified data may be provided upon reasonable request to the corresponding author and with the appropriate institutional and ethical approvals.
Ethics Approval and Consent to Participate
The creation and publication of this study did not require Institutional Review Board (IRB) approval as it did not meet the criteria for IRB oversight as specified by Columbia University policy.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. The patient was informed that identifying information would be removed or anonymized as much as possible, but that anonymity could not be fully guaranteed. The patient has provided written informed consent for the case details to be published.
Acknowledgments
The authors have no acknowledgements.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Eye Institute under Core Grant P30EY019007 and an unrestricted grant from Research to Prevent Blindness.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Chang S, Ozmert E, Zimmerman NJ. Intraoperative perfluorocarbon liquids in the management of proliferative vitreoretinopathy. Am J Ophthalmol. 1988;106(6):668–674. doi:10.1016/0002-9394(88)90698-8
2. Abboud EB, Al-Falah M. Nine years of retained perfluoro-n-octane in the anterior chamber after retinal detachment repair with no signs of ocular toxicity. Middle East Afr J Ophthal. 2014;21(3):279–282. doi:10.4103/0974-9233.134697
3. Scott IU, Flynn Jr HW, Murray TG, Feuer WJ, Perfluoron Study Group. Outcomes of surgery for retinal detachment associated with proliferative vitreoretinopathy using perfluoro-n-octane: a multicenter study. Am J Ophthalmol. 2003;136(3):454–463. doi:10.1016/S0002-9394(03)00241-1
4. Chang S, Sparrow JR, Iwamoto T, Gershbein A, Ross R, Ortiz R. Experimental studies of tolerance to intravitreal perfluoro-n-octane liquid. Retina. 1991;11(4):367–374. doi:10.1097/00006982-199110000-00001
5. Elsing SH, Fekrat S, Green WR, Chang S, Wajer SD, Haller JA. Clinicopathologic findings in eyes with retained perfluoro-n-octane liquid. Ophthalmology. 2001;108(1):45–48. doi:10.1016/S0161-6420(00)00481-4
6. Scott IU, Murray TG, Flynn Jr HW, Smiddy WE, Feuer WJ, Schiffman JC. Outcomes and complications associated with perfluoro-n-octane and perfluoroperhydrophenanthrene in complex retinal detachment repair. Ophthalmology. 2000;107(5):860–865. doi:10.1016/S0161-6420(00)00076-2
7. Mikhail MA, Mangioris G, Best RM, McGimpsey S, Chan WC. Management of giant retinal tears with vitrectomy and perfluorocarbon liquid postoperatively as a short-term tamponade. Eye. 2017;31(9):1290–1295. doi:10.1038/eye.2017.157
8. Yu Q, Liu K, Su L, Xia X, Xu X. Perfluorocarbon liquid: its application in vitreoretinal surgery and related ocular inflammation. Biomed Res Int. 2014;2014(1):250323. doi:10.1155/2014/250323
9. Cauchi P, Azuara-Blanco A, McKenzie J. Corneal toxicity and inflammation secondary to retained perfluorodecalin. Am J Ophthalmol. 2005;140(2):322–323. doi:10.1016/j.ajo.2005.01.034
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.