Back to Journals » Local and Regional Anesthesia » Volume 13
Ankle Surgery in a Patient with Acute Subdural Hematoma Under Combined Lumbar Plexus and Proximal Sciatic Nerve Block – A Case Report
Received 27 January 2020
Accepted for publication 4 April 2020
Published 15 April 2020 Volume 2020:13 Pages 29—32
DOI https://doi.org/10.2147/LRA.S247413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Utsav Acharya, Ritesh Lamsal
Department of Anaesthesiology, Tribhuvan University Teaching Hospital, Institute of Medicine, Tribhuvan University, Kathmandu, Nepal
Correspondence: Utsav Acharya
Department of Anaesthesiology, Tribhuvan University Teaching Hospital, Institute of Medicine, Tribhuvan University, Kathmandu 44600, Nepal
Tel +977 9843613683
Fax +977 14473059
Email [email protected]
Abstract: Acute subdural hematoma (aSDH) is commonly encountered in the emergency department in patients with traumatic injuries. If the hematoma is small, non-expanding and asymptomatic, it is managed conservatively. However, other injuries sustained during trauma may warrant surgical intervention, during which anesthetic management becomes challenging. There have been reports of rebleeding in patients with aSDH after undergoing surgery under either general or spinal anesthesia. Here we present a case where ankle surgery for tri-malleolar fracture was successfully performed in a patient with traumatic aSDH under combined lumbar plexus and proximal (para-sacral) sciatic nerve block.
Keywords: intracranial hemorrhage, regional anesthesia, traumatic brain injury, ultrasound
Introduction
Acute subdural hematoma is an important cause of death and disability that usually occurs due to tearing of the bridging veins in the subdural space. The decision to choose between operative and conservative management of aSDH is based on several factors such as clot thickness, degree of midline shift, associated brain lesions, Glasgow Coma Scale, neurological findings, clinical stability and the patient’s age.1 In some instances, there can be concomitant injuries like long-bone fractures or chest and abdominal trauma that may necessitate surgery. The anesthetic management of extracranial surgery in the presence of conservatively-managed aSDH is a challenge for anesthesiologists. Here we report a case of a young man who had aSDH along with tri-malleolar ankle fracture, where regional anesthesia with combined lumbar plexus and proximal sciatic nerve blocks came to the rescue. We are not aware of any previously published report that describes this technique for major lower limb surgery in the presence of acute traumatic brain injury.
Case Report
A 35-year-old man was admitted to our hospital with right fronto-parietal aSDH with left ankle tri-malleolar fracture/dislocation after a road traffic accident. After consultation with the neurosurgical team, the aSDH was managed conservatively and the patient was kept under close observation in the high dependency unit. The patient had intense headache that persisted for several days requiring frequent doses of intravenous analgesics; otherwise, his hemodynamic parameters and neurologic profile were stable. He was not able to ambulate because of the skeletal traction applied on the lower limb. After about one week of conservative management, the orthopedic team suggested the fracture should be fixed soon to allow the patient to mobilize and prevent ankle-joint dysfunction, limb wasting and infection. During the preoperative assessment, we explained the patient in detail about the anesthetic plan including regional and general anesthesia, and the risks associated with the surgery. Informed written consent was obtained from the patient, which also included consent for publication of case details and the pictures.
On the day of surgery, standard monitoring was applied in the preoperative holding area. Midazolam 1 mg and fentanyl 50 µg intravenous were given for procedural sedation. Lumbar plexus block (Shamrock technique) was administered on the left side under combined ultrasound (USG) and peripheral nerve stimulator (PNS) guidance with 25 mL 0.375% bupivacaine (Figure 1). Subsequently, proximal (para-sacral) sciatic nerve block was done on the same side under combined USG and PNS guidance with 25 mL 0.375% bupivacaine (Figure 2). Ten minutes later, the adequacy of the block was confirmed after testing for motor and sensory modalities, and the patient was transferred to the operating room. The patient was calm and relaxed throughout the surgery. Hemodynamic parameters were normal throughout, and the patient had no pain complaints. The procedure lasted about three hours, after which the patient was transferred to the recovery room for observation. Two hours later, the patient was transferred to the wards.
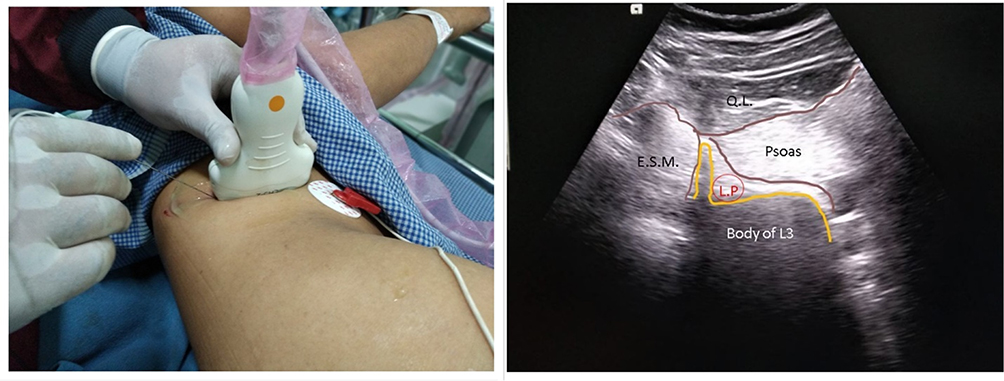 |
Figure 1 The Lumbar Plexus Block. Abbreviations: E.S.M, Erector Spinae Muscle; Q.L, Quadratus Lumborum; L.P, Lumbar Plexus. |
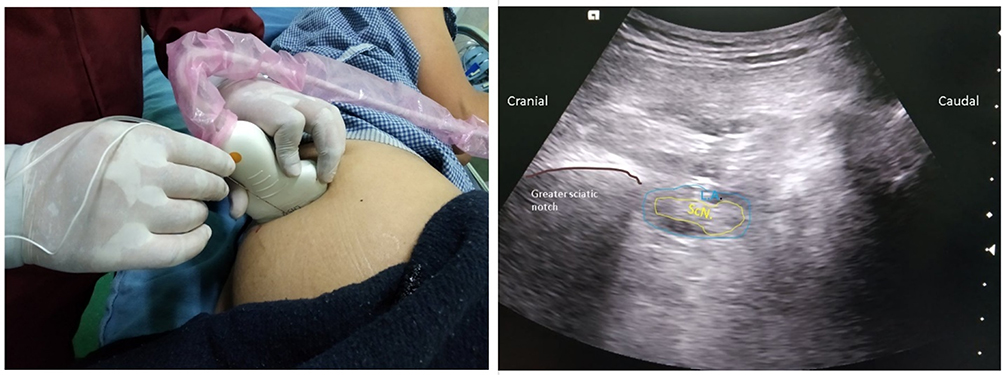 |
Figure 2 Parasacral Sciatic Nerve Block. Abbreviations: ScN, Sciatic Nerve; L.A, Local Anesthetic. |
Discussion
The appropriate timing of long-bone surgeries in the presence of a major systemic injury, including acute intracranial bleeding, remains a matter of clinical debate.2,3 The risks of hematoma expansion and worsening of secondary neurological injury have to be weighed against the risks of prolonged immobilization and permanent joint or limb damage. Most of the times, the decision is based on clinical judgment. Although controversial, there is evidence suggesting that closed ankle fractures should be surgically treated as soon as reasonably possible, as delay leads to increased risk of infectious and functional complications. One retrospective study suggested that ankle fractures should be preferably treated within the first day.4 The presence of concomitant trauma, such as head-injury will obviously influence the timing of surgery as major systemic injuries take precedence over ankle fractures. The decision to operate and timing of surgery in such cases will require a multi-disciplinary approach to decision-making as clear guidelines do not exist.
There is a wide array of techniques for anesthetic management of uncomplicated ankle surgeries. Subarachnoid block (SAB) with or without epidural analgesia is the commonest choice in most cases. General anesthesia (GA) is another option, if SAB is contraindicated or fails. Peripheral nerve/plexus blocks can provide alternative choices; however, they require expertise and technical precision to achieve surgical anesthesia.
The use of central neuraxial block in the presence of intracranial lesions like aSDH is extremely risky. There are several reports of development of both acute and chronic SDH after neuraxial blocks.5–7 In a review of 56 cases of intracranial SDH following neuraxial anesthesia, Cuypers et al8 found that in most of these cases, the patients did not have any predisposing factor. These reports highlight strong safety concerns of using neuraxial anesthesia for surgery in acute intracranial bleed, even though we were not able to find any published report describing its use in such a scenario.
GA is a safer choice than neuraxial anesthesia in the presence of traumatic brain injury (TBI), but is not devoid of risks. Firstly, any hemodynamic fluctuation associated with GA can have a detrimental effect on neurological outcome. There is always the possibility of re-bleeding and hematoma expansion due to hemodynamic disturbances and sympathetic surge associated with the use of general anesthesia. The use of GA also hinders continuous neurologic assessment during surgery, which is possible in an awake patient. Delayed recovery from anesthesia, masking of the occurrence of re-bleeding and deterioration of neurological status are other possibilities. For ankle surgeries, combined sciatic nerve block (popliteal approach) and saphenous nerve block would be the ideal regional anesthesia technique, given the ease of administration and excellent surgical anesthesia below the knee. However, use of tourniquet and the resulting tourniquet pain should also be addressed. If the tourniquet is to be applied on the thigh, then one must consider regional techniques that would cover the thigh as well, such as the lumbar plexus block in combination with proximal sciatic nerve block. The femoral, obturator, sciatic and the lateral femoral cutaneous nerves may be blocked separately, but large volumes of local anesthetic will be required if these nerves are individually blocked. Therefore, we believe lumbar plexus block with proximal sciatic nerve block would be the ideal option in such cases.
The Shamrock technique of USG-guided lumbar plexus block was first described in 2013. Two recent studies describe this method as faster, safer and more comfortable to the patients than conventional lumbar plexus block technique.9,10 When local anesthetic is deposited correctly, this technique reliably blocks transmission from L2, L3 and L4 spinal nerves. With the parasacral sciatic nerve block, all three branches of the sciatic nerve can be adequately blocked. It can be safely performed even by relatively inexperienced physicians.11 Excellent analgesia can be achieved when lumbar plexus and sciatic nerve blocks are combined for lower limb surgeries.
Conclusion
We are not aware of any previous report that describes lumbar plexus block (Shamrock technique) with proximal sciatic nerve block for surgical anesthesia in the presence of intracranial bleeding. The emphasis of this report is on the point that regional anesthesia is an extremely handy tool in any patient with neurological lesions.
Consent for Publication
Informed written consent was obtained from the patient for publication of case details and related images. Institutional approval was not required for publication of case details.
Disclosure
The authors declare no conflicts of interest in this report.
References
1. Bullock MR, Chesnut R, Ghajar J, et al. Surgical management of acute subdural hematomas. Neurosurgery. 2006;58:S16–S24.
2. Velly L, Pellegrini L, Bruder N. Chirurgie périphérique chez le traumatisé crânien grave : précoce ou retardée? [Early or delayed peripheral surgery in patients with severe head injury?]. Ann Fr Anesth Reanim. 2010;29:e183–188. doi:10.1016/j.annfar.2010.06.008. French.
3. Wang MC, Temkin NR, Deyo RA, et al. Timing of surgery after multisystem injury with traumatic brain injury: effect on neuropsychological and functional outcome. J Trauma. 2007;62:1250–1258. doi:10.1097/01.ta.0000215581.50234.56
4. Schepers T, De Vries MR, Van Lieshout EM, et al. The timing of ankle fracture surgery and the effect on infectious complications; a case series and systematic review of the literature. Int Orthop. 2013;37:489–494. doi:10.1007/s00264-012-1753-9
5. Acharya R, Chhabra SS, Ratra M, et al. Cranial subdural haematoma after spinal anaesthesia. Br J Anaesth. 2001;86:893–895. doi:10.1093/bja/86.6.893
6. Gioia S, Mirtella D, Lancia M, et al. Fatal acute intracranial subdural hematoma after spinal anesthesia for cesarean delivery: case report and review of the literature. Am J Forensic Med Pathol. 2019;40:381–385. doi:10.1097/PAF.0000000000000505
7. Metin KM, Guzel II, Oskovi A, et al. Chronic subdural hematoma following spinal anesthesia for cesarean section. J Exp Ther Oncol. 2017;11:97–99.
8. Cuypers V, Van de Velde M, Devroe S. Intracranial subdural haematoma following neuraxial anaesthesia in the obstetric population: a literature review with analysis of 56 reported cases. Int J Obstet Anesth. 2016;25:58–65. doi:10.1016/j.ijoa.2015.09.003
9. Strid JMC, Sauter AR, Ullensvang K, et al. Ultrasound-guided lumbar plexus block in volunteers; a randomized controlled trial. Br J Anaesth. 2017;118:430–438. doi:10.1093/bja/aew464
10. Nielsen MV, Bendtsen TF, Borglum J. Superiority of ultrasound-guided shamrock lumbar plexus block. Minerva Anestesiol. 2018;84:115–121. doi:10.23736/S0375-9393.17.11783-9
11. Ripart J, Cuvillon P, Nouvellon E, et al. Parasacral approach to block the sciatic nerve: a 400-case survey. Reg Anesth Pain Med. 2005;30:193–197. doi:10.1016/j.rapm.2004.08.026
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.