Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Androgenetic Alopecia: Relationship to Anthropometric Indices, Blood Pressure and Life-Style Habits
Authors Danesh-Shakiba M, Poorolajal J ![]() , Alirezaei P
, Alirezaei P ![]()
Received 21 September 2019
Accepted for publication 20 January 2020
Published 5 February 2020 Volume 2020:13 Pages 137—143
DOI https://doi.org/10.2147/CCID.S231940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Mohammad Danesh-Shakiba,1 Jalal Poorolajal,2,3 Pedram Alirezaei4
1School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran; 2Department of Epidemiology, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran; 3Modeling of Noncommunicable Diseases Research Center, Hamadan University of Medical Sciences, Hamadan, Iran; 4Psoriasis Research Center, Hamadan University of Medical Sciences, Hamadan, Iran
Correspondence: Pedram Alirezaei
Psoriasis Research Center, Department of Dermatology, Farshchian Hospital, Mirzadeh Eshghi Street, Hamadan 6517838678, Iran
Tel +98 81 3821 868
Fax +98 8138381591
Email [email protected]
Purpose: The association of androgenetic alopecia (AGA) with cardiovascular risk factors including hypertension, smoking and high body mass index (BMI) has been investigated in several studies. However, the results are discrepant. The aim of the present study was to evaluate the association of AGA with anthropometrics, blood pressure and lifestyle habits.
Patients and Methods: In this case-control study, 256 men with AGA and 256 age-matched healthy controls were evaluated. Systolic and diastolic blood pressures, as well as anthropometric indices were measured. Data on lifestyle habits including smoking, hookah use and alcohol consumption were also collected.
Results: Patients with AGA had significantly lower BMI and lower waist to hip ratio as compared to controls (p = 0.012 and p = 0.002, respectively). Other anthropometrics as well as mean systolic and diastolic blood pressures were not significantly different between the two groups. There was no significant difference between patients and controls in terms of lifestyle habits. Patients with severe AGA (Norwood-Hamilton classification type IV-VII) had significantly higher systolic and diastolic blood pressures as compared to those with mild to moderate AGA (Norwood-Hamilton classification type II, III), but the mean age of the former group was also significantly higher (p < 0.001).
Conclusion: In contrast to some previous studies, our findings did not show a significant association between certain cardiovascular risk factors (such as hypertension and smoking) and AGA. Although lower BMI and lower waist to hip ratio were observed in the patient group, these values were within normal limits and therefore not biologically significant.
Keywords: androgenetic alopecia, anthropometric, blood pressure, life style, smoking
Introduction
Androgenetic alopecia is considered to be the most prevalent form of hair loss,1 and an interaction between genetic and environmental factors (including circulating androgens) is believed to be involved in its etiopathogenesis.2 Some studies have claimed that androgenetic alopecia may be associated with hypertension, metabolic syndrome, central obesity and other cardiovascular risk factors.3–7 For example, it has been shown that body mass index (BMI) of male patients with androgenetic alopecia may be higher than BMI of healthy controls and higher BMI might be correlated with lower level of zinc in hair, which in turn, may have a role in the pathogenesis of androgenetic alopecia.8 There are other studies that show that moderate or severe androgenetic alopecia may be associated with the combination of high BMI and smoking.9 The mechanism by which smoking may induce androgenetic alopecia is not completely recognized, but damage to blood supply of hair follicles, increased oxidative stress and aromatase inhibition (which causes a hypoestrogenic state) may be involved.10 Conversely, some studies have denied any relationship between high BMI or smoking and androgenetic alopecia.11
The association of hypertension and androgenetic alopecia has also been investigated in several studies, but the results are discrepant. Some studies show a strong relationship between androgenetic alopecia and hypertension,12 while others fail to show such association.13
Furthermore, the possible relationship between anthropometric indices (such as waist circumference) and androgenetic alopecia has been investigated in several previous studies, but they also yielded inconsistent results. Some studies have clearly shown that waist circumference (WC) may be higher in patients with androgenetic alopecia as compared to control subjects,14,15 while other studies have claimed that WC may be lower in androgenetic alopecia patients.16
The aim of the present study was to examine the association of androgenetic alopecia with anthropometric indices (BMI, waist and hip circumferences), blood pressure and lifestyle habits (smoking, hookah use and alcohol consumption).
Patients and Methods
Written informed consent was obtained from all study participants and the study protocol was approved by the ethics committee of Hamadan University of Medical Sciences (ethics code: IR.UMSHA.REC.1396.605). The study was carried out in accordance with the Declaration of Helsinki (1975, revised in 2000).
Study Participants
This was a case-control study. Two hundred fifty-six male patients with androgenetic alopecia were recruited from the outpatient clinic of dermatology, Sina Hospital, Hamadan, Iran from January 2018 to September 2018. Two hundred fifty-six age-matched male volunteers without androgenetic alopecia (serving as controls) were also included in the study. Participants’ age and familial history of androgenetic alopecia, as well as smoking (including cigarette and hookah) and alcohol drinking habits were recorded. Those who had smoked cigarettes or hookah in the past 30 days were considered cigarette smokers or hookah smokers, respectively. In addition, those who had used any alcoholic beverages during the past 30 days were considered alcohol consumers. The Norwood-Hamilton scale17 was employed to determine the presence and severity of androgenetic alopecia in all study participants by one single physician. The applied inclusion criteria for patients with androgenetic alopecia were: male individuals aged ≥20 years, Norwood-Hamilton scale ≥ II. The control group was also selected from ≥20 year-old male subjects without androgenetic alopecia. The applied exclusion criteria were as follows: administration of androgens, anti-androgens, systemic corticosteroids, thyroid hormones and anti-hair loss medications since 3 months ago, history of any illness or surgery or accident that required hospitalization during the last 3 months, thyroid diseases, cushing disease, diet-induced weight loss during the last 3 months, history of malignancy and history of liposuction or other body contouring procedures that may have effects on hip or waist circumference.
Anthropometric and Blood Pressure Measurements
All anthropometric measurements were carried out by the same physician. Weight and height were measured with light clothes and barefoot on a column scale with height rod (Seca, Hamburg, Germany). Weight was recorded to the nearest 100 g and height was measured to the nearest 0.5 cm with the patient’s feet together and bare. For Body Mass Index (BMI) calculation, weight (in kilograms) was divided by the square of height (in meters squared). Waist and hip circumferences were obtained with a flexible tape measure. In order to measure waist circumference, midway between the lowest margin of the rib cage and the top of iliac crest was considered at the end of patient’s normal expiration. Hip circumference was measured at the level of maximum protrusion of the buttocks.
Blood pressure of each subject was taken twice using a mercury sphygmomanometer in seated position after 20 mins of rest, and the average of two measurements was recorded. High blood pressure was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg.
Statistical Analysis
Statistical analysis was performed using SPSS version 16.0 software (SPSS Inc., Chicago, IL, USA). Quantitative variables were demonstrated as mean ± standard deviation. Frequency and percentage were used to summarize qualitative variables. Independent samples t-test was applied to compare means between the two groups (patients and controls). Chi-square test was used to examine the association between categorical variables. The level of statistical significance was set at p < 0.05.
Results
A total of 256 patients, as well as 256 age-matched healthy individuals (as control subjects) were included in the study. There was no statistically significant difference between mean age of patients and control subjects (38.33 ± 8.85 years versus 38.40 ± 8.59 years, respectively. P = 0.935).
In patients’ group, there was a positive family history of androgenetic alopecia in first degree relatives of 124 patients (48.4%) and second-degree relatives of 43 patients (16.8%), while 89 patients (34.8%) did not have positive family history. In controls’ group, 22 (8.6%) had positive family history of androgenetic alopecia in their first degree relatives and 40 (15.6%) in their second-degree relatives, while the remaining 194 (75.8%) had no positive family history. There was a statistically significant difference between patients and controls in terms of positive family history (p < 0.001).
Mean values of BMI, waist circumference (WC) and hip circumference (HC) in patients were 23.13 ± 3.43 kg/m2, 88.16 ± 11.06 cm, and 105.46 ± 9.79 cm. In control subjects, mean values of BMI, WC and HC were as follows: 23.86 ± 3.09 kg/m2, 89.66 ± 10.10 cm and 106.58 ± 9.01 cm. The difference between mean values of BMI was statistically significant (p = 0.012). However, mean values of WC and HC were not significantly different between the two groups (p = 0.110 and p = 0.178, respectively). Waist to hip circumference ratio in controls was significantly higher than patients (0.839 ± 0.037 versus 0.829 ± 0.038, p = 0.002).
There was no statistically significant difference between mean systolic blood pressure of patients and mean systolic blood pressure of controls (115.7 ± 10.5 mm Hg versus 116.8 ± 10.3 mm Hg, p = 0.252). Mean diastolic blood pressure of control subjects was higher than mean diastolic blood pressure of patients, but the difference was not statistically significant (75.9 ± 7.9 mmHg versus 75.4 ± 10.2 mm Hg, p = 0.523). Table 1 summarizes the distribution of anthropometrics and blood pressure values among patients and controls.
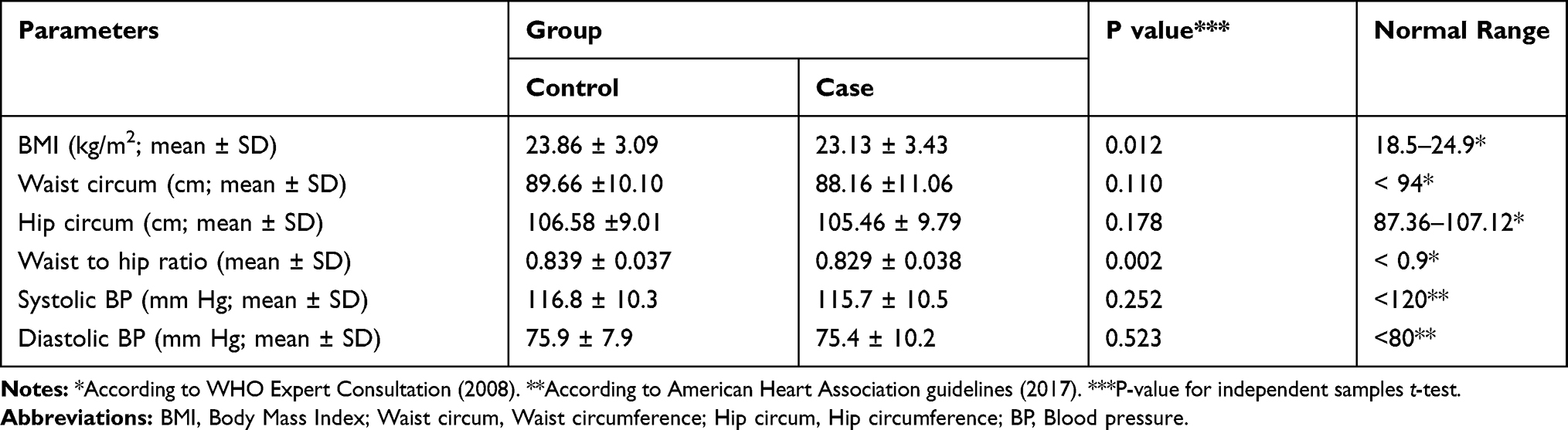 |
Table 1 Distribution of Anthropometric Indices and Blood Pressure in Patients and Controls |
In patients’ group, there were 72 (28.1%) smokers and the remaining 184 (71.9%) were non-smokers. In controls’ group, there were 66 (25.8%) smokers and the remaining 190 (74.2%) were non-smokers. There was no statistically significant difference between the two groups in terms of smoking (p = 0.550).
There were 36 (14%) hookah (smoking water pipe) users in patients with androgenetic alopecia, while in controls’ group, there were 38 (14.8%) hookah (smoking water pipe) users and the difference between the two groups were not statistically significant (p = 0.801).
We found 26 (10.1%) alcohol consumers in patients with androgenetic alopecia, while in controls’ group there were 20 (7.8%) alcohol consumers and the difference between the two groups was not statistically significant (p = 0.353). Table 2 summarizes the distribution of life-style habits among cases and controls.
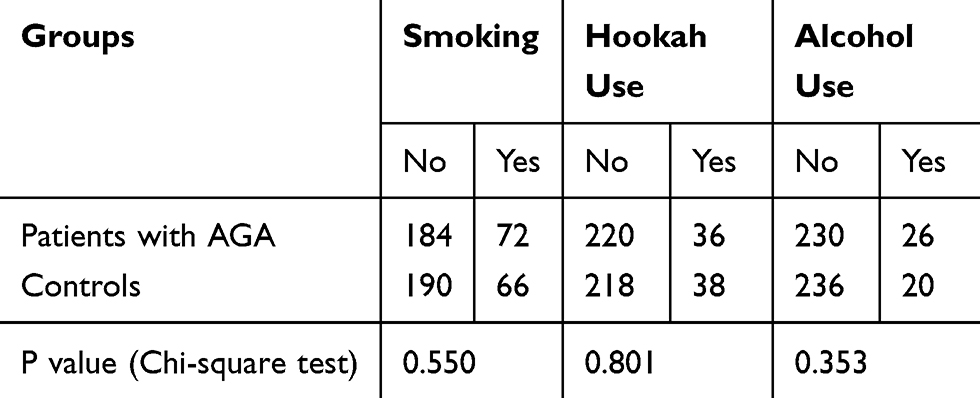 |
Table 2 Distribution of Smoking, Hookah Use and Alcohol Consumption in Patients and Controls |
There were 28 patients (10.9%) with androgenetic alopecia who also had high blood pressure, while in controls’ group there were 26 (10.1%) hypertensive individuals and the difference between the two groups was not statistically significant (p = 0.773).
One hundred fourteen patients (44.5%) had severe hair loss (Norwood-Hamilton classification type IV-VII), and the remaining 142 (55.4%) had mild to moderate hair loss (Norwood-Hamilton classification type II, III). Mean age of patients with severe hair loss was significantly higher than mean age of patients with mild to moderate hair loss (44.40 ± 6.90 years versus 33.46 ± 7.06 years, p < 0.001).
Mean values of BMI, waist circumference, hip circumference and waist to hip ratio were not significantly different between patients with severe hair loss and those with mild to moderate hair loss (p = 0.190, p = 0.279, p = 0.578 and p = 0.085, respectively).
Patients with severe hair loss had significantly higher systolic blood pressures as compared to those with mild to moderate hair loss (120.7 ± 10.4 mm Hg versus 111.8 ± 8.7 mm Hg, p < 0.001). Mean value of diastolic blood pressure was also significantly higher in patients with severe hair loss (78.9 ± 10.7 mm Hg versus 72.6 ± 8.8 mm Hg, p < 0.001). Table 3 summarizes the distribution of age, anthropometric indices and blood pressure among patients with mild to moderate versus severe hair loss.
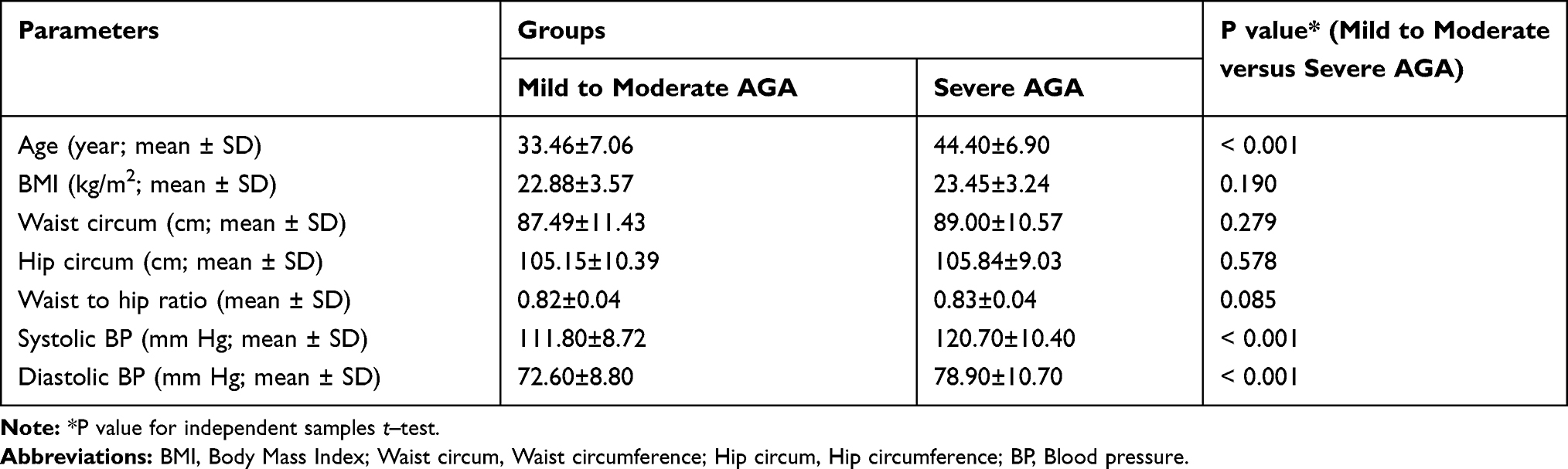 |
Table 3 Distribution of Age, Anthropometric Indices and Blood Pressure Among Patients with Mild to Moderate AGA versus Severe AGA |
Positive family history was significantly more prevalent in patients with mild to moderate hair loss, as compared to patients with severe hair loss (71% versus 57%, p = 0.027). Although smoking and alcohol consuming were not significantly more common in patients with mild to moderate hair loss compared to those with severe hair loss (p = 0.276, p = 0.313, respectively), hookah (smoking water pipe) use was significantly more prevalent in the former group (p < 0.001). Table 4 summarizes the distribution of life-style habits among patients with mild to moderate versus severe hair loss.
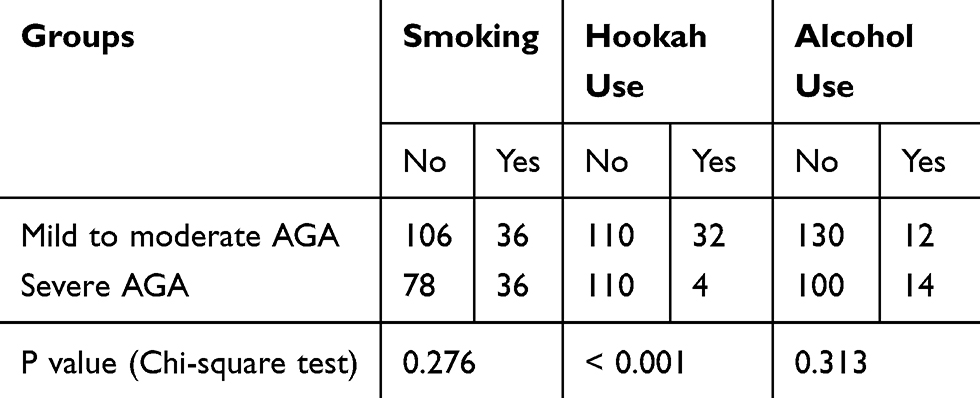 |
Table 4 Distribution of Smoking, Hookah Use and Alcohol Consumption in Patients with Mild to Moderate versus Severe AGA |
Discussion
The findings of the present study argue against the relationship between androgenetic alopecia and certain cardiovascular risk factors. We showed that mean values of BMI and waist to hip ratio were significantly lower in patients with androgenetic alopecia as compared to control subjects. However, the difference observed between cases and controls in terms of BMI and waist to hip ratio may be biologically non-significant. In other words, although statistically significant difference was observed between patients and controls in terms of BMI and waist to hip ratio, this difference is probably of no biological significance. It is also worth mentioning that mean values of BMI in cases and controls are both within normal limits. Patients with severe AGA had significantly higher systolic and diastolic blood pressures as compared to those with mild to moderate AGA, but the mean age of the former group was also significantly higher. We also found that mean values of WC, HC and systolic or diastolic blood pressure are not significantly different between patients and control subjects. Although numerous studies have investigated the probable relationship between androgenetic alopecia and cardiovascular risk factors, the results are discrepant.11,16,18–20 Furthermore, the true pathophysiological mechanism by which androgenetic alopecia and cardiovascular risk factors may be related has not been clearly explained.
We believe that there may be certain explanations for the inconsistency observed between the results of our study and other studies that show a positive association between cardiovascular risk factors and androgenetic alopecia. It should be emphasized that all our study participants were male, while in a study conducted by Yi and colleagues no significant relationship was found between the prevalence of metabolic syndrome (as a cardiovascular risk factor) and androgenetic alopecia in males. They also observed no significant association between each constituent of metabolic syndrome (such as waist circumference and blood pressure) and androgenetic alopecia.21 In order to shed a light on this gender-specific relationship between androgenetic alopecia and metabolic syndrome, we should take a look at the pathophysiology of androgenetic alopecia. Although the true pathogenic mechanism of androgenetic alopecia is not fully recognized, it is currently believed that a polygenic contribution as well as endocrine interaction is involved in its pathogenesis.22,23 The androgen receptor gene on chromosome Xq12 was probably one of the first genes related to androgenetic alopecia,24 but some other genetic loci (such as chromosome 20p11 and chromosome 3q26) have also been recognized.25,26 Interestingly, these loci may have no interaction with androgen receptor locus on X chromosome and therefore contribute to pathogenesis of androgenetic alopecia independently.27 Moreover, several studies have also shown that there may be no association between the etiology of female androgenetic alopecia and androgens.28–30 In other words, the etiopathogenesis of androgenetic alopecia in female patients may be different from males.
Although there are several studies that have investigated the link between certain cardiovascular risk factors and androgenetic alopecia, the results are not consistent. A recent case-control study conducted by Vora and colleagues has demonstrated that the prevalence of abdominal obesity, hypertension and smoking is significantly higher among male patients with early-onset androgenetic alopecia as compared to controls. However, mean values of BMI and WC were not significantly different between patients and controls. The investigators concluded that the risk factors for cardiovascular disease are more prevalent among males with early-onset androgenetic alopecia.3 In another study conducted by Vayá and colleagues on 50 male patients with early-onset androgenetic alopecia, it was demonstrated that the prevalence of metabolic syndrome or its components was not significantly different between patients and controls. They also found no statistically significant difference between patients and controls in terms of insulin resistance, lipid levels (triglyceride, total cholesterol and HDL cholesterol) or hormone levels (sex hormone binding globulin, testosterone and free androgen index). However, they demonstrated that patients with early-onset androgenetic alopecia have increased levels of C-reactive protein and lipoprotein(a).13 It can be concluded that the increased risk of cardiovascular disease in patients with androgenetic alopecia may be due to factors other than insulin resistance, increased lipid levels, metabolic syndrome or its components. In another study conducted by Ozbas Gok and colleagues, no significant difference was observed between patients with androgenetic alopecia and controls in terms of weight, BMI, triglyceride, total cholesterol, LDL, HDL and diastolic blood pressure. They even found that mean values of waist circumference and fasting blood glucose level were significantly higher in controls as compared to patients. However, in patients with androgenetic alopecia, mean value of systolic blood pressure was significantly higher.16 A recent study conducted by Chung and colleagues showed that early-onset androgenetic alopecia may have no significant association with certain cardiovascular risk factors such as hypertension, increased waist circumference, BMI or serum lipid levels.31 Strikingly, the findings of our study showed that patients with androgenetic alopecia may have lower BMI and waist to hip ratio as compared to healthy controls. This finding may be attributable to confounding variables, such as exercise habits. In fact, a recent study conducted by Choi and colleagues has demonstrated that patients with androgenetic alopecia have more physical activity than normal population.32 However, there is not sufficient evidence supporting this hypothesis. Hence, it is difficult to definitely accept or reject it.
Several studies have also investigated the probable association between risk habits (such as smoking and alcohol consumption) with androgenetic alopecia. In a study conducted by Fortes and colleagues, it was demonstrated that high BMI (25 or more) and smoking may be associated with moderate or severe androgenetic alopecia. However, no such association was found between wine consumption and androgenetic alopecia.9 In another study conducted by Park and colleagues, it was shown that smoking and drinking are more prevalent in patients with androgenetic alopecia, as compared to controls. They also showed that with increasing the severity of androgenetic alopecia, the rate of smoking (but not drinking) also increased. The true pathophysiologic mechanism by which smoking may cause hair loss is not fully clarified. However, it has been suggested that local ischemia due to vasoconstriction, DNA damage to follicular cells, impaired tissue remodeling and production of pro-inflammatory cytokines may be responsible.33–36 The findings of our study did not confirm a statistically significant association between risk habits (smoking and alcohol drinking) and androgenetic alopecia. Similarly, a study conducted by Salman and colleagues demonstrated no significant association between these habits (smoking and alcohol consumption) and androgenetic alopecia.11
Conclusion
In contrast to some previous studies, the findings of our study did not show a significant association between certain cardiovascular risk factors (such as hypertension and smoking habits) and androgenetic alopecia in male patients. Strikingly, mean values of BMI and waist to hip ratio were even lower in patients with androgenetic alopecia as compared to age-matched healthy controls. This finding may be due to confounding variables such as exercise habits. Further studies considering these variables are therefore recommended.
Acknowledgments
This study was done based on the approved MD thesis of the first author (Mohammad Danesh-Shakiba), under the supervision of Vice-Chancellor for Research and Technology of Hamadan University of Medical Sciences, Hamadan, Iran (thesis No. 9609215874). We would like to thank the Vice-Chancellor for Research and Technology of Hamadan University of Medical Sciences for thesis approval. The authors also thank all patients for their participation in the study.
Disclosure
The authors declare no conflicts of interest.
References
1. Blume-Peytavi U, Blumeyer A, Tosti A, et al. S1 guideline for diagnostic evaluation in androgenetic alopecia in men, women and adolescents. Br J Dermatol. 2011;164(1):5–15. doi:10.1111/bjd.2010.164.issue-1
2. Ellis JA, Sinclair R, Harrap SB. Androgenetic alopecia: pathogenesis and potential for therapy. Expert Rev Mol Med. 2002;4(22):1–11. doi:10.1017/S1462399402005112
3. Vora RV, Kota R, Singhal RR, Anjaneyan G. Clinical profile of androgenic alopecia and its association with cardiovascular risk factors. Indian J Dermatol. 2019;64(1):19–22. doi:10.4103/ijd.IJD_526_16
4. Swaroop MR, Kumar BM, Sathyanarayana BD, Yogesh D, Raghavendra JC, Kumari P. The association of metabolic syndrome and insulin resistance in early-onset androgenetic alopecia in males: a Case-Control Study. Indian J Dermatol. 2019;64(1):23–27. doi:10.4103/ijd.IJD_724_16
5. Bakry OA, El Farargy SM, Ghanayem N, Soliman A. Atherogenic index of plasma in non-obese women with androgenetic alopecia. Int J Dermatol. 2015;54(9):e339–e344. doi:10.1111/ijd.2015.54.issue-9
6. Agac MT, Bektas H, Korkmaz L, et al. Androgenetic alopecia is associated with increased arterial stiffness in asymptomatic young adults. J Eur Acad Dermatol Venereol. 2015;29(1):26–30. doi:10.1111/jdv.2014.29.issue-1
7. Lotufo PA, Chae CU, Ajani UA, Hennekens CH, Manson JE. Male pattern baldness and coronary heart disease: the Physicians’ Health Study. Arch Intern Med. 2000;160(2):165–171. doi:10.1001/archinte.160.2.165
8. Ozturk P, Kurutas E, Ataseven A, et al. BMI and levels of zinc, copper in hair, serum and urine of Turkish male patients with androgenetic alopecia. J Trace Elem Med Biol. 2014;28(3):266–270. doi:10.1016/j.jtemb.2014.03.003
9. Fortes C, Mastroeni S, Mannooranparampil TJ, Ribuffo M. The combination of overweight and smoking increases the severity of androgenetic alopecia. Int J Dermatol. 2017;56(8):862–867. doi:10.1111/ijd.2017.56.issue-8
10. Su LH, Chen TH. Association of androgenetic alopecia with smoking and its prevalence among Asian men: a community-based survey. Arch Dermatol. 2007;143(11):1401–1406. doi:10.1001/archderm.143.11.1401
11. Salman KE, Altunay IK, Kucukunal NA, Cerman AA. Frequency, severity and related factors of androgenetic alopecia in dermatology outpatient clinic: hospital-based cross-sectional study in Turkey. An Bras Dermatol. 2017;92(1):35–40. doi:10.1590/abd1806-4841.20175241
12. Ahouansou S, Le Toumelin P, Crickx B, Descamps V. Association of androgenetic alopecia and hypertension. Eur J Dermatol. 2007;17(3):220–222. doi:10.1684/ejd.2007.0152
13. Vaya A, Sarnago A, Ricart JM, Lopez V, Martinez-Triguero ML, Laiz B. Inflammatory markers and Lp(a) levels as cardiovascular risk factors in androgenetic alopecia. Clin Hemorheol Microcirc. 2015;61(3):471–477. doi:10.3233/CH-141913
14. Gopinath H, Upadya GM. Metabolic syndrome in androgenic alopecia. Indian J Dermatol Venereol Leprol. 2016;82(4):404–408. doi:10.4103/0378-6323.174421
15. Agamia NF, Abou Youssif T, El-Hadidy A, El-Abd A. Benign prostatic hyperplasia, metabolic syndrome and androgenic alopecia: is there a possible relationship? Arab J Urol. 2016;14(2):157–162. doi:10.1016/j.aju.2016.01.003
16. Ozbas Gok S, Akin Belli A, Dervis E. Is there really relationship between androgenetic alopecia and metabolic syndrome? Dermatol Res Pract. 2015;2015:980310. doi:10.1155/2015/980310
17. Norwood OT. Male pattern baldness: classification and incidence. South Med J. 1975;68(11):1359–1365. doi:10.1097/00007611-197511000-00009
18. Arias-Santiago S, Gutierrez-Salmeron MT, Castellote-Caballero L, Buendia-Eisman A, Naranjo-Sintes R. Androgenetic alopecia and cardiovascular risk factors in men and women: a comparative study. J Am Acad Dermatol. 2010;63(3):420–429. doi:10.1016/j.jaad.2009.10.018
19. Bakry OA, Shoeib MAM, El Shafiee MK, Hassan A. Androgenetic alopecia, metabolic syndrome, and insulin resistance: is there any association? A case-control study. Indian Dermatol Online J. 2014;5(3):276–281. doi:10.4103/2229-5178.137776
20. Ellis JA, Stebbing M, Harrap SB. Male pattern baldness is not associated with established cardiovascular risk factors in the general population. Clin Sci. 2001;100(4):401–404. doi:10.1042/cs1000401
21. Yi SM, Son SW, Lee KG, et al. Gender-specific association of androgenetic alopecia with metabolic syndrome in a middle-aged Korean population. Br J Dermatol. 2012;167(2):306–313. doi:10.1111/bjd.2012.167.issue-2
22. Lolli F, Pallotti F, Rossi A, et al. Androgenetic alopecia: a review. Endocrine. 2017;57(1):9–17. doi:10.1007/s12020-017-1280-y
23. Yap CX, Sidorenko J, Wu Y, et al. Dissection of genetic variation and evidence for pleiotropy in male pattern baldness. Nat Commun. 2018;9(1):5407. doi:10.1038/s41467-018-07862-y
24. Ellis JA, Stebbing M, Harrap SB. Polymorphism of the androgen receptor gene is associated with male pattern baldness. J Invest Dermatol. 2001;116(3):452–455. doi:10.1046/j.1523-1747.2001.01261.x
25. Liang B, Yang C, Zuo X, et al. Genetic variants at 20p11 confer risk to androgenetic alopecia in the Chinese Han population. PLoS One. 2013;8(8):e71771. doi:10.1371/journal.pone.0071771
26. Hillmer AM, Flaquer A, Hanneken S, et al. Genome-wide scan and fine-mapping linkage study of androgenetic alopecia reveals a locus on chromosome 3q26. Am J Hum Genet. 2008;82(3):737–743. doi:10.1016/j.ajhg.2007.11.014
27. Hillmer AM, Brockschmidt FF, Hanneken S, et al. Susceptibility variants for male-pattern baldness on chromosome 20p11. Nat Genet. 2008;40:1279–1281. doi:10.1038/ng.228
28. Redler S, Tazi-Ahnini R, Drichel D, et al. Selected variants of the steroid-5-alpha-reductase isoforms SRD5A1 and SRD5A2 and the sex steroid hormone receptors ESR1, ESR2 and PGR: no association with female pattern hair loss identified. Exp Dermatol. 2012;21(5):390–393. doi:10.1111/exd.2012.21.issue-5
29. Schmidt JB, Lindmaier A, Trenz A, Schurz B, Spona J. Hormone studies in females with androgenic hairloss. Gynecol Obstet Invest. 1991;31(4):235–239. doi:10.1159/000293166
30. Cousen P, Messenger A. Female pattern hair loss in complete androgen insensitivity syndrome. Br J Dermatol. 2010;162(5):1135–1137. doi:10.1111/bjd.2010.162.issue-5
31. Chung H-C, Choe SJ, Lee S, Oh -S-S, Lee W-S. Medical comorbidities and the onset of androgenetic alopecia: a population-based, Case-Control Study. Ann Dermatol. 2018;30(2):251–252. doi:10.5021/ad.2018.30.2.251
32. Choi J, Jun M, Lee S, Oh SS, Lee WS. The association between exercise and androgenetic alopecia: a Survey-Based Study. Ann Dermatol. 2017;29(4):513–516. doi:10.5021/ad.2017.29.4.513
33. Trueb RM. Effect of ultraviolet radiation, smoking and nutrition on hair. Curr Probl Dermatol. 2015;47:107–120.
34. Liu CS, Kao SH, Wei YH. Smoking-associated mitochondrial DNA mutations in human hair follicles. Environ Mol Mutagen. 1997;30(1):47–55. doi:10.1002/(SICI)1098-2280(1997)30:1<47::AID-EM7>3.0.CO;2-9
35. D’Agostini F, Balansky R, Pesce C, et al. Induction of alopecia in mice exposed to cigarette smoke. Toxicol Lett. 2000;114(1–3):117–123. doi:10.1016/S0378-4274(99)00268-4
36. Yin L, Morita A, Tsuji T. Alterations of extracellular matrix induced by tobacco smoke extract. Arch Dermatol Res. 2000;292(4):188–194. doi:10.1007/s004030050476
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.