Back to Journals » International Medical Case Reports Journal » Volume 19
Anatomical Variant or Pathological Anomaly? A Case Report of an Asymptomatic Cardiac Apical Cleft
Authors Posite CM ![]() , Katongole A, Mohamed MS, Omega P, Ongaria J, Ambayo R, Byaruhanga ME, Mutumba M, Usman IM
, Katongole A, Mohamed MS, Omega P, Ongaria J, Ambayo R, Byaruhanga ME, Mutumba M, Usman IM
Received 8 December 2025
Accepted for publication 13 February 2026
Published 18 February 2026 Volume 2026:19 587320
DOI https://doi.org/10.2147/IMCRJ.S587320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Charles Malisaba Posite,1– 3 Abdul Katongole,4 Mahad Said Mohamed,1 Phillip Omega,5 Joseph Ongaria,4 Richard Ambayo,4 Moses Elly Byaruhanga,4 Male Mutumba,4 Ibe Michael Usman6
1Department of Pathology, Kampala International University, Ishaka, Uganda; 2Faculty of Medicine, Université Catholique du Graben, Butembo, Democratic Republic of the Congo; 3Department of Planetary Health and Climate Resilience Lab, EarthRoost+, Beni, Democratic Republic of the Congo; 4Department of Forensic Medicine, Kampala Capital City Authority, Kampala, Uganda; 5Department of Pathology, Makerere University, Kampala, Uganda; 6Department of Anatomy, University of Rwanda, Butare, Rwanda
Correspondence: Charles Malisaba Posite, Email [email protected]
Background: Congenital cardiac malformations are the most common birth defects, with a global prevalence of approximately 8 per 1000 live births. While most are symptomatic, a small subset of structural variants can remain clinically silent. We report a rare case of a deep apical cleft, an incidental and benign post-mortem finding that must be differentiated from clinically significant pathologies such as left ventricular non-compaction cardiomyopathy, ventricular diverticula, or aneurysms.
Case Presentation: During an autopsy of a 38-year-old African male, deceased from a road traffic accident, a deep, V-shaped cleft was discovered at the anterior cardiac apex, measuring 4.2 cm in length and 1.5 cm in depth. The heart was otherwise grossly normal, with no evidence of hypertrophy, septal defects, or vascular anomalies. The patient had no prior history of cardiac symptoms.
Conclusion: The isolated cardiac apical cleft in this asymptomatic adult is a rare anatomical variant, likely a benign developmental anomaly. This case highlights the critical importance of meticulous post-mortem examination and anatomical knowledge to distinguish between a harmless congenital variant and a pathological condition, serving as a valuable educational case for forensic pathologists and cardiac specialists.
Keywords: cardiac cleft, apex cordis, anatomical variant, post-mortem, congenital heart anomaly, case report
Introduction
Congenital cardiac malformations are the most common birth defects, with a global prevalence estimated at approximately 8 per 1000 live births.1–3 While a significant portion of these anomalies, such as septal defects and malformations of the great vessels, are clinically evident in infancy, a small subset of structural variants can remain clinically silent throughout a patient’s life.4,5 These incidental findings pose a unique diagnostic challenge, particularly in the post-mortem setting where there is no opportunity for live imaging or symptom correlation.3,4
We present an extremely rare case of an isolated, asymptomatic cleft at the cardiac apex. This anomaly is distinct from more clinically significant pathologies, including left ventricular non-compaction cardiomyopathy (LVNC), which is characterized by extensive trabeculations and deep inter-trabecular recesses, as well as ventricular diverticula or aneurysms, which involve outpouchings of the ventricular wall.4,5
The significance of this case extends beyond its rarity. It serves as a crucial teaching example for forensic pathologists, radiologists, and cardiac surgeons, emphasizing the importance of differentiating between benign anatomical variants and potentially life-threatening pathologies.
Case Presentation
A 38-year-old Black African male, with an estimated height of 1.75 meters and weight of 78 kilograms, was the subject of a post-mortem examination at the Kampala Capital City Mortuary following his demise from a fatal road traffic accident. The external examination revealed extensive blunt force trauma consistent with the circumstances of death, with no external evidence of cardiovascular disease.
Internal examination of the thoracic cavity revealed a heart of normal size and weight for the subject’s build, weighing approximately 310 grams. The pericardium was intact and there was no pericardial effusion. The epicardial surface was smooth and glistening. A notable and isolated anatomical anomaly was identified at the cardiac apex. The apex presented with a deep, V-shaped cleft measuring 4.2 cm in length and approximately 1.5 cm at its maximum depth. The cleft was oriented longitudinally along the anterior aspect of the apex, aligned with the terminal portion of the anterior interventricular groove (Figure 1). The myocardium surrounding the cleft was well-formed, firm, and did not show any signs of hypertrophy or thinning.
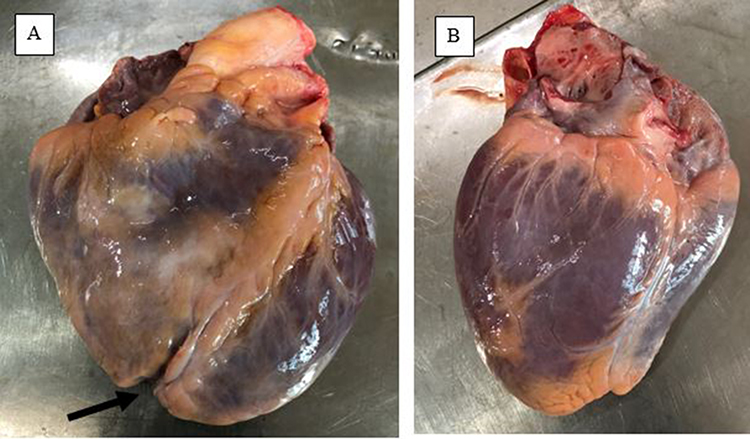 |
Figure 1 The anterior aspect of the heart with an aperture at the cardiac apex (Black arrow in (A)) versus the posterior aspect of the heart (B). |
Subsequent dissection revealed no intracardiac or great vessel anomalies. The right and left ventricles were of normal size, and the interventricular septum was intact and without any defects. The ventricular wall thickness was within normal limits (left ventricular wall: 1.1 cm, right ventricular wall: 0.3 cm). The atrial septum was also intact, with a fully closed fossa ovalis. The pulmonary artery and aorta originated from their correct respective ventricles in their usual anatomical positions. All four valves-tricuspid, mitral, aortic, and pulmonary-were grossly normal, with supple leaflets and no evidence of vegetation or sclerosis (Figure 2). The coronary arteries were patent, with no evidence of atherosclerotic plaque. Both the foramen ovale and ductus arteriosus were fully obliterated, a finding consistent with adult anatomy. However, the histological examination was not performed to rule out microscopic abnormalities such as myocardial fibrosis or inflammation. All other major organs, including the lungs, liver, and kidneys, were unremarkable. A detailed inquiry with the deceased’s family confirmed the absence of any prior cardiac symptoms, including syncope, dyspnea on exertion, or chronic fatigue. The individual was reported to have maintained an active lifestyle without any limitations.
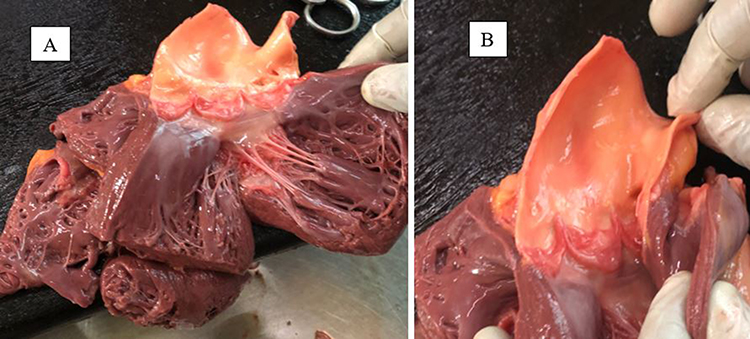 |
Figure 2 Heart cavities with intact septa (A) and unremarkable pulmonary and aortic arteries (B). |
Discussion
The morphological finding of a cleft at the cardiac apex is an exceptionally rare condition.6–8 It must be carefully differentiated from other, more clinically significant anatomical and pathological entities. A deep apical cleft could potentially be confused with conditions such as left ventricular diverticulum, aneurysm, or the clefts seen in LVNC.4,5 However, the presence of well-formed, non-trabeculated myocardium and the absence of any communication with the ventricular chamber effectively rule out diverticulum or aneurysm. Furthermore, the absence of extensive trabeculations or inter-trabecular recesses that are characteristic of LVNC, along with the patient’s asymptomatic life history, reinforces the conclusion that this was a benign anatomical variant.3,4
While the nomenclature varies between “bifid apex” and “apical cleft,” reported cases in world literature remain sparse, often appearing as isolated clinical case reports rather than systematic series. Historically, cardiac bifid apices have been associated with more complex congenital syndromes or ectopia cordis; however, the isolated, asymptomatic apical cleft in an otherwise normal heart-as seen in our case-is significantly rarer.9–11 Most recent documentations of such anomalies have been clinical findings identified via imaging, including ultrasound scan, Multidetector Computed Tomography (MDCT) or cardiac Magnetic Resonance Imaging (MRI).11–13 Despite these clinical advances, a distinct research gap exists in the forensic literature. There is a profound lack of post-mortem and autopsy-based reports documenting the macroscopic appearance of isolated apical clefts, leading to a potential risk of misinterpretation during forensic investigations of sudden death or trauma.
The embryological basis for such an anomaly is hypothesized to be an incomplete fusion of the apical myocardial segments during ventricular septation and remodeling. Unlike septal defects, which involve the failure of a specific septum to form or close, this finding appears to be a localized failure of the apical myocardial walls to completely merge, creating an external cleft with no internal communication.2,4,7
In a clinical setting, distinguishing an isolated apical cleft from more serious pathologies requires a multi-modal imaging approach. On echocardiography, an apical cleft appears as a distinct V-shaped indentation; unlike a left ventricular diverticulum, it lacks a narrow neck and does not show synchronous contraction with the ventricle. On MDCT and Cardiac MRI, the key diagnostic feature is the integrity of the myocardium; a benign cleft is characterized by a well-defined, smooth-walled indentation of the epicardium with preserved myocardial thickness, whereas LVNC would display a thickened, two-layered myocardium with a high non-compacted to compacted ratio (>2.3 in diastole) and deep inter-trabecular recesses.11,13 Crucially, during contrast-enhanced imaging, an apical cleft will show no communication between the ventricular chamber and the cleft itself, and no evidence of late gadolinium enhancement, which helps rule out apical aneurysms or localized scarring. Recognizing these “negative” findings-the absence of trabeculation, communication, and dyskinesis-is essential for avoiding the misdiagnosis of this benign variant as a cardiomyopathy.11,12,14
This case is of significant value to radiologists, cardiac surgeons, and forensic pathologists. In a clinical or radiologic setting, such a finding might be misinterpreted as a pathological process, leading to unnecessary and invasive diagnostic procedures. For the forensic pathologist, it provides a crucial example of a benign variation that must be distinguished from a potential cause of death. It underscores the importance of a comprehensive post-mortem examination to establish a clear cause of death, especially when incidental findings are present.
Study Limitations
Despite the clinical and forensic insights provided by this case, several limitations must be acknowledged. First, because the apical cleft was identified during a post-mortem examination following a traumatic event, no pre-mortem functional data-such as echocardiographic strain imaging or cardiac MRI flow dynamics-were available to correlate the anatomical structure with the patient’s live cardiac physiology. Second, while the patient was reportedly asymptomatic, the lack of a comprehensive longitudinal medical history or detailed familial screening prevents a definitive exclusion of subclinical hereditary syndromes. Finally, genetic testing was not performed; therefore, we cannot rule out rare germline mutations associated with ventricular morphogenesis. As a single-case report, these findings highlight a rare anatomical variant but do not provide data on the broader epidemiological prevalence or long-term prognostic outcomes of isolated apical clefts in this population.
Conclusion
We present a rare case of a deep, isolated cardiac apical cleft identified as an incidental finding during a post-mortem examination of a young, asymptomatic adult. The absence of any other cardiac or systemic pathology and the lack of clinical symptoms throughout the individual’s life confirm this finding as a benign anatomical variant. This report contributes to the understanding of rare cardiac morphology and serves as an important educational case for a variety of medical and surgical specialties.
Ethics Approval
The authors complied with the ethical requirements of Kampala Capital City Mortuary. Institutional ethical approval was not required to publish the case details.
Consent for Publication
Written informed consent for the publication of this case report was obtained from the deceased’s legal next-of-kin. All identifying information was removed to ensure the subject’s anonymity and privacy.
Author Contributions
All authors made a significant contribution to the work reported, took part in drafting and reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Combémorel N, Cavell N, Tyser RCV. Early heart development: examining the dynamics of function-form emergence. Biochem Soc Trans. 2024;52:1579–5. doi:10.1042/BST20230546
2. Romero Flores BG, Guzmán LV, García MS, Lazzarini R. Normal development of the heart: a review of new findings. Bol Med Hosp Infant Mex. 2023;80:79–93. doi:10.24875/BMHIM.22000138
3. Bragança J, Pinto R, Silva B, Marques N, Leitão HS, Fernandes MT. Charting the path: navigating embryonic development to potentially safeguard against congenital heart defects. J Pers Med. 2023;13:1263. doi:10.3390/jpm13081263
4. Thomford NE, Biney RP, Okai E, et al. Clinical Spectrum of congenital heart defects (CHD) detected at the child health clinic in a tertiary health facility in Ghana: a retrospective analysis. J Congenit Cardiol. 2020;4:3. doi:10.1186/s40949-020-00034-y
5. Osarenkhoe OJ, Aiwuyo OH, Osaghae D. Congenital heart diseases: pattern of clinical presentations in children less than 2-years of age in a pediatric practice in southsouth Nigeria. Res J Heal Sci. 2023;11:327–335. doi:10.4314/rejhs.v11i4.5
6. Esmaeilzadeh M, Maleki M, Alizadeasl A, Hashemi A. Bifid Cardiac Apex: A Unique Finding in Left Ventricle. Vol. 8. 2013.
7. Masoura C, Aggeli C, Aznaouridis K, Felekos I, Tousoulis D. Bifid cardiac apex in an old woman. J Cardiovasc Ultrasound. 2017;25:70–71. doi:10.4250/jcu.2017.25.2.70
8. Missouris CG, Okonko DO, Bharucha A, et al. Registry report of structural and functional cardiac abnormalities diagnosed by echocardiography in an asymptomatic population. Postgrad Med J. 2016;92:450–454. doi:10.1136/postgradmedj-2014-133001
9. Gitzel L, Kurtz E, Pusukur B, Dogra S, Mehta N, Patel R. A rare case of bifid left ventricular apex. J Am Coll Cardiol. 2024;83:3514. doi:10.1016/S0735-1097(24)05504-9
10. Ibrahim R, Gaignard S, Patel K, Jokhadar M, Williams BR. An atypical case of isolated symptomatic bifid left ventricle. J Am Coll Cardiol. 2024;83:3224. doi:10.1016/S0735-1097(24)05214-8
11. Sedmera D, Baldini A, Van Den Hoff M. International Cardiovascular Development, Anatomy, and Regeneration (ICDAR) Community Meeting: Prague 2024. J Cardiovasc Dev Dis. 2024;11:390. doi:10.3390/jcdd11120390
12. Sahebjam M, Toofaninejad N. An aberrant papillary muscle causes bifid shape of cardiac apex. J Cardiovasc Echogr. 2023;33:57–58. doi:10.4103/jcecho.jcecho
13. Stabile M, Rispoli AF, Capuozzo M, Ferbo U, Stabile G. Bifid cardiac apex and spongiform cardiomyopathy in fetus with small microdeletion 16p12.2 of paternal origin. Critical points in family communication on 16p12.2 microdeletion. Clin Case Rep. 2023;11. doi:10.1002/ccr3.7602
14. Stougiannou TM, Koutini M, Mitropoulos F, Karangelis D. In vivo models of cardiovascular disease: drosophila melanogaster as a genetic model of congenital heart disease. Biomedicines. 2025;13:2569. doi:10.3390/biomedicines13102569
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.