Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Anatomical Foundations and Clinical Utility of Personalized Free Ilioinguinal Zone Flap for Hand Skin and Soft Tissue Defect Reconstruction
Authors Zhang H, Luo QJ, Ding MC, Qi JW
Received 12 June 2025
Accepted for publication 1 November 2025
Published 3 December 2025 Volume 2025:21 Pages 1645—1656
DOI https://doi.org/10.2147/TCRM.S546752
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Hui Zhang,1 Qiu-Jing Luo,2 Mao-Chao Ding,3 Jian-Wu Qi1
1Department of Hand Microsurgery and Plastic Reconstruction Center, Ningbo No.6 Hospital, Ningbo, 315040, People’s Republic of China; 2Department of Hand Surgery, Yuyao People’s Hospital, Ningbo, 315040, People’s Republic of China; 3Department of Human Anatomy, School of Basic Medical Sciences, Wenzhou Medical University, Wenzhou, Zhejiang, 325035, People’s Republic of China
Correspondence: Jian-Wu Qi, Department of Hand Microsurgery and Plastic Reconstruction Center, Ningbo No.6 Hospital, No. 1059 of Zhongshan East Road, Yinzhou District, Ningbo, 315040, People’s Republic of China, Tel/Fax +86 18906627772, Email [email protected]
Objective: This study aims to explore the anatomical foundations and clinical utility of personalized free ilioinguinal zone flaps for reconstructing skin and soft tissue defects in the hand.
Methods: Anatomical evaluations of the superficial circumflex iliac and the superficial epigastric arteries and veins were performed on 10 cadavers within the inguinal region. Forty-two patients received flap transplants from January 2017 to December 2022 to repair hand tissue defects. Flap areas ranged from 4.0 cm × 6.0 cm to 11.0 cm × 23.0 cm, with arterial anastomosis ensuring vascular connection to recipient sites. Donor sites were directly sutured for closure and healing.
Results: The arteries, sourced from the femoral artery, were consistently identified in all cadavers, with a common trunk found in 70% of cases. Of the 42 transplants, 40 successfully survived, showing a high efficacy rate. Complications included two vascular crises; one was successfully managed, and one led to necrosis. Post-operative observations included soft flap texture, mild bloating, sensory recovery from S2 to S3, and minimal scarring at the donor site.
Conclusion: The personalized free ilioinguinal zone flap is highly effective for repairing hand skin and soft tissue defects, offering advantages like direct donor site closure and reliable vascularity. This method shows great promise in enhancing outcomes in reconstructive hand surgery.
Keywords: free, hand skin tissue defects, ilioinguinal flap, perforator flap, personalized
Introduction
In 1972, Professor Yang Dongyue from China1 and McGregor from Australia2 achieved successful ilioinguinal flap free transplantation. This technique concealed the flap donor area, resulting in minimal damage and enabling a large cutting area. Notably, it allowed for the incorporation of iliac bone into a composite tissue flap for free transplantation, aligning with the principle of “effective repair and reconstruction of the recipient area with minimal loss or damage to the donor area.” Both clinicians and patients favor the repair concept. In addition, in clinical work, we found that in the ilioinguinal flap transplantation, the length and caliber of anastomosis vessels between donor and recipient areas still did not match. These problems reduce the survival rate of ilioinguinal flap transplantation.
Therefore, our study aimed to explore the microanatomical basis of free ilioinguinal flap and observe the clinical efficacy of the personalized repair method formed on this basis in the repair of skin and soft tissue defects of the hand, so as to further provide a theoretical basis for the transplantation and repair of free ilioinguinal flap.
Data and Methods
This study was divided into two parts: exploring the microanatomical structure of ilioinguinal flaps and evaluating the clinical efficacy of personalized flap transplantation. Firstly, we performed microdissection of ilioinguinal region of 5 fresh cadaver samples of 10 cases. Based on the microanatomy of blood supply of the flap, we explored the related anatomy of axial vessels of the flap. On this basis, a personalized flap transplantation method was developed. Subsequently, from January 2017 to December 2022, 42 patients with hand skin tissue defects repaired by personalized ilioinguinal free flap transplantation were included in this retrospective study to explore the clinical efficacy of personalized flap transplantation. This study was approved by the Medical Ethics Committee of Ningbo No.6 Hospital. Patients provided written informed consent for the collection of images and data outlined in this article.
Anatomical Instruction Anatomy of the Skin Flap
Five cohorts comprising 10 freshly obtained adult specimens were provided free of charge by Wenzhou Medical University. Initially, perfusion of lead oxide gelatin was carried out through the femoral artery (FA). Subsequently, three-dimensional vascular casts were acquired via computed tomography (CT), while X-ray angiography was employed to observe the distribution of the flap arteries. Finally, through dissection of the area ventrally above the FA, the superficial circumflex iliac artery (SCIA) was successfully identified. The SCIA was released outward, its entry into the skin flap was meticulously observed, and its vascular course dissected. The anatomical position was marked and the length of the main trunk of the SCIA was measured. The origin, trajectory, and distribution of its vessels were examined, alongside an assessment of the area supplied by the flap, and the dimensions of the flap itself. Subsequently, a slight incision was made in the skin at the groin, slightly medial to the midpoint, in order to identify the superficial epigastric artery (SEA) along with its accompanying vein. The origin, trajectory, and distribution of the vessels were observed. Measurements were taken of the outer diameter at the vessels’ point of origin and the length of their trunks. The data obtained from 10 specimens on each side were recorded and analyzed.
Clinical Data
In this study, a total of 42 patients were included, comprising 25 males and 17 females. Their ages spanned from 18 to 65 years, with a mean age of 35.6 years. Between January 2017 and December 2022, the distribution of defects was as follows: 23 cases of right hand defects, 19 cases of left hand defects, 3 cases of forearm defects, 28 cases of skin defects in the hand alone, and 11 cases of combined skin defects involving the skin of the hand along with finger and metacarpal regions. The dimensions of the skin defects varied from 4.0 cm × 6.0 cm to 11.0 cm × 23.0 cm. Of the cases observed, 41 cases were categorized as sub-acute surgeries, conducted after the trauma site had been cleaned and cleared of obvious secretions;1 case was an elective surgery performed to address a scar contracture defect. The surgical interventions included 27 cases of SCIA flaps, with 10 of these involving SCIA composite flaps with iliac bone. Furthermore, 6 cases utilized SEA flaps, and 9 cases involved combined flaps of SCIA and SEA, including 3 cases of lobulated skin flaps. The size of the skin excised ranged from a minimum of 4.0 cm × 6.0 cm, to a maximum of 11.0 cm × 23.0 cm.
Surgical Approach
Preparation of the Recipient Area
Sub-acute trauma cases underwent an initial phase of debridement to address the trauma. Following the cleaning of the wound and confirmation of the absence of infection, the second-stage surgery was carried out. Elective surgeries involved the excision of scar tissue. The recipient area for the anastomosis of the arterial vein and placement of the free skin graft was determined based on the location of the skin defects on the affected limb in preparation for the surgery.
Harvesting of Skin Flap
Before the harvesting of Skin Flap surgery, experienced ultrasound doctors will mark the location of the flap puncture point. During the operation, the specific type of the flap will be determined based on the size, shape and area of the wound defect after debridement.
Based on the location of the traumatic defect, the crucial aspect for personalized flap design was identifying the FA pulsation point, located 2.5 cm below the inguinal ligament. To accommodate this, the flap cutting area had to be expanded by 1.0 cm in diameter compared to the actual defect area. The distance between the key point and the flap was adjusted based on the actual distance between the blood vessels in the recipient area and the trauma margin. This adjustment ensured a tension-free anastomosis between the vascular tip of the flap and the blood vessels in the recipient area.
SCIA flap: The SCIA flap was delineated utilizing the axis line formed by the trajectory between the key point and the anterior superior iliac spine. The axis line was partitioned, with 2/3 allocated to the upper segment of the flap and the remaining 1/3 to the lower segment. Furthermore, the flap could be extended outward to encompass the furthest extent along the posterior iliac line. The proximal axis of the flap was incised first, initially revealing a thicker superficial circumflex iliac vein. Subsequently, the lower edge of the flap was incised, enabling the elevation of the flap within the superficial layer of the tendon membrane of the external abdominal oblique muscle. The alignment of the SCIA and its accompanying vein within the flap was meticulously scrutinized. Following this examination, the upper edge of the flap was incised, allowing for the complete retrograde liberation of the flap. Care was taken to safeguard the continuity of the SCIA from the origin at the FA and the superficial circumflex iliac vein extending to the saphenous vein, while any branches encountered were ligated appropriately. Finally, the vascular circulation of the flap was assessed. Following the protocol for creating a composite bone flap from the iliac bone, meticulous attention was given to preserving the SCIA, which supplies the deep branch of the iliac bone. The dimensions and extent of the actual bone defect in the recipient area were assessed to guide the cutting of the iliac bone with a bone knife. This procedure ensured the retention of the flap, iliac bone, and the fascial tissues between the iliac bone without any separation, thus guaranteeing continuous blood supply to the iliac bone.
The process of cutting the SEA flap involved lifting the key point vertically upward along the designated axis line. Flaps on either side of this axis line were configured to extend up to the level of the umbilicus. The axis line of the flap tip was incised, and the superficial abdominal wall vein was located. Initially, the lateral edge of the flap was incised to ascertain the alignment of the superficial abdominal wall artery within the flap, and subsequently, the vascular tip was released. Following this, the medial edge of the flap was incised in accordance with the vascular alignment observed within the flap. The flap, along with the vascular tip connected to the FA and the saphenous vein, were completely detached, and the blood flow within the flap was observed to ensure proper circulation.
The dissection of the SCIA and SEA necessitated a systematic approach, beginning with a specific procedure to incise the SCIA. Initially, the tip and the lower edge of the flap were incised, followed by the release of the flap within the superficial layer of the tendon membrane of the external oblique muscle of the abdomen, directed upwards. The alignment of the SCIA and the SEA within the flap was explored to ensure inclusion of both vascular tips. Subsequently, the opposite side of the flap was incised. The flaps and vascular tips were freed retrogradely towards the FA and the great saphenous vein. Observations were conducted to determine whether the two vascular tips exhibited co-dominance. When creating a lobulated flap, it was imperative to ensure separation at the posterior aspect in alignment with the vascular pedicles. This approach ensured that each flap was supplied by a single vessel, and preserved the integrity of their common trunks in instances of shared SCIA and SEA. Additionally, attention was devoted to observing the flap’s hemodynamics.
The incision in the abdominal donor area was meticulously managed to ensure hemostasis. Intracutaneous suturing was performed with the patient positioned in the hip-flexion posture. Careful attention was paid to suturing the subcutaneous soft tissues directly to the external abdominal oblique muscle to eliminate any potential gaps in the wound. Additionally, an internal negative pressure drainage device was inserted to facilitate wound drainage.
Treatment of the Recipient Area and Vascular Anastomosis
Following the dissection of the flap, the tibial vascular artery was flushed with heparinized saline, enabling observation of blood flow from the tibial vascular vein, effectively clearing the stagnant blood. The vascular tip of the flap was positioned near the blood vessels in the recipient area through either subcutaneous or open tunnels. Subsequently, the flap was sutured to the skin at the wound margin. In cases involving a composite tissue flap with an iliac bone, securing was achieved using Kirschner’s needles or plates in the iliac bone, with priority given to addressing the bone defect in the recipient area.
Postoperative Treatment
Postoperatively, the patients underwent a regimen of strict bed rest for a duration of one week in a tranquil environment. Room temperature was maintained within the range of 25—28 °C. The patients received routine administration of anti-inflammatory, anticoagulation, anti-spasmodic, and dilation treatments. Blood flow was monitored on an hourly basis, with immediate intervention for any instances of arteriovenous crises.
Follow-up and Postoperative Functional Evaluation
Patients were discharged from the hospital with scheduled appointments for postoperative checkups. Follow-up visits were scheduled at intervals of 2 weeks, 1 month, 2 months, 3 months, 6 months, 9 months, 12 months, and 24 months after surgery. These appointments entailed comprehensive assessments, including evaluation of flap blood flow, appearance of bloating, sensory recovery, and patients’ satisfaction with both donor-recipient areas. Consistency in the follow-up process was ensured by assigning the same group of physicians to conduct all assessments.
Results
In the examination of 10 ilioinguinal sites dissected from 5 adult specimens, it was observed that the SEA and the SCIA originated directly from the FA in 3 cases (30%). In 7 cases (70%), both arteries shared a common trunk originating from the FA. Notably, none of the dissected specimens exhibited absence of either SEA or SCIA (Figure 1). Additionally, analysis of the 10 ilioinguinal sites.revealed that both the SEA and SCIA originated from the FA in 100% of cases, with no instances of the SCIA originating from the deep FA. The SCIA was found to originate from the lateral aspect of the FA, positioned at an average distance of (6.0±0.5) cm from the anterior superior iliac spine. Originating from either the deep or superficial surface of the broad fascia, the SCIA bifurcated into two branches. Both branches traversed towards the anterior superior iliac spine. The superficial branch provided vascular supply to the skin of the inguinal region, while the deep branch penetrated the periosteum along the anterior margin of the iliac crest.
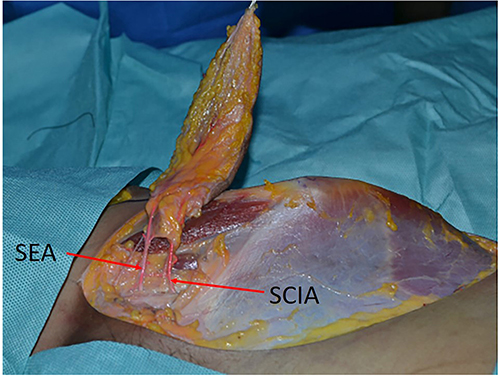 |
Figure 1 Flap dissection in the inguinal region of the specimen. Abbreviations: SCIA, superficial circumflex iliac artery (red arrow); SEA, superficial epigastric artery (red arrow). |
The trunk length of the SCIA averaged (4.0±0.8) cm, exhibiting an external diameter of (1.6±0.5) mm. Notably, the superficial circumflex iliac vein was observed to originate solely from the saphenous vein in 80% of cases (8 sides), while in 20% of the cases (2 sides), it originated in conjunction with the SEA. The length of the vein’s trunk averaged (3.8±0.6) cm, with an external diameter at its origin measuring (2.0±0.6) mm. The SEA was found to originate from the anterior wall of the upper segment of the FA. In 70.0% of cases (7 sides), it shared a common origin with the SCIA, while in 30.0% of cases (3 sides) it originated independently from the anterior wall of the upper segment of the FA. Notably, the superficial pubic artery was observed to diverge into medial and lateral branches at its inception, distinct from the co-stemming pattern exhibited by the SEA. The SEA exhibited an average length of (3.0±0.6) cm, with an external diameter at its origin measuring (1.4±0.4) mm. Regarding the superficial epigastric vein, it was observed to originate independently from the saphenous vein in 80% of the cases (8 sides), while in 20% of cases (2 sides), it shared a common origin with the superficial circumflex iliac vein. The external diameter of the superficial epigastric vein averaged (1.9±0.3) mm (Figure 2). The external diameters of the superficial circumflex iliac artery and vein as well as the superficial epigastric artery and vein, and the length of the vascular pedicle obtained from the dissection of 10 sides of 5 cadaver specimens are presented in Table 1 below. The table showed the diameters of the blood vessels of each flap, which helps in clinical practice by enabling the selection of flaps with appropriate blood vessel diameter.
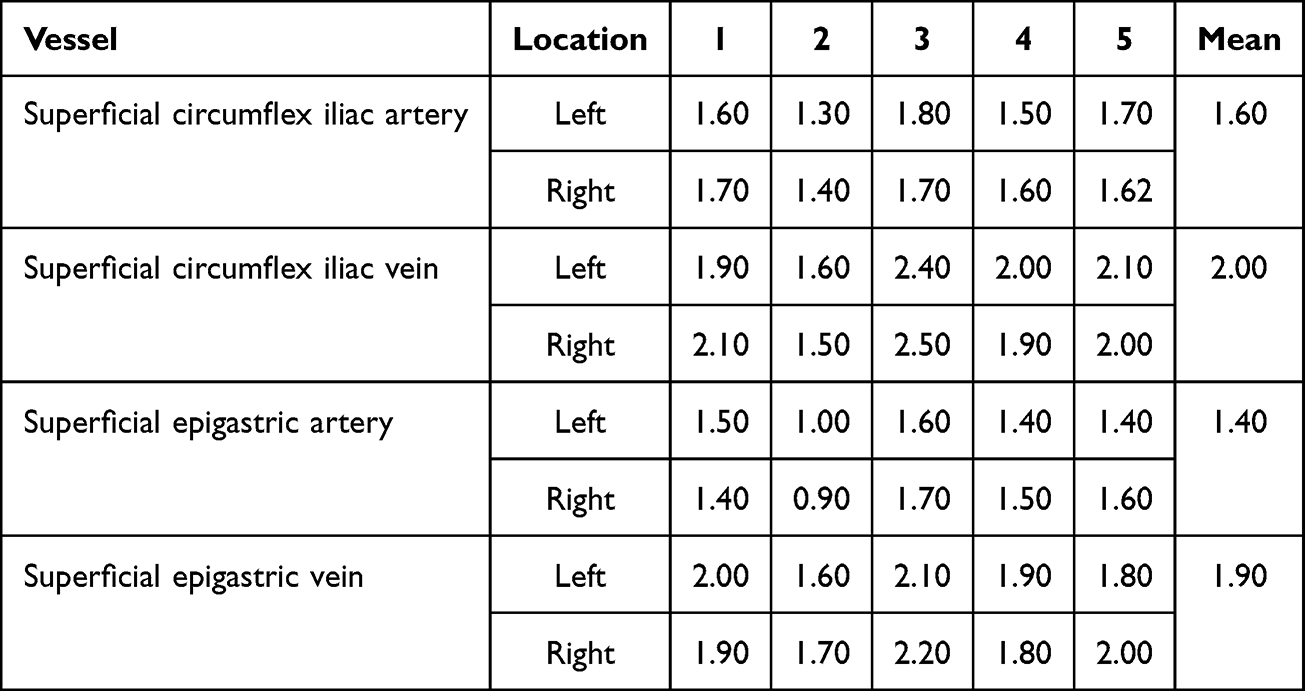 |
Table 1 Flap Vessel Size Anatomical Data (Mm) |
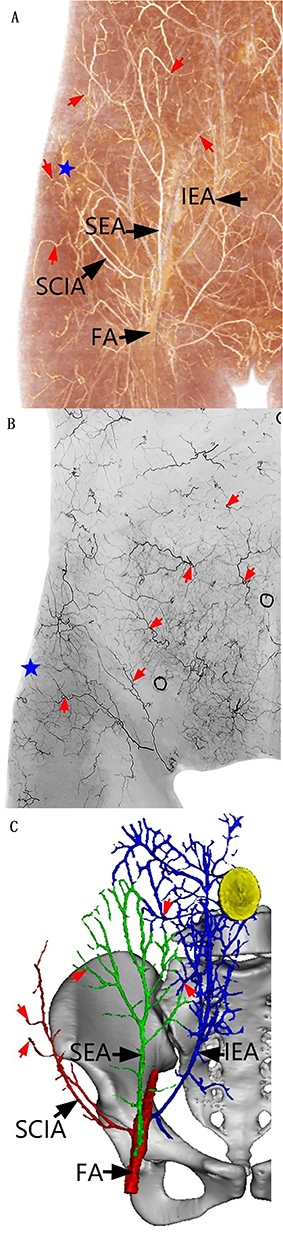 |
Figure 2 (A) Volumetric reconstruction, (B) Three-dimensional reconstruction (C) Skin angiograms. Abbreviations: FA, femoral artery; SCIA, superficial circumflex iliac artery; SEA, superficial epigastric artery; IEA, inferior epigastric artery. Notes: Black arrow, P: perforator (red arrow), blue pentagram: anterior superior iliac spine. |
Vascular anastomosis showed that the flap artery was anastomosed end-to-end with the terminal branch of the radial artery in 2 cases, end-to-side anastomosed with the radial artery in 25 cases, end-to-side anastomosed with the ulnar artery in 7 cases, and end-to-end anastomosed with the common digital artery in 8 cases. Additionally, all cases entailed repair of the spinothalamic superficial iliac vein or the superficial epigastric vein, with simultaneous repair of a companion vein in 13 cases. In the clinical application of this flap, a total of 42 cases were treated, resulting in a survival rate of 40 cases. However, post-surgery, 1 case experienced an arterial crisis and another case encountered a venous crisis. One case underwent surgical exploration, while the other was managed conservatively. Only 1 case survived, albeit with the development of necrotic skin crusting. Subsequent observation during the second stage of crusting revealed that the subcutaneous soft tissue remained viable. Additionally, there was an incidence of a split incision in 1 case, 8 days after the extraction of the combined SCIA and SEA flap. This wound was successfully healed following a two-stage suture, whereas the remaining donor areas healed in a single stage.
During the follow-up period spanning from 6 to 24 months, observations indicated that the flaps exhibited characteristics of softness and slight swelling, accompanied by sensory recovery ranging from grades S2 to S3. A single linear scar persisted in the donor area across all patients, with 11 patients requiring a second-stage flap revision due to flap bloating. Patient satisfaction regarding both the appearance of the donor area and the flap was generally high. Typical cases exemplifying these outcomes are illustrated in Figures 3–6.
 |
Figure 3 Case of the SCIA flap. (A) Preoperative design of the SCIA flap in the left inguinal region; (B and C) Intraoperative separation of the flap; (D) Completely free flap and left dorsal trauma; (E) Intraoperative immediate hemoperitoneum of the flap repair trauma; (F and G) Postoperative follow-up of the flap and scarring of the abdominal donor area after 1 year. |
 |
Figure 4 Case of the SEA flap. (A) Preoperative design of the SEA flap in the right inguinal region; (B and C) Intraoperative separation of the flap; (D) Completely free flap and right hand dorsal trauma; (E) Intraoperative immediate hemoperitoneum of the flap repair trauma; (F) Direct intradermal suture in the abdominal donor area; (G and H) Postoperative follow-up of the flap and scarring of the abdominal donor area after 2 years. |
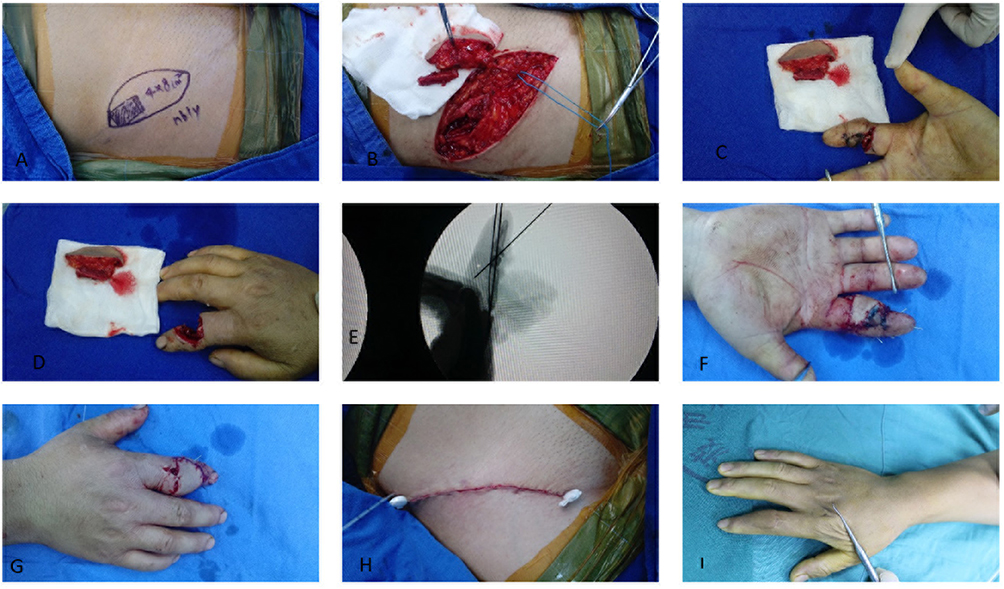 |
Figure 5 Composite flap of the SCIA with iliac bone. (A) Preoperative design of the right inguinal region with iliac bone flap; (B) Intraoperative separation of the flap and iliac bone; (C and D) Complete freeing of the composite flap with iliac bone and the trauma of the right index finger; (E) Intraoperative internal fixation of the iliac bone graft taken from the right index finger; (F and G) Intraoperative immediate hemoperitoneum of the flap repair trauma; (H) Direct intradermal suture in the abdominal donor area; (I) Postoperative follow-up for flap status after 1 year. |
 |
Figure 6 Combined flap. (A) Right hand disfigurement, skin and soft tissue defect; (B and C) Left inguinal region SCIA and SEA leaflet flap design and isolation; (D) Completely free SCIA and SEA lobular flap and right hand trauma; (E and F) Intraoperative flap repair trauma immediate blood flow; (G) Abdominal donor area direct intradermal suture; (H and I) Postoperative follow-up for flap status after 1 year. |
Discussion
Anatomical Basis of the Ilioinguinal Flap
The ilioinguinal zone flap receives its vascular supply from the SCIA and the SEA. These arteries typically originate from the lateral wall of the FA and commonly exhibit co-dominance at their origins, as evidenced by previous studies reporting rates ranging from 39–70%.3 In our present study group, consisting of anatomical specimens, this co-dominance was observed in 70% (7 out of 10) of cases. The vascular pathways of these arteries extend outwardly superior to the anterior superior iliac spine (in the case of the SCIA) and vertically upward (in the case of the SEA), providing vascular nourishment to the respective skin tissues through an extensive network of branching connections. In all cases within our clinical group, both united and lobulated flaps exhibited the co-dominant type of vascular arrangement.
The SCIA exhibits a branching pattern comprising superficial and deep branches along its course. Typically, the superficial branch accompanies the superficial circumflex iliac vein, traversing along the surface of the subcutaneous or adipose layer to provide vascular nourishment the skin. Conversely, the deep branch is consistently present in all cases, following a trajectory similar to that of the superficial branch. The deep branch is distinguished from the superficial branch solely by the presence of the deep fascia. It travels between the fascial layers of the vastus lateralis muscle and the muscularis mucosae, extending towards the slightly lateral aspect of the anterior superior iliac spine. This deep branch serves to nourish the tissues of the iliac bone.4 The venous return system of the flap encompasses the companion veins associated with the SCIA and SEA, along with their corresponding veins. Both the superficial spinous circumflex iliac vein and the superficial epigastric vein eventually converge into the saphenous vein. The saphenous vein typically possesses a thicker outer diameter compared to the companion vein, which tends to be much thinner. Therefore, the saphenous vein primarily serves as the main venous drainage vessel for the flap.5 Based on the anatomical characteristics outlined above, personalized ilioinguinal flaps can be customized to address skin defects of varying sizes, shapes, and locations on the hand, including composite defects involving metacarpal and phalangeal bones. Personalized free superficial circumflex iliac artery perforator (SCIP) or superficial epigastric artery perforator (SEAP) flaps offer viable options for repairing normal-sized skin and soft-tissue defects. These two types of flaps can be utilized individually or in combination to address larger or irregular defects. Moreover, they can also be utilized to create composite tissue flaps, utilizing the SCIA and iliac bone to address composite tissue defects alongside bone defects.
Clinical Applications and Advantages of Personalized Ilioinguinal Flap
In recent years, scholars have been exploring the use of free ilioinguinal flaps supplied by the perforating branch of the SCIA to repair skin defects on the hands and limbs.6–9 They have been investigating the application of SCIA flaps to address composite tissue defects, such as metacarpal bone defects.10 Additionally, successful treatment outcomes have been reported for large skin defects on the hand using lower abdominal united or leaflet flaps.11–13 All these approaches have demonstrated satisfactory curative outcomes. By considering the actual size and shape of traumatic defects on the hand, particularly when combined with metacarpophalangeal defects, the utilization of personalized ilioinguinal area flap free grafting allows for the optimal use of the most discreet abdominal donor area. This approach offers several advantages: (1) The donor area is concealed, allowing for extensive excision without the need for additional skin grafting. Closure with sutures can be achieved by flexing the hip and knee. (2) Supplied by the SCIA and/or SEA, the flap is accompanied by a corresponding superficial vein for efficient venous return. Its superficial location ensures consistent vascular access. (3) As an axial flap, it facilitates convenient dissection, easy separation of vascular tips, and minimal flap cutting time. (4) The flap can be thinned directly before vascular dissection to address issues such as a bloated flap shape while retaining sufficient adipose tissue to fill the traumatic defect as needed. (5) Utilizing the nutrition provided by the deep branch of the SCIA to the iliac bone, a composite bone flap with blood vessels can be harvested and transplanted into the bone defect, thereby promoting fracture healing.
Surgical Improvements and Considerations
Surgical improvements and considerations for this flap include addressing its main drawback, which is the short and thin vascular tip that may not adequately match the length and caliber required for anastomosis with recipient vessels. To overcome this limitation, certain enhancements are necessary: (1) Extension of vascular tip length: Determining the length of the proximal end of the flap and the critical point of the vascular tip should be based on the distance between the trauma site and the recipient vessels. This ensures that the vascular tip of the flap is sufficiently long for a tension-free anastomosis with the recipient blood vessels. (2) Refinement of vascular anastomosis technique: Given the relatively small calibers of the SCIA and SEA, which are slightly smaller than the caliber of the common digital artery and significantly differ from the ulnar and radial arteries, it is crucial to refine the vascular anastomosis technique. Utilizing an end-to-side anastomosis to connect the flap vessels with the ulnar or radial artery proves to be an effective solution to address the inconsistency in vessel caliber between the supplying and receiving areas. This method helps safeguard the ulnar or radial artery from damage while ensuring adequate blood supply to the recipient area.
At the same time, the following points should be noted: (1) When cutting the flap with iliac bone, it is imperative to keep the deep branch of the SCIA intact within the iliac bone. This ensures that the iliac bone retains sufficient soft tissue fascia connected to the flap, thereby maintaining adequate blood supply. (2) After cutting the flap, especially following the creation of a joint or leaflet flap, the donor area can be sutured directly by flexing the hip and knee. Nonetheless, it is critical to advise the patient to keep their hips and knees in a flexed position while in bed for one week post-surgery. Following this period, the patient is recommended to ambulate with a flexed knee for an additional two to three weeks upon rising, to mitigate the risk of incision dehiscence. In this study, there was one case where a patient failed to follow medical advice and got up one week after the operation without bending over and walking. As a result, the abdominal incision experienced cracking; however, it was subsequently healed through suturing. The remaining patients diligently adhered to the doctor’s advice, resulting in no other instances of incision cracking observed.
Conclusion
Therefore, for patients presenting with hand skin and soft tissue defects or combined bone defects, irrespective of the shape and size of the trauma, personalized ilioinguinal free flaps can be employed for one-stage transplantation and repair. This approach embodies the concept of flap micro prosthesis, aiming to achieve “effective repair and reconstruction of the recipient area with minimal loss or damage to the donor area.”
Abbreviations
FA, Femoral artery; SCIA, Superficial circumflex iliac artery; IEA, Inferior epigastric artery; SEA, Superficial epigastric artery; P, Perforator; SCIP, the superficial circumflex iliac artery perforator; SEA, the superficial Epigastric Artery perforator.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki.This study was conducted with approval from the Ethics Committee of Ningbo NO.6 Hospital.A written informed consent was obtained from all participants.
Acknowledgments
The authors are grateful for Xin Wang for obtaining the financial support from.
Author Contributions
Conception and design of the research: Jianwu Qi, Hui Zhang. Acquisition of data: Qiu-Jing Luo, Maochao Ding, Analysis and interpretation of the data: Hui Zhang, Jianwu Qi. Statistical analysis: Maochao Ding, Qiu-Jing Luo. Writing of the manuscript: Hui Zhang. Critical revision of the manuscript for intellectual content: Jianwu Qi. All authors read and approved the final draft. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Ningbo Major Science and Technology Task Research Project, No. 2022Z146; Major Project of Ningbo Medical and Health high-end Team (2022020506); Funded by Ningbo Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation (2024L004).
Disclosure
All authors have contributed significantly to the manuscript and declare that the work is original and has not been submitted or published elsewhere. None of the authors have any financial disclosure or conflict of interest.
References
1. Gu YD. Advocate the use of abdominal flaps for coverage of skin defects of the hand. Chin J Hand Surg. 2009;25(5):257.
2. McGregor IA, Jackson IT. The groin flap. Br J Plast Surg. 1972;25:3–16. doi:10.1016/S0007-1226(72)80003-1
3. Mahdi F, Ebrahim H, Reza FH, et al. The anatomy of superficial inferior epigastric artery flap. Acta Cir Bras. 2008;23(5):429–434. doi:10.1590/S0102-86502008000500007
4. Cédric Z, David H, Ruslan H, et al. The anatomical reliability of the superficial circumflex iliac artery perforator (SCIP) flap. Ann Anat. 2021;234:151624. doi:10.1016/j.aanat.2020.151624
5. M CAR, Koudstaal maarten J, Bulstrode Neil W, et al. Free groin flap in hemifacial volume reconstruction. Br J Oral Maxillofac Surg. 2013;51(4):301–306. doi:10.1016/j.bjoms.2012.09.004
6. Hidehiko Y, Takumi Y, Akitatsu H, et al. Use of the transverse branch of the superficial circumflex iliac artery as a landmark facilitating identification and dissection of the deep branch of the superficial circumflex iliac artery for free flap pedicle: anatomical study and clinical applications. Microsurgery. 2019;39(8):721–729. doi:10.1002/micr.30518
7. Pio HJ. The superficial circumflex iliac artery perforator flap in lower extremity reconstruction. Clin Plast Surg. 2021;48(2):225–233. doi:10.1016/j.cps.2020.12.005
8. Liang OC, Ji L, Xin Z, et al. Repair of multiple hand defects with superficial circumflex iliac artery perforator flap. Injury. 2023;54(10):940–946. doi:10.1016/j.injury.2023.110998
9. Nicolás P, Josefa V, Vanessa O, et al. Extremity reconstruction with superficial circumflex iliac artery perforator free flap: refinements and innovations after 101 cases. J Plast Reconstr Aesthet Surg. 2023;85:1–9. doi:10.1016/j.bjps.2023.06.048
10. Yoshimatsu H, Iida T, Yamamoto T, Hayashi A. Superficial circumflex iliac artery-based iliac bone flap transfer for reconstruction of bony defects. J Reconstr Microsurg. 2018;34(9):719–728. PMID: 29753300. doi:10.1055/s-0038-1651489
11. Yoshimatsu H, Hayashi A, Karakawa R, Yano T. Combining the superficial circumflex iliac artery perforator flap with the superficial inferior epigastric artery flap or the deep inferior epigastric artery perforator flap for coverage of large soft tissue defects in the extremities and the trunk. Microsurgery. 2020;40(6):649–655. PMID: 32539208. doi:10.1002/micr.30620
12. Li Z, Zheng D, Zheng J, Qi W, Qi Q, Liu Y. Free superficial circumflex iliac artery perforator flap with a single-pedicle bilobed design for pediatric multi-digit defect reconstruction. J Orthop Surg Res. 2020;15(1):216. PMID: 32527269; PMCID: PMC7291421. doi:10.1186/s13018-020-01733-3
13. Ou CL, Li J, Zhou X, Luo XC, Zou YG. Repair of multiple hand defects with superficial circumflex iliac artery perforator flap. Injury. 2023;54(3):940–946. doi:10.1016/j.injury.2023.01.016
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.