Back to Journals » International Journal of Women's Health » Volume 18
Analyzing Global Trends in Uterine Prolapse Burden: A Comprehensive Study of Incidence and DALYs Across 204 Countries from 1990 to 2021
Authors Bai J, Zhu L, Zheng Y, Lu C, Liu X, Li D, Zhao X, Guo R ![]() , Wu W
, Wu W ![]()
Received 27 March 2026
Accepted for publication 1 July 2026
Published 10 July 2026 Volume 2026:18 612363
DOI https://doi.org/10.2147/IJWH.S612363
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Jing Bai,1,* Li Zhu,2,* Yuchen Zheng,3 Chang Lu,1 Xinyue Liu,1 Daning Li,3 Xiuliang Zhao,3 Ruixia Guo,1 Wentao Wu3
1Department of Gynecology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, Henan Provincial Chest Hospital (Chest Hospital of Zhengzhou University), Zhengzhou, Henan, People’s Republic of China; 3Department of Cardiac Surgery, Henan Provincial Chest Hospital (Chest Hospital of Zhengzhou University), Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruixia Guo, Department of Gynecology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China, Email [email protected] Wentao Wu, Department of Cardiac Surgery, Henan Provincial Chest Hospital (Chest Hospital of Zhengzhou University), Zhengzhou, Henan, People’s Republic of China, Email [email protected]
Background: Uterine prolapse is a common and debilitating pelvic floor disorder that significantly impairs women’s quality of life worldwide. With global population aging and lifestyle transitions, its disease burden has become increasingly pronounced. However, comprehensive analyses of long-term epidemiological trends, driving factors, and health inequalities across different socioeconomic settings remain limited.
Methods: This study analyzed data from the Global Burden of Disease (GBD) 2021 study, covering 204 countries and territories from 1990 to 2021. Age-standardized incidence and Disability-Adjusted Life Years (DALYs) rates were calculated. Estimated annual percentage changes (EAPCs) were computed to evaluate temporal trends. Decomposition analysis was performed to quantify the contributions of population growth, population aging, and epidemiological changes to DALY changes. Health inequality was assessed using the Slope Index of Inequality (SII) and Concentration Index (CI) across Socio-demographic Index (SDI) quintiles.
Results: Globally, the age-standardized DALYs rate for uterine prolapse was 9.90 per 100,000 in 2021. Incidence exhibited a bimodal peak at 45– 54 years and 90+ years, whereas DALYs increased monotonically with age, peaking in the oldest-old (90+ years). Low and low-middle SDI regions exhibited declining trends, whereas middle, high-middle, and high SDI regions showed increasing trends, with high SDI regions demonstrating a U-shaped resurgence. Decomposition analysis revealed that population growth and aging were the primary drivers of global DALY increases, with epidemiological changes partially offsetting the increase, although this effect varied considerably across SDI levels. Health inequality analysis demonstrated that the burden of uterine prolapse has progressively concentrated among higher SDI populations, with this inequality widening substantially over the past three decades.
Conclusion: The global burden of uterine prolapse has risen over the past three decades, with marked heterogeneity across SDI levels. Interventions should prioritize early screening for midlife women, tiered management for older women, metabolic risk control in high SDI regions, and surgical access in low SDI regions, with resource allocation tailored to national SDI levels and population age structures.
Keywords: uterine prolapse, disease burden, global trends, decomposition analysis, health policy implications
Introduction
Uterine prolapse, a prevalent and debilitating form of pelvic organ prolapse (POP), significantly impacts women’s health on a global scale, causing substantial morbidity and markedly affecting quality of life.1 This condition, characterized by the descent of the uterus into the vaginal canal due to weakened pelvic support structures, manifests with a spectrum of symptoms ranging from mild pelvic discomfort to severe urinary and bowel dysfunction, as well as sexual health issues.2 The clinical consequences of uterine prolapse, including dyspareunia, reduced sexual satisfaction, and sexual dysfunction, are frequently overlooked yet substantially impair quality of life, potentially triggering psychological issues such as anxiety, depression, and marital tension.3
With the global population aging and lifestyles evolving, the burden of uterine prolapse, quantified in Disability-Adjusted Life Years (DALYs), has become increasingly pronounced.4 Over the past three decades, the incidence of uterine prolapse has demonstrated a rising trend, particularly in regions with aging demographics and higher socio-demographic indices (SDIs).5 This escalating burden imposes significant strains on healthcare systems, necessitating a deeper understanding of the underlying factors driving this trend.6 Multiple risk factors contribute to the development and progression of uterine prolapse, including obstetric trauma, age-related tissue degeneration, chronic elevated intra-abdominal pressure due to conditions like chronic cough or constipation, obesity, and genetic predisposition.7 Furthermore, environmental and lifestyle factors, such as multiparity and comorbidities including chronic obstructive pulmonary disease, diabetes, and osteoporosis, further exacerbate the risk and severity of this condition.8
The Global Burden of Disease Study 2021 (GBD 2021), a comprehensive resource for disease burden metrics, offers unique insights into the epidemiology of uterine prolapse across different countries and regions.9 By integrating epidemiological data from 204 countries and territories, the GBD study analyzes the impact of 369 diseases and 88 risk factors on global health.10 The GBD 2021 database, accessible through the Global Health Data Exchange (GHDx) platform, provides a wealth of information, including population registration records, verbal autopsy data, health examination data, demographic survey data, and medical institution datasets.11 This extensive data repository enables systematic and robust analyses of disease trends, facilitating a deeper understanding of the global burden of uterine prolapse.
According to the GBD 2021 study, significant disparities exist in the burden of uterine prolapse across different countries and regions, closely linked to demographic changes, healthcare access, and health policies.12 Systematic epidemiological research is essential to elucidate these trends and guide effective interventions. Prior studies have reported the global burden of pelvic floor disorders, but most have focused on pelvic floor dysfunction as a broad category, with few studies examining the long-term epidemiological trends of a single condition such as uterine prolapse.13–15 A strength of the present study is that, using GBD 2021 data, we systematically analyzed the long-term trends in the incidence and DALYs of uterine prolapse across 204 countries and territories worldwide from 1990 to 2021. More importantly, this study not only describes changes in disease burden but also further applies decomposition analysis to quantify the relative contributions of population growth, population aging, and changes in epidemiological factors to these changes, thereby revealing the drivers of evolving disease burden across regions with different SDI levels. Moreover, through health inequality analysis using the Slope Index of Inequality (SII) and the Concentration Index (CI), we have, for the first time at the global level, quantified the distributional disparities in uterine prolapse burden among countries at different SDI levels and their temporal trends. These analytical dimensions have rarely been addressed in previous studies on the burden of pelvic floor disorders, providing a more precise evidence base for formulating targeted regional health policies and equitable resource allocation. This study investigates global, regional, and national trends in the incidence and DALYs of uterine prolapse from 1990 to 2021, utilizing data from the GBD 2021 study. By incorporating age and SDI into the analysis, this study identifies long-term burden patterns and regional disparities, while age-specific assessments provide evidence for predicting future trends. The findings underscore the need for targeted interventions to address demographic and epidemiological changes, emphasizing the importance of considering regional disparities in health policy formulations to mitigate the disease burden effectively and improve women’s health globally.
Methods
Data Sources and Disease Definition
We extracted epidemiological data from the GBD 2021 via the GHDx platform (https://vizhub.healthdata.org/gbd-results/).16 The GBD 2021 covers 204 countries and territories, 369 diseases and 88 risk factors.17 The dataset facilitated an in-depth analysis of health metrics, including incidence, prevalence, mortality, and DALYs. Specifically, we extracted data on the incidence and DALYs of uterine prolapse for the period spanning from 1990 to 2021.
DALYs Calculation
DALYs represent a composite measure of health loss, combining Years of Life Lost (YLL) due to premature mortality and Years Lived with Disability (YLD) attributable to illness or disability.18 DALYs are computed based on the duration of the disease and the severity of the disability, incorporating disability weights to quantify the health impact numerically. This metric allows for the comparison of disease burden across different diseases, regions, or countries. Specifically, DALYs for uterine prolapse were calculated using the GBD 2021 study’s standard methodology, integrating data on incidence, prevalence, mortality, and disability weights.
Decomposition Analysis
Decomposition analysis was employed to dissect the contributions of demographic factors (population growth and aging) and epidemiological factors to the observed changes in DALYs.19 This method enabled us to quantify the relative impact of each factor on the overall disease burden. Specifically, we used a decomposition framework to separate the net change in DALYs into components attributable to population growth, population aging, and epidemiological changes (ie., changes in incidence, prevalence, or mortality rates). This approach provided insights into the drivers of changes in the disease burden of uterine prolapse over time.
Health Inequality Analysis
Health inequality analysis was conducted to assess disparities in the disease burden of uterine prolapse across different SDI levels.20 This analysis involved the calculation of the SII and the CI to quantify the magnitude and direction of inequalities. The SII represents the absolute difference in DALYs rates between the highest and lowest SDI groups, while the CI measures the relative inequality, taking into account the entire distribution of DALYs across SDI levels. These metrics provided a comprehensive understanding of health inequalities in uterine prolapse burden globally.
Statistical Analysis
Age-standardized rates (ASR) of uterine prolapse incidence and DALYs, along with their corresponding 95% uncertainty interval (UI), were extracted from the GBD 2021 database for the period 1990–2021. To evaluate long-term temporal trends, we calculated the estimated annual percentage change (EAPC) for ASR. EAPC is a widely used indicator for measuring the change trend of ASR within a specified time interval in time series data, and is calculated as EAPC=100×(Exp(β)−1), where β refers to the regression coefficient of the ASR trend over time. Specifically, when the EAPC value and the lower limit of its 95% CI are both positive, the ASR is considered to be increasing; conversely, when the EAPC value and the upper limit of its 95% CI are both negative, the ASR is considered to be decreasing. To quantify the contributions of demographic and epidemiological factors to the observed changes in DALYs from 1990 to 2021, we performed decomposition analysis.19 This method enables the separation of the net change in DALYs into three components: (1) population growth, (2) population aging, and (3) epidemiological changes (ie., changes in age-specific incidence, prevalence, or mortality rates). The decomposition framework was based on the method developed by Das Gupta, which provides a standardized approach for partitioning the total change in a health metric across different time points. Specifically, the contribution of each factor was calculated by holding the other two factors constant at their reference levels. The results are expressed as absolute contributions (per 100,000 population) and relative percentages of the total net change. Health inequality analysis was conducted to assess disparities in the disease burden of uterine prolapse across different SDI levels. This analysis involved the calculation of two standard indicators:
(1) The SII represents the absolute difference in DALYs rates between the highest and lowest SDI groups. It is estimated as the slope of a robust linear regression of the DALYs rate on the SDI rank (ranging from 0 to 1, with 0 representing the lowest SDI and 1 representing the highest SDI). A positive SII indicates that the disease burden is concentrated among populations with higher SDI, whereas a negative SII indicates the opposite.
(2) The CI measures relative inequality by capturing the entire distribution of DALYs across SDI levels. The CI is defined as twice the area between the concentration curve (which plots the cumulative proportion of DALYs against the cumulative proportion of the population, ranked by SDI) and the line of equality (the 45-degree line). The CI ranges from −1 to 1; a positive value indicates that the disease burden is disproportionately concentrated among higher SDI populations, while a negative value indicates concentration among lower SDI populations. Both SII and CI were calculated using standard methods as previously described in GBD-based inequality analyses.
All statistical analyses and visualizations were performed using R software (version 4.4.2. Figures were generated to compare temporal trends, SDI-stratified patterns, decomposition contributions, and health inequality metrics. All hypothesis tests were two-sided, and statistical significance was defined as P<0.05.
Results
Global Level for Uterine Prolapse
The global DALYs rate for uterine prolapse in 2021 was 9.90 [95% UI (4.86, 18.59)] (Figure 1 and Table 1). At the national level, the countries with the highest DALYs rates for uterine prolapse were Germany [21.13, 95% UI (9.58, 40.89)], Monaco [20.42, 95% UI (9.41, 39.06)], and Norway [20.28, 95% UI (9.92, 38.27)] (Figure 1). In contrast, the countries with the lowest DALYs rates were Venezuela (Bolivarian Republic of) [3.63, 95% UI (1.63, 7.11)], Papua New Guinea [3.77, 95% UI (1.78, 7.10)], and Samoa [3.91, 95% UI (1.88, 7.44)].
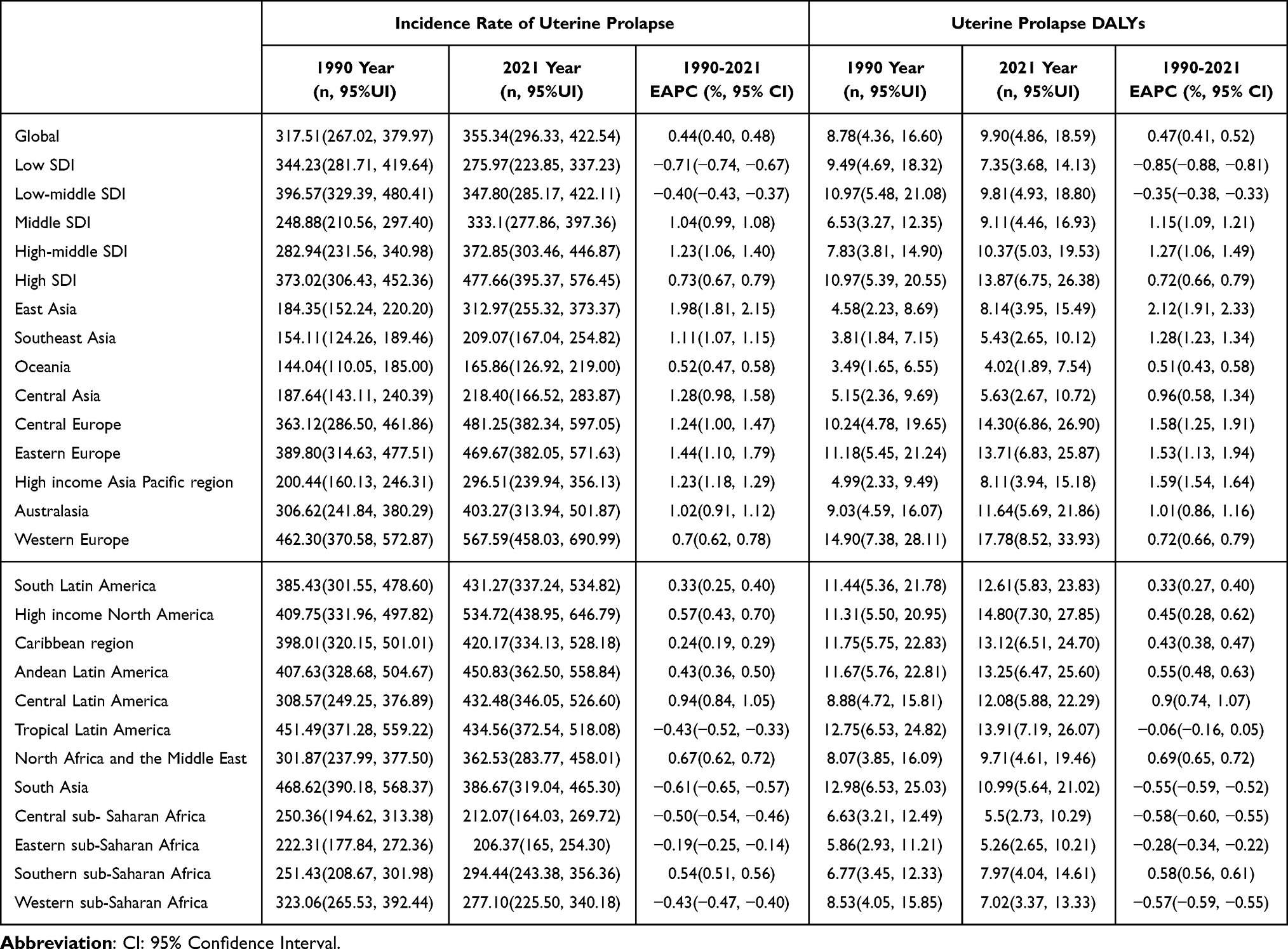 |
Table 1 Changes in Burden of Uterine Prolapse Disease from 1990 to 2021 |
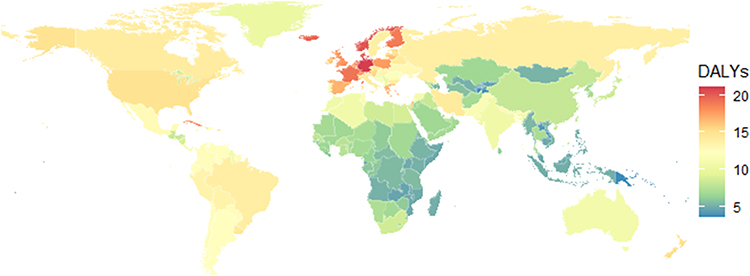 |
Figure 1 The global distribution of Disability-Adjusted Life Years (DALYs) rates for uterine prolapse in females (per 100,000 people) in 2021. The color gradient on the world map represents DALYs rates, with the legend indicating the specific rate values corresponding to each color. |
Age Analysis for Uterine Prolapse
The incidence of uterine prolapse shows a noticeable increase starting from the age group of 40–44 years (Figure 2). It reaches a staged peak in the 45–54 year old age groups. There is a slight decline in the 55–64 year old age group, followed by a resurgence in those aged 65 years and above, with a peak observed in the 90 year old and above age group. Correspondingly, the age-specific DALYs exhibit an approximately monotonic increase with age. The increment is more pronounced in the older age groups, indicating that the elderly population bears a heavier disease burden. This pattern highlights the significant impact of aging on both the occurrence and the disability burden associated with uterine prolapse.
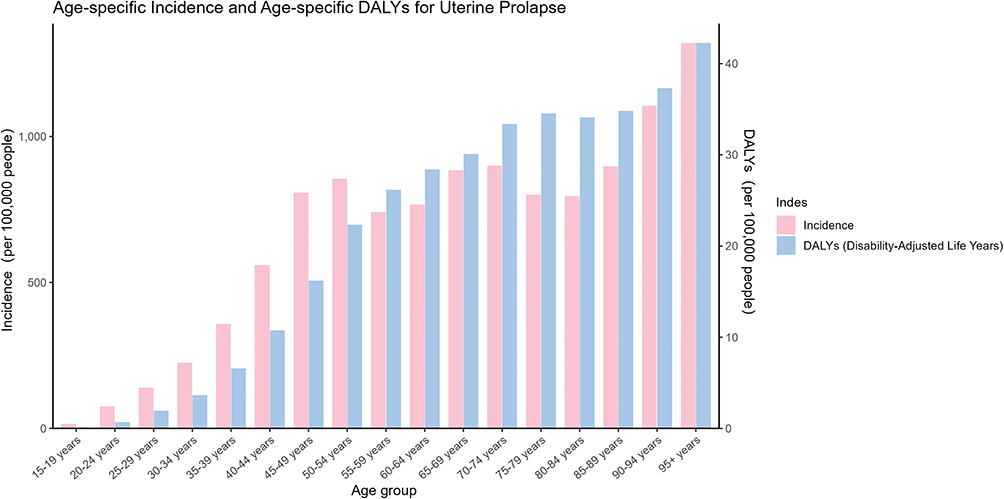 |
Figure 2 The age-specific incidence and age-specific Disability-Adjusted Life Years (DALYs) for uterine prolapse. The left-hand vertical axis corresponds to the values of incidence (per 100,000 people), while the right-hand vertical axis corresponds to the values of DALYs (per 100,000 people). |
SDI Analysis for Uterine Prolapse
During the period from 1990 to 2021, there was a significant heterogeneity in the trends of DALYs and incidence of uterine prolapse across different SDI levels (Figure 3). Low and low-middle SDI regions started at relatively high levels and showed a continuous decline. Middle SDI regions exhibited a continuous increase starting from the year 2000. The high SDI regions demonstrated a U-shaped trend, surpassing the low-middle SDI regions between 2008 and 2010 and approaching/exceeding the low SDI regions by 2015. High-middle SDI regions mainly showed a monotonic increase and experienced an accelerated growth in the rate from 2019 to 2021, ranking at the top in terms of gradient at the end of the period. The global overall curve showed a slow upward trend.
 |
Figure 3 The disease burden trends of uterine prolapse from 1990 to 2021 across the globe and in regions/countries categorized into five Socio-Demographic Index (SDI) levels. (A) The global and SDI-specific trends in the Disability-Adjusted Life Years (DALYs) of uterine prolapse. (B) The global and SDI-specific trends in the incidence of uterine prolapse. |
Decomposition Analysis for Uterine Prolapse
Compared to 1990, the net change in global DALYs for uterine prolapse in 2021 was primarily driven by demographic factors (Figure 4). Population growth and the contribution of population aging were positive, while epidemiological factors had a negative contribution. Across SDI strata, the high SDI group had the highest proportion of DALYs contribution from population aging, followed by population growth, with limited improvement from epidemiological factors, resulting in a continuous net increase. The high-middle SDI group was simultaneously influenced by population growth and aging, showing a significant net increase. Epidemiological factors were most prominent in the low-middle and low SDI groups, partially offsetting the increase caused by population factors and leading to a relatively small net increase.
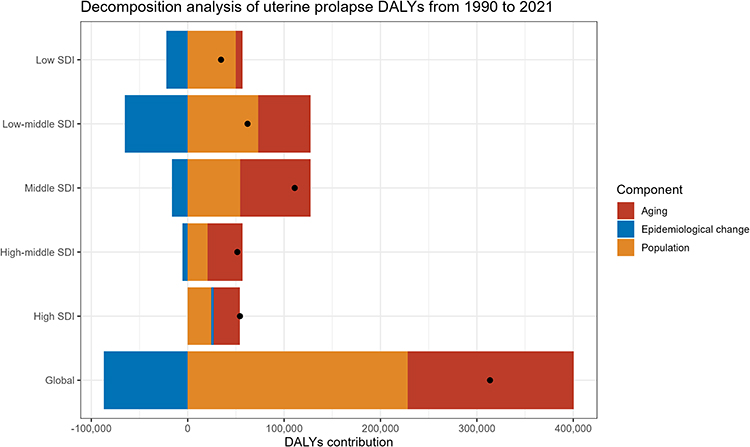 |
Figure 4 The decomposition analysis of Disability-Adjusted Life Years (DALYs) for uterine prolapse from 1990 to 2021. The figure displays the DALYs contributions for different Socio-Demographic Index (SDI) levels, including Low SDI, Low-middle SDI, Middle SDI, High-middle SDI, High SDI, as well as the Global level, with each SDI category shown as a separate bar divided into the three components. Black dots are overlaid on each bar segment, representing specific data points. |
Health Inequality Analysis for Uterine Prolapse
From 1990 to 2021, the inequality in the disease burden of uterine prolapse has significantly increased (Figure 5). The SII obtained from robust regression has changed from a relatively gentle positive slope in 1990 to a steeper positive slope in 2021, with the absolute difference along the SDI gradient widening. The concentration index (based on rate) has risen from 0.016 in 1990 to 0.092 in 2021, indicating an increase in relative inequality. Both indicators are positive, suggesting that the disease burden is more concentrated among populations with higher SDI.
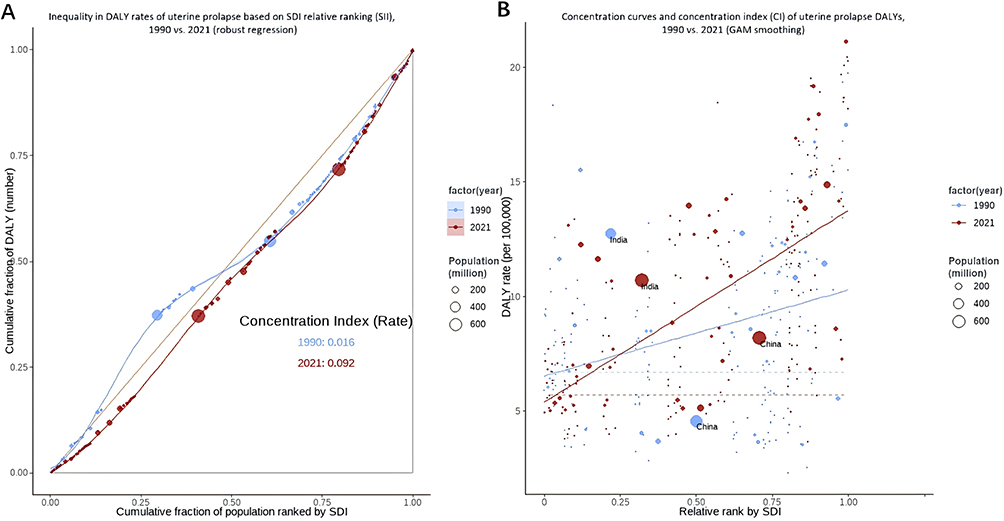 |
Figure 5 The health inequality analysis of uterine prolapse burden. (A) The horizontal axis represents the relative ranking (0–1) of countries according to the Socio-Demographic Index (SDI), arranged from low to high. The vertical axis denotes the DALYs rate (per 100,000 people) of uterine prolapse. The size of the bubbles is scaled according to the population (in millions), and example annotations (India and China) are provided. The solid lines represent the robust linear regressions fitted by year. The SII (Slope Index of Inequality) is defined as the absolute difference in the regression line values between SDI rank 1 and SDI rank 0 (indicating absolute inequality). (B) Sorts countries from low to high SDI. The horizontal axis represents the cumulative population share, while the vertical axis represents the cumulative DALYs share. The 45-degree line signifies complete equality. A curve located below the 45 - degree line and with a larger Concentration Index (CI, twice the area between the curve and the 45-degree line) indicates greater and positive inequality, meaning the disease burden is more concentrated in higher SDI populations. |
Discussion
Our study conducted a comprehensive analysis of global trends in the incidence and DALYs of uterine prolapse from 1990 to 2021 across 204 countries, revealing significant insights into the disease burden and its determinants. The results demonstrate a notable rise in the global DALYs rate for uterine prolapse, reaching 9.90 per 100,000 population in 2021, with pronounced regional variations. Countries such as Germany, Monaco, and Norway exhibited the highest DALYs rates, while Venezuela, Papua New Guinea, and Samoa had the lowest. This disparity underscores the influence of regional factors, including healthcare access, demographic changes, and health policies, on the burden of uterine prolapse.
Uterine prolapse, a common and debilitating form of pelvic organ prolapse, poses a significant threat to women’s health worldwide, contributing to considerable morbidity and a diminished quality of life.21 Our study’s findings align with and extend upon previous research, providing a nuanced understanding of the global burden of this condition. Consistent with prior studies,22 our research reveals a marked increase in the incidence of uterine prolapse starting from the 40–44 year age group, peaking notably in the 45–54 year olds, and experiencing a resurgence among those aged 90 years and above. This mirrors the age-specific DALYs pattern, which exhibits a nearly monotonic rise with age. Such trends underscore the profound impact of aging on both the incidence and the disability burden associated with uterine prolapse, highlighting the imperative for targeted interventions tailored to aging populations. Of note, the incidence of uterine prolapse reaches a staged peak at 45–54 years of age, whereas DALYs attributable to uterine prolapse reach a pronounced peak in those aged 90 years and older. This phenomenon can be explained by several factors. First, there is a fundamental distinction between incidence and DALYs by definition: Incidence measures the number of new cases per year divided by the total population, reflecting the risk of developing the disease.23 In contrast, DALYs represent the health loss due to accumulated prevalent cases over one year, capturing the total burden of established disease.24 Therefore, even though the incidence of new cases appears lower in the oldest age groups, the accumulation of prior cases with long disease duration allows DALYs to peak at very advanced ages. Second, it is important to note that the incidence peak at 45–54 years is actually a “staged peak”, and the incidence among those aged 90+ years remains higher than that in the 45–54 age group. Thus, the oldest-old population experiences both a higher incidence rate and an accumulated burden of pre-existing cases, which further explains the persistently rising DALYs in this age group. Third, as a progressive condition, uterine prolapse in older patients is characterized by a longer disease duration, leading to more severe histopathological changes and functional deficits in pelvic support structures.25 The DALY metric itself incorporates both disability weight and duration; each remaining year of life carries a higher disability weight.26 Finally, women in this age group face higher perioperative risks27 or have lower preference for surgical intervention,28 resulting in a predominance of conservative management, which allows the disability state to persist and accumulate. This cumulative effect leads to persistently high DALYs in the oldest-old.
Mäkinen J et al has similarly emphasized the role of hormonal changes, reduced pelvic support tissue elasticity, and multiple childbirths as contributing factors to the increased prevalence in older women29 Our analysis across different SDI levels reveals significant heterogeneity in the trends of DALYs and incidence of uterine prolapse, echoing and refining observations from previous studies.12 Low and low-middle SDI regions commenced at relatively elevated levels but demonstrated a continuous decline, whereas middle, high-middle, and high SDI regions witnessed increases. Notably, high SDI regions exhibited a U-shaped trend, overtaking low-middle SDI regions and nearing/exceeding low SDI regions by 2015. High-middle SDI regions displayed a monotonic increase with accelerated growth from 2019 to 2021. These trends suggest that regions with higher SDI levels are experiencing a rising burden of uterine prolapse, likely attributed to demographic shifts, lifestyle modifications, and enhanced disease detection capabilities. Previous research has also pointed to increased obesity rates, decreased physical activity, and higher parity in developed nations as potential contributors to these trends.30–32 Decomposition analysis confirmed divergent drivers across global SDI strata, with distinct offset effects from epidemiological interventions observed in low- and low-middle SDI settings.33 Notably, epidemiological improvements including standardized maternal pelvic floor screening,34 basic gynecological healthcare popularization and affordable conservative treatment locally offset approximately 20% of the population-related DALY growth in low-SDI nations. Such offset effect carries prominent public health implications:35 for resource-limited developing regions, scaling up low-cost preventive and primary care services can effectively counteract the extra disease burden induced by population expansion and aging, without relying on expensive surgical interventions. In contrast, population aging dominated DALY increments in high-SDI territories,36 where optimized diagnosis elevated case detection and further lifted recorded disease burden. This stratified discrepancy highlights the necessity of tailoring region-specific health policies according to demographic and epidemiological profiles. Prior studies have similarly emphasized the importance of understanding these multifaceted influences on disease trends.5,37
Health inequality analysis indicated a substantial increase in the inequality of uterine prolapse burden from 1990 to 2021. Both the SII and the CI demonstrated an upward trend, suggesting that the disease burden is increasingly concentrated among populations with higher SDI. This finding aligns with previous research indicating disparities in healthcare access and outcomes across socio-economic strata.38,39 It underscores the need for targeted interventions to address health disparities and ensure equitable access to healthcare services, particularly in regions with higher SDI levels. While our study provides valuable insights, it is not without limitations. Variations in data availability and quality across countries may affect the accuracy of estimates. Changes in diagnostic criteria, screening methods, and treatment practices over time may also influence observed trends. Additionally, potential confounding factors such as genetic predisposition, environmental factors, and lifestyle changes were not accounted for. Future research should delve deeper into understanding the underlying factors driving these trends, evaluating the effectiveness of specific interventions, and developing strategies tailored to regional contexts.
This study revealed that the global age-standardized DALY rate for uterine prolapse showed a slow increase from 1990 to 2021, with marked heterogeneity across SDI levels. Low and low-middle SDI regions declined, whereas middle, high-middle, and high SDI regions increased, with high SDI regions showing a U-shaped resurgence. Incidence exhibited a bimodal peak at 45–54 years and 90+ years, while DALYs peaked in the oldest-old, suggesting that both new-onset risk and accumulated disability drive the burden. Population growth and aging were identified as the primary drivers of global DALY increases, with epidemiological changes only partially offsetting the increase in low SDI regions. The burden of uterine prolapse progressively concentrated among higher SDI populations, with inequality widening over the past three decades. We recommend early screening for midlife women, tiered management for older women, metabolic risk control in high SDI regions, surgical access in low SDI regions, and resource allocation tailored to national SDI levels and population age structures.
Data Sharing Statement
The datasets analyzed in this study are publicly available from the GHDx platform: https://vizhub.healthdata.org/gbd-results/.
Ethics Approval and Consent to Participate
This study used publicly available, de-identified summary data from the GBD 2021 database and did not involve direct contact with human participants or identifiable personal information. This research was reviewed by Henan Provincial Chest Hospital and determined to be exempt from formal ethical review in accordance with Item 1 and Item 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (dated February 18, 2023, China). The requirement for informed consent was also waived, as only aggregated, anonymized public data were analyzed. All procedures were performed in accordance with the principles of the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Chronic Disease Management Research Project of National Health Commission Capacity Building and Continuing Education Center (GWJJMB202510021166).
Disclosure
The authors declare no competing interests in this work.
References
1. Voelker R. What is uterine prolapse? JAMA. 2024;331(7):624. doi:10.1001/jama.2023.22744
2. Houmaid H, Harou K, Fakhir B, et al. Uterine prolapse in pregnancy: a case report and literature review. Pan Afr Med J. 2024;49:101. doi:10.11604/pamj.2024.49.101.43712
3. Loukopoulou A, Tzanni E, Bothou A, et al. Uterine prolapse across the female lifespan: clinical insights and practical considerations from Greece. Nurs Rep. 2025;15(6):212. doi:10.3390/nursrep15060212
4. Muldoon J. Uterine prolapse: impact of the condition and practical advice. Br J Nurs. 2022;31(18):S8–11. doi:10.12968/bjon.2022.31.18.S8
5. Mannella P, Palla G, Bellini M, Simoncini T. The female pelvic floor through midlife and aging. Maturitas. 2013;76(3):230–234. doi:10.1016/j.maturitas.2013.08.008
6. Pakbaz M, Rolfsman E, Mogren I, Löfgren M. Vaginal prolapse--perceptions and healthcare-seeking behavior among women prior to gynecological surgery. Acta Obstet Gynecol Scand. 2011;90(10):1115–1120. doi:10.1111/j.1600-0412.2011.01225.x
7. Iida R, Piñeiro C, Koketsu Y. Incidences and risk factors for prolapse removal in Spanish sow herds. Prev Vet Med. 2019;163:79–86. doi:10.1016/j.prevetmed.2018.12.016
8. Catanzarite T, Rambachan A, Mueller MG, Pilecki MA, Kim JY, Kenton K. Risk factors for 30-day perioperative complications after Le Fort colpocleisis. J Urol. 2014;192(3):788–792. doi:10.1016/j.juro.2014.03.040
9. Murray CJL. GBD 2021 collaborators. findings from the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2259–2262. doi:10.1016/S0140-6736(24)00769-4
10. GBD 2021 Forecasting Collaborators. Burden of disease scenarios for 204 countries and territories, 2022-2050: a forecasting analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2204–2256. doi:10.1016/S0140-6736(24)00685-8
11. Jani CT, Kareff SA, Morgenstern-Kaplan D, et al. Evolving trends in lung cancer risk factors in the ten most populous countries: an analysis of data from the 2019 Global Burden of Disease Study. EClinicalMedicine. 2025;79:103033. doi:10.1016/j.eclinm.2024.103033
12. He X, Su J, Wang K, Liang Y, Wang L. Global, regional, and national prevalence and trends of gynecological diseases among women of childbearing age from 1990 to 2021: an analysis of the global burden of disease study 2021. PLoS One. 2025;20(8):e0329336. doi:10.1371/journal.pone.0329336
13. Hagenbeck C, Kössendrup J, Soff J, Thangarajah F, Scholten N. Pelvic floor-related sexual functioning in the first 24 months postpartum: findings of a large cross-sectional study. Acta Obstet Gynecol Scand. 2025;104(1):203–214. doi:10.1111/aogs.14990
14. Dułak NA, Trzciński R. The burden of pelvic floor dysfunction. J Sci Med Sport. 2022;25(4):293. doi:10.1016/j.jsams.2021.11.042
15. Assefa Demissie B, Tennfjord MK, Mihiret T, et al. Prevalence and associated factors of symptomatic pelvic floor disorders among women living in Debre Tabor Town, Northwest Amhara, Ethiopia. BMC Womens Health. 2024;24(1):367. doi:10.1186/s12905-024-03176-y
16. Global Burden of Disease Collaborative Network. Global burden of disease, institute of health metrics and evaluation; Seattle: 2023. Global Burden of Disease Study 2019 (GBD 2019) results. Available from: https://vizhub.healthdata.org/gbd-results/.
17. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of Disease Study 2019. Lancet. 2020;396:1204–1222.
18. Wang F, Ma B, Ma Q, Liu X. Global, regional, and national burden of inguinal, femoral, and abdominal hernias: a systematic analysis of prevalence, incidence, deaths, and DALYs with projections to 2030. Int J Surg. 2024;110(4):1951–1967. doi:10.1097/JS9.0000000000001071
19. Li J, Guo K, Qiu J, et al. Epidemiological status, development trends, and risk factors of disability-adjusted life years due to diabetic kidney disease: a systematic analysis of Global Burden of Disease Study 2021. Chin Med J. 2025;138(5):568–578. doi:10.1097/CM9.0000000000003428
20. Liu W, Deng W, Gong X, Ou J, Yu S, Chen S. Global burden of Alzheimer’s disease and other dementias in adults aged 65 years and over, and health inequality related to SDI, 1990-2021: analysis of data from GBD 2021. BMC Public Health. 2025;25(1):1256. doi:10.1186/s12889-025-22378-z
21. Doshani A, Teo RE, Mayne CJ, Tincello DG. Uterine prolapse. BMJ. 2007;335(7624):819–823. doi:10.1136/bmj.39356.604074.BE
22. Allard P, Rochette L. The descriptive epidemiology of hysterectomy, Province of Quebec, 1981-1988. Ann Epidemiol. 1991;1(6):541–549. doi:10.1016/1047-2797(91)90026-9
23. Abbass NJ, Yazji I, Allan KC, Kaelber DC, Talcott KE, Singh RP. Trends and disparities in the incidence and prevalence of inherited retinal diseases in the United States. Am J Ophthalmol. 2025;279:165–173. doi:10.1016/j.ajo.2025.07.021
24. GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
25. Handa VL, Garrett E, Hendrix S, Gold E, Robbins J. Progression and remission of pelvic organ prolapse: a longitudinal study of menopausal women. Am J Obstet Gynecol. 2004;190(1):27–32. doi:10.1016/j.ajog.2003.07.017
26. Verguet S, Chakrabarti A. Examining the computation of the underlying components of DALYs. Health Policy Plan. 2023;38(5):648–654. doi:10.1093/heapol/czad017
27. Wang Q, Wu N, Li Y, Lin C, Xu Y, Chen X. Outcomes of Manchester procedure combined with high uterosacral ligament suspension for uterine prolapse. J Obstet Gynaecol Res. 2023;49(4):1273–1282. doi:10.1111/jog.15574
28. Tola EN, Erdemoğlu E, Erdemoğlu E. Uterine sparing surgical methods in pelvic organ prolapse. Turk J Obstet Gynecol. 2015;12(3):168–172. doi:10.4274/tjod.43179
29. Mäkinen J, Kähäri VM, Söderström KO, Vuorio E, Hirvonen T. Collagen synthesis in the vaginal connective tissue of patients with and without uterine prolapse. Eur J Obstet Gynecol Reprod Biol. 1987;24(4):319–325. doi:10.1016/0028-2243(87)90157-2
30. Lee UJ, Kerkhof MH, van Leijsen SA, Heesakkers JP. Obesity and pelvic organ prolapse. Curr Opin Urol. 2017;27(5):428–434. doi:10.1097/MOU.0000000000000428
31. Strain T, Flaxman S, Guthold R, et al. National, regional, and global trends in insufficient physical activity among adults from 2000 to 2022: a pooled analysis of 507 population-based surveys with 5·7 million participants. Lancet Glob Health. 2024;12(8):e1232–e1243. doi:10.1016/S2214-109X(24)00150-5
32. Deeb ME, Awwad J, Yeretzian JS, Kaspar HG. Prevalence of reproductive tract infections, genital prolapse, and obesity in a rural community in Lebanon. Bull World Health Organ. 2003;81(9):639–645.
33. Xu Q, Qiao Z, Kan Y, Wan B, Qiu X, Yang Y. Global, regional, and national burden of depression, 1990-2021: a decomposition and age-period-cohort analysis with projection to 2040. J Affect Disord. 2025;391:120018. doi:10.1016/j.jad.2025.120018
34. Xie J, Li W, Li X, et al. Global, regional, and national epidemiology of type 1 diabetes in children from 1990 to 2021: trend and health inequality analyses based on the Global Burden of Disease Study 2021. Diabetol Metab Syndr. 2025;17(1):337. doi:10.1186/s13098-025-01905-3
35. Tan EL, Qin Y, Yang J, et al. Global burden of MDR-TB and XDR-TB: trends, inequities, and future implications for public health planning. BMC Infect Dis. 2025;25(1):1225. doi:10.1186/s12879-025-11566-2
36. Liu J, Xu A, Zhao Z, et al. Epidemiology and future trend predictions of ischemic stroke based on the global burden of disease study 1990-2021. Commun Med. 2025;5(1):273. doi:10.1038/s43856-025-00939-y
37. Serván-Mori E, Pineda-Antúnez C, Cerecero-García D, et al. Health system financing fragmentation and maternal mortality transition in Mexico, 2000-2022. Int J Equity Health. 2025;24(1):32. doi:10.1186/s12939-024-02357-3
38. Hirani BA, Mchome BL, Mazuguni NS, Mahande MJ. The decision delivery interval in emergency caesarean section and its associated maternal and fetal outcomes at a referral hospital in northern Tanzania: a cross-sectional study. BMC Pregnancy Childbirth. 2017;17(1):411. doi:10.1186/s12884-017-1608-x
39. Ferrari A, Bellè N, Giannini A, Simoncini T, Vainieri M. Determinants of women’s preferences for surgical versus conservative management for pelvic organ prolapse: a survey-based study from Italy. BMJ Open. 2024;14(7):e084034. doi:10.1136/bmjopen-2024-084034
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Global Burden and Trends of UTI in Premenopausal and Postmenopausal Women from 1990 to 2021 and Projections to 2044
Tang K, Feng J, Lai H, Zhao Z, Zou Y, Lv Q, Dai F, Qiu X, Lai W
International Journal of Women's Health 2025, 17:1375-1392
Published Date: 14 May 2025
Trends in the Disease Burden of Migraine Among Women of Reproductive Age (15–49 Years) in Low- and Middle-Income Countries, 1990–2023
Deng Q, Lu H, He R, Zhang H, Yan H, Chen Y, Bi J, Zhang R, Tang K, Wang Z, Zhang W
International Journal of Women's Health 2026, 18:597042
Published Date: 18 April 2026