Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Analysis on clinical effects of dilation and curettage guided by ultrasonography versus hysteroscopy after uterine artery embolization in the treatment of cesarean scar pregnancy
Authors Qiu J, Fu Y ![]() , Xu J, Huang X, Yao G, Lu W
, Xu J, Huang X, Yao G, Lu W
Received 18 August 2018
Accepted for publication 13 November 2018
Published 7 January 2019 Volume 2019:15 Pages 83—89
DOI https://doi.org/10.2147/TCRM.S184387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Jian Qiu,1,2 Yunfeng Fu,1 Jiewei Xu,3 Xiaohong Huang,2 Guorong Yao,2 Weiguo Lu1
1Department of Gynecologic Oncology, Women’s Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang 310006, China; 2Department of Obstetrics and Gynaecology, Huzhou Central Hospital, Huzhou, Zhejiang 313000, China; 3Department of General Surgery, Huzhou Central Hospital, Huzhou, Zhejiang 313000, China
Purpose: The purpose of this study was to investigate the efficiency, complications, and subsequent fertility outcomes of two methods in treating patients with cesarean scar pregnancy (CSP) after receiving uterine artery embolization (UAE) treatment.
Patients and methods: A total of 62 CSP patients who visited our hospital and underwent UAE from January 2013 to January 2018 were retrospectively analyzed. Patients were either treated by dilation and curettage (D&C) guided by ultrasonography or hysteroscopy. The differences of related clinical indicators, clinical efficacy, complications, and subsequent fertility outcomes between the two groups were analyzed.
Results: The rates of therapeutic success of the ultrasonography group and hysteroscopy group were 84.6% and 95.7%, respectively, the difference was not statistically significant (P=0.243). However, the intraoperative blood loss, duration of hospitalization, and overall complications were significantly lower in hysteroscopy group compared with D&C guided by ultrasonography group (P<0.05 for all). Meanwhile, hysteroscopy had the advantage of discovering potential diverticulum in the lower segment of anterior wall of uterus (P<0.001).
Conclusion: D&C guided by ultrasonography or hysteroscopy for the treatment of CSP after UAE resulted in similarly good clinical outcomes. Compared with treatment of D&C guided by ultrasonography, hysteroscopy had less complications and had the advantages of discovering diverticulum. It can be used as an effective way for the treatment of CSP.
Keywords: cesarean scar pregnancy, uterine artery embolization, dilation and curettage, ultrasonography-guided, hysteroscopy
Introduction
Cesarean scar pregnancy (CSP), which refers to the implantation of a gestational sac within the scar of a previous cesarean section, has been increased in recent years due to an increased rate of cesarean section and accurate diagnosis of high-resolution ultrasound scanning.1 The incidence ranges from 1/1,800 to 1/2,200 pregnancies, and it constitutes 6.1% of all ectopic pregnancies with a history of one or more cesarean deliveries.2 Previously, Vial et al proposed two different types of CSP: The first is a superficial invasion of the amniotic sac into the scar with the progression of the pregnancy into the cervicoisthmic space and uterine cavity and hence is known as endogenous CSP (type I). The second type involves a deep implantation into the scar with the progression toward the uterine myometrium and the serosal surface and is named exogenous CSP (type II).3 Since CSP is associated with serious and emergency medical complications, such as uterine rupture, life-threatening hemorrhage, and risk of hysterectomy, prompt and accurate ultrasound diagnosis is essential for conservative treatment and preservation of fertility. Currently, many treatment strategies have been established, including systemic methotrexate (MTX), uterine artery embolization (UAE), dilation and curettage (D&C), hysterotomy, and hysteroscopy. However, no clear guidelines have been established for the treatment of CSP until now. It is reported that medical treatment options alone for the treatment of CSP are often insufficient. Combination therapy is considered to be effective with less complications.4 UAE has been proved to be a safe and viable intervention to control hemorrhaging and preserve the uterus in the treatment of uterine fibroids, uterine arteriovenous fistula, or postpartum hemorrhage,5–7 but for the treatment of CSP, UAE usually need to be combined with D&C or other therapies. Tumenjargal et al suggested that UAE combined with D&C can be efficient and safe for CSP management, and it should be considered as one of the treatment options which enable preservation of fertility after treatment.8 Qiao et al reported that UAE combined with D&C significantly shortened the time for β human chorionic gonadotropin (β-HCG) normalization and hospital stay and reduced blood losses and adverse events compared with the administration of MTX plus curettage. It appears to be more advantageous and may be a priority option for the treatment of CSP.9 In our hospital, all CSP patients who were treated by UAE received D&C guided by ultrasonography or hysteroscopy. So the aim of the present study was to analyze the efficacy, complications, and subsequent fertility outcomes of these two methods in the treatment of patients with CSP.
Patients and methods
Data collection and ethics committee
This study was a retrospective analysis of a prospectively collected database. Data of all patients who were diagnosed as CSP and underwent UAE combined with D&C guided by ultrasonography or hysteroscopy treatment from January 2013 to January 2018 were collected in our study. This study was approved by the ethics committee of Huzhou Central Hospital. Signed informed consent forms were not required for this retrospective study. But all patients’ data were kept confidentially.
Diagnostic criteria
Patients were diagnosed with CSP according to cesarean delivery history, β-HCG level, and ultrasonography. Ultrasound diagnosis was made according to the following criteria:10 1) an empty uterine cavity with a clearly demonstrated endometrium; 2) an empty cervical canal; 3) the gestational sac was located in the anterior part of the uterine isthmus, with decreased myometrial thickness between the bladder and the sac; 4) the gestational sac was implanted in the myometrium and fibrous tissue of the cesarean delivery scar.
Inclusion and exclusion criteria for enrolled patients in our cohort
The inclusion criteria were: 1) diagnosed as CSP according to the criteria described above; 2) gestational age <10 weeks; 3) patients did not receive any other treatments except UAE combined with D&C guided by transabdominal ultrasound or hysteroscopy.
The exclusion criteria were: 1) patients with severe internal and external diseases; 2) patients with abnormal coagulation and pelvic inflammatory disease; 3) received other treatment before UAE; 4) clinical data incomplete and lost to follow-up.
Clinical treatments, follow-up, and evaluation of therapeutic effects
All CSP patients received D&C guided by ultrasonography or hysteroscopy after UAE treatment. The procedure of UAE was performed through a right femoral artery puncture under local anesthesia, a Rosch hepatic catheter was advanced into the right internal iliac artery, then embolization was carried out by injection of gel foam sponge particles (900–1,200 μm) into the feeding vessels. D&C guided by ultrasonography or hysteroscopy were performed in the next 24 hours. Blood loss during the operation was counted through the amount and weight of medical gauze.
After the treatment, patients were closely observed by performing serum β-HCG level test, liver function test, and blood routine test and monitoring vital signs and the amount of vaginal bleeding. At discharge, patients were asked to return every week for serum β-HCG level testing and transvaginal ultrasonography examination until serum β-HCG level returned to its normal level. They were also instructed to use contraception for 1 year. Telephone follow-up was conducted every 3 months after CSP treatment and ended on May 31, 2018. The content of follow-up mainly included complications (hemorrhage, anemia, infection, retained products of conception, and intrauterine adhesions), duration of vaginal bleeding, time for recovery of the menstrual cycle (days), changes of menstrual cycle and menstrual amount, time for β-HCG reduction to normal level and subsequent fertility outcomes.
Success of any treatment was defined as the disappearance of the CSP sac and normalized serum β-HCG level without an additional intervention requirement or any severe complication, such as bleeding, uterine rupture, or hysterectomy. Treatment failure was defined as uterine perforation, active and abundant vaginal bleeding requiring blood transfusion (which was identified as hemoglobin declined below 7 g/dL), and/or β-HCG levels that plateaued after the treatments implemented, and need for further therapeutic modalities, such as administration of systemic or local MTX, hysteroscopic treatment, and laparoscopic or laparotomic resection of the gestational sac.
Statistical analysis
Statistical analyses were performed using SPSS 16.0 software package. Descriptive statistics are given as mean ± standard deviation, frequency, and percentage. Comparisons between the two groups were analyzed by Student’s t-test for continuous variables and the chi-squared test or Fisher’s exact test for categorical data. Values of P<0.05 were considered statistically significant.
Results
General information
A total of 103 patients diagnosed as CSP from January 2013 to January 2018 visited our hospital. Among them, eight patients refused further treatment and to see a doctor in other hospitals. Twenty-nine patients received MTX combined with D&C guided by ultrasonography or hysteroscopy. Four patients were lost in the follow-up. Finally, according to the criteria described above, a total of 62 CSP patients were included in the observation. Among them, 39 patients underwent UAE combined with D&C guided by ultrasonography (Group 1, N=39), while the other 23 patients received UAE combined with hysteroscopy (Group 2, N=23). The clinical characteristics of the two groups were summarized in Table 1. There was no obviously statistic differences in age, gravidity, parity, number of cesarean section, time interval between the last cesarean section and current pregnancy, days of menopause, β-HCG level at the hospitalized time, diameter of the gestational sac, and ultrasound type (P>0.05).
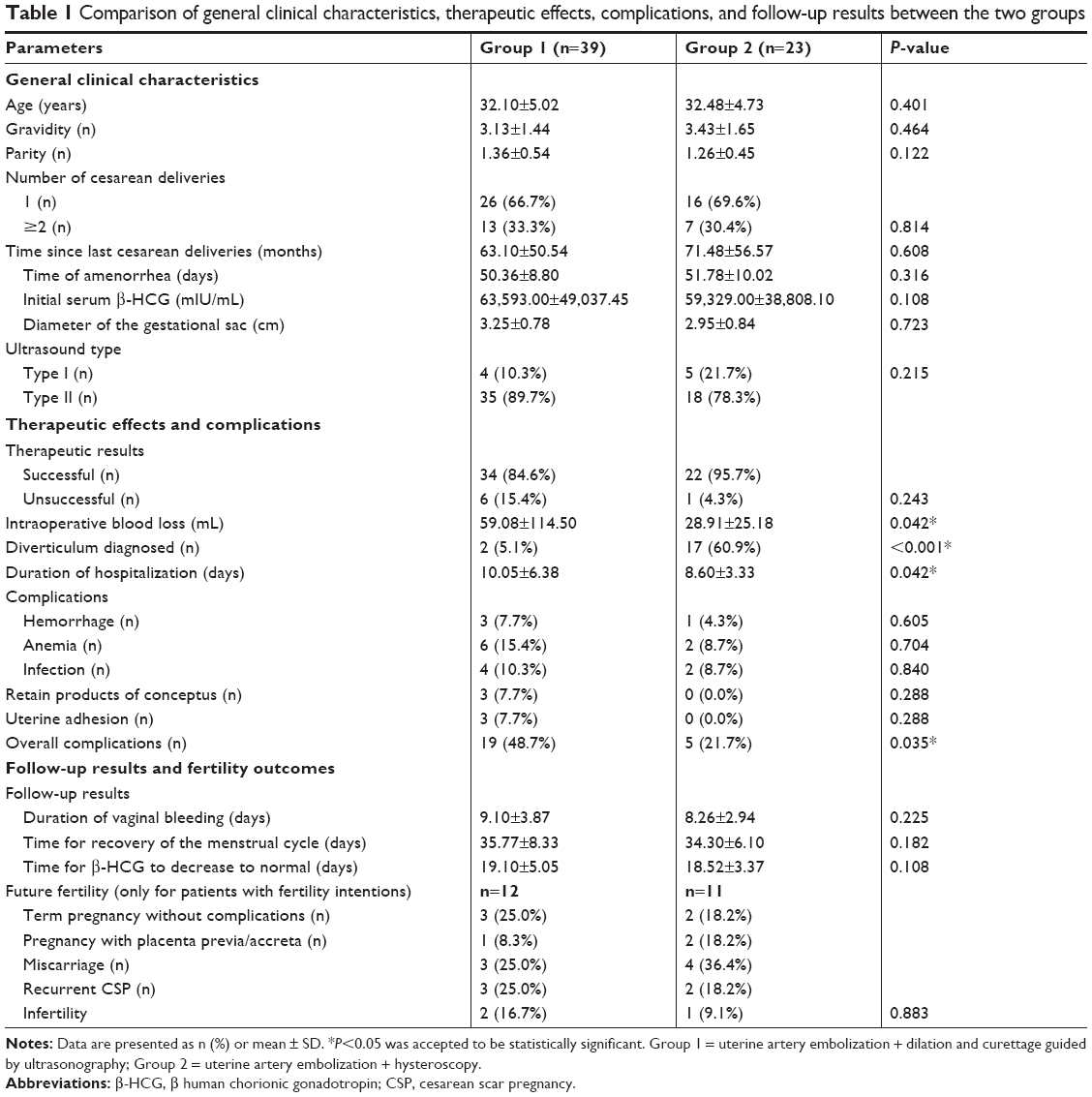 | Table 1 Comparison of general clinical characteristics, therapeutic effects, complications, and follow-up results between the two groups |
Comparison of therapeutic efficacy and complications
Clinical outcomes and complications of patients were also shown in Table 1. Both the treatments demonstrated high success rates and had no significantly statistical difference (84.6% vs 95.7%, P=0.243). In Group 1, treatment failures were observed in six patients. Among the six failed patients: three patients presented massive vaginal bleeding (one patient recovered after undergoing hysteroscopy and electrocoagulate the hemorrhagic spot; the other two patients recovered after treatment with iodoform gauze packing into their uterine cavities and vagina as well as intravenous oxytocin treatment, without other therapies). The other three patients returned to hospital due to vaginal bleeding exceeding 2 weeks as well as unsatisfactory decrease in serum β-HCG level after discharge. Two of them had the retained products of conception in the lower segment of the anterior uterine revealed by ultrasonography. Hysteroscopy was performed to remove pregnancy remnants. The remained one received intramuscular injection of MTX (systematic, total of 75 mg) and was discharged after a steady decline of serum β-HCG level. All of them eventually achieved clinical cure during follow-up. In Group 2, only one presented massive vaginal bleeding. Due to the extremely thin level of the lower segment of anterior uterine wall, tamponade of iodoform gauze into uterine cavity and vagina was performed instead of the electrocoagulation of hemorrhagic spot. She recovered after removing the gauze without any complication.
The intraoperative blood loss in Group 2 was significantly less than that in Group 1 (P=0.042). Besides, duration of hospitalization of Group 2 was also significantly shorter than that of Group 1 (P=0.042). Although there were no significant differences in each complication such as hemorrhage, anemia, infection, retained products of conception, and intrauterine adhesion between the two groups (P>0.05), when they were all added up, the overall complications were significantly lower in Group 2 (P=0.035). Meanwhile, 14 patients were found with diverticulum in the lower segment of the anterior uterine wall under the hysteroscopy (14/23), while two patients in Group 1 were also found with diverticulum revealed by hysteroscopy in subsequent follow-up due to the retained products of conception as described above, the difference was significant (P<0.001, Table 1).
Comparison of subsequent follow-up results
During the follow-up, the duration of vaginal bleeding and the time for serum β-HCG reduction to normal after operation did not differ between the two groups (P>0.05 for all, Table 1). Besides, all patients in both the groups returned to a regular menstrual cycle after treatment (range from 26 to 56 days after operation). The mean time for recovery of the menstrual cycle in Group 1 and Group 2 were 35.77+8.33 vs 34.30+6.10 (days), respectively. The difference was not significant. The reproductive outcomes after CSP included normal intrauterine term pregnancy without complications, pregnancy with placenta previa/accreta, miscarriage, recurrent CSP (RCSP), and infertility. In our study, a total of 23 women in both the groups desired to conceive in future. During the follow-up time, 20 patients result in subsequent pregnancy. Among them, five patient (three of Group 1, two of Group 2) delivered at term without any complications, three patient (one of Group 1, two of Group 2) present placenta previa/accreta in late period of pregnancy, seven patients (three of Group 1, four of Group 2) miscarried spontaneously in early days. Five patients (three of Group 1, two of Group 2) were diagnosed with RCSP. The remaining three patients (two of Group 1, one of Group 2) were diagnosed as infertility. There was no statistical difference for future fertility outcome between the two groups (P>0.05, Table 1). Of the remaining 39 patients in both the groups who did not want to conceive in future, five patients (three of Group 1, two of Group 2) were pregnant unexpectedly. Among them, four patients (one of Group 1, three of Group 2) had intrauterine pregnancies and underwent artificial abortion. One patient of Group 2 resulted in RCSP. Interestingly, we found that all RCSP patients and patients with placenta previa/accreta in Group 2 were found with diverticulum in the lower segment of anterior wall of uterus under hysteroscopy.
Discussion
In the present study, we showed that CSP patients treated with UAE combined with D&C guided by ultrasonography or hysteroscopy were both result in good clinical success. Compared with the treatment of D&C guided by ultrasonography, hysteroscopy had the less complications and intraoperative blood loss as well as shorter duration of hospitalization, besides, it had the advantage of discovering potential diverticulum, indicating that it is a safe and effective method for treatment of patients with CSP. To our knowledge, this is the first systematic study for the comparative analysis of these two methods for treatment of CSP in recent years.
Until now, many strategies have been established, and each method has its advantages and disadvantages. Based on previous studies, treatments like systemic MTX injections, D&C, or UAE alone are not recommended for treatment of CSP due to their high complication rates previously reported.11 Combining therapeutic approaches should be considered when selecting the treatment options. UAE is originally developed as a conservative treatment for postpartum hemorrhage, uterine leiomyomas, pelvic trauma, and cervical pregnancy with the goal of avoiding hysterectomy and preserving fertility. In the past decades, it is widely used in the treatment of CSP when combined with other therapies for its safe, more efficacy with less complications, and a rapider recovery.12–14 UAE blocked the blood flow in the uterine arteries so as to decrease blood supply to the gestational sac, leading to ischemic necrosis of the gestational sac, timely termination of embryonic development, and rapid deactivation of trophoblasts, thus avoiding uterine hemorrhage. However, after complete occlusion of the uterine arteries by UAE, extensive collateral circulation will be established soon, if the gestational sac is not terminated after UAE, the gestational tissues may continue to grow, resulting in bleeding once again.15 Hence, subsequent D&C or hysteroscopy is very important to evacuating conception tissue.
Clinically, D&C guided by ultrasonography or hysteroscopy have been commonly used for CSP treatment after UAE therapy in China.13,16,17 Both the methods provided effective results as shown in our study. In the method of D&C guided by ultrasonography, the uterine position, the location of the gestational sac can be displayed on a computer screen when ultrasonography is performed at the time of D&C; thus, it reduces the likelihood of complications that is caused by the blindness of the operation.18 However, it also has some defects. For example, it cannot find those conception products invading anterior muscle wall of the lower uterine segment, thus leading to retained products of conception. Besides, endometrium injury may occur due to excessive curettage caused by unclear visualization of ultrasound monitoring or limited technology of ultrasound operator, leading to the subsequent intrauterine adhesions. This would explain why there were several cases presenting retained products of conceptus and uterine adhesion in D&C guided by ultrasonography group in our study.
The method of hysteroscopy allows direct visualization of the gestational sac; thus, it can remove the trophoblast tissue precisely without injuring the endometrium.19–21 It can also coagulate the related vascular texture at the implantation site so that any profuse bleeding may be prevented. Meanwhile, it has the advantage of discovering the previous cesarean scar defect or diverticulum. It is known to all that the diverticulum in myometrial scar is associated with increased risk of complications in future pregnancies such as CSP, placenta previa or placenta accreta, as well as with various chronic conditions such as abnormal uterine bleeding, secondary infertility, hypogastric pain, dysmenorrhea, micturition disorders, and so on.22,23 Thus, for these patients who want to conceive in the future, much more attention should be considered. In present study, we found that patients in the hysteroscopy group had less intraoperative blood loss and fewer complications than those in the ultrasound monitoring group, besides, all patients who had diverticulum discovered by hysteroscopy presented pathologic pregnancies in follow-up (RCSP or placenta previa/accreta), indicating that hysteroscopy monitoring could not only be a safe and effective method but also be a procedure for discovering diverticulum so as to advice these women be referred to tertiary centers for further management if they want to conceive in the future.
Another important issue raised from this study was that whether patients’ ovarian function and fertility were influenced by UAE. Previously, some studies have shown that uterine arteries blocked by UAE may reduce blood supply to the ovaries, which may further influence the ovarian function and subsequent fertility. There were reports in the literature regarding adverse events associated with performing UAE for fibroids, including endometrial atrophy and ovarian failure.24 Besides, patients receiving UAE were also at a risk of secondary and uncontrolled vaginal bleeding, which may lead to inevitable hysterectomy.25 However, other studies found that UAE intervention did not change the time before the resumption of menstruation when used in the treatment of CSP, indicating it had an advantage for preserving fertility.14 Hirakawa et al reported successful natural intrauterine pregnancies following UAE treatment in three patients.26 In the present study, all patients returned to regular menstrual cyclicity within 1–2 months after UAE treatment, suggesting that their ovarian function was not influenced by UAE. In addition, 86.9% (20/23) of patients who desired to conceive in future had successful pregnancies although some of them presented pathologic pregnancies (seven miscarried spontaneously, three had placenta previa and placenta implantation, five with RCSP). These findings suggest that UAE is a safe intervention in the treatment of CSP.
Conclusion
In summary, D&C guided by ultrasonography or hysteroscopy after UAE treatment showed good clinical efficacy. However, compared with D&C guided by ultrasonography, hysteroscopy had less complications and had the advantage of discovering potential diverticulum. Although UAE had little influence on patients’ ovarian function and fertility, for patients with usual diverticulum or large defect in the lower part of anterior uterine, further management is recommended to avoid RCSP or other pathologic pregnancies and much more attention should be paid for subsequent pregnancy so as to discover pathologic pregnancy earlier and receive treatment immediately. This study is a retrospective research with only a small sample size; hence, it has some limitations such as the possibility of bias, and the grouping of patients is not completely random. Further studies with a large size or multiple centers as well as longer follow-up are needed to confirm this outcome.
Acknowledgment
This study was financially supported by the Project of the Huzhou Municipal Science and Technology Bureau of Zhejiang Province (No 2018GYB29), which provided funding for publication fees.
Disclosure
The authors report no conflicts of interest in this work.
References
Rotas MA, Haberman S, Levgur M. Cesarean scar ectopic pregnancies: etiology, diagnosis, and management. Obstet Gynecol. 2006;107(6):1373–1381. | ||
Khunda A, Tay J. Caesarean scar pregnancy. BJOG: An International J Obstet Gynecol. 2007;114(10):1304. | ||
Vial Y, Petignat P, Hohlfeld P. Pregnancy in a cesarean scar. Ultrasound Obstet Gynecol. 2000;16(6):592–593. | ||
Maheux-Lacroix S, Li F, Bujold E, Nesbitt-Hawes E, Deans R, Abbott J. Cesarean scar pregnancies: a systematic review of treatment options. J Minim Invasive Gynecol. 2017;24(6):915–925. | ||
Kim YS, Han K, Kim MD, et al. Uterine Artery Embolization for pedunculated subserosal leiomyomas: evidence of safety and efficacy. J Vasc Interv Radiol. 2018;29(4):497–501. | ||
Kondo W, Tessmann Zomer M, Erzinger FL. Uterine arteriovenous fistula after perforation during the placement of an intrauterine device – Minimally invasive treatment using uterine artery embolization. Clin Exp Obstet Gynecol. 2016;43(4):602–605. | ||
Liu Z, Wang Y, Yan J, et al. Uterine artery embolization versus hysterectomy in the treatment of refractory postpartum hemorrhage: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2018;1(17):1–13. | ||
Tumenjargal A, Tokue H, Kishi H. Uterine artery embolization combined with dilation and curettage for the treatment of cesarean scar pregnancy: efficacy and future fertility. Cardiovasc Intervent Radiol. 2018;41(8):1165–1173. | ||
Qiao B, Zhang Z, Li Y. Uterine artery embolization versus methotrexate for cesarean scar pregnancy in a Chinese population: a meta-analysis. J Minim Invasive Gynecol. 2016;23(7):1040–1048. | ||
Ouyang Z, Yin Q, Xu Y. Heterotopic cesarean scar pregnancy diagnosis, treatment, and prognosis. J Ultras Med. 2014;33(9):1533–1537. | ||
Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy. A review (vol 207, pg 14, 2012). Am J Obstet Gynecol. 2014;210(4):371–374. | ||
Cao S, Zhu L, Jin L, Gao J, Chen C. Uterine artery embolization in cesarean scar pregnancy: safe and effective intervention. Chin Med J. 2014;127(12):2322–2326. | ||
Gao L, Huang Z, Gao J, Mai H, Zhang Y, Wang X. Uterine artery embolization followed by dilation and curettage within 24 hours compared with systemic methotrexate for cesarean scar pregnancy. Int J Gynaecol Obstet. 2014;127(2):147–151. | ||
Li Y, Wang W, Yang T, Wei X, Yang X. Incorporating uterine artery embolization in the treatment of cesarean scar pregnancy following diagnostic ultrasonography. Int J Gynaecol Obstet. 2016;134(2):202–207. | ||
Wang Y, Xu B, Dai S, Zhang Y, Duan Y, Sun C. An efficient conservative treatment modality for cervical pregnancy: angiographic uterine artery embolization followed by immediate curettage. Am J Obstet Gynecol. 2011;204(1):31.e1–e7. | ||
Bayoglu Tekin Y, Mete Ural U, Balık G, et al. Management of cesarean scar pregnancy with suction curettage: a report of four cases and review of the literature. Arch Gynecol Obstet. 2014;289(6):1171–1175. | ||
He Y, Wu X, Zhu Q, et al. Combined laparoscopy and hysteroscopy vs. uterine curettage in the uterine artery embolization-based management of cesarean scar pregnancy: a retrospective cohort study. BMC Womens Health. 2014;14(116):116. | ||
Wang CX, Wang J, Chen YY, et al. Randomized controlled study of the safety and efficacy of nitrous oxide-sedated endoscopic ultrasound-guided fine needle aspiration for digestive tract diseases. World J Gastroenterol. 2016;22(46):10242–10248. | ||
Wang CJ, Yuen LT, Chao AS, Lee CL, Yen CF, Soong YK. Caesarean scar pregnancy successfully treated by operative hysteroscopy and suction curettage. BJOG. 2005;112(6):839–840. | ||
Deans R, Abbott J. Hysteroscopic management of cesarean scar ectopic pregnancy. Fertil Steril. 2010;93(6):1735–1740. | ||
Chao A, Wang TH, Wang CJ, Lee CL, Chao AS. Hysteroscopic management of cesarean scar pregnancy after unsuccessful methotrexate treatment. J Minim Invasive Gynecol. 2005;12(4):374–376. | ||
Fleisch MC, Lux J, Schoppe M, Grieshaber K, Hampl M. Placenta percreta leading to spontaneous complete uterine rupture in the second trimester. Example of a fatal complication of abnormal placentation following uterine scarring. Gynecol Obstet Invest. 2008;65(2):81–83. | ||
van der Voet LF, Bij de Vaate AM, Veersema S, Brölmann HA, Huirne JA. Long-term complications of caesarean section. The niche in the scar: a prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG. 2014;121(2):236–244. | ||
Seals JG, Jones PA, Wolfe C. Uterine artery embolization as a treatment for symptomatic uterine fibroids: a review of literature and case report. J Am Acad Nurse Pract. 2006;18(8):361–367. | ||
Shen L, Tan A, Zhu H, Guo C, Liu D, Huang W. Bilateral uterine artery chemoembolization with methotrexate for cesarean scar pregnancy. Am J Obstet Gynecol. 2012;207(5):386.e1–e6. | ||
Hirakawa M, Tajima T, Yoshimitsu K, et al. Uterine artery embolization along with the administration of methotrexate for cervical ectopic pregnancy: technical and clinical outcomes. AJR Am J Roentgenol. 2009;192(6):1601–1607. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.