Back to Journals » Clinical Ophthalmology » Volume 20
Analysis of Ocular Biometric Differences Between Two Optical Biometers in High Myopia Cataract Patients: A Prospective Study
Authors Gong J, Yao Y, Li Y, Wu N, Zhu Y ![]() , Wang X
, Wang X
Received 12 September 2025
Accepted for publication 4 December 2025
Published 8 January 2026 Volume 2026:20 566911
DOI https://doi.org/10.2147/OPTH.S566911
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Bharat Gurnani
Jinping Gong,1– 4,* Yihua Yao,1– 5,* Yufei Li,1– 4 Nuozhou Wu,1– 4 Yihua Zhu,1– 4 Xiaohui Wang1– 4
1Department of Ophthalmology, The First Affiliated Hospital of Fujian Medical University, Fuzhou, People’s Republic of China; 2Department of Ophthalmology, National Regional Medical Center, Binghai Campus of the First Affiliated Hospital, Fujian Medical University, Fuzhou, People’s Republic of China; 3Department of Ophthalmology, Fujian Institute of Ophthalmology, Fuzhou, People’s Republic of China; 4Fujian Provincial Clinical Medical Research Center of Eye Diseases and Optometry, The First Affiliated Hospital of Fujian Medical University, Fuzhou, People’s Republic of China; 5Department of Ophthalmology, The Quangang General Hospital, Quanzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohui Wang, Department of Ophthalmology, The First Affiliated Hospital of Fujian Medical University, No. 20 Chazhong Road, Fuzhou, 350005, People’s Republic of China, Tel/Fax +86 0591 87981039, Email [email protected]
Purpose: To compare the differences and consistency of Lenstar LS 900 and IOL Master 700 in measuring ocular biometry for cataract patients with high myopia.
Patients and Methods: In this prospective study, 48 cataract patients (67 eyes) with high myopia were included. Paired comparisons were performed for axial length (AL), anterior chamber depth (ACD), lens thickness (LT), keratometry (K1, K2), corneal astigmatism (AST), and white-to-white distance (WTW) in IOL Master 700 and Lenstar LS 900. Agreement between devices was evaluated using Bland-Altman plots, and AL-based subgroup analysis was conducted using measurements from the IOL Master 700.
Results: Among the 67 eyes, AL measurement failed in 6 eyes with Lenstar LS 900 but in none with IOL Master 700. Mean inter-device differences were as follows: AL: 0.07 ± 0.11 mm (p = 0.001); ACD: − 0.02 ± 0.16 mm (p = 0.351); LT: − 0.02 ± 0.28 mm (p = 0.534); K1: − 0.03 ± 0.50 D (p = 0.658); K2: − 0.04 ± 0.47 D (p = 0.492); AST: − 0.03 ± 0.35 D (p = 0.492); WTW: − 0.13 ± 0.43 mm (p = 0.017). Two devices were highly correlated for AL, ACD, LT, K1, K2 and AST (ICC > 0.75). Bland-Altman analysis indicated high agreement, with 95% of differences within limits of agreement. No statistically significant difference was found in absolute IOL power prediction between devices.
Conclusion: In highly myopic cataract patients, IOL Master 700 shows a higher AL acquisition rate than Lenstar LS 900. Despite statistically significant differences in AL and WTW, no clinically relevant effect on refractive prediction was observed.
Keywords: cataract, high myopia, ocular optical measurement, IOL calculation
Introduction
In modern cataract surgery, patient expectations extend beyond vision restoration to achieving excellent visual acuity and quality.1,2 This shift has transformed the procedure into a refractive surgery aimed at optimal visual outcomes. In order to acquire optimal visual outcomes, the accurate preoperative ocular biometry is essential for evaluating the surgical eye and selecting the appropriate intraocular lens (IOL) power.3 It enables surgeons to optimize refractive results and enhance patient satisfaction, which makes the precise biometry more critical than ever in contemporary practice.4,5
With the rising prevalence of high myopia, cataract surgery in this patient group has become a significant societal concern.6 Studies indicate that cataract patients with high myopia experience more severe preoperative visual impairment, undergo surgery at a younger age, and have higher levels of anxiety, leading to greater expectations for postoperative visual quality.7 However, while the optical biometers have been validated in the general population, their measurement agreement and accuracy in cataract patients with high myopia—compromised by factors like elongated axial length, posterior staphyloma, and lens opacity—require further evaluation. Meanwhile, achieving ideal refractive outcomes in these patients is also particularly challenging. Pathological ocular changes and poor fixation often complicate preoperative biometry, leading to measurement errors.8 What troubles clinicians is the inability to accurately assess the patient’s ocular structures and calculate the correct IOL power. These inaccuracies in IOL power calculation can cause postoperative refractive surprises, hindering satisfactory visual outcomes. To enhance postoperative outcomes in these patients, current research has focused mainly on optimizing IOL power calculation formulas.9–11 These efforts aim to minimize refractive errors through formula improvements and preoperative compensation for myopia. However, no single formula has proven universally applicable, and undesirable hyperopic shifts remain common after surgery.
To tackle this challenge, our study compares two widely used optical biometers based on different principles—Lenstar LS 900 (Haag-Streit AG, Switzerland) and the IOL Master 700 (Carl Zeiss Meditec AG, Germany)—within highly myopic cataract patients and analyzes ocular biometric data from two devices. Our goal is to assess the consistency and discrepancies in biometric measurements between these devices. Through our study, we hope to offer clinicians better insight into ocular biometry in highly myopic eyes, supporting more precise surgical planning and improved postoperative visual quality for patients.
Materials and Methods
Study Design and Ethics
This study was a prospective, comparative study evaluating two optical biometers. The study was approved by the Medical Research and Clinical Technology Application Sub-Committee of the Ethics Committee of First Affiliated Hospital of Fujian Medical University (Approval No.: MTCA, FECFAH of FMU (12) 084–2) and adhered to the principles of the Declaration of Helsinki and its amendments. All patients were informed of the study’s purpose and provided informed consent.
Patient Enrollment
This study enrolled patients diagnosed with high myopia complicated by cataract who were admitted to The First Affiliated Hospital of Fujian Medical University between February 2024 and February 2025. These patients had a history of either high myopia (S.E < −6.00D) or Axial length (AL), >26 mm and clinically confirmed lens opacities. The patients exhibited decreased visual acuity that could not be corrected with glasses, which affect their daily lives and met the indications for surgery. The exclusion criteria included eyes with retinal or macular pathologies, a history of corneal disease, previous ocular surgery, ocular trauma, or prior intraocular lens implantation. Based on the previous studies,12 the sample size calculation performed to detect a mean difference of 0.01 mm of AL with a standard deviation of 0.02 mm. Using a 2-sided level of significance (α) at 0.05 and power (β) at 90%, revealed a minimum sample size of 48 is needed for each group within a paired analysis. Ultimately, 48 patients (67 eyes) were recruited in the study.
Measurement Protocol
The two optical biometrys is IOL Master 700 is based on the principle of swept source optical coherence tomography (SS-OCT) and Lenstar LS 900 is a newly developed biometry device that uses the principle of low-coherence reflectometry (OLCR). After enrollment, all patients were examined by the same experienced optometrist in the same examination room. The Lenstar LS 900 optical biometer and the IOL Master 700 were used in a random order to measure AL, anterior chamber depth (ACD), lens thickness (LT), average corneal curvature (K1, K2), corneal astigmatism (AST), and white-to-white distance (WTW). Measurements with poor signal quality or obvious outliers were excluded and re-measured. Then, three consecutive measurements were taken for each eye with each device, and the average of the three measurements was recorded as the final value for statistical analysis. Finally, the other surgeon will select the appropriate type and power of IOL based on patients’ personal needs and ocular biometry measurements. All patients underwent phacoemulsification cataract extraction with primary IOL implantation.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics Version 22.0 (IBM Corp., Armonk, NY, USA). Performing the Shapiro–Wilk test find that the data follow a normal distribution, then the paired t-tests were used to analyze whether there were significant differences between the two devices. Bland-Altman plots were used to graphically assess the agreement between the two devices. p-value < 0.05 was considered statistically significant.
Results
The demographic data of the patients are shown in Table 1. A total of 48 cataract patients (67 eyes) were included. Among them, 22 were male (30 eyes) and 26 were female (37 eyes); 34 were right eyes and 33 were left eyes. The patients’ ages ranged from 31 to 86 years, with a mean age of 55.09 ± 12.18 years. The duration of cataract history at the time of range from 0.1 to 20 years, with a mean of (2.03 ± 3.01) years. The history of high myopia ranged from 10 to 50 years, with a mean of (19.33 ± 8.52) years. The mean visual acuity (VA) of the examined eyes was (1.54 ± 0.36) LogMAR, and the best-corrected visual acuity (BCVA) was (0.69 ± 0.59) LogMAR. The detailed information is presented in Table 1.
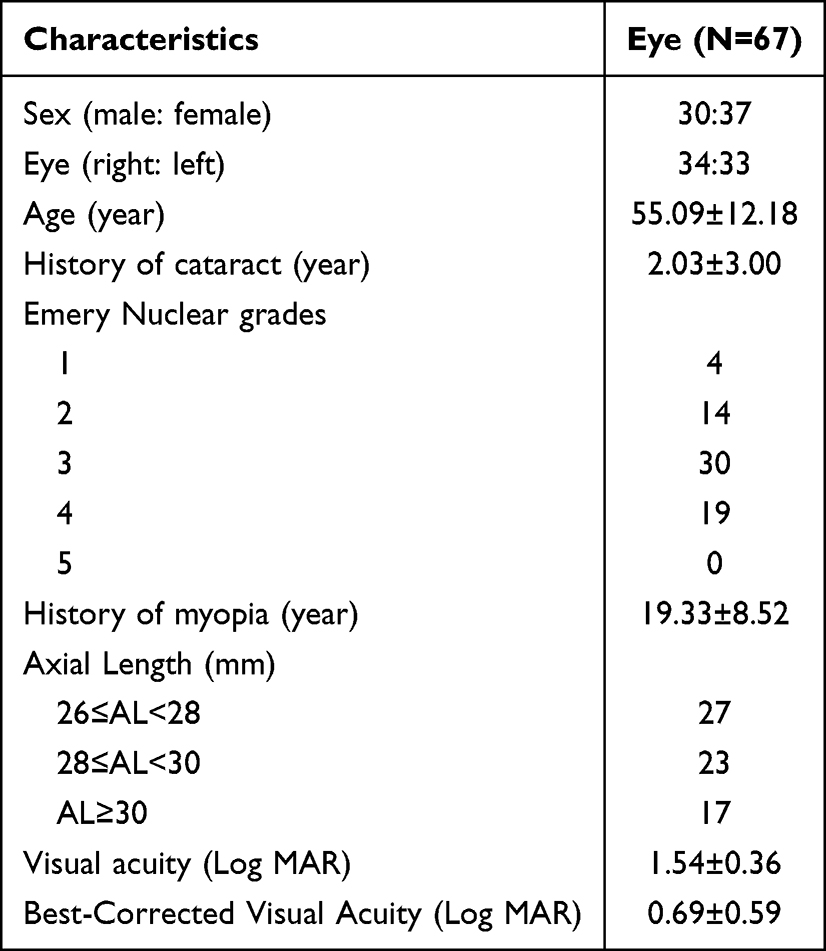 |
Table 1 Patients’ Characteristics and Perioperative Data |
The performance of the two apparatuses in ocular biometry is shown in Table 2. In a comparative analysis of ocular biometric measurements from 67 eyes with high myopia complicated by cataract, the detection rate of AL was 91.04% using the Lenstar LS 900 and 100% using the IOL Master 700, a difference that was statistically significant (P = 0.028). In contrast, no statistically significant differences were observed in the detection rates of ACD (P = 1.000), LT (P = 0.619), K1 (P=NS), K2 (P=NS),AST (P=NS), or WTW (P = 0.208) between the two devices.
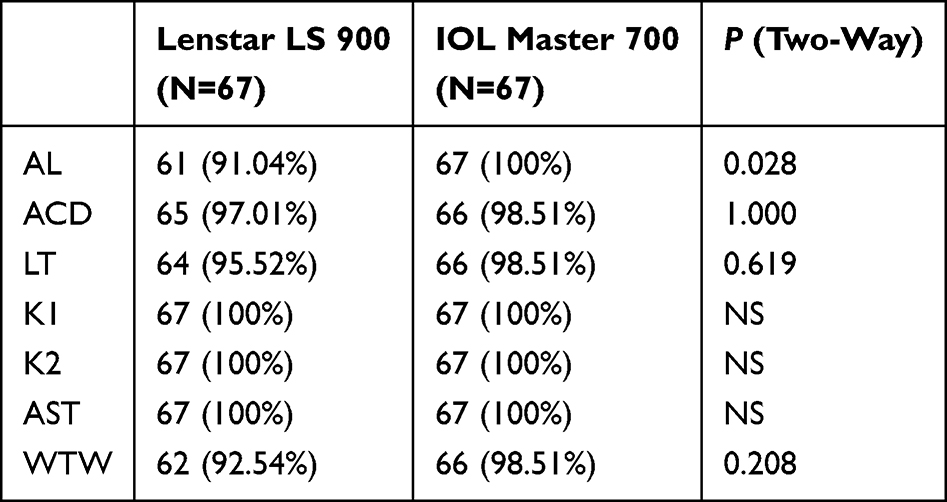 |
Table 2 The Number of Detections in Each of the Patient’s Ocular Biodata in the Lenstar LS 900 and IOL Master 700 |
The mean measurements with two optical ocular biometry devices are shown in Table 3. In cataract patients with high myopia, the mean AL measured by the Lenstar LS 900 and IOLMaster 700 was (28.80 ± 1.92) mm and (28.72 ± 1.90) mm, respectively. The mean ACD was (3.40 ± 0.41) mm and (3.42 ± 0.40) mm, LT was (4.27 ± 0.49) mm and (4.29 ± 0.45) mm, K1 was (42.92 ± 1.35) D and (42.95 ± 1.32) D, K2 was (44.15 ± 1.40) D and (44.19 ± 1.33) D, AST was (1.22 ± 0.84) D and (1.25 ± 0.87) D, and WTW was (11.74 ± 0.54) mm and (11.88 ± 0.47) mm, respectively. The mean difference in AL and WTW were (0.07 ± 0.11) mm (Lenstar LS 900 vs IOL Master 700, P = 0.001) and (−0.13 ± 0.43) mm (Lenstar LS 900 vs IOL Master 700, P = 0.017). In contrast, the mean differences in ACD, LT, K1, K2, and AST were not statistically significant (P > 0.05).
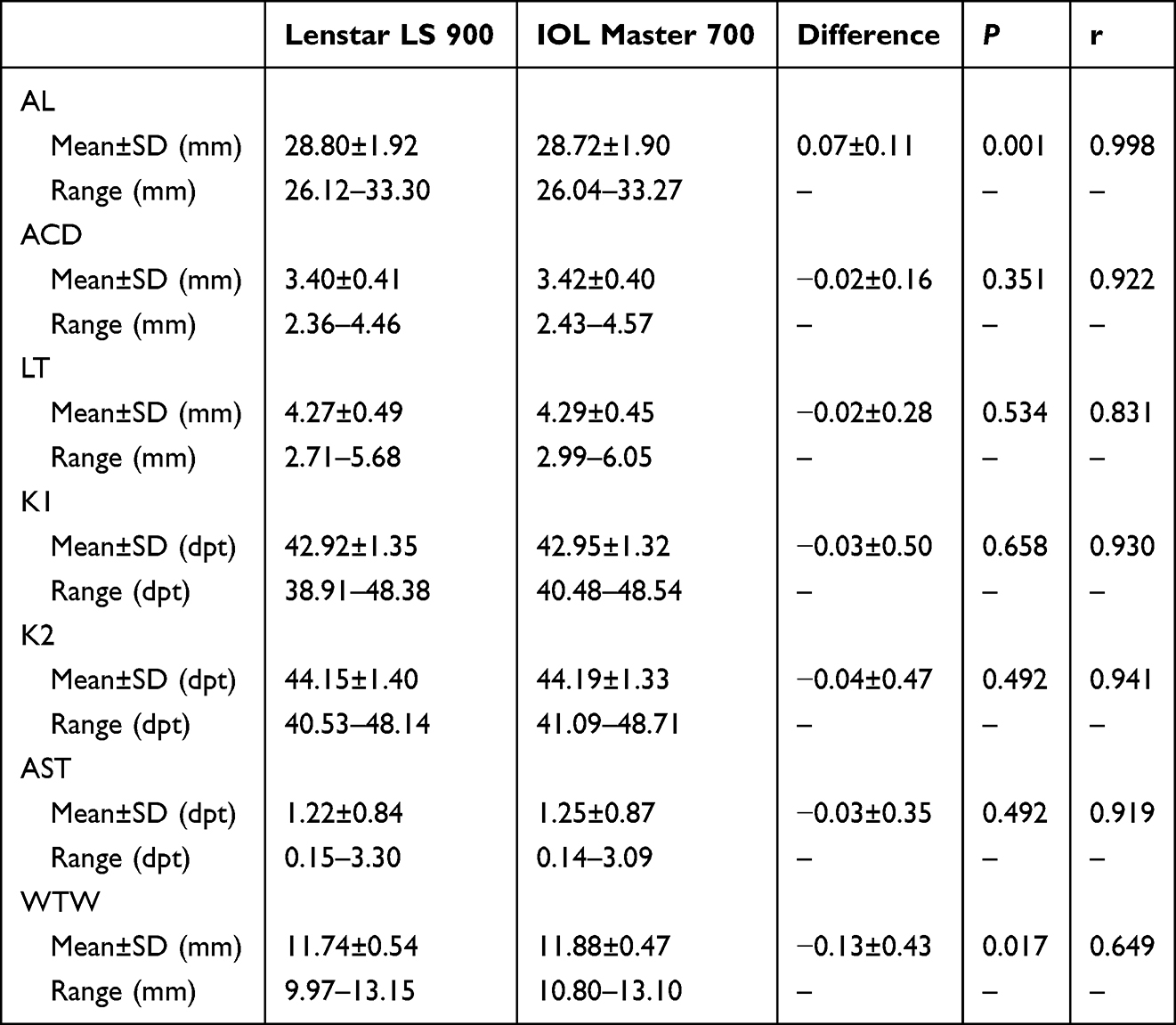 |
Table 3 Biometry Measurements by Lenstar LS 900 and IOL Master 700 |
Patients were stratified into three groups according to axial length (AL) for intergroup comparisons: a long AL group (26 mm ≤ AL < 28 mm), an ultra-long AL group (28 mm ≤ AL < 30 mm), and an extremely long AL group (AL ≥ 30 mm) Figure 1. The interdevice differences in AL measurements between the Lenstar LS 900 and IOL Master 700 were significantly different across all groups. Specifically, the mean difference was (0.04 ± 0.08) mm in the long AL group (Lenstar LS 900 vs IOL Master 700, P = 0.010), (0.09 ± 0.15) mm in the ultra-long AL group (Lenstar LS 900 vs IOL Master 700, P = 0.011), and (0.09 ± 0.07) mm in the extremely long AL group (Lenstar LS 900 vs IOL Master 700, P =0.0004).
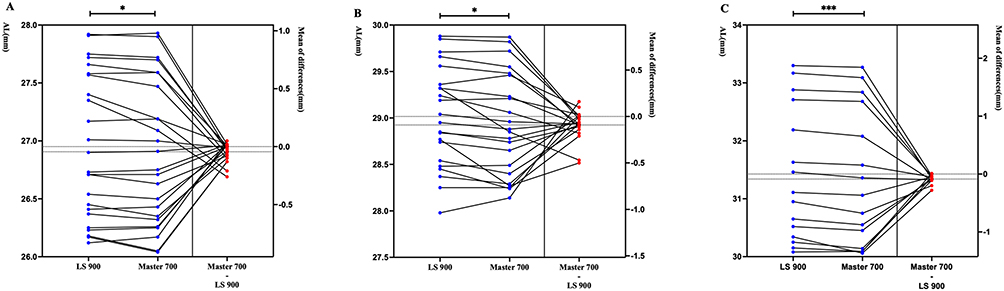 |
Figure 1 Comparison of axial length (AL) measurements between Lenstar LS 900 and IOL Master 700 in different AL subgroups. Note: The central solid line represents the mean difference between devices, with the upper and lower dashed lines indicating the 95% limits of agreement (±1.96 SD). (A) Long eyes group (26mm≤AL<28mm). (B) Very long eyes group (28mm≤AL<30mm). (C) Extremely long eyes group (AL≥30mm). Paired t-test; * P<0.05; *** P<0.001. |
Figure 2 shows Bland-Altman plots for AL, ACD, LT, K, AST, and WTW between the two devices. All plots show a high level of agreement and 95% limits of agreement for the ocular parameters measured by the two instruments.
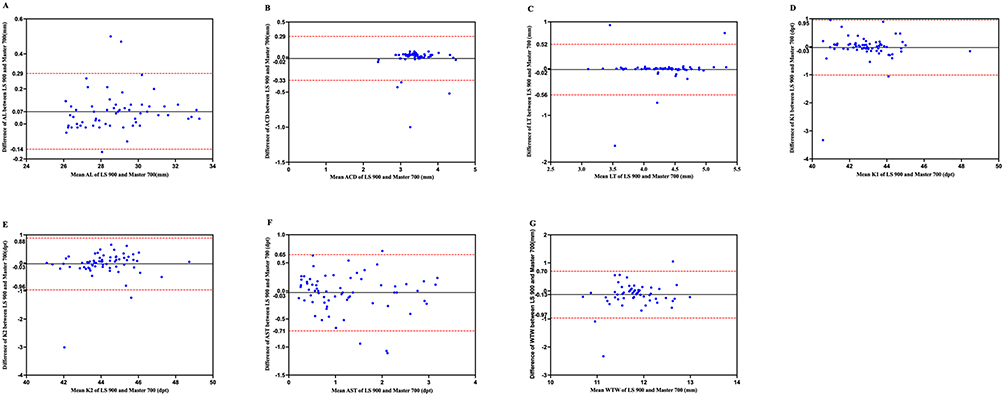 |
Figure 2 Bland-Altman plots comparing ocular biometric measurements between Lenstar LS 900 and IOL Master 700. Notes: The central solid line indicates the mean difference between devices, with the upper and lower dashed lines representing the 95% limits of agreement (mean difference ±1.96 standard deviation). (A) Axial length (AL); (B) Anterior chamber depth (ACD); (C) Lens thickness (LT) (D) Flat keratometry (K1); (E) Steep keratometry (K2); (F) Corneal astigmatism (AST); (G) White-to-white corneal diameter (WTW). |
Subsequently, the surgeon comprehensively analyzed the patient’s medical history and the results from both examinations. Then the surgeon selected the ocular biometric data obtained from either the Lenstar LS 900 or the IOL Master 700 to calculate the IOL power by using the Barrett Universal II formula. After getting a suitable IOL power, we repeated the same calculation formula with another set of ocular biometric measurements to get the same IOL power. When the same IOL power was selected, the predicted residual spherical equivalent (S.E.) was (−2.64 ± 2.06) D for the Lenstar LS 900 and (−2.59 ± 2.10) D for the IOL Master 700 by using the Barrett Universal II formula. The difference in the predicted residual S.E. between the two devices was (−0.06 ± 0.32) D, which was not statistically significant (P = 0.169).
Discussion
This prospective comparative study evaluated two optical biometers (Lenstar LS 900 and IOL Master 700) for ocular biometry in cataract patients with highly myopia. The IOL Master 700 exhibited a significantly higher detection rate for AL than the Lenstar LS 900, while no significant differences were found in the detection rates of ACD, LT, K1, K2, AST, or WTW. Regarding measurement values, AL was greater with the Lenstar LS 900, whereas WTW was smaller, compared to the IOL Master 700. No other parameters showed significant inter-device differences. Importantly, the use of biometric data from either device in IOL power calculation yielded comparable postoperative refractive outcomes, with no significant difference in residual S.E.
In recent decades, advances in ocular biometry have enhanced the precision of preoperative measurements in cataract and refractive surgery. However, inconsistencies in results persist due to differences in measurement principles across devices,4 underscoring the need for comparative evaluations. Most previous studies have focused on general or cataract-only populations and examined only a limited set of parameters, such as AL,13 leaving broader biometric comparisons underexplored. For instance, in a study comparing the IOL Master 500, IOL Master 700, and Lenstar LS 900 in a general cataract population, Jae et al14 found no significant difference in detection rates between the IOL Master 700 and Lenstar LS 900. While AL measurements from the Lenstar LS 900 were longer than those from both IOL Master, ACD and K-values did not differ significantly between the IOL Master 700 and Lenstar LS 900.
Whether these findings extend to highly myopic cataract patients remain unclear. This group is at increased risk of postoperative refractive accidences, the causes of which are not well understood. Although modified IOL formulas have been proposed to improve refractive accidences, they are often validated using data from a single type of optical biometer, limiting their applicability across devices based on different optical principles. To bridge this gap, our study systematically evaluates seven key biometric parameters obtained from multiple optical biometers in a cohort of highly myopic cataract patients. By analyzing inter-device agreement and discrepancies, we aim to provide an evidence base to help clinicians optimize formula parameters and IOL power selection according to the specific biometer used.
Lenstar LS 900 and IOL Master 700, as two of the commonly advanced optical biometers, have demonstrated extensive validation in terms of measurement accuracy across populations. The Lenstar LS 900 is a non-contact optical biometer utilizing OLCR.15 It employs an 820 nm superluminescent diode to measure axial length by analyzing reflections between the corneal surface and retina. The device also functions as a dual-zone keratometer, using 32 points across two optical zones to assess corneal curvature and astigmatism. Its OLCR technology provides precise differentiation of ocular interfaces with minimal signal loss, enabling comprehensive anterior segment measurement in a single acquisition.15 The IOL Master 700 employs SS-OCT with a 1055 nm laser scanning at 2000 times per second.16 This technology enhances signal-to-noise ratio and tissue penetration, improving reliability in eyes with lens opacities. It features telecentric keratometry using an 18-point triple-ring pattern and integrates anterior segment OCT with fixation technology to measure both anterior and posterior corneal curvature for full refractive power analysis.4
Our study shows that the IOL Master 700 exhibited a significantly higher detection rate for AL than the Lenstar LS 900. In previous general population studies, no significant differences were detected in the detection rates among different types of optical eye measurement instruments based on different principles.13,16 In our study, however, the AL detection rate of the IOL Master 700 was found to be higher than that of the Lenstar LS 900 among cataract patients with high myopia. We suggests that the IOL Master 700, which employs a 1055 nm laser, offers improved penetration through opacified lenses relative to the 820 nm light source used by the Lenstar, thereby reducing interference from turbid media and enhancing AL acquisition. Consequently, when using the Lenstar LS 900 in such cases, prolonged measurement time may be required, and AL data may still not be obtainable in all instances. It is noteworthy that both devices showed limited efficacy in cases of grade 5 nuclear cataracts, underscoring the ongoing necessity of acoustic biometry in patients with advanced lens opacity.17 Enhancing the penetration of optical biometers and minimizing the impact of media opacities remain critical objectives for improving the accuracy and success rate of ocular biometry.
Consistent with studies conducted in pure cataract populations,18 our research also indicates that the AL measured by the Lenstar LS 900 is longer than that by the IOL Master 700 in eyes with high myopia complicated by cataract. Potential explanations include differences in measurement principles and signal processing in irregular ocular media. In the absence of a gold standard for AL assessment, the absolute accuracy of either device remains uncertain in highly myopic eyes. These findings indicate that current optical biometers lack absolute consistency in this population and underscore the need for device-specific AL adjustment rules to optimize intraocular lens power calculation accuracy.19
Our study shows that Significant differences in WTW measurements were observed between the two devices, which is consistent with previous studies conducted in populations with mild to moderate cataracts.20,21 As WTW is critical for IOL calculation using the Barrett Universal II formula and influences effective lens position, its accurate assessment is essential.10 Both devices determine WTW by analyzing digital ocular images based on the contrast between the iris and sclera.22 However, this boundary can be ambiguous and susceptible to variations in illumination. To mitigate environmental effects, all measurements were conducted sequentially under consistent lighting conditions. We attribute the observed discrepancies primarily to differences in illumination wavelengths and resolution: the IOL Master 700 employs an 830 nm near-infrared source, while the Lenstar LS 900 uses 820 nm, both with lateral resolutions of 20–30 μm, though actual performance depends on optical design and sampling density.23 Additionally, poor fixation in highly myopic cataract patients may further reduce image clarity and measurement reproducibility.24,25 These findings suggest that WTW measurements exhibit higher variability in highly myopic eyes, and values from different devices should not be used interchangeably. Enhancing the accuracy of WTW assessment is crucial for improving biometry quality and IOL prediction precision.
No significant differences were detected in other biometric parameters—including ACD, LT, K1, K2, and AST—between the two devices in highly myopic cataract patients. For ACD and LT, the IOL Master 700 employs SS-OCT-based longitudinal scanning, whereas the Lenstar LS 900 acquires these metrics in a single integrated measurement. The comparable results indicate that both technologies provide sufficient penetration and accuracy for anterior segment evaluation. Similarly, despite differing methodologies for corneal curvature—IOL Master 700 uses telecentric keratometry with 18 points across three zones, and Lenstar employs dual-zone keratometry with 32 points—both devices yielded consistent K1, K2, and AST values, demonstrating reliability in assessing corneal refractive power.
This study has several limitations. First, the inclusion of patients with mixed cataract types precluded a classification-based comparison of device success rates. Second, despite meeting sample size requirements, the cohort remains relatively small. Third, while we compared the theoretical accuracy of IOL calculations derived from biometric data obtained with the IOL Master 700 and Lenstar LS 900, the actual postoperative outcomes following IOL implantation were not assessed, limiting the clinical applicability of our findings. Future work will include follow-up of patients receiving the same IOL to evaluate practical differences in prediction accuracy between the two devices. Finally, although the only use of the Barrett Universal II formula—selected for its established stability in the cataract with high myopia—facilitated result comparison, future studies should incorporate additional formulas tailored to high myopic cataract to improve generalizability.
Conclusion
This study compared ocular biometric measurements from two optical biometers based on different principles—the Lenstar LS 900 and the IOL Master 700—in patients with high myopia and cataracts. The key findings including: Firstly, The IOL Master 700 demonstrated a higher acquisition rate for AL than the Lenstar LS 900. Secondly, Significant differences were observed in AL and WTW measurements between devices, highlighting the need for careful interpretation in clinical practice and IOL formula adjustments. Thirdly, both devices provided consistent IOL power calculations using the Barrett Universal II formula, supporting their reliability.
Data Sharing Statement
Data supporting this study are available from the corresponding author upon reasonable request under institutional data sharing protocols.
Ethics Approval and Consent to Participate
This research protocol received ethical approval from the Medical Research and Clinical Technology Application Sub-Committee of the Ethics Committee of First Affiliated Hospital of Fujian Medical University (Approval No.: MTCA, FECFAH of FMU (12)084-2), and all procedures strictly adhered to the ethical principles outlined in the Declaration of Helsinki.
Acknowledgments
The authors extend sincere gratitude to all clinical participants whose invaluable engagement in surgical protocols and postoperative assessments directly informed the refinement of ophthalmic operative techniques. Special recognition is accorded to nursing teams for their meticulous coordination of perioperative care, which ensured protocol adherence across all study phases.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by grants from the Joint Funding Project of Science and Technology Innovation from the Fujian Provincial Department of Science and Technology (No. 2023Y9027, Yao Yihua), the Fujian Provincial Clinical Medical Research Center for Eye Diseases and Optometry (YK-YJZX, Zhu Yihua), the Science and Technology Innovation Joint Fund Project of the Fujian Provincial Department of Science and Technology (No. 2021Y9013, Wang Xiaohui), and the Natural Science Foundation of Fujian Province (No. 2023J01591, Wang Xiaohui, No.2025J0112, Yao Yihua).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Chang DF. The continuing evolution of cataract surgery. Asia Pac J Ophthalmol. 2017;6(4):308. doi:10.22608/APO.2017191
2. Liu Y-C, Wilkins M, Kim T, Malyugin B, Mehta JS. Cataracts. Lancet. 2017;390(10094):600–9. doi:10.1016/S0140-6736(17)30544-5
3. Rong X, He W, Zhu Q, Qian D, Lu Y, Zhu X. Intraocular lens power calculation in eyes with extreme myopia: comparison of Barrett Universal II, Haigis, and Olsen formulas. J Cataract Refract Surg. 2019;45(6):732–737. doi:10.1016/j.jcrs.2018.12.025
4. Zarei-Ghanavati S, Nikpayam M, Namdari M, Bakhtiari E, Hassanzadeh S, Ziaei M. Agreement between a spectral-domain ocular coherence tomography biometer with a swept-source ocular coherence tomography biometer and an optical low-coherence reflectometry biometer in eyes with cataract. J Curr Ophthalmol. 2023;35(2):153–158. doi:10.4103/joco.joco_30_23
5. Moshirfar M, Buckner B, Ronquillo YC, Hofstedt D. Biometry in cataract surgery: a review of the current literature. Curr Opin Ophthalmol. 2019;30(1):9–12. doi:10.1097/ICU.0000000000000536
6. Wu P-C, Huang H-M, Yu H-J, Fang P-C, Chen C-T. Epidemiology of Myopia. Asia Pac J Ophthalmol. 2016;5(6):386–393. doi:10.1097/APO.0000000000000236
7. Tan Y, Liu L, Li J, Qin Y, Sun A, Wu M. Effect of cataract surgery on vision-related quality of life among cataract patients with high myopia: a prospective, case-control observational study. Eye. 2022;36(8):1583–1589. doi:10.1038/s41433-021-01697-6
8. Ravalico G, Michieli C, Vattovani O, Tognetto D. Retinal detachment after cataract extraction and refractive lens exchange in highly myopic patients. J Cataract Refract Surg. 2003;29(1):39–44. doi:10.1016/s0886-3350(02)01508-0
9. Popovic M, Schlenker MB, Campos-Möller X, Pereira A, Ahmed IIK. Wang-Koch formula for optimization of intraocular lens power calculation: evaluation at a Canadian center. J Cataract Refract Surg. 2018;44(1):17–22. doi:10.1016/j.jcrs.2017.09.035
10. Roberts TV, Hodge C, Sutton G, Lawless M. Comparison of Hill-radial basis function, Barrett Universal and current third generation formulas for the calculation of intraocular lens power during cataract surgery. Clin Exp Ophthalmol. 2018;46(3):240–246. doi:10.1111/ceo.13034
11. Wang L, Shirayama M, Ma XJ, Kohnen T, Koch DD. Optimizing intraocular lens power calculations in eyes with axial lengths above 25.0 mm. J Cataract Refract Surg. 2011;37(11):2018–2027. doi:10.1016/j.jcrs.2011.05.042
12. Hoffer KJ, Hoffmann PC, Savini G. Comparison of a new optical biometer using swept-source optical coherence tomography and a biometer using optical low-coherence reflectometry. J Cataract Refract Surg. 2016;42(8):1165–1172. doi:10.1016/j.jcrs.2016.07.013
13. McAlinden C, Wang Q, Pesudovs K, et al. Axial length measurement failure rates with the IOLMaster and Lenstar LS 900 in eyes with cataract. PLoS One. 2015;10(6):e0128929. doi:10.1371/journal.pone.0128929
14. Jeon S, Kim HS. Clinical characteristics and outcomes of cataract surgery in highly myopic Koreans. Korean J Ophthalmol. 2011;25(2):84–89. doi:10.3341/kjo.2011.25.2.84
15. Arriola-Villalobos P, Almendral-Gómez J, Garzón N, et al. Agreement and clinical comparison between a new swept-source optical coherence tomography-based optical biometer and an optical low-coherence reflectometry biometer. Eye. 2017;31(3):437–442. doi:10.1038/eye.2016.241
16. Song JS, Yoon DY, Hyon JY, Jeon HS. Comparison of ocular biometry and refractive outcomes using IOL Master 500, IOL Master 700, and Lenstar LS900. Korean J Ophthalmol. 2020;34(2):126–132. doi:10.3341/kjo.2019.0102
17. Kubo E, Kumamoto Y, Tsuzuki S, Akagi Y. Axial length, myopia, and the severity of lens opacity at the time of cataract surgery. Arch Ophthalmol. 2006;124(11):1586–1590.
18. Epitropoulos A. Axial length measurement acquisition rates of two optical biometers in cataractous eyes. Clin Ophthalmol. 2014;8:1369–1376. doi:10.2147/OPTH.S62653
19. Geggel HS. Comparison of formulas and methods for high myopia patients requiring intraocular lens powers less than six diopters. Int Ophthalmol. 2018;38(4):1497–1504. doi:10.1007/s10792-017-0611-6
20. Domínguez-Vicent A, Pérez-Vives C, Ferrer-Blasco T, Albarrán-Diego C, Montés-Micó R. Interchangeability among five devices that measure anterior eye distances. Clin Exp Optom. 2015;98(3):254–262. doi:10.1111/cxo.12247
21. Hill W, Angeles R, Otani T. Evaluation of a new IOLMaster algorithm to measure axial length. J Cataract Refract Surg. 2008;34(6):920–924. doi:10.1016/j.jcrs.2008.02.021
22. Xi W, Yang M, Wan J, et al. Effect of pupil dilation on biometry measurements and intraocular lens power in eyes with high myopia. Front Med. 2022;9:963599. doi:10.3389/fmed.2022.963599
23. Arriola-Villalobos P, Almendral-Gómez J, Garzón N, et al. Effect of pharmacological pupil dilation on measurements and iol power calculation made using the new swept-source optical coherence tomography-based optical biometer. J Fr Ophtalmol. 2016;39(10):859–865. doi:10.1016/j.jfo.2016.09.003
24. Abdi P, Atighehchian M, Farsiani AR. Comparison of corneal measurements using two different Scheimpflug analyzers in Sirius and Pentacam devices. Sci Rep. 2023;13(1):16956. doi:10.1038/s41598-023-44133-3
25. McCarty CA, Livingston PM, Taylor HR. Prevalence of myopia in adults: implications for refractive surgeons. J Refract Surg. 1997;13(3):229–234. doi:10.3928/1081-597X-19970501-08
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Visual Outcomes and Complication Rates of Cataract Surgery in Asian High Myopic Patients: A Meta-Analysis and Systematic Review
Zhao KB, Zhang JS, Wan XH
Clinical Ophthalmology 2025, 19:2239-2248
Published Date: 12 July 2025