Back to Journals » International Journal of Women's Health » Volume 14
Analysis of Adverse Events and Medical Errors in Long-Term Hormone Treatments for Endometriosis: A Study Based on the US Food and Drug Administration Event Reporting System
Received 10 June 2022
Accepted for publication 29 August 2022
Published 6 September 2022 Volume 2022:14 Pages 1237—1250
DOI https://doi.org/10.2147/IJWH.S377418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marleen van Gelder
Yuxin Zhang, Yiping Zhu, Jing Sun
Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China
Correspondence: Jing Sun, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China, Tel +86 21 20261062, Fax +86 21 50730190, Email [email protected]
Purpose: To investigate adverse events and medical errors, as well as their possible risk factors, of combined oral contraceptives and progestins used in patients with endometriosis.
Patients and Methods: Reports between January 1, 2014 and September 30, 2021 about patients with endometriosis in US Food and Drug Administration Adverse Event Reporting System were analyzed. Disproportional analysis was performed with the Gamma-Poisson Shrinker model to detect overreported drug-event pairs. Logistic regression analysis was utilized to explore potential risk factors.
Results: There were 823 reports on long-term hormone treatments and 6247 reports on other drugs after removing duplicates, most of which were reported by consumers and were from the United States. Procedural complications and product issues were common among long-term hormone treatment users, while some other new adverse events emerged in subgroup analysis of different dosage forms of progestin. Polytherapy was negatively associated with off label use (adjusted OR = 0.47, 95% CI 0.22– 0.94) and product use in unapproved indication (adjusted OR = 0.36, 95% CI 0.15– 0.76) for combined oral contraceptive users. Combined oral contraceptive users aged greater than or equal to 30 were less likely to have product use issue (adjusted OR = 0.33, 95% CI 0.12– 0.82) but were at higher risk of pulmonary embolism (adjusted OR = 4.04, 95% CI 1.35– 17.43).
Conclusion: Long-term hormone treatment products in this study are generally safe for endometriosis, while newly detected signals need to be validated by further exploration. Patients’ tolerance and fertility desire should be considered when preparing treatment plans.
Keywords: adverse side effect, endometriosis, hormone therapy, pharmacovigilance
Introduction
As a hormone-dependent disease, endometriosis is observed in nearly 10% of women at reproductive age.1 Combined oral contraceptives (COCs) and progestins may be implemented as an alternative to surgery or a prevention of postoperative recurrence.2 They can be used alone or be recommended as add-back hormone therapies for patients using gonadotropin-releasing hormone (GnRH) analogues.3–5 Given that the efficacy of COCs and progestins have been widely acknowledged, they are suggested to be the reference comparator for randomized controlled trials on new endometriosis drugs.6
As suppressive solutions to endometriosis, COCs and progestins have similar efficacy in relieving pain and other symptoms,5 leaving them as the safest long-term treatment for endometriosis.7–9 However, patients’ tolerance could be highly personalized,10,11 not to mention that women with endometriosis have a higher rate of allergies on medication.12 In addition to painful symptoms, side effects may increase patients’ suffering.13,14 Patient compliance may be affected due to side effects, especially for the long courses of these hormone drugs,6 which could be detrimental to the management of the disease. There have been some real-world studies focusing on specific drugs for endometriosis, but they either produced negative result or concentrated on drug efficacy.15–17 Pharmacovigilance evidence determining adverse reactions of long-term hormone drugs for endometriosis are still inadequate.
Post-marketing adverse events reports of drugs and therapeutic biologic products that were submitted to US Food and Drug Administration (FDA) are stored in the FDA Adverse Event Reporting System (FAERS), providing materials for drug safety surveillance. Adverse events and medication errors in FAERS are recorded using Preferred Terms (PTs) in the Medical Dictionary for Regulatory Activities (MedDRA) terminology.18,19 This study portrayed reports about long-term hormone therapies for endometriosis in FAERS and performed a disproportional analysis, aimed at investigating drug-type-specific adverse events and exploring their possible risk factors.
Materials and Methods
Data Processing
FAERS reports from patients with endometriosis between Jan 1, 2014 and Sep 30, 2021 were retrieved (date of access: Mar 5, 2022). After removing duplicates, reports were filtered to select those whose diagnosis was coded as endometriosis or endometriosis ablation. Medications of interest in this study included COC, oral progestin, progestin-eluting intrauterine device (IUD), depot progestin, and progestin implant. Cases about these drugs and devices were extracted and were classified as the long-term hormone treatment group by filtering drug names and product active ingredients of the records. Cases whose indication were endometriosis but were treated without any of the drugs mentioned above were classified as the control group.
Statistical Analysis
We calculated counts and rates of major baseline characteristics in the long-term hormone treatment group and the control group separately. Gamma–Poisson Shrinker (GPS) model was used for disproportional analysis and to detect overreported drug-event pairs.20,21 This model represented relative reporting ratios by Empirical Bayes Geometric Mean (EBGM) scores after Bayesian shrinkage. EBGM score, 5th percentile (EB05), and 95% percentile (EB95), i.e. lower and upper limit of 90% confidence interval (CI), were calculated with R (version 4.0.4; The R Foundation for Statistical Computing, Vienna, Austria) and R package openEBGM (version 0.8.3). EB05 ≥ 2 was considered signal detected.22 According to MedDRA hierarchy,23 PTs whose signals were detected by disproportional analysis were presented in groups according to their primary System Organ Class (SOCs).
Considering the wide age distribution of the cases and that GnRH-analogue/antagonists, aromatase inhibitors, and analgesics are commonly co-administered, logistic regression analysis was performed to explore potential risk factors of the signals detected above. According to 10 events per variable recommendation on sample size for developing a clinical prediction model,24 events whose drug-event pair counts were greater than 20 were selected for logistic regression analysis. Logistic regression analysis was performed with R (version 4.0.4; The R Foundation for Statistical Computing, Vienna, Austria).
Results
Descriptive Analysis
Between January 1, 2014 and September 30, 2021, there were 1823 reports on long-term hormone treatment and 6247 reports on other drugs applied for endometriosis. Long-term hormone treatment accounted for 501 (27.5%) reports on COCs, 924 (50.7%) reports on oral progestin, 102 (5.6%) reports on depot progestin, 255 (14.0%) reports on progestin-eluting IUD, and 41 (2.2%) reports on progestin implant.
Clinical features of reports are presented in Table 1. The majority of women included were at their reproductive age. In the long-term hormone treatment group, most of the cases were reported from the United States (75.0%), followed by other countries (9.7%) and France (3.2%). While in the control group, most of the cases were reported from the United States (84.5%), followed by Canada (6.0%) and other countries (4.7%). Apart from the category of Other serious event, the most common outcome of both groups was hospitalization (17.2% in long-term hormone treatment group and 9.8% in the control group), and disability came in second (3.6% and 2.6%, respectively).
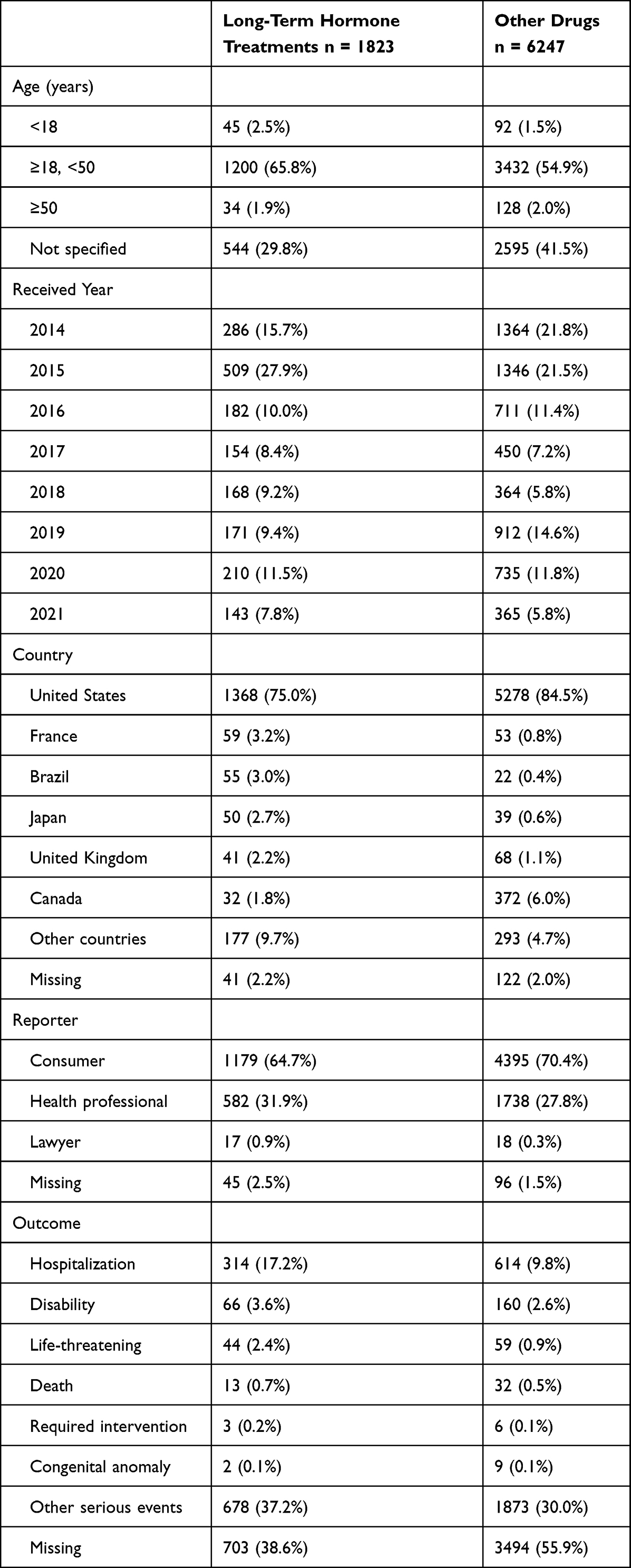 |
Table 1 Baseline Characteristics of Patients with Endometriosis |
Disproportional Analysis
In both COC and progestin groups, the most prevalent PT was off label use (N = 130 in the COC group, and N = 119 in progestin group), followed by product use in unapproved indication (N = 102 in the COC group, and N = 55 in progestin group). However, these 2 PTs were not overreported in progestin users (EB05 were 1.6 and 1.3, respectively). Overreported PTs among COC users were more diverse, while PTs among progestin users were mainly under the SOCs of injury, poisoning and procedural complications and product issues. Signals of some uncommon adverse events including eye disorders and nervous system disorders were detected, too (Table 2).
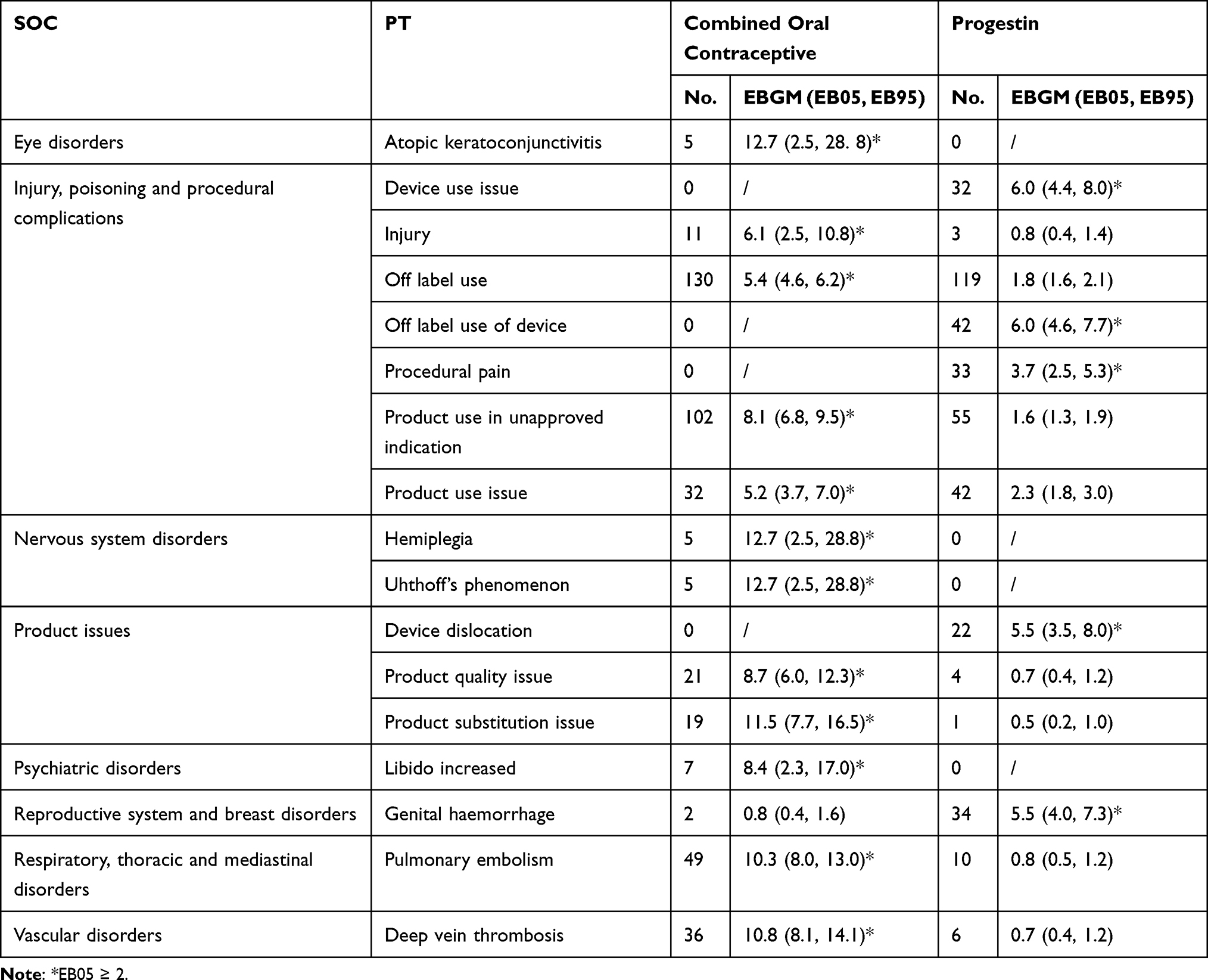 |
Table 2 Preferred Terms of Overreported Adverse Events and Medical Errors of Endometriosis Patients Receiving Long-Term Hormone Treatment |
Disproportional analysis was also performed in different dosage forms of progestin (Table 3). All signals detected in overall progestin users were specified in subgroups, and signals of some new adverse events such as cardiac disorders, gastrointestinal disorders, metabolism and nutrition disorders, and musculoskeletal disorders emerged in subgroup analysis. Among oral progestin users, only PTs of hepatic adenoma (N = 14, EB05 = 2.3), meningioma (N = 11, EB05 = 4.0), and ulnar tunnel syndrome (N = 11, EB05 = 4.6) were overreported. PTs belonging to injury, poisoning and procedural complications and product issues were mainly reported among progestin-eluting IUD users and depot progestin users. Besides, plenty of nervous system disorders occurred in the depot progestin subgroup. Most overreported PTs in the progestin implant subgroup were under the SOC of general disorders and administration site conditions.
 |  |  |
Table 3 Preferred Terms of Overreported Adverse Events and Medical Errors of Endometriosis Patients Receiving Different Dosage Forms of Progestin |
Risk Factors for Overreported Events
Logistic regression analysis indicated that among adverse events or medical errors that happened over 20 times, polytherapy was negatively associated with off label use (adjusted OR = 0.47, 95% CI 0.22−0.94) and product use in unapproved indication (adjusted OR = 0.36, 95% CI 0.15−0.76) for COC users. COC users aged greater than or equal to 30 were less likely to have product use issue (adjusted OR = 0.33, 95% CI 0.12−0.82) but were at higher risk of pulmonary embolism (adjusted OR = 4.04, 95% CI 1.35−17.43). Meanwhile, age greater than or equal to 30 and polytherapy seemed to have no statistical association with adverse events or medical errors in progestin-eluting IUD users. Detailed data are presented in Table 4.
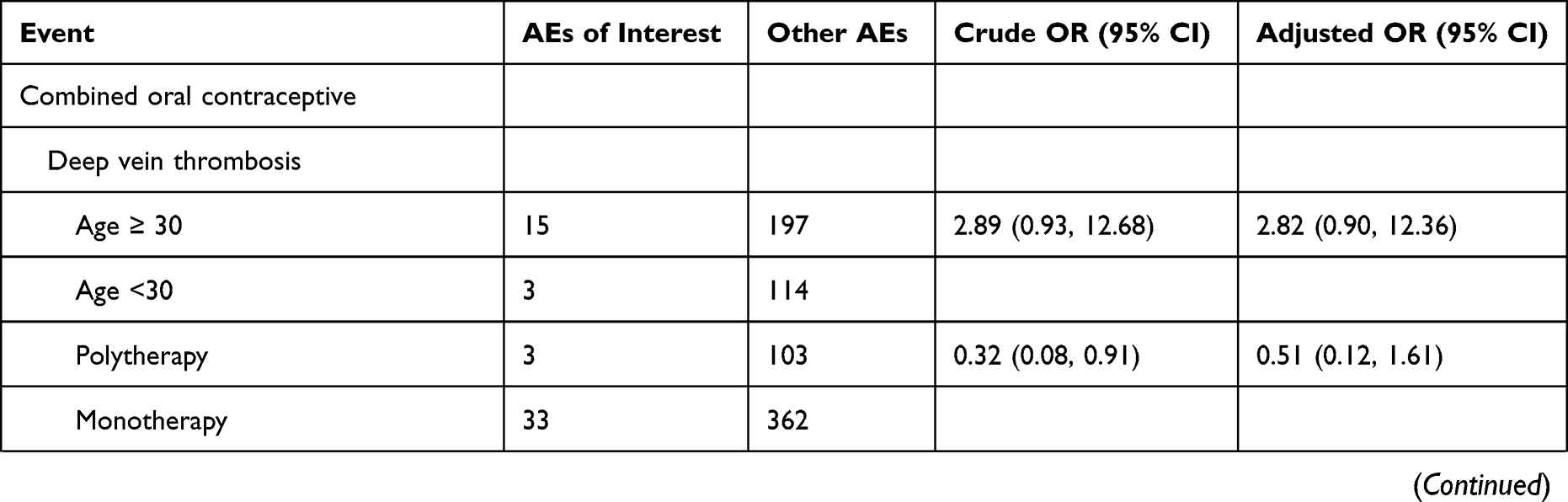 | 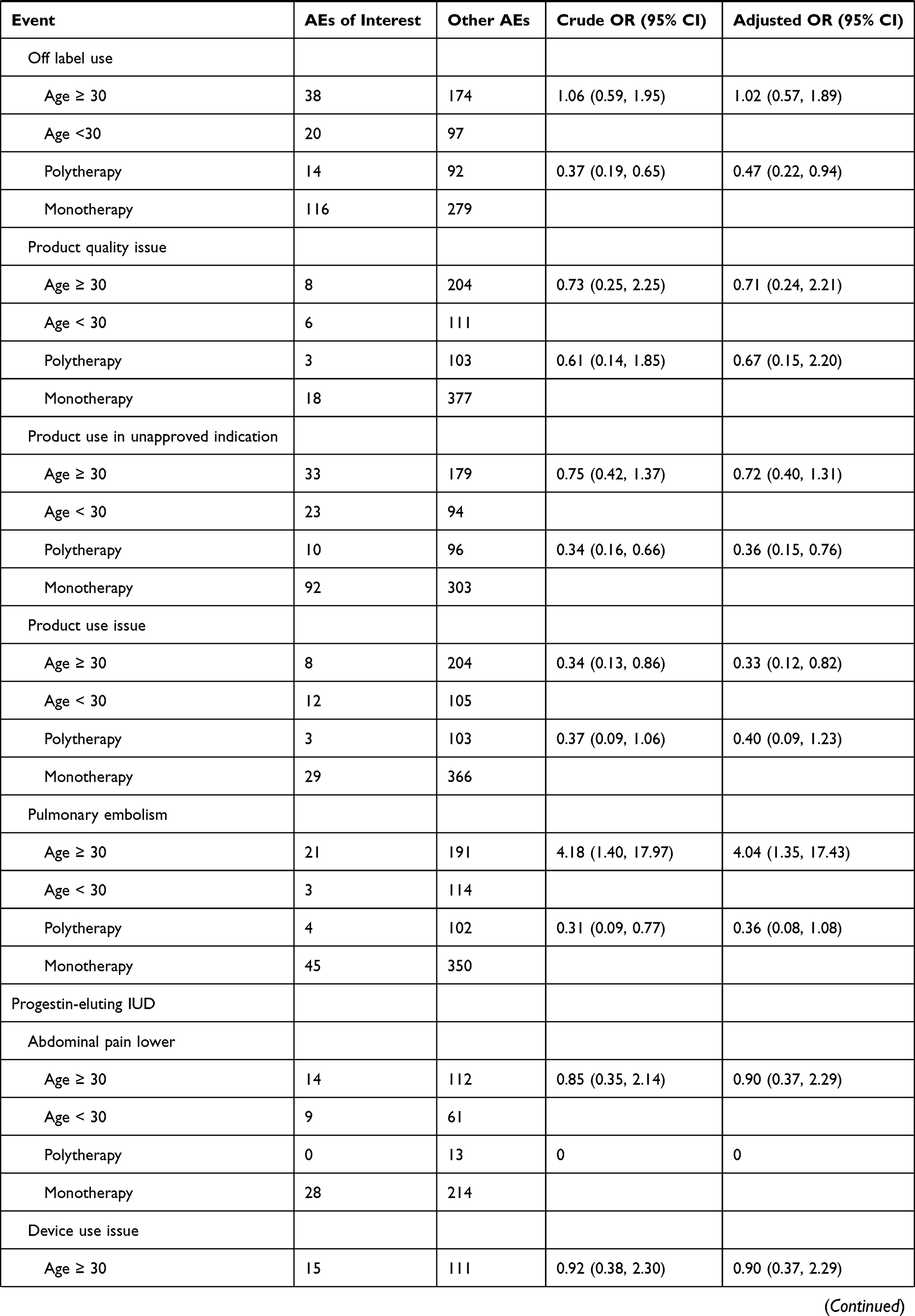 | 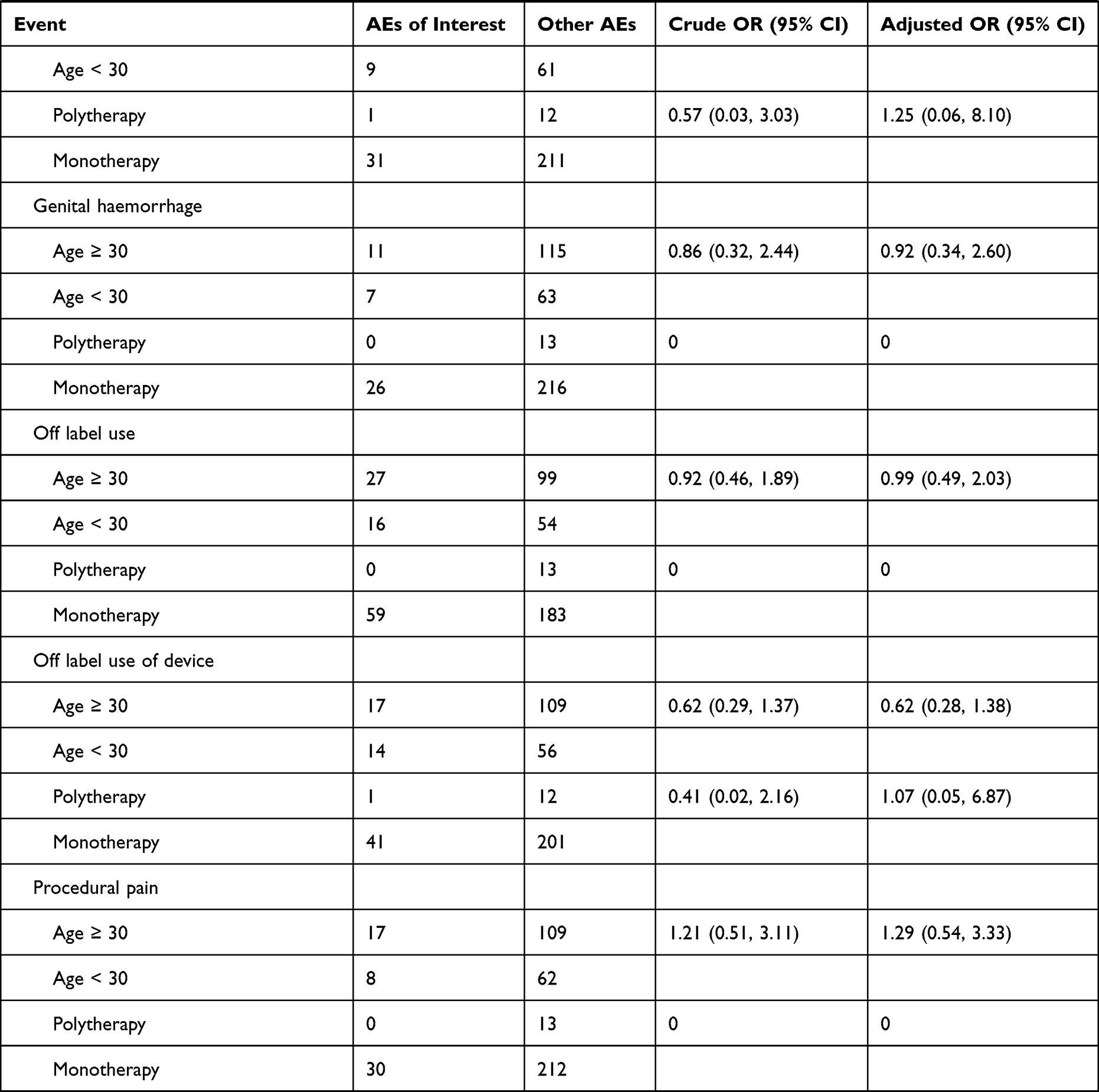 |
Table 4 Logistic Analysis of Patients with Common Adverse Events and Medical Errors |
Discussion
By reviewing FAERS data, this study comprehensively described reports of endometriosis patients treated with COCs and progestin on adverse event signals overall and in different dosage form subgroups. We also explored the possible effects of age and polytherapy on frequently reported adverse events.
During hormone treatment for endometriosis, change in hormone levels can lead to hormone-related adverse events. Besides, lifestyle and diet may affect symptoms, too.25 The broad spectrum of PTs detected in this study may result from individual variation in ER-alpha and PR distributions.26 It is reported that for patients with endometriosis who are intolerant of COC or norethisterone acetate’s side effects, shifting one to the other could improve their satisfaction.27 Since patients suffering from adverse effects of one drug may benefit from another, the regimen they receive should be adjusted in time once intolerable.
Common side effects of COC and progestins include bleeding, mastodynia, psychological disorders, weight gain, constipation, emotional fluctuation, galactorrhoea, thrombosis, decreased bone mineral density, libido changes, meningioma, hepatocellular adenoma, and some androgenic symptoms.28–37 In this study, signals of similar PTs as well as their secondary outcomes: genital haemorrhage, mental disability, abnormal weight gain, constipation, pulmonary embolism, deep vein thrombosis, hemiplegia, bone disorder, osteopenia, loss of libido, libido increased, anhedonia, meningioma, and hepatic adenoma were detected by proportional analysis. Since there was no true control in our study, some minor discrepancies lied between this pharmacovigilance research and previous clinical trials.
Some medical therapies for endometriosis aim to create a hypoestrogenic environment to delay disease progression,26 leading to menopause-like side effects. While GnRH-analogues and aromatase inhibitors are well known for their hypoestrogenic effects,38,39 the effects of COC and progestins vary in different age groups and dosages.40,41 Several studies indicated that oral progestin and progestin-eluting IUDs had an unapparent hypoestrogenic effect,42 except that DMPA users may encounter more menopausal symptoms.40,43,44 In this study, we detected signals of heart rate irregular, bone disorder, osteopenia, and autonomic nervous system imbalance in depot progestin users. Signals of feeling hot, abnormal weight gain, and loss of libido were detected in progestin-eluting IUD users as well. To determine the effect of different dosage forms of progestin on estrogen level, further researches with larger sample size need to be conducted. Besides, the signal of decreased appetite was detected in depot progestin users in this study. Since progestin metabolites have been reported to modulate GABA-A receptors directly rather than lowering estrogen levels to regulate appetite and mood,45 exact mechanisms behind the effect of progestins remain to be further investigated.
We detected plenty of signals about procedural complications, product issues, and administration site conditions as well as their potentially secondary PT: abdominal pain lower. But no signal of more serious PTs such as uterine perforation or fat necrosis was detected. Perforation rates of levonorgestrel-releasing intrauterine systems (LNG-IUS) and copper IUDs in the literature were both approximately 1/1000,46 which is relatively low. And relevant fat necrosis was only reported in a case report.47 Lactation, atrophic uterus due to long-term administration of depot injectables, and mismatch between uterine cavity size and the size of the IUD could be risk factors for IUD dislocation.48 As infection remains a considerable cause of withdrawal from IUD use,49,50 and the reasons for these events are clear, they may be avoided by comprehensively assessing the patient’s condition, standardizing procedures, and improving perioperative care.
In this study, we found that the PT spectrum varied in different dosage forms of progestin. Therefore, patients’ tolerance should be considered before regimen recommendation. When choosing among these long-term hormone treatments with contraceptive effects, patients’ fertility desires should be taken into account, too. The techniques of ovarian stimulation and egg freezing have been quite advanced51,52 and have been applied in the early stage of malignancy.53–55 Especially in cases of ovarian endometrioma that requires surgical intervention, fertility-sparing procedures and fertility preservation should be included in the therapy plan.
There were signals of some uncommon adverse effects, too. This study identified increased risk of meningioma with oral progestin treatment. Estrogen receptors (ER) and progesterone receptors (PR) are both expressed in meningioma tissue,56,57 the association between progestin and meningioma remains to be explored in large-sample clinical trials.
We found that atopic keratoconjunctivitis (AKC) and ocular discomfort cases were elevated in COC users (EB05 = 2.5). As an allergic conjunctival disease, inflammatory cells play an important role in the pathophysiology of AKC.58 Estrogen and progesterone receptors have been found positive in conjunctival biopsies from vernal keratoconjunctivitis (VKC), which is another subtype of the allergic conjunctival disease, and the majority of positive cells were eosinophils.59 Therefore, it is possible that the altered sex hormone level of COC users is related to AKC, which should raise concerns in future clinical practice and research.
Other nonspecific PTs, such as Uhthoff’s phenomenon, ulnar tunnel syndrome, mitral valve prolapse, chromatopsia, throat tightness, and mental disability were also detected in this study. None of them has reported relationship with sex hormones. A study which included more than 4000 patients with surgically diagnosed endometriosis reported no higher mitral valve prolapse prevalence in endometriosis patients than in general population.60 These nonspecific signals were detected possibly because of some underlying pathophysiological mechanisms or even entry errors. Though some of them may have already existed before drug administration, they still require proper treatment.
Product use issue in COC users was associated negatively with user’s age older than 30, which was observed on similar PTs of off label use and product use issue in unapproved indication. It is estimated that pregnancies caused by incorrect use of contraceptives are 9 times the rate of pregnancies with perfect use of contraceptives.61,62 There are over 1 million unintended pregnancies associated with the use, misuse, or discontinuation of oral contraceptives each year in the United States.63 In a national survey involving almost 2000 women in 2004,61 almost all oral contraceptive users set a daily reminder about taking the pill, but 38% had missed at least one pill within 3 months before the survey. In different age subgroups, users younger than 24 years old had a higher inconsistent use rate than older participants, too.61 Another study focusing on college and graduate students demonstrated that stress, long hours of paid employment, and living with a sex partner were associated positively with missed doses.64 As our study also revealed age-related differences in drug adherence, possible hidden factors behind the age, such as understanding of contraception, work/study pressure, medical insurance status, should be considered in future research.
We also found that age greater or equal to 30 was associated positively with pulmonary embolism in COC users. Age as a risk factor for thrombosis in COC users has been the consensus of medical professionals.32,33,65 Unfortunately, our regression analysis failed to demonstrate more associations between drug users’ characteristics and adverse events. Much of the age information of cases in our study was missing, resulting in a very limited number of valid data for regression analysis. The numbers of some drug-event pairs were inadequate for regression analysis, too. Due to these sampling errors, the results of regression analysis may not reflect the true situation of all patients with endometriosis in FAERS.
The FAERS provides sufficient reports from multiple countries for pharmacovigilance research. Not only manufacturers but also healthcare practitioners and users can report adverse events and medical errors to the FAERS. The MedDRA terminology helps to standardize the description of adverse events and diagnoses, making it easier for researchers to process and summarize these real-world data in batches. Meanwhile, this FAERS-based pharmacovigilance study has some drawbacks, too. Firstly, some identical events might be reported as similar but different PTs such as off label use and off label use of device according to the reporter’s understanding of the MedDRA terminology. Some other events which were different might be coded as the same general PT. For example, “libido decreased” and libido increased could both be coded as libido disorder. These coding inaccuracies could lead to imprecise results of statistical analysis. Secondly, one PT may have multiple different SOCs. MedDRA terminology has assigned a primary SOC for each PT.66 In this study, we grouped PTs by their primary SOCs. However, primary SOC may only indicate manifestation site rather than aetiology of the PT in some circumstances, which may mislead pathophysiological investigations. For example, the primary SOC of throat tightness is respiratory, thoracic and mediastinal disorders, while its secondary SOC is psychiatric disorders. These two SOCs are quite different. Thirdly, demographic information and detailed clinical records of these reports were limited for regression analysis, and existing variables including age had lots of missing values. Therefore, the regression analysis in our research could only yield preliminary results. Fourthly, information about drug or medical device users who never encounter any adverse event or medical error cannot be accessed from the FAERS, leaving it impossible to calculate the rates of the events. What is more, submitting reports by consumers, patients and health professionals are not mandatory, leaving some events missed by the FAERS. Reporting awareness of consumers, patients and healthcare professionals should be encouraged so that more comprehensive information can be collected.
Conclusion
Both COCs and progestin products are relatively safe for patients with endometriosis. Polytherapy was negatively associated with some medical errors for COC users, while patients older than or equal to 30 had more pulmonary embolisms, but fewer product use issues were reported. Newly detected signals in this pharmacovigilance study should be monitored in clinical practice and need to be validated in future research. When choosing hormone treatment regimens, gynaecologists should consider the patient’s satisfaction and fertility desire, and assess efficacy, costs, and side effects comprehensively.
Abbreviations
COC, combined oral contraceptive; GnRH, gonadotropin-releasing hormone; FDA, US Food and Drug Administration; FAERS, the FDA Adverse Event Reporting System; PT, preferred term; MedDRA, Medical Dictionary for Regulatory Activities; IUD, intrauterine device; GPS, Gamma-Poisson Shrinker; EBGM, Empirical Bayes Geometric Mean; CI, confidence interval; SOC, System Organ Class; DMPA, depot medroxyprogesterone acetate; LNG-IUS, levonorgestrel-releasing intrauterine system; PRL, prolactin; ER, estrogen receptor; PR, progesterone receptor; AKC, atopic keratoconjunctivitis; VKC, vernal keratoconjunctivitis.
Data Sharing Statement
All raw data used in this study have been released on FAERS website (https://www.fda.gov/drugs/questions-and-answers-fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-latest-quarterly-data-files) and are available to the public.
Ethics Approval and Informed Consent
Exemption from the ethical review has been granted by the Ethics Committee of Shanghai First Maternity and Infant Hospital since the FAERS is an anonymized publicly available database.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Commission of Shanghai Municipality (grant number 19411960300), the Shanghai Municipal Health Commission (grant number 2019SY002), the Shanghai Hospital Development Center (grant number SHDC12019113), and the Shanghai Municipality: Shanghai Outstanding Academic Leaders Plan (Year 2019).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shafrir AL, Farland LV, Shah DK, et al. Risk for and consequences of endometriosis: a critical epidemiologic review. Best Pract Res Clin Obstet Gynaecol. 2018;51:1–15. doi:10.1016/j.bpobgyn.2018.06.001
2. Mechsner S. Endometriosis, an ongoing pain-step-by-step treatment. J Clin Med. 2022;11(2):467. doi:10.3390/jcm11020467
3. Casper RF. Progestin-only pills may be a better first-line treatment for endometriosis than combined estrogen-progestin contraceptive pills. Fertil Steril. 2017;107(3):533–536. doi:10.1016/j.fertnstert.2017.01.003
4. Mehdizadeh Kashi A, Niakan G, Ebrahimpour M, et al. A randomized, double-blind, placebo-controlled pilot study of the comparative effects of dienogest and the combined oral contraceptive pill in women with endometriosis. Int J Gynaecol Obstet. 2022;156(1):124–132. doi:10.1002/ijgo.13677
5. Bedaiwy MA, Allaire C, Alfaraj S. Long-term medical management of endometriosis with dienogest and with a gonadotropin-releasing hormone agonist and add-back hormone therapy. Fertil Steril. 2017;107(3):537–548. doi:10.1016/j.fertnstert.2016.12.024
6. Vercellini P, Crosignani P, Somigliana E, Viganò P, Frattaruolo MP, Fedele L. ‘Waiting for Godot’: a commonsense approach to the medical treatment of endometriosis. Hum Reprod. 2011;26(1):3–13. doi:10.1093/humrep/deq302
7. Armstrong C. ACOG Practice Bulletin No. 110: noncontraceptive uses of hormonal contraceptives. Obstet Gynecol. 2010;115(1):206–218. doi:10.1097/AOG.0b013e3181cb50b5
8. Cibula D, Gompel A, Mueck AO, et al. Hormonal contraception and risk of cancer. Hum Reprod Update. 2010;16(6):631–650. doi:10.1093/humupd/dmq022
9. Hannaford PC, Iversen L, Macfarlane TV, Elliott AM, Angus V, Lee AJ. Mortality among contraceptive pill users: cohort evidence from Royal college of general practitioners’ oral contraception study. BMJ. 2010;340:c927. doi:10.1136/bmj.c927
10. Bedaiwy MA, Alfaraj S, Yong P, Casper R. New developments in the medical treatment of endometriosis. Fertil Steril. 2017;107(3):555–565. doi:10.1016/j.fertnstert.2016.12.025
11. TmotEGC G, Becker CM, Bokor A, et al. ESHRE guideline: endometriosis. Human Reproduction Open. 2022. doi:10.1093/hropen/hoac009
12. Matalliotakis I, Cakmak H, Matalliotakis M, Kappou D, Arici A. High rate of allergies among women with endometriosis. J Obstet Gynaecol. 2012;32(3):291–293. doi:10.3109/01443615.2011.644358
13. Vercellini P, Somigliana E, Vigano P, Abbiati A, Barbara G, Crosignani PG. Endometriosis: current therapies and new pharmacological developments. Drugs. 2009;69(6):649–675. doi:10.2165/00003495-200969060-00002
14. Vercellini P, Somigliana E, Vigano P, Abbiati A, Daguati R, Crosignani PG. Endometriosis: current and future medical therapies. Best Pract Res Clin Obstet Gynaecol. 2008;22(2):275–306. doi:10.1016/j.bpobgyn.2007.10.001
15. Moehner S, Becker K, Lange JA, von Stockum S, Heinemann K. Risk of depression and anemia in users of hormonal endometriosis treatments: results from the VIPOS study. Eur J Obstet Gynecol Reprod Biol. 2020;251:212–217. doi:10.1016/j.ejogrb.2020.05.049
16. Techatraisak K, Hestiantoro A, Soon R, et al. Impact of long-term dienogest therapy on quality of life in Asian women with endometriosis: the prospective non-interventional study ENVISIOeN. Reprod Sci. 2022;29(4):1157–1169. doi:10.1007/s43032-021-00787-w
17. Kitawaki J, Koga K, Kanzo T, Momoeda M. An assessment of the efficacy and safety of dydrogesterone in women with ovarian endometrioma: an open-label multicenter clinical study. Reprod Med Biol. 2021;20(3):345–351. doi:10.1002/rmb2.12391
18. MedDRA; [Updated May 2, 2022]. Available from: https://www.meddra.org/.
19. Questions and answers on FDA’s Adverse Event Reporting System (FAERS). U.S. Food and Drug Administration; [Updated April 6, 2018]. Available from: https://www.fda.gov/drugs/surveillance/questions-and-answers-fdas-adverse-event-reporting-system-faers. Accessed May 2, 2022.
20. Dumouchel W. Bayesian data mining in large frequency tables, with an application to the FDA spontaneous reporting system. Am Stat. 1999;53(3):177–190. doi:10.1080/00031305.1999.10474456
21. DuMouchel W, Pregibon D. Empirical Bayes screening for multi-item associations.
22. Szarfman A, Machado SG, O’Neill RT. Use of screening algorithms and computer systems to efficiently signal higher-than-expected combinations of drugs and events in the US FDA’s spontaneous reports database. Drug Saf. 2002;25(6):381–392. doi:10.2165/00002018-200225060-00001
23. MedDRA Hierarchy. The International council for harmonisation of technical requirements. Available from: https://www.meddra.org/how-to-use/basics/hierarchy. Accessed May 2, 2022.
24. Riley RD, Ensor J, Snell KIE, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. 2020;368:m441. doi:10.1136/bmj.m441
25. Habib N, Buzzaccarini G, Centini G, et al. Impact of lifestyle and diet on endometriosis: a fresh look to a busy corner. Prz Menopauzalny. 2022;21(1):124–132.
26. Brichant G, Laraki I, Henry L, Munaut C, Nisolle M. New therapeutics in endometriosis: a review of hormonal, non-hormonal, and non-coding RNA treatments. Int J Mol Sci. 2021;22(19):10498. doi:10.3390/ijms221910498
27. Vercellini P, Ottolini F, Frattaruolo MP, Buggio L, Roberto A, Somigliana E. Shifting from oral contraceptives to norethisterone acetate, or vice versa, because of drug intolerance: does the change Benefit women with endometriosis? Gynecol Obstet Invest. 2018;83(3):275–284. doi:10.1159/000486335
28. Sharma SC, Basu NN. Galactorrhea/Galactocele after breast augmentation: a systematic review. Ann Plast Surg. 2021;86(1):115–120. doi:10.1097/SAP.0000000000002290
29. Mishell DR
30. Momoeda M, Harada T, Terakawa N, et al. Long-term use of dienogest for the treatment of endometriosis. J Obstet Gynaecol Res. 2009;35(6):1069–1076. doi:10.1111/j.1447-0756.2009.01076.x
31. Dragoman MV, Gaffield ME. The safety of subcutaneously administered depot medroxyprogesterone acetate (104mg/0.65mL): a systematic review. Contraception. 2016;94(3):202–215. doi:10.1016/j.contraception.2016.02.003
32. Sitruk-Ware R. Hormonal contraception and thrombosis. Fertil Steril. 2016;106(6):1289–1294. doi:10.1016/j.fertnstert.2016.08.039
33. Pfeifer S, Butts S, Dumesic D, Practice Committee of the American Society for Reproductive Medicine. Electronic address Aao, Practice Committee of the American Society for Reproductive M. Combined hormonal contraception and the risk of venous thromboembolism: a guideline. Fertil Steril. 2017;107(1):43–51. doi:10.1016/j.fertnstert.2016.09.027
34. Welling LL. Psychobehavioral effects of hormonal contraceptive use. Evol Psychol. 2013;11(3):718–742. doi:10.1177/147470491301100315
35. Bachrach LK. Hormonal contraception and bone health in adolescents. Front Endocrinol (Lausanne). 2020;11:603. doi:10.3389/fendo.2020.00603
36. Hage M, Plesa O, Lemaire I, Raffin Sanson ML. Estrogen and progesterone therapy and meningiomas. Endocrinology. 2022;163(2). doi:10.1210/endocr/bqab259
37. Edmondson HA, Henderson B, Benton B. Liver-cell adenomas associated with use of oral contraceptives. N Engl J Med. 1976;294(9):470–472. doi:10.1056/NEJM197602262940904
38. Smitz J, Ron-El R, Tarlatzis BC. The use of gonadotrophin releasing hormone agonists for in vitro fertilization and other assisted procreation techniques: experience from three centres. Hum Reprod. 1992;7(Suppl 1):49–66. doi:10.1093/humrep/7.suppl_1.49
39. Della Corte L, Barra F, Mercorio A, et al. Tolerability considerations for gonadotropin-releasing hormone analogues for endometriosis. Expert Opin Drug Metab Toxicol. 2020;16(9):759–768. doi:10.1080/17425255.2020.1789591
40. Rocca ML, Palumbo AR, Bitonti G, Brisinda C, C DIC. Bone health and hormonal contraception. Minerva Obstet Gynecol. 2021;73(6):678–696. doi:10.23736/S2724-606X.20.04688-2
41. Duijkers IJM, Klipping C, Rautenberg T, et al. Effect on ovarian activity and ovulation inhibition of different oral dosages of levonorgestrel. Contraception. 2022;110:6–15. doi:10.1016/j.contraception.2022.01.018
42. Kyvernitakis I, Kostev K, Thomasius F, Stumpf U, Hadji P. Effect of progestogen-only contraception on premenopausal fracture risk: a case-control study. Osteoporos Int. 2020;31(9):1801–1806. doi:10.1007/s00198-020-05437-6
43. Lopez LM, Chen M, Mullins Long S, Curtis KM, Helmerhorst FM. Steroidal contraceptives and bone fractures in women: evidence from observational studies. Cochrane Database Syst Rev. 2015;7:CD009849. doi:10.1002/14651858.CD009849.pub3
44. Raine-Bennett T, Chandra M, Armstrong MA, Alexeeff S, Lo JC. Depot medroxyprogesterone acetate, oral contraceptive, intrauterine device use, and fracture risk. Obstet Gynecol. 2019;134(3):581–589. doi:10.1097/AOG.0000000000003414
45. Das R, Ragagnin G, Sjostedt J, et al. Medroxyprogesterone acetate positively modulates specific GABAA-receptor subtypes - affecting memory and cognition. Psychoneuroendocrinology. 2022;141:105754. doi:10.1016/j.psyneuen.2022.105754
46. Heinemann K, Reed S, Moehner S, Minh TD. Risk of uterine perforation with levonorgestrel-releasing and copper intrauterine devices in the European active surveillance study on intrauterine devices. Contraception. 2015;91(4):274–279. doi:10.1016/j.contraception.2015.01.007
47. Kataoka Y, Wada M, Bito M, Asai J, Katoh N. Subcutaneous nodules at progesterone injection sites after fertility treatment. Australas J Dermatol. 2019;60(2):143–144. doi:10.1111/ajd.12929
48. Wildemeersch D, Hasskamp T, Goldstuck N. Intrauterine devices that do not fit well cause side effects, become embedded, or are expelled and can even perforate the uterine wall. J Minim Invasive Gynecol. 2015;22(2):309–310. doi:10.1016/j.jmig.2014.09.010
49. Aoun J, Dines VA, Stovall DW, Mete M, Nelson CB, Gomez-Lobo V. Effects of age, parity, and device type on complications and discontinuation of intrauterine devices. Obstet Gynecol. 2014;123(3):585–592. doi:10.1097/AOG.0000000000000144
50. Bayer LL, Jensen JT, Li H, Nichols MD, Bednarek PH. Adolescent experience with intrauterine device insertion and use: a retrospective cohort study. Contraception. 2012;86(5):443–451. doi:10.1016/j.contraception.2012.03.014
51. Gullo G, Petousis S, Papatheodorou A, et al. Closed vs. open oocyte vitrification methods are equally effective for blastocyst embryo transfers: prospective study from a sibling oocyte donation program. Gynecol Obstet Invest. 2020;85(2):206–212. doi:10.1159/000506803
52. Prapas Y, Ravanos K, Petousis S, et al. GnRH antagonist administered twice the day before hCG trigger combined with a step-down protocol may prevent OHSS in IVF/ICSI antagonist cycles at risk for OHSS without affecting the reproductive outcomes: a prospective randomized control trial. J Assist Reprod Genet. 2017;34(11):1537–1545. doi:10.1007/s10815-017-1010-7
53. Tanos P, Dimitriou S, Gullo G, Tanos V. Biomolecular and Genetic prognostic factors that can facilitate Fertility-Sparing Treatment (FST) decision making in Early Stage Endometrial Cancer (ES-EC): a systematic review. Int J Mol Sci. 2022;23(5):2653.
54. Cavaliere AF, Perelli F, Zaami S, et al. Fertility sparing treatments in endometrial cancer patients: the potential role of the new molecular classification. Int J Mol Sci. 2021;22(22):12248. doi:10.3390/ijms222212248
55. Gullo G, Etrusco A, Cucinella G, et al. Fertility-sparing approach in women affected by stage I and low-grade endometrial carcinoma: an updated overview. Int J Mol Sci. 2021;22(21):11825. doi:10.3390/ijms222111825
56. Poisson M, Magdelenat H, Foncin JF, et al. [Estrogen and progestin receptors in meningiomas: a study in 22 cases]. Recepteurs d’oestrogenes et de progesterone dans les meningiomes. Etude de 22 cas. Rev Neurol (Paris). 1980;136(3):193–203.
57. Donnell MS, Meyer GA, Donegan WL. Estrogen-receptor protein in intracranial meningiomas. J Neurosurg. 1979;50(4):499–502. doi:10.3171/jns.1979.50.4.0499
58. Chen JJ, Applebaum DS, Sun GS, Pflugfelder SC. Atopic keratoconjunctivitis: a review. J Am Acad Dermatol. 2014;70(3):569–575. doi:10.1016/j.jaad.2013.10.036
59. Bonini S, Lambiase A, Schiavone M, Centofanti M, Palma LA, Bonini S. Estrogen and progesterone receptors in vernal keratoconjunctivitis. Ophthalmology. 1995;102(9):1374–1379. doi:10.1016/s0161-6420(95)30861-5
60. Gemmill JA, Stratton P, Cleary SD, Ballweg ML, Sinaii N. Cancers, infections, and endocrine diseases in women with endometriosis. Fertil Steril. 2010;94(5):1627–1631. doi:10.1016/j.fertnstert.2009.07.1698
61. Frost JJ, Darroch JE. Factors associated with contraceptive choice and inconsistent method use, United States, 2004. Perspect Sex Reprod Health. 2008;40(2):94–104. doi:10.1363/4009408
62. Kost K, Singh S, Vaughan B, Trussell J, Bankole A. Estimates of contraceptive failure from the 2002 National Survey of Family Growth. Contraception. 2008;77(1):10–21. doi:10.1016/j.contraception.2007.09.013
63. Rosenberg MJ, Waugh MS, Long S. Unintended pregnancies and use, misuse and discontinuation of oral contraceptives. J Reprod Med. 1995;40(5):355–360.
64. Hughey AB, Neustadt AB, Mistretta SQ, Tilmon SJ, Gilliam ML. Daily context matters: predictors of missed oral contraceptive pills among college and graduate students. Am J Obstet Gynecol. 2010;203(4):323 e1–7. doi:10.1016/j.ajog.2010.05.039
65. Teal S, Edelman A. Contraception selection, effectiveness, and adverse effects: a review. JAMA. 2021;326(24):2507–2518. doi:10.1001/jama.2021.21392
66. Multiaxiality. Medical dictionary for regulatory activities. Available from: https://www.meddra.org/multiaxiality. Accessed May 2, 2022.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.