Back to Journals » International Journal of Women's Health » Volume 17
Analysis and Prediction Study on the Disease Burden of Inflammatory Bowel Disease Among Chinese Women of the Reproductive Age
Authors Xie C, Shi S, Li X, Guo S ![]() , Xiao J
, Xiao J ![]() , Xie H
, Xie H ![]() , Cai S
, Cai S
Received 3 July 2025
Accepted for publication 30 September 2025
Published 11 October 2025 Volume 2025:17 Pages 3655—3666
DOI https://doi.org/10.2147/IJWH.S551379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Chunying Xie,1 Siqi Shi,1 Xiaoyun Li,1 Shimin Guo,1 Jingjing Xiao,2 Huihui Xie,3 Shu Cai1
1School of Nursing, Guangdong Pharmaceutical University, Guangzhou, Guangdong Province, 510310, People’s Republic of China; 2Guangdong Women and Children Hospital, Guangzhou, Guangdong Province, 511442, People’s Republic of China; 3Shenzhen Luohu Maternal and Child Health Hospital, Shenzhen, Guangdong Province, 518000, People’s Republic of China
Correspondence: Shu Cai, School of Nursing, Guangdong Pharmaceutical University, Guangzhou, Guangdong Province, 510310, People’s Republic of China, Email [email protected]
Purpose: To analyze the disease burden of inflammatory bowel disease (IBD) among Chinese women of reproductive age (WRA) from 1990 to 2021, as well as the projected trends through 2035.
Patients and Methods: A segmented regression analysis was carried out to assess the temporal trend of the disease burden. Additionally, the age period cohort (APC) model was applied to explore the impact of each factor on IBD. Based on the APC model, a Bayesian approach was used to predict the disease burden during the period from 2022 to 2035.
Results: In 2021, the number of Chinese WRA with IBD was approximately 38,701, with a standardized prevalence rate of 9.47 per 100,000, both of which were lower than the global averages. From 1990 to 2021, the standardized prevalence rate of IBD among Chinese WRA showed an upward trend with an average annual percentage change (AAPC) of 1.53%, while the standardized DALY rate of IBD showed a downward trend with an AAPC of − 3.36%. The APC model showed that the longitudinal age curves of IBD prevalence and DALY rate increased with age. Over time, the risk of IBD among Chinese WRA showed a trend of first increasing and then decreasing, while the risk of DALY showed an overall downward trend with the passage of time. Results regarding birth cohorts indicated that the risk of IBD among Chinese WRA gradually increased with the advancement in birth cohorts, whereas the risk of DALY gradually decreased.
Conclusion: Age, period, and birth cohort have significant impacts on the disease burden of IBD among WRA. Going forward, it remains necessary to strengthen attention to the population of WRA with IBD and formulate appropriate health measures and strategies to prevent and manage the prevalence of IBD among WRA.
Keywords: women of reproductive age, inflammatory bowel disease, burden of disease, segmented regression model, age-period-cohort model
Introduction
Inflammatory bowel disease (IBD) is a chronic, recurrent autoimmune disease of the bowel of unknown etiology, including ulcerative colitis (UC) and Crohn’s disease (CD).1 It is mainly manifested as abdominal pain, diarrhea, mucus, pus, and blood in stool, etc., with the characteristics of repeated attacks.2 Not only does this disease severely impact patients’ quality of life and augment the family’s burden, but it also has an effect on the physical and mental well-being of patients.3–5 Over the recent years, the incidence of IBD across the world keeps increasing, and obvious differences exist among different regions; high incidence in Europe and North America, and relatively low in Asia.6 In the European and American continents, North America and Northern Europe are areas where the incidence rate is high.7 Among Asian countries, China has the highest prevalence of IBD.8 From the age distribution point of view, IBD prevalence presents bimodal characteristics, with the first peak occurring at the age of 15–25 years old and the second peak at the age of 50–80 years old, the data show that about 50% of the IBD patients were diagnosed at the age of 35 years old, and 25% of the patients face the problem of the first birth immediately after the diagnosis of IBD.9 In addition, according to the 2019 Global Burden of Disease (GBD) data, most female IBD patients in China develop the disease during young and middle age, with a prevalence rate of 44.28 per 100,000, which is increasing year by year, and fertility has become one of their major concerns.10 It is evident that the first peak of prevalence is directly associated with the reproductive age group, and early-onset disease may have profound impacts on their fertility and long-term health; meanwhile, the existence of the second peak further underscores the importance of early prevention and control during the reproductive years. Therefore, it is crucial to pay attention to the prevalence of IBD among women of reproductive age.
Given China’s large population base, the number of IBD patients is likely to increase over time, potentially imposing a substantial burden on the economy and healthcare system. However, studies investigating long-term trends in IBD among Chinese women of reproductive age (WRA), particularly concerning the influences of age, period, and birth cohort on disease burden, remain limited. Thus, in this research, we analyzed data from GBD 2021 database. By employing a segmented regression model, we analyzed the prevalence of IBD among Chinese WRA from 1990 to 2021, trends of DALYs, and the effects of age, time period, and cohort. Furthermore, we predicted the disease burden of IBD in this population from 2022 to 2035, to provide a theoretical reference for the subsequent formulation of IBD prevention and control policies targeting Chinese WRA.
Materials and Methods
Data Sources
The data used in this research were obtained from the 2021 Global Burden of Disease (GBD) database (https://vizhub.healthdata.org/gbd-results/). This database utilizes various health information indicators, such as disease statistics indicators and disease burden indicators, to assess the disease burden caused. This study utilized data for both China and the global aggregate from the GBD database spanning 1990 to 2021 to analyze the disease burden of IBD among Chinese WRA and predict future prevalence and DALY trends.
Parameters were configured within the free data download interface of GBD 2021 according to the study objectives as follows: Under “GBD Estimate”, “cause of death or injury” was selected. Under “Measure”, both “prevalence” and “DALYs” were selected. In the “Metric” column, both “number” and “rate” were selected. In the “Age” column, the following groups were selected: “15–19”, “20–24”, “25–29”, “30–34”, “35–39”, “40–44”, “45–49”, and “15–49”. In the “Sex” column, “Female” was selected. The retrieved data were saved in CSV format. For details on the GBD data extraction and analytical methods, please refer to references.11–13
Case Definition
The diagnosis of IBD is determined according to the International Classification of Diseases, 10th edition (ICD–10 codes: K50–K52, K52.8–K52.9; ICD–9 codes: 555–556.9, 558–558.9, 569.5).14 Prevalence refers to the proportion of a population with a specific disease at a given time, typically expressed as a rate per 1,000 or 100,000 individuals. DALY measures the number of healthy life years lost due to disease or disability, serving as a metric to evaluate the overall burden of diseases or injuries and reflect the extent of health impairment. In this study, prevalence and DALY data were downloaded from the GBD database and presented with uncertainty intervals (UI), while metrics such as net drift, derived from APC model calculations, were reported with confidence intervals (CI). This was done to convey the uncertainty and precision associated with these estimations, thereby enabling a more thorough comprehension of the related research outcomes.
Segmented Regression Model
The method developed by the National Cancer Institute and based on R was employed to analyze the temporal trends of various disease burden indicators for IBD among Chinese WRA from 1990 to 2021. The average annual percentage change (AAPC), annual percentage change (APC), and 95% confidence interval (CI) were computed respectively. If both the estimated value of AAPC/APC and the lower limit of its 95% CI were positive, it indicated an upward trend over a certain period; conversely, it indicated a downward trend. Additionally, if the 95% CI did not include 0, the trend of change was statistically significant (p < 0.05); otherwise, it was not statistically significant.15
Age-Period-Cohort (APC) Model
This model operates on the basis of the Poisson distribution. It treats different ages, periods, and birth cohorts as independent variables and analyzes their respective impacts on the disease.16 The model segments age, period and cohort in 5-year intervals, stratifies age into seven groups (ages 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49), divides the 30-year period from 1992 to 2021 into six periods,and calculates the birth cohort through the existence of a deterministic algebraic relationship between the three: birth cohort = period-age. The birth cohort was divided into a total of twelve groups. Using this modelling tool, the prevalence of IBD and DALYs in Chinese WRA was investigated in three dimensions: age, period, and birth cohort, respectively.
Bayesian Age-Period-Cohort (BAPC) Model
The BAPC model was employed to forecast the prevalence of IBD and DALYs among WRA in China from 2022 to 2035. The BAPC model operates under the premise that the age, period, and cohort effects exhibit similarity over time. It utilizes an integrated nested Laplace approximation method to estimate the marginal posterior distributions. For its establishment, we utilized the BAPC and INLA packages in the R programming language.17
Statistical Analyses
The prevalence of IBD in the WRA and DALY data were processed using R4.4.2 software to describe the burden of disease of IBD in the WRA in China and globally. To ensure the comparability of statistical indicators, age-standardised rates (asrs) were used to reduce the effects of demographic changes and age distribution over time.18
Ethics Approval
According to Article 32, Item 1 and Item 2 of the “Ethical Review Measures for Life Sciences and Medical Research Involving Human Subjects” issued by China on February 18, 2023, the following situations can be exempted from additional ethical review: (1) Research conducted using legally obtained public data, or data obtained through observation without interfering with public behavior; (2) Research using anonymized information data. Since all the data used in this study are from the publicly available GBD 2021 database. This database contains fully de-identified data at the national level and does not contain any individual-level or personally identifiable information. Therefore, our research meets the conditions that do not require additional ethical approval.
Results
Disease Burden of IBD in the WRA in China and Globally in 2021
In 2021, the number of IBD cases and DALYs among Chinese WRA accounted for approximately 4.46% and 4.22% of the global total for WRA with IBD, respectively. The number of Chinese WRA with IBD was 38,701 (95% UI=30,920, 49,214), while the global figure stood at 866,997 (95% UI=704,036, 1,053,395). Both the standardized prevalence of IBD and DALY rate among Chinese WRA were lower than the global levels. The standardized prevalence of IBD among Chinese WRA was 9.47 per 100,000, which was lower than the global average of 45.90 per 100,000 (Table 1).
 |
Table 1 Burden of IBD in the WRA in 2021: China and Global Comparison |
IBD Burden Trends in Chinese WRA, 1990 to 2021
Between 1990 and 2021, the number of cases and prevalence of IBD among WRA showed an upward trend (Figure 1A and B), while the number of DALYs first increased and then decreased, with the DALY rate showing an overall downward trend (Figure 1C and D).
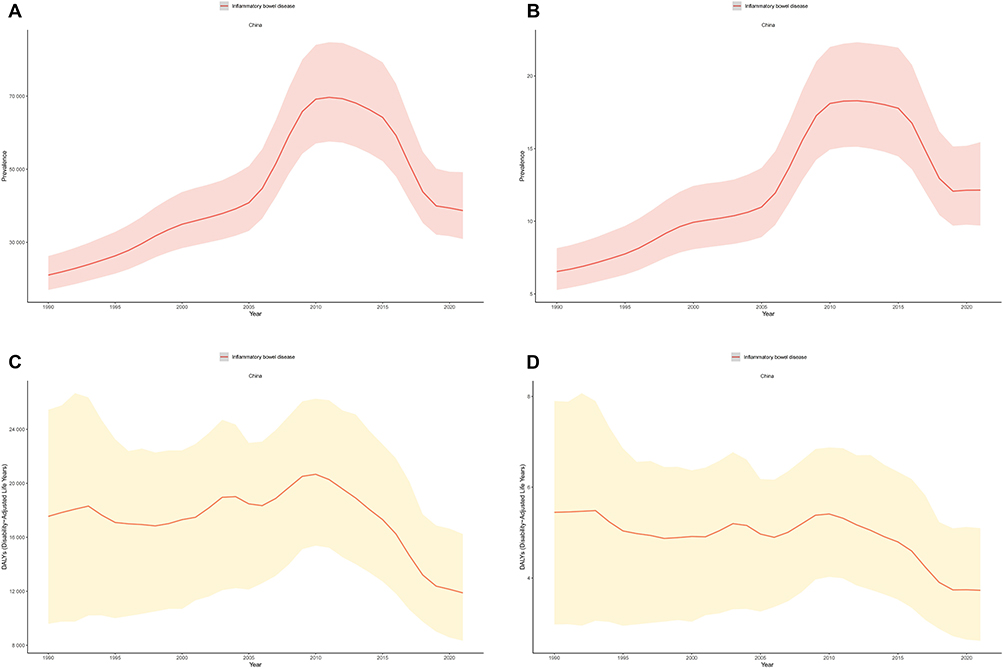 |
Figure 1 Trends of IBD burden among Chinese WRA, 1990–2021. (A) Number of prevalent cases. (B) Prevalence rate. (C) Number of DALYs. (D) DALY rate. In (A) and (C) the Y-axis represents absolute numbers; in (B) and (D) the Y-axis represents rates. Shaded areas indicate the upper and lower bounds of the 95% confidence interval. Abbreviations: WRA, Women of Reproductive Age; DALY, Disability-Adjusted Life Year. |
Specifically, comparing data from 1990 and 2021, the number of IBD cases among Chinese WRA increased from 21,058 to 38,701, representing an 83.78% increase. The standardized prevalence rate rose from 5.9 per 100,000 in 1990 to 9.47 per 100,000. In contrast, the total number of DALYs among Chinese WRA with IBD decreased from 17,553 to 11,887, a reduction of 32.28%, and the standardized DALY rate dropped from 19.18 per 100,000 in 1990 to 6.23 per 100,000 (Table 2).
 |
Table 2 Prevalence and DALY Burden of IBD in Chinese WRA |
The segmented regression model showed that from 1990 to 2021, the standardized prevalence rate of IBD among Chinese WRA exhibited a fluctuating upward trend, with an AAPC of 1.53% (95% CI=0.94, 2.11. p < 0.001), indicating a statistically significant difference. The increase was most rapid between 2005 and 2011, with an APC of 7.87% (95% CI=6.40, 9.36. p < 0.05), also showing a statistically significant difference. The standardized DALY rate for the total population showed a downward trend, with an AAPC of −3.64% (95% CI=−3.82, −3.46. p < 0.001), indicating a statistically significant difference (Table 3).
 |
Table 3 Disease Burden Trends of IBD in Chinese WRA, 1990 to 2021 |
Age-Specific Disease Burden Status of IBD Among WRA in China, 2021
In 2021, among Chinese WRA, the number of IBD cases, prevalence rate, DALYs, and DALY rate generally increased steadily with age (Figure 2A and B). Across all age groups, the 15–19-year age group had the lowest values for the number of cases, prevalence rate, DALYs, and DALY rate, whereas the 45–49-year age group had the highest. Notably, in the 30–44-year age group, the number of IBD cases remained relatively stable with no significant increasing trend (Figure 2A).
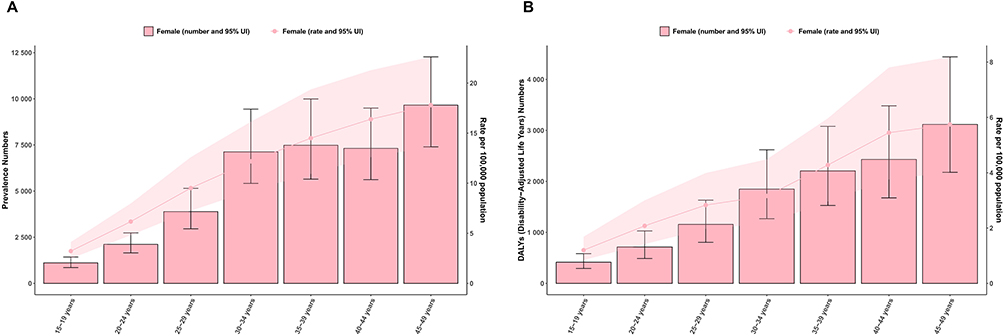 |
Figure 2 Age-stratified burden of IBD among Chinese women of reproductive age, 2021. (A) Age-related Trends of IBD Case Numbers and Prevalence in Chinese WRA, 2021. (B) Age-related Trends of IBD DALYs and DALY rate in Chinese WRA, 2021. Shaded areas indicate the upper and lower bounds of the 95% confidence interval. Abbreviations: WRA, Women of Reproductive Age; DALY, Disability-Adjusted Life Year. |
APC Modelling Analysis of IBD in Chinese WRA, 1990–2021
Given that traditional trend analysis struggles to simultaneously disentangle the independent contributions of age, period, and birth cohort to disease risk, this study employed the age-period-cohort (APC) model. It used net drift to measure overall annual changes and local drift to measure annual changes within each age group, thereby identifying, respectively, the inherent risk differences across age groups reflected by age effects, the external influences at specific time points embodied by period effects, and the differences in long-term exposure represented by birth cohort effects, so as to systematically clarify the epidemiological trends of IBD among Chinese WRA from 1990 to 2021.
Net and Localized Drift Results for IBD in Chinese WRA, 1990–2021
Net drift showed that from 1990 to 2021, the prevalence of IBD among Chinese WRA exhibited a significant upward trend, with a net drift value of 2.19 (95% CI=2.0, 2.38). Conversely, the DALY rate showed a significant downward trend, with a net drift value of −1.47 (95% CI=−1.72, −1.21).
Local drift showed that from 1990 to 2021, the IBD prevalence among Chinese WRA exhibited an upward trend across all age groups, with local drift values all > 0 (Figure 3A). In contrast, changes in the DALY rate within age groups showed a fluctuating trend of first increasing and then decreasing; yet, local drift values in all age groups were < 0 (Figure 4A), indicating that the DALY rate of IBD in all age groups of Chinese WRA still showed an overall downward trend.
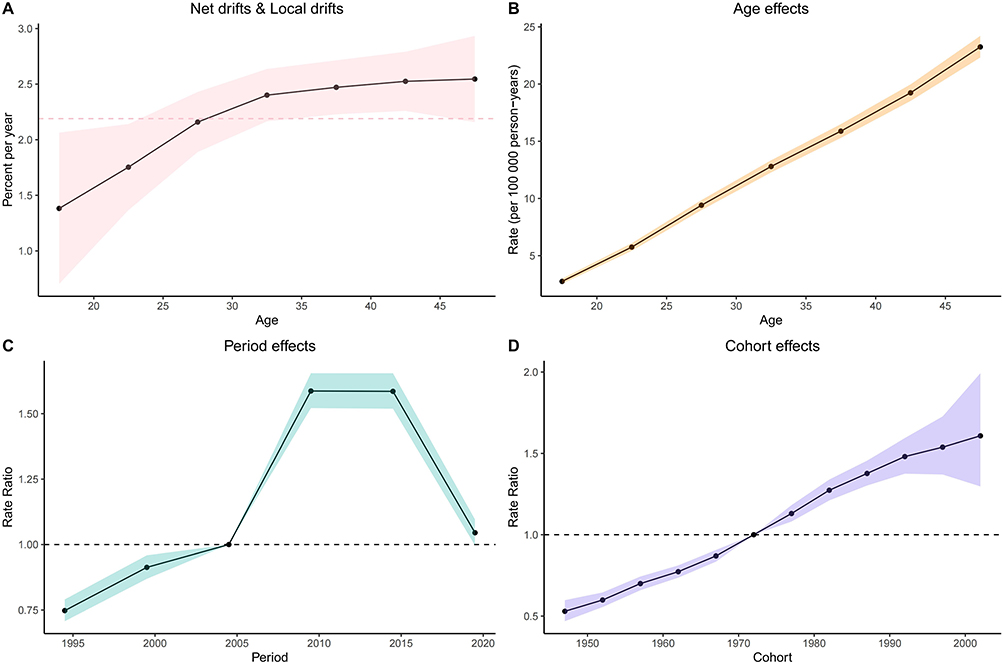 |
Figure 3 APC Model Analysis of IBD Prevalence in Chinese WRA,1990 to 2021. (A) Net drifts and local drifts. (B) Age effects. (C) Period effects. (D) Cohort effects. In (A) the dashed red line represents the overall annual percent change of 2.19% across all ages (Net Drift), and the black line represents the local annual percent change (Local Drift). In (C) and (D) the dashed line represents the reference line (RR=1). Shaded areas indicate the upper and lower bounds of the 95% confidence interval. Abbreviations: WRA, Women of Reproductive Age; DALY, Disability-Adjusted Life Year, APC, Annual Percentage Change. |
 |
Figure 4 APC Model Analysis of IBD DALY Rates in Chinese WRA, 1990–2021. (A) Net drifts and local drifts. (B) Age effects. (C) Period effects. (D) Cohort effects. In (A) the dashed red line represents the overall annual percent change of −1.47% across all ages (Net Drift), and the black line represents the local annual percent change (Local Drift). In (C) and (D) the dashed line represents the reference line (RR=1). Shaded areas indicate the upper and lower bounds of the 95% confidence interval. Abbreviations: WRA, Women of Reproductive Age; DALY, Disability-Adjusted Life Year; APC, Annual Percentage Change. |
Age Trends in the Prevalence of IBD and DALY Rate in Chinese WRA, 1990 to 2021
Age effect showed that both the prevalence of IBD and the DALY rate among Chinese WRA exhibited a gradual upward trend with increasing age. Specifically, the prevalence increased from 2.75 per 100,000 in the 15–19-year age group to 23.24 per 100,000 in the 45–49-year age group (Figure 3B). The DALY rate increased from 2.41 per 100,000 in the 15–19-year age group to 6.28 per 100,000 in the 45–49-year age group, suggesting that increasing age may be an important influencing factor for the prevalence and disease burden of IBD in WRA (Figure 4B).
Periodic Trends in the Prevalence of IBD and DALY Rate in Chinese WRA, 1990 to 2021
Period effect showed that the risk of IBD prevalence among Chinese WRA fluctuated with changing periods, presenting a “rise-first-then-fall” trend: With 2002–2006 as the reference period (RR=1.00), during 1992–1996, RR < 1, and the risk was the lowest (RR=0.75, 95% CI=0.71, 0.79), indicating a reduced relative risk. During 2007–2011 and 2012–2016, RR > 1, and the risk peaked (with an RR of 1.59 for both periods, 95% CI=1.52, 1.65). However, the risk decreased slightly in 2017–2021 (RR=1.05, 95% CI=1.00, 1.10) (Figure 3C), indicating an increased relative risk followed by a slight decrease.
Meanwhile, the risk of DALY rate showed an overall downward trend with changing periods: With 2002–2006 as the reference period (RR=1.00), the risk was highest in 1992–1996 (RR=1.06, 95% CI=0.99, 1.14) and dropped to the lowest in 2017–2021 (RR=0.66, 95% CI=0.61, 0.71) (Figure 4C).
Birth Cohort Trends in the Prevalence of IBD and DALY Rate in Chinese WRA, 1990 to 2021
Cohort effect showed that the risk of IBD prevalence among Chinese WRA showed a gradual upward trend with the progression of birth cohorts. Using the 1972–1976 birth cohort as the reference (RR=1.00), during 1947–1951, RR < 1, with the birth cohort having the lowest risk (RR=0.53, 95% CI=0.47, 0.59), indicating a reduced relative risk of IBD prevalence among Chinese WRA; while the 2002–2006 birth cohort had the highest risk (RR=1.61, 95% CI=1.30, 1.99) (Figure 3D), indicating an increased relative risk.
Meanwhile, the risk of DALY rate showed a gradual downward trend with the progression of birth cohorts. The 1947–1951 birth cohort had the highest risk (RR=1.55, 95% CI=1.36, 1.77), and the 2002–2006 birth cohort had the lowest risk (RR=0.58, 95% CI=0.43, 0.80) (Figure 4D).
Prediction of IBD Prevalence and DALY Rate in Chinese WRA, 2022 to 2035
Based on the above data analysis, the standardized prevalence of IBD among Chinese WRA is projected to show a slow upward trend between 2022 and 2035, slightly increasing from 10.87 per 100,000 in 2022 to 11.77 per 100,000 in 2035. However, the standardized DALY rate of IBD among Chinese WRA is expected to show a downward trend over the same period, decreasing from 3.28 per 100,000 in 2022 to 2.34 per 100,000 in 2035 (Figure 5A and B).
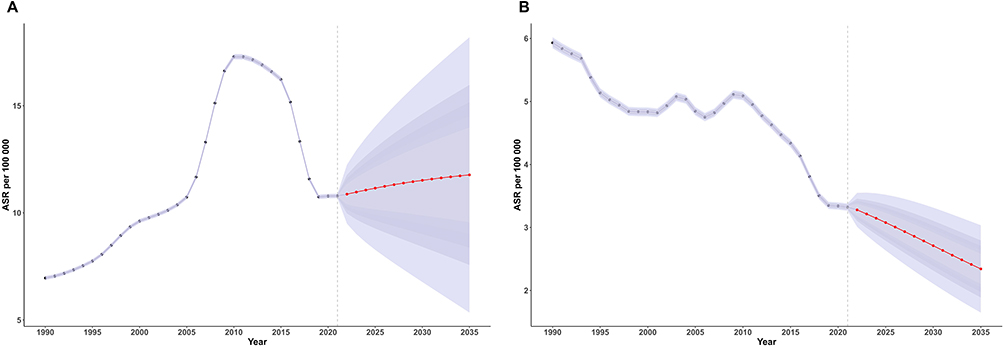 |
Figure 5 Prediction of standardized IBD Prevalence and DALY rate in Chinese WRA, 2022 to 2035. (A) Prediction of standardized IBD Prevalence. (B) Prediction of standardized IBD DALY rate. The red line represents the fitted projection, and the surrounding purple band represents the upper and lower bounds of the 95% confidence interval. Abbreviations: WRA, Women of Reproductive Age; DALY, Disability-Adjusted Life Year; ASR, Age Standardized Rate; BAPC, Bayesian Age-Period-Cohort. |
Discussion
The standardized prevalence of IBD among Chinese WRA in 2021 was 9.47 per 100,000, significantly lower than the global average of 44.49 per 100,000. This disparity may be attributed to the traditional Chinese dietary pattern (high-fibre, low-processed foods).19 Shin Y et al demonstrated that dietary fibre has anti-inflammatory and intestinal barrier-protecting effects by regulating intestinal flora and short-chain fatty acid production.20 In contrast, the high-fat diets prevalent in Western countries are associated with elevated IBD prevalence.21 This is because a high-fat diet disrupts the intestinal barrier, triggers inflammatory responses, breaks the balance between NK-T cells and Treg cells, and exacerbates symptoms.22 In addition, genetic factors may potentially influence differences in IBD risk. A meta-analysis found that although most IBD risk loci are shared across different ethnic groups, a few specific risk loci exhibit differences in effect sizes.23 Global genomics research in 2023 showed that the frequency of carrying high-risk alleles for IBD in East Asian populations is significantly lower than that in European and American populations.24 Therefore, it is necessary to strengthen dietary guidance and disease screening for high-risk populations to reduce the risk of the disease.
Our research findings demonstrate that the prevalence of IBD among Chinese WRA increased significantly from 1990 to 2021. The standardized prevalence rate showed a fluctuating upward trend, with the most rapid growth observed during 2005–2011, which aligns with the global trend of rising IBD prevalence.25 The epidemiological evolution of IBD can be divided into four stages: emergence, accelerated incidence, composite prevalence, and prevalence equilibrium. Developing countries are in the emerging stage, while newly industrialized countries with rapid economic development are in the accelerated incidence stage.26 For China, this increase may be attributed to the rapid economic development and accelerated industrialization in developing countries. As China’s economic level has grown rapidly, lifestyle changes have occurred: Western-style diets high in calories, fat, and low in fiber have become increasingly common, which may have played a contributing role.27 Studies have shown that such dietary patterns disrupt intestinal microbiota balance, reducing the abundance of beneficial bacteria while promoting harmful microorganism growth, thereby inducing intestinal inflammation.28 At the same time, environmental factors like industrialization-induced pollution may impair gut immune and barrier functions, increasing susceptibility to IBD.29
Additionally, the increased use of antibiotics and other drugs may also be one of the factors contributing to the elevated prevalence of IBD. This is because antibiotic treatment can trigger complex dynamic changes in intestinal microbiota, potentially altering the composition and physiological functions of the intestinal microbiota.30 During the same period, the standardized DALY rate decreased significantly over the same period (AAPC = −0.43%). This reflects the substantial effectiveness of national advancements in medical technology and healthcare policy reforms, including the application of biologic agents and endoscopic early diagnosis in improving disease prognosis,31–35 as well as the New Rural Cooperative Medical Scheme in enhancing treatment accessibility.36
Notably, a brief plateau in the declining trends of both prevalence and DALY rates was observed from 2019 to 2021, a period that coincided with the outbreak of the COVID-19 pandemic and the implementation of strict prevention and control measures. The potential reasons may include the redistribution of medical resources and restricted access to medical care during the pandemic, leading to delays in new diagnoses and reduced elective treatments.37 Secondly, IBD patients receiving treatment with immunomodulatory biologic agents exhibit impaired humoral immunity following SARS-CoV-2 mRNA vaccination, resulting in an increased risk of breakthrough infections.38 Infections themselves can induce disease recurrence, which may potentially push up both prevalence and DALY rates in the short term.
In terms of the age effect.the 2021 disease burden indicators of IBD among Chinese WRA showed a consistent upward trend with age, peaking in the 45–49-year age group.This may be attributed to age-related declines in intestinal barrier function, altered immune cell activity, and reduced pathogen resistance.39 Studies by Woelfel et al found that with increasing age, Prevotella, Clostridiales, and Bifidobacterium gradually decrease. The loss of these microbiota impairs the production of short-chain fatty acids and antimicrobial peptides, disrupts intestinal barrier integrity, and thereby increases the risk of pathogen invasion and subsequent inflammatory responses.40 Meanwhile, hormonal fluctuations (eg, changes in estrogen) may impair intestinal mucosal repair and immune regulation, thus increasing the risk of IBD.41
In terms of period effect the disease risk peaks in 2007–2011 and 2012–2016 (RR = 1.59), potentially linked to economic transition–induced environmental changes and increased psychosocial stress. Studies indicate that genetic predisposition and environmental factors (such as diet and stress) disrupt immune homeostasis.42,43 However, the post-2017 decline in DALY risk (RR = 0.66) reflects improvements in public health awareness, healthcare access, and IBD management, which enhanced early diagnosis and treatment efficacy.
The birth cohort effect demonstrates an overall trend of fluctuating growth in disease risk, while DALY rate has gradually declined. Early birth cohorts (1992–1996), raised in relatively simple and natural environments, had more stable gut microbiota, whereas the later cohort (2002–2006) exhibited higher disease risk (RR = 1.61). This may be attributed to gut microbiota disruption from antibiotic misuse and environmental pollution, increasing IBD susceptibility.30,44 Meanwhile, with the continuous advancement of medical technology, the post-birth cohort is able to receive more timely and effective treatment after illness, which is an important reason for the reduced risk of DALYs.45
This study further indicates that the standardized prevalence is projected to show a slight upward trend from 2022 to 2035, while the DALY rate will continue its downward trend, with relatively stable overall fluctuations. These findings are consistent with the research results of scholars such as Luo.46 Potential driving factors include advancements in medical technology, which are expected to bring new therapeutic breakthroughs for IBD, including the clinical application progress of emerging technologies such as targeted adhesion molecule therapy, cytokine inhibitors, stem cell therapy, and host-microbiome interaction-based therapies, thereby reducing disease activity and improving long-term prognosis.47 Secondly, China’s dietary prevention and control strategies may have played a positive role. Among them, the Dietary Guidelines for Chinese Residents (2022) first proposed the “Oriental Healthy Dietary Pattern” to guide residents in making scientific dietary choices, meeting the needs of normal human growth and development, immunity, and physiological functions, ensuring the supply of energy and nutrients, and reducing the risk of diet-related chronic diseases.48 This pattern indirectly affects the risk of IBD through the dietary fiber-microbiota-immune axis mechanism.49
However, there remains a certain degree of uncertainty in the future. New environmental risk factors may continue to emerge, such as new pollutants and unknown pathogens, which may increase the prevalence risk of IBD. Therefore, we must not relax the prevention and control of IBD due to the projected results; instead, we need to continuously monitor disease dynamics and strengthen prevention and control measures.
However, The data in the GBD 2021 disease database relies on model-derived calculations rather than direct observed data, which may introduce deviations from real-world scenarios. Future research could integrate national e-health databases with multi-centre registry studies to acquire more precise epidemiological data.
Conclusion
From 1990 to 2021, the standardized prevalence rate of IBD among Chinese WRA showed an upward trend, while the standardized DALY rate showed a downward trend. Age, period, and birth cohort had significant impacts on the disease burden. It is predicted that the prevalence rate of IBD among Chinese WRA will show a slight upward trend from 2022 to 2035, while the DALY rate will continue to show a downward trend.
Abbreviations
IBD, Inflammatory Bowel Disease; WRA, Women of Reproductive Age; DALY, disability adjusted life year; GBD, Global Burden of Disease; AAPC, Average Annual Percentage Change; APC, Annual Percentage Change.
Data Sharing Statement
The data used for these analyses are all publicly available at online GBD repository (http://ghdx.healthdata.org/gbdresults-tool).
Acknowledgments
We extend our gratitude to the contributors of the Global Burden of Diseases, Injuries, and Risk Factors Study 2021 for their invaluable work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no potential conflicts of interest in this work.
References
1. Lamb CA, Kennedy NA, Raine T. et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1–s106. doi:10.1136/gutjnl-2019-318484
2. Inflammatory Bowel Disease Group CSOG, China IBDQ. Chinese Clinical Practice Guideline on Management of Ulcerative Colitis(2023, Xi′an). Gastroenterology. 2024;29(03):145–173.
3. Knowles SR, Keefer L, Wilding H, Hewitt C, Graff LA, Mikocka-Walus A. Quality of Life in Inflammatory Bowel Disease: a Systematic Review and Meta-analyses-Part II. Inflamm Bowel Dis. 2018;24(5):966–976. doi:10.1093/ibd/izy015
4. Park KT, Ehrlich OG, Allen JI, et al. The Cost of Inflammatory Bowel Disease: an Initiative From the Crohn’s & Colitis Foundation. Inflamm Bowel Dis. 2020;26(1):1–10. doi:10.1093/ibd/izz104
5. Hoogkamer AB, Brooks AJ, Rowse G, Lobo AJ. Predicting the development of psychological morbidity in inflammatory bowel disease: a systematic review. Frontline Gastroenterol. 2021;12(2):137–144.
6. Kaplan GG, Ng SC. Globalisation of inflammatory bowel disease: perspectives from the evolution of inflammatory bowel disease in the UK and China. Lancet Gastroenterol Hepatol. 2016;1(4):307–316. doi:10.1016/S2468-1253(16)30077-2
7. Dahlhamer JM, Zammitti EP, Ward BW, Wheaton AG, Croft JB. Prevalence of Inflammatory Bowel Disease Among Adults Aged ≥18 Years - United States, 2015. MMWR Morb Mortal Wkly Rep. 2016;65(42):1166–1169. doi:10.15585/mmwr.mm6542a3
8. Ng SC, Tang W, Ching JY, et al. Incidence and phenotype of inflammatory bowel disease based on results from the Asia-pacific Crohn’s and colitis epidemiology study. Gastroenterology. 2013;145(1):158–165.
9. Kappelman MD, Rifas–Shiman SL, Kleinman K, et al. The prevalence and geographic distribution of Crohn’s disease and ulcerative colitis in the United States. Clin Gastroenterol Hepatol. 2007;5(12):1424–1429. doi:10.1016/j.cgh.2007.07.012
10. Zhang Y, Liu J, Han X, et al. Long-term trends in the burden of inflammatory bowel disease in China over three decades: a joinpoint regression and age-period-cohort analysis based on GBD 2019. Front Public Health. 2022;10:994619. doi:10.3389/fpubh.2022.994619
11. H Wang, KM Abbas, M Abbasifard. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950-2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1160–1203. doi:10.1016/S0140-6736(20)30977-6
12. CJL Murray, AY Aravkin, P Zheng, C Abbafati. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1223–1249. doi:10.1016/S0140-6736(20)30752-2
13. CYTG May. Analysis for trends in disease burden of congenital birth defects among children under 5 years old in China. J Central South Univ. 2023;48(6):877–886.
14. VCF Pepito. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
15. Zhang J, Ma B, Han X, Ding S, Li Y. Global, regional, and national burdens of HIV and other sexually transmitted infections in adolescents and young adults aged 10–24 years from 1990 to 2019: a trend analysis based on the Global Burden of Disease Study 2019. Lancet Child Adolesc Health. 2022;6(11):763–776. doi:10.1016/S2352-4642(22)00219-X
16. Wang Y, Wang Y, Fan L, Yu Y. The Burden of Severe Periodontitis in China From 1990 to 2021, With Projections to 2050: a Comprehensive Analysis From The Global Burden of Disease Study 2021. Int Dent J. 2025;75(1):32–44. doi:10.1016/j.identj.2024.12.013
17. Hu W, Fang L, Zhang H, Ni R, Pan G. Global disease burden of COPD from 1990 to 2019 and prediction of future disease burden trend in China. Public Health. 2022;208:89–97. doi:10.1016/j.puhe.2022.04.015
18. T Vos, SS Lim, C Abbafati, KM Abbas. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
19. Hu XF, Zhang R, Chan HM. Identification of Chinese dietary patterns and their relationships with health outcomes: a systematic review and meta-analysis. Public Health Nutr. 2024;27(1):e209. doi:10.1017/S1368980024001927
20. Shin Y, Han S, Kwon J, et al. Roles of Short-Chain Fatty Acids in Inflammatory Bowel Disease. Nutrients. 2023;15(20):4466. doi:10.3390/nu15204466
21. Yan J, Zeng Y, Guan Z, et al. Inherent preference for polyunsaturated fatty acids instigates ferroptosis of Treg cells that aggravates high-fat-diet-related colitis. Cell Rep. 2024;43(8):114636. doi:10.1016/j.celrep.2024.114636
22. Gulhane M, Murray L, Lourie R, et al. High Fat Diets Induce Colonic Epithelial Cell Stress and Inflammation that is Reversed by IL-22. Sci Rep. 2016;6(1):28990. doi:10.1038/srep28990
23. Liu JZ, van Sommeren S, Huang H, et al. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat Genet. 2015;47(9):979–986. doi:10.1038/ng.3359
24. Liu Z, Liu R, Gao H, et al. Genetic architecture of the inflammatory bowel diseases across East Asian and European ancestries. Nat Genet. 2023;55(5):796–806. doi:10.1038/s41588-023-01384-0
25. Alatab S, Sepanlou SG, Ikuta K. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–30. doi:10.1016/S2468-1253(19)30333-4
26. Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2021;18(1):56–66. doi:10.1038/s41575-020-00360-x
27. Hua H, Jiang Q, Sun P, Xu X. Risk factors for early-onset colorectal cancer: systematic review and meta-analysis. Front Oncol. 2023;13:1132306. doi:10.3389/fonc.2023.1132306
28. Clemente JC, Ursell LK, Parfrey LW, Knight R. The impact of the gut microbiota on human health: an integrative view. Cell. 2012;148(6):1258–1270. doi:10.1016/j.cell.2012.01.035
29. Cui G, Liu H, Xu G, Laugsand JB, Pang Z. Exploring Links Between Industrialization, Urbanization, and Chinese Inflammatory Bowel Disease. Front Med Lausanne. 2021;8:757025. doi:10.3389/fmed.2021.757025
30. Münch PC, Eberl C, Woelfel S, et al. Pulsed antibiotic treatments of gnotobiotic mice manifest in complex bacterial community dynamics and resistance effects. Cell Host Microbe. 2023;31(6):1007–1020. doi:10.1016/j.chom.2023.05.013
31. Song YY, Zhang YF, Sun M, Zhang JF. Research advances of nano drug delivery systems for the treatment ofinflammatory bowel disease. Chin J Front Med. 2024;16(10):18–25.
32. Wu AQ, Luo ZN, Jang Y, Wang ZK, Zhu XP. Exploratory study on the ameliorative effects of Trichinella spiralisparamyosin on chronic inflammatory bowel disease. J Capital Med Univ. 2024;45(05):891–899.
33. Neurath MF. Strategies for targeting cytokines in inflammatory bowel disease. Nat Rev Immunol. 2024;24(8):559–576. doi:10.1038/s41577-024-01008-6
34. Borowitz SM. The epidemiology of inflammatory bowel disease: clues to pathogenesis? Front Pediatr. 2022;10:1103713. doi:10.3389/fped.2022.1103713
35. Abd-El KAA, Fahmy DM. Diagnostic Value of Diffusion-Weighted Imaging and Apparent Diffusion Coefficient in Assessment of the Activity of Crohn Disease: 1.5 or 3 T. Journal of Computer Assisted Tomography. 2018;42(5):688–696. doi:10.1097/RCT.0000000000000754
36. Meng Q, Fang H, Liu X, Yuan B, Xu J. Consolidating the social health insurance schemes in China: towards an equitable and efficient health system. Lancet. 2015;386(10002):1484–1492. doi:10.1016/S0140-6736(15)00342-6
37. Xiao H, Dai X, Wagenaar BH, et al. The impact of the COVID-19 pandemic on health services utilization in China: time-series analyses for 2016–2020. Lancet Reg Health West Pac. 2021;9:100122. doi:10.1016/j.lanwpc.2021.100122
38. Woelfel S, Dütschler J, König M, et al. STAR SIGN study: evaluation of COVID-19 vaccine efficacy against the SARS-CoV-2 variants BQ.1.1 and XBB.1.5 in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2023;58(7):678–691. doi:10.1111/apt.17661
39. Guo WW, Qi LL, Wang MT, Ke ZJ, Mao HG. The Relationship Between Intestinal Flora and Intestinal Mucosal lmmune Senescence. Adv Biochem Biophys. 2024;2024:1–17.
40. Woelfel S, Silva MS, Stecher B. Intestinal colonization resistance in the context of environmental, host, and microbial determinants. Cell Host Microbe. 2024;32(6):820–836. doi:10.1016/j.chom.2024.05.002
41. Khalili H, Higuchi LM, Ananthakrishnan AN, et al. Hormone therapy increases risk of ulcerative colitis but not Crohn’s disease. Gastroenterology. 2012;143(5):1199–1206. doi:10.1053/j.gastro.2012.07.096
42. Mawdsley JE, Rampton DS. Psychological stress in IBD: new insights into pathogenic and therapeutic implications. Gut. 2005;54(10):1481–1491. doi:10.1136/gut.2005.064261
43. Abegunde AT, Muhammad BH, Bhatti O, Ali T. Environmental risk factors for inflammatory bowel diseases: evidence based literature review. World J Gastroenterol. 2016;22(27):6296–6317. doi:10.3748/wjg.v22.i27.6296
44. Blaser MJ. Antibiotic use and its consequences for the normal microbiome. Science. 2016;352(6285):544–545. doi:10.1126/science.aad9358
45. Jones JL, Nguyen GC, Benchimol EI, et al. The Impact of Inflammatory Bowel Disease in Canada 2018: quality of Life. J Can Assoc Gastroenterol. 2019;2(Suppl 1):S42–S48. doi:10.1093/jcag/gwy048
46. Wang S, Dong Z, Wan X. Global, regional, and national burden of inflammatory bowel disease and its associated anemia, 1990 to 2019 and predictions to 2050: an analysis of the global burden of disease study 2019. Autoimmun Rev. 2024;23(3):103498. doi:10.1016/j.autrev.2023.103498
47. Higashiyama M, Hokari R. New and Emerging Treatments for Inflammatory Bowel Disease. Digestion. 2023;104(1):74–81. doi:10.1159/000527422
48. Cao QM, Wang WJ, Zhang L, Zw H, Wang YQ. The practice of balanced diet model for Chinese residents:Interpretation ofdietary guidelines for Chinese residents. Food Mach. 2022;38(06):22–29.
49. Alexander M, Turnbaugh PJ. Deconstructing Mechanisms of Diet-Microbiome-Immune Interactions. Immunity. 2020;53(2):264–276. doi:10.1016/j.immuni.2020.07.015
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Global Burden of Inflammatory Bowel Disease Among Women of Reproductive Age From 1990 to 2021 and Future Projections to 2050: A Comprehensive Analysis Using Eight Machine Learning Algorithms
Zhao J, Liu H, Tong L, Pu L, Yin X, Hu Y, Yang J, Zhu Y
International Journal of Women's Health 2025, 17:4471-4496
Published Date: 14 November 2025
Burden and Trends of Crohn’s Disease Among Women of Reproductive Age in China, India, and the United States, 1990–2023, with Projections to 2040: A Systematic Analysis for the Global Burden of Disease Study 2023
Lin F, Wei X, Song L, Xu G, Li J
International Journal of Women's Health 2026, 18:601157
Published Date: 18 May 2026