Back to Journals » International Medical Case Reports Journal » Volume 19
An Unusual Presentation of Superficial Temporal Artery Pseudoaneurysm Following Penetrating Head Injury
Authors Alasow MOD ![]() , Abdi MN, Osman FAO
, Abdi MN, Osman FAO ![]() , Osman AA
, Osman AA ![]() , Ali AA
, Ali AA
Received 10 November 2025
Accepted for publication 29 January 2026
Published 31 January 2026 Volume 2026:19 580465
DOI https://doi.org/10.2147/IMCRJ.S580465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Mohamed Osman Dahir Alasow,1 Mohamed Nor Abdi,2 Faisal Abdi Osoble Osman,1 Ahmed Adam Osman,1 Ali Abdikadir Ali3
1Radiology Department, Mogadishu Somali Turkey Recep Tayyip Erdogan Training and Research Hospital, Mogadishu, Somalia; 2ENT Department, Mogadishu Somali Turkey Recep Tayyip Erdogan Training and Research Hospital, Mogadishu, Somalia; 3Cardiovascular Department, Mogadishu Somali Turkey Recep Tayyip Erdogan Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Osman Dahir Alasow, Radiology Department, Mogadishu Somali Turkey Recep Tayyip Erdogan Training and Research Hospital, 30 Street, Albarako, Hodan District, Mogadishu, Somalia, Tel +252615428952, Email [email protected]
Abstract: Superficial temporal artery (STA) pseudoaneurysm is a rare vascular lesion that usually arises after blunt or penetrating trauma to the temporal region. Because the STA is only superficially covered by skin and subcutaneous tissue, it is highly susceptible to injury. We report the case of a 21-year-old male who presented with a painless, pulsatile swelling over the left temporal area three weeks after sustaining a knife injury. Doppler ultrasonography demonstrated a 4× 1.2 cm pseudoaneurysm with a characteristic “to-and-fro” flow pattern, and contrast-enhanced CT angiography confirmed an oval pseudoaneurysm originating from the left STA. Following surgical ligation and excision of the pseudoaneurysm, the patient recovered without incident. Any patient who presents with a pulsatile mass after facial or scalp trauma should be suspected of having a STA pseudoaneurysm. To ensure positive results, early diagnosis using Doppler or CT angiography and timely surgical management are crucial in preventing rupture, hemorrhage, and cosmetic deformity.
Keywords: superficial temporal artery, pseudoaneurysm, temporal region, blunt head injury, yin-yang sign
Introduction
A pseudoaneurysm is an arterial dilatation characterized by a deficiency in one or more layers of the arterial wall. Pseudoaneurysm of the superficial temporal artery (STA) is an uncommon complications of minor head trauma. It manifests gradually over a period of two to six weeks. It is often devoid of discomfort, gentle, and pulsatile. They predominantly impact the anterior branch of the STA.1–3 Head injuries can readily harm the artery because of this location, where the skin and fat tissues are its only defense. The typical manifestation features a pulsatile, painful edema that arises many days post-injury, frequently accompanied by cephalalgia or discomfort in the ipsilateral auricular area.2 In order to prevent consequences like skin ulcers and aneurysm rupture, it is essential to get a diagnosis and treatment immediately.2,4,5 If treatment is not received, these pseudoaneurysms tend to grow more and more until they cause significant bleeding.6 This report describes a case of pseudoaneurysm of the left superficial temporal artery resulting from blunt facial trauma inflicted by a knife.
Case Report
A 21-year-old male came to the ENT outpatient department with a primary complaint of a painless, pulsatile mass on the left side of the face, located anterior to the pinna, persisting for three weeks. The patient had a history of penetrating trauma (knife injury) to the same region from a battle around 24 days prior to presentation (Figure 1).
 |
Figure 1 Clinical photograph showing a linear laceration over the anterior aspect of the left ear, associated with localized swelling and tenderness. The wound appears clean, with no active bleeding, as indicated by the white arrow. |
Ultrasonography (USG) with Color Doppler identified a pseudoaneurysm of 4×1.2 cm in the subcutaneous tissue of the left superficial temporal area. Spectral Doppler analysis revealed a distinctive “to-and-fro” flow pattern around the lesion’s neck, accompanied by partial thrombotic adherence (Figure 2).
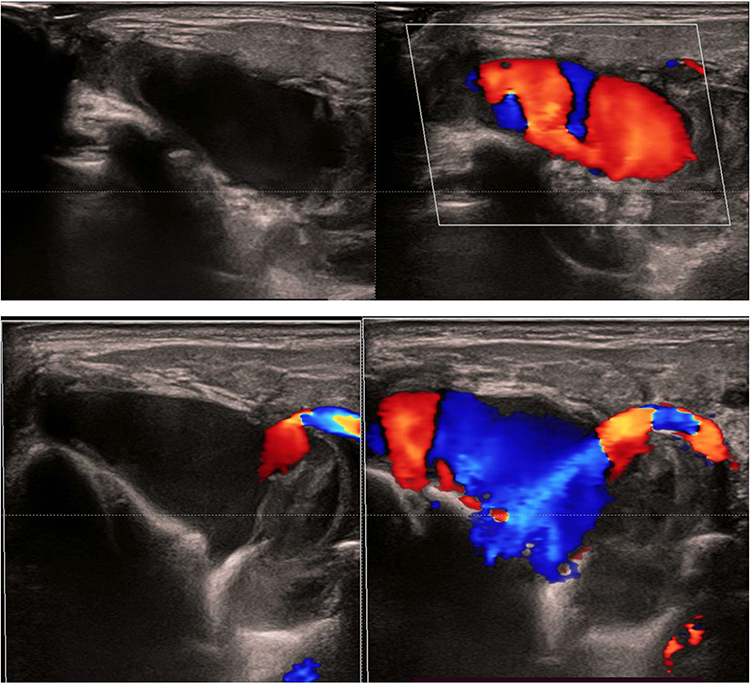 |
Figure 2 Ultrasonography with color Doppler demonstrates a well-defined pseudoaneurysm measuring approximately 4×1.2 cm within the subcutaneous tissue of the left superficial temporal region. Spectral Doppler analysis shows a characteristic “to-and-fro” flow pattern at the neck of the lesion, with evidence of partial mural thrombosis. |
A follow-up evaluation using contrast-enhanced computed tomography (CT) angiography showed a well-defined, oval-shaped pseudoaneurysm coming from the left superficial temporal artery. It was located in the left temporal region just in front of the parotid gland and was surrounded by mild soft-tissue swelling (Figures 3A, B and 4). The patient was later referred to the cardiovascular surgery section for surgical exploration. The artery next to the pseudoaneurysm was ligated, and the pseudoaneurysm was excised. The postoperative period was unremarkable, and the patient was discharged home seven days post-surgery.
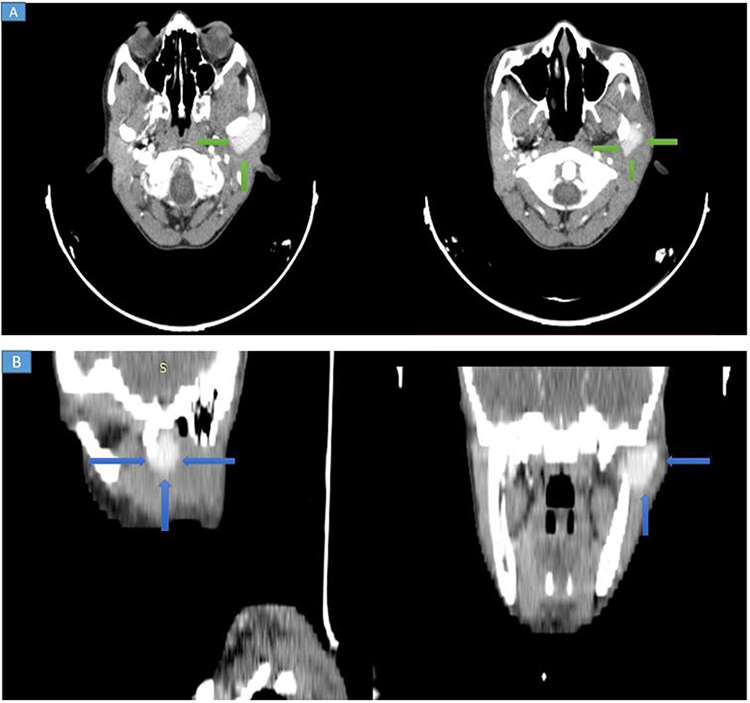 |
Figure 3 (A and B). Neck CT angiography demonstrates a well-defined, oval-shaped pseudoaneurysm arising from the left superficial temporal artery. The lesion is located in the left temporal region, anterior to the parotid gland, and is associated with mild surrounding soft-tissue swelling (blue and green arrows). |
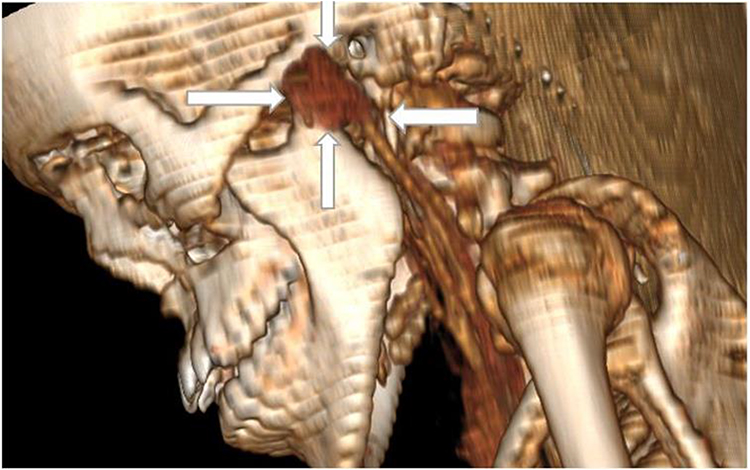 |
Figure 4 Three-dimensional reconstructed CT angiography image clearly delineates the pseudoaneurysm and its arterial origin from the left superficial temporal artery (white arrow). |
Discussion
In 1740, Thomas Bartholin reported the first instance of a superficial temporal artery pseudoaneurysm, which was caused by forceful trauma. The predominant etiology of superficial temporal artery pseudoaneurysm is blunt trauma, which constitutes 75% to 95% of cases; penetrating injuries or iatrogenic factors account for the remainder. STA pseudoaneurysms resulting from iatrogenic damage have been documented following cyst excision, temporomandibular joint arthroplasty, punch hair transplantation, and craniotomies.3,6–8
The STA and the internal maxillary artery are both branches that terminate in the external carotid artery. The anterior auricular artery, which supplies blood to the ears and nose, branches off to the orbicularis oculi muscle, which supplies the zygomatic orbital branch, the transverse facial artery, which supplies blood to the face and neck, and the temporalis muscle, which supplies blood to the back of the neck. It is common practice to classify the branches of the scalp as either frontal or parietal. The emissary veins’ foramina, which connect to the superior sagittal sinus, may form anastomoses between the STA and the meningeal system. The usual spot for these is somewhere around the midline.9–11 The diagnosis of a STA pseudoaneurysm is primarily clinical, based on a history of recent trauma and an examination revealing a pulsatile, painless, cystic mass in the temple, occasionally accompanied by an audible bruit during auscultation. The diagnosis is subsequently confirmed through imaging, generally via duplex ultrasound or CT angiography. The differential diagnosis encompasses epidermal inclusion cysts, lipomas, simple hematomas, enlarged lymph nodes, abscesses, hemangiomas or other vascular abnormalities, neuromas of the supraorbital nerve, and other soft tissue masses.9–13 Colour-flow The “yin-yang sign” and “to-and-fro” signs are Doppler ultrasonography markers of a partly thrombosed aneurysm.14 In our case, CT angiography confirmed the diagnosis (Figures 3 and 4).
Preventing rupture or bleeding, reducing pain, and achieving acceptable cosmetic outcomes are the objectives of pseudoaneurysm treatment.15 Proposed a treatment plan for STA pseudoaneurysm. Pseudoaneurysms are categorized according to the duration from commencement as follows: acute (<3 weeks), subacute (3 weeks to 3 months), or chronic (>3 months). Emergency surgery is indicated for individuals presenting with an acute pseudoaneurysm and hemodynamic instability. Subacute and chronic pseudoaneurysms may be addressed using surgical or endovascular methods, contingent upon the patient’s clinical circumstances or aesthetic preferences. The most effective conventional treatment is surgical ligation and resection, which entails the closure of afferent and efferent vessels and the removal of the pseudoaneurysm. Because there is a vast network of arterial collaterals, the consequences of removing the diseased artery segment can be minimal.2,15 Coil embolization, as an alternate therapeutic approach, is very efficacious, resulting in little face scarring; nevertheless, thickening in the temporal region may remain visible. Ultrasound-guided thrombin injection has been documented as a safe and effective treatment for subacute aneurysms persisting beyond three weeks and chronic aneurysms lasting over three months. Nonetheless, it may induce distant tissue necrosis.4 Surgical complications include facial nerve palsy resulting from lesions of the fronto-zygomatic branch of the facial nerve, skin defects arising from dissection near the skin, excessive bleeding, and cosmetic issues related to scarring from the procedure.1
Conclusion
Superficial temporal artery pseudoaneurysm is an infrequent yet clinically important complication of craniofacial trauma. Due to its subtle and frequently delayed manifestation, a heightened level of suspicion is crucial for prompt diagnosis. Duplex ultrasonography and CT angiography continue to be dependable, noninvasive modalities for validation. Prompt surgical ligation and excision are the best ways to treat the problem, and they have great functional and cosmetic results. Recognizing and acting quickly are very important to avoid rupture, too much bleeding, or other problems that could leave you with scars.
Ethical Approval
Ethical approval for this study was waived by ethical committee of Mogadishu Somali Turkey, Recep Tayyip Erdogan Training and Research Hospital.
Patient Consent Statement
The patient provided written informed consent for the publication of this case report and all related clinical images.
Disclosure
The authors declare that they have no financial or personal relationships that could inappropriately influence or bias the content of this case report.
References
1. Sommer C, Braye E, Rotman S, Joseph JM. Superficial temporal artery pseudoaneurysm after head injury in a teenager. J Pediatr Surg Case Rep. 2020;61:101592. doi:10.1016/j.epsc.2020.101592
2. Modugno P, Nocerino M, Modugno FM, et al. Symptomatic pseudoaneurysm of the superficial temporal artery: three case reports. Ann Vasc Surg - Br Reports Innov. 2025;5(3):100393. doi:10.1016/j.avsurg.2025.100393
3. Younus SM, Imran M, Qazi R. Superficial Temporal Artery Pseudoaneurysm: a Case Report. Front Surg. 2015;2(October):2–6. doi:10.3389/fsurg.2015.00051
4. Starzak M, Jakubiak GK, Pietrzak M, Cieślar G, Stanek A. Superficial temporal artery aneurysm. Acta Angiol. 2023;29(1):25–29. doi:10.5603/AA.2023.0002
5. Yadav R, Verma U, Tiwari R, Article O. Heterogeneous conceptualization of etiopathogenesis: oral pyogenic granuloma. Natl J Maxillofac Surg. 2019;10(1):3–7. doi:10.4103/njms.NJMS
6. Brandt A, Schaefer IM, Rustenbeck HH, Matthias C, Laskawi R. Aneurysm of the superficial temporal artery following parotid gland surgery-Case report and review of the literature. Oral Maxillofac Surg. 2013;17(4):307–309. doi:10.1007/s10006-012-0385-y
7. Fukunaga N, Hanaoka M, Masahira N, et al. Traumatic pseudoaneurysm of superficial temporal artery. Am J Surg. 2010;199(1):e1–e2. doi:10.1016/j.amjsurg.2009.03.022
8. Leeman M, Leus A, Ernst C. Post-Traumatic Pseudoaneurysm of the Superficial Temporal Artery in a Pediatric Patient. J Belgian Soc Radiol. 2023;107(1):1–4. doi:10.5334/jbsr.3024
9. Walker MT, Liu BP, Salehi SA, Badve S, Hunt Batjer H. Superficial temporal artery pseudoaneurysm: diagnosis and preoperative planning with CT angiography. Am J Neuroradiol. 2003;24(1):147–150.
10. Mann GS, Heran MKS. Percutaneous thrombin embolization of a post-traumatic superficial temporal artery pseudoaneurysm. Pediatr Radiol. 2007;37(6):578–580. doi:10.1007/s00247-007-0447-8
11. Disch K, McKee J. Posttraumatic pseudoaneurysm involving the superficial temporal artery in a pediatric patient. J Pediatr Surg Case Rep. 2021;69:101850. doi:10.1016/j.epsc.2021.101850
12. Stapleton CJ, Fusco MR, Thomas AJ, Levy EI, Ogilvy CS. Traumatic pseudoaneurysms of the superficial temporal artery: case series, anatomy, and multidisciplinary treatment considerations. J Clin Neurosci. 2014;21(9):1529–1532. doi:10.1016/j.jocn.2014.02.004
13. Burleson S, Cirillo F, Gibson C, Gullett J, Pigott D. Superficial Temporal Artery Pseudoaneurysm Diagnosed by Point-of-Care Ultrasound. Clin Pract Cases Emerg Med. 2019;3(1):77–78. doi:10.5811/cpcem.2018.11.40958
14. Bernstein JM, Bury RW, Nigam A. Superficial temporal artery pseudoaneurysm: first reported case after parotid surgery. J Laryngol Otol. 2010;124(4):441–442. doi:10.1017/S0022215109991575
15. Kang I, Mo YW, Jung GY, Shin HK. Pseudoaneurysm of the superficial temporal artery after blunt trauma: case report and literature review. Arch Craniofacial Surg. 2022;23(3):130–133. doi:10.7181/acfs.2022.00178
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.