Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
An Uncommon Clinical Patterns of Proximal Subungual Onychomycosis Caused by Penicillium rubens
Authors Dong X, Luo L, Zhang W
Received 10 December 2025
Accepted for publication 4 March 2026
Published 11 March 2026 Volume 2026:19 586209
DOI https://doi.org/10.2147/CCID.S586209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Xian Dong,1 Liqiong Luo,2 Wei Zhang1
1Department of Dermatology, the Affiliated Hospital of Guizhou Medical University, Guiyang, People’s Republic of China; 2Department of Dermatology, the First People’s Hospital of Fuquan City, Fuquan, People’s Republic of China
Correspondence: Wei Zhang, Department of Dermatology, the Affiliated Hospital of Guizhou Medical University, No. 28 Guiyi Street, Guiyang, Guizhou, 550001, People’s Republic of China, Email [email protected]
Abstract: Proximal subungual onychomycosis (PSO) is a rare type of onychomycosis, which is commonly seen in patients with compromised immune systems. The pathogens include Trichophyton rubrum, Microsporum canis, Fusarium species, Aspergillus brasiliensis, Trichophyton erinacei, Aspergillus niger, and Aspergillus flavus. Onychomycosis caused by Penicillium is rarely reported. We report a rare clinical manifestation of proximal subungual onychomycosis caused by Penicillium rubens in an immunocompetent individual.
Keywords: proximal subungual onychomycosis, penicillium rubens
Introduction
Onychomycosis is a common infectious disease of the fingernails or toenails, mainly caused by dermatophytes, non-dermatophytic molds (NDMs) and yeast.1 Proximal subungual onychomycosis (PSO) is the least frequently observed clinical subtype of onychomycosis. In most cases, the fungal infection originates from the proximal nail fold and subsequently involves the nail plate.1 The pathogens include Trichophyton rubrum, Microsporum canis, Fusarium species, Aspergillus brasiliensis, Trichophyton erinacei, Aspergillus niger, and Aspergillus flavus.1–7 Previous relevant literature reports indicate that proximal subungual onychomycosis is commonly seen in patients with compromised immune function, especially in those with AIDS.8,9 The most common pathogens is Trichophyton rubrum. However, in healthy individuals, proximal subungual onychomycosis is rare. We report a case of proximal subungual onychomycosis caused by Penicillium rubens exhibiting rare clinical manifestations in an immunocompetent patient.
Case Report
A 29-year-old healthy woman presented with a crescent-shaped white discoloration and a pale pink nodule on her right thumbnail, which had persisted for 20 days. Physical examination revealed a crescent-shaped white discoloration at the proximal portion of the patient’s right thumbnail (red arrow) (Figure 1A). The nail surface was smooth (yellow arrow) (Figure 1A). Moreover, desiccation and desquamation of the proximal nail fold were observed (blue arrow) (Figure 1A). A pale pink nodule (green arrow, Figure 1A) (dermoscopic examination revealed unstructured white areas, green arrow, Figure 1B) was noted at the proximal nail fold, along with atypical vessels (purple arrow) (Figure 1A). The patient denied any prior trauma. The results of the rapid plasma reagin (RPR) titer, treponema pallidum particle agglutination assay (TPPA), and human immunodeficiency virus (HIV) test were all within the reference range. Microscopic analysis of nail material with potassium hydroxide revealed septate hyphae (Figure 2A). Subsequently, nail scrapings from the patient were cultured (in duplicate), using Sabouraud’s dextrose agar (SDA) as the medium, and incubated at 26°C for two weeks. The Penicillium isolated from all cultures had a characteristic green color (Figure 2B). Microscopic examination of the isolate stained with cotton blue revealed broom-shaped conidia and septate hyphae (Figure 2C). The DNA sequence of the internal transcribed spacer region of the clinical sample was a 100% match to that of Penicillium rubens. The patient refused to undergo an immediate pathological biopsy of the pale pink nodule at the proximal nail fold. She was subsequently diagnosed with Penicillium rubens-induced proximal subungual onychomycosis (PSO). The patient underwent pulse therapy with itraconazole (200 mg bid for one week each month), resulting in significant improvement after three courses. The pale pink nodule and atypical vessels dilation at the proximal nail fold of the patient have both subsided, and the nail returned to normal (Figure 3); then the patient was lost to follow-up. Six months after the treatment, we conducted a follow-up by phone. The patient reported that the nail lesion had completely subsided and there were no signs of recurrence.
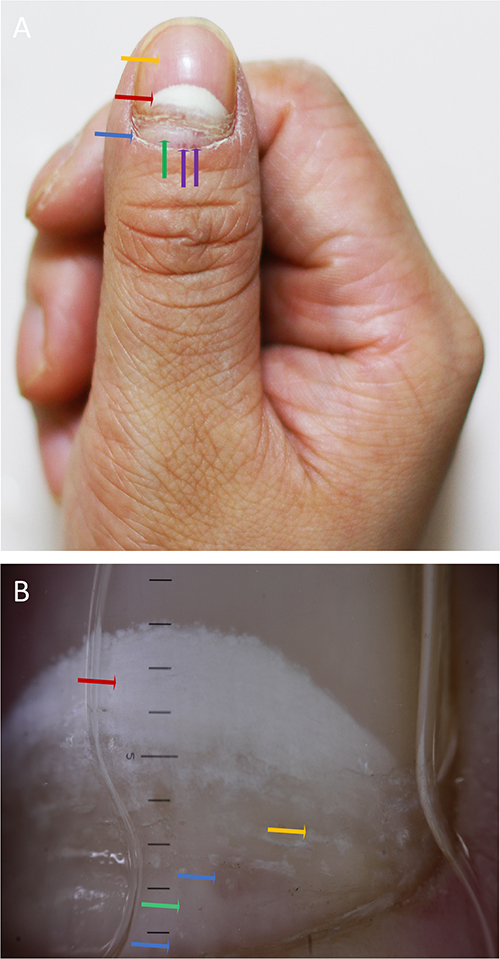 |
Figure 1 Clinical and dermatoscopic images of the patient before treatment. (A): Clinical image of the patient prior to treatment: a crescent-shaped white discoloration of the right thumbnail (red arrow), a smooth nail surface (yellow arrow), desiccation and desquamation of the proximal nail folds (blue arrow), a notable light pink nodule (green arrow) and atypical vessels (purple arrow) at the proximal nail fold; (B) Dermatoscopic image of the patient prior to treatment: a crescent-shaped, marble-like turbid area (red arrow), point-like turbidity (yellow arrow), and a pale red area (blue arrow, atypical vessels not clearly visible due to compression), with unstructured white areas (green arrow). |
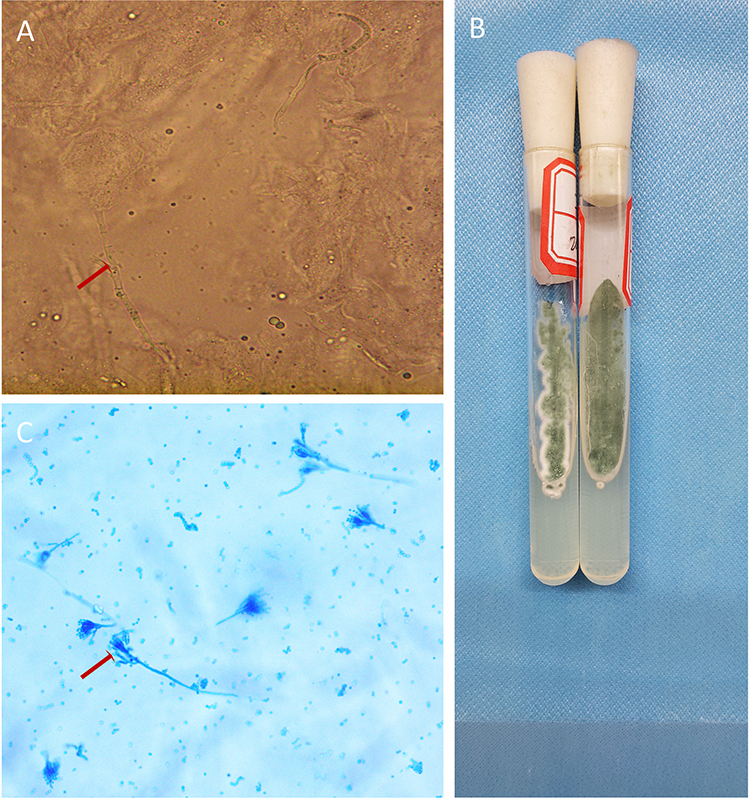 |
Figure 2 Direct microscopy, culture, and identification of fungi from the patient’s nail. (A): Direct microscopy of the patient’s nail plate scales reveals septate hyphae (red arrow), x400; (B): Culture of the patient’s nail plate scales shows greenish colonies; (C): Microscopic examination of the isolate stained with cotton blue reveals broom-shaped conidia and septate hyphae (red arrow), x200). |
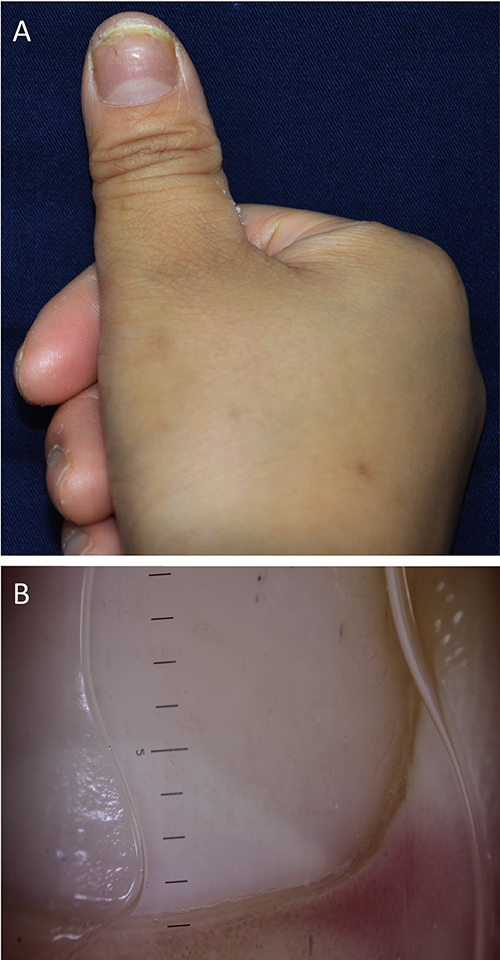 |
Figure 3 Clinical and dermatoscopic images of the patient after treatment. (A): Clinical image of the patient after treatment: the notable light pink nodule and atypical vessels at the proximal nail fold in the patient disappeared, and the nail returned to normal; (B): Dermatoscopic image of the patient after treatment: the crescent-shaped, marble-like turbid area, point-like turbidity, the pale red area and unstructured white areas disappeared). |
Discussion
Penicillium was first described in 1809 and is characterized by its minute, brush-like fruiting structures.1 This genus represents an opportunistic saprophyte that exhibits widespread distribution and can thrive in a variety of environments, including soil. They are more common in temperate regions but relatively rare in arid tropical areas. Currently, over 350 species have been classified within the genus Penicillium, with Penicillium rubens being an important representative species. This fungus represents one of the earliest filamentous fungi to garner significant attention due to its potential value and has been extensively utilized in the production of penicillin.10,11
Onychomycosis is one of the most common nail diseases worldwide, mainly caused by dermatophyte mold infections.1 Onychomycosis resulting from mold infection is uncommon. Onychomycosis can be classified into five types: white superficial onychomycosis, distal and lateral subungual onychomycosis, candidal onychomycosis, proximal subungual onychomycosis, and endonyx onychomycosis.1 Proximal subungual onychomycosis primarily involves the nail plate at the proximal nail fold and represents one of the less common forms of onychomycosis. This condition is typically associated with immunocompromised states and is exceedingly rare in the general population.2 The main pathogen of proximal subungual onychomycosis is Trichophyton rubrum, but there are also reports indicating that Microsporum canis, Fusarium species, Aspergillus brasiliensis, Trichophyton erinaceid, Aspergillus niger and Aspergillus flavus may be potential pathogens.1–7 This article reports a case of PSO caused by Penicillium rubens. The patient was an adult female with normal immune function, highlighting the pathogenicity of non-dermatophytic molds in onychomycosis.
In contrast to the majority of previously published literatures, which typically describe proximal subungual onychomycosis (PSO) as a slowly progressive fungal nail infection with a duration spanning several months,3–7 the clinical course observed in this case deviates from the conventional pattern. In this case, the patient exhibited a markedly abbreviated disease course, with only 20 days elapsing between the initial appearance of visible lesions and clinical presentation, reflecting an atypically rapid clinical progression. Notably, this patient lacks commonly recognized predisposing factors, including immunodeficiency, diabetes mellitus, or a history of long-term glucocorticoid or immunosuppressant use, and the assessment of immune function is also normal. Despite the absence of traditional high-risk factors, a small, pale pink nodule with well-defined margins and mild elevation developed rapidly at the proximal nail fold of the right thumb. No significant pain or tenderness was observed. More particularly, dermoscopy revealed atypical vascular structures within the nodule, which are extremely rarely reported in fungal infections.
Direct microscopic examination revealed the presence of septate hyphae, and subsequent fungal culture confirmed infection with Penicillium rubens (corroborated by DNA sequencing). This finding is particularly significant, as Penicillium rubens is rarely recognized as a common pathogen of proximal subungual onychomycosis (PSO), especially in individuals with normal immune function. Sporadic case reports have indicated that some species of Penicillium may be associated with onychomycosis; however, the underlying pathogenic mechanisms, invasive potential, and clinical characteristics remain poorly understood.12,13
Therefore, the pale pink nodules at the proximal nail fold with atypical vascular patterns in this case may represent an early and atypical clinical manifestation of proximal subungual onychomycosis in immunocompetent individuals, especially possibly related to rare pathogenic fungi such as Penicillium infection. This manifestation is prone to be misdiagnosed as whether it is accompanied by pyogenic granuloma of the nail, periungual fibroma, subungual exostosis, onychopapilloma, squamous cell carcinoma or amelanotic melanoma. This underscores the need for clinicians to adopt a broad differential diagnostic approach when evaluating patients with abnormal nail morphology.
Conclusions
Currently, it remains undetermined whether these atypical clinical manifestations are specific to Penicillium infection, and no definitive association with particular species has been established. Future studies should focus on accumulating additional cases and conducting systematic investigations that integrate microbiological identification, antifungal drug susceptibility testing, histopathological analysis, and imaging characteristics to elucidate the epidemiological profile, underlying pathogenic mechanisms, and prognostic implications of this form of PSO. Regarding the limitation of this study that the antifungal drug sensitivity test was not conducted, we will pay close attention to it in the subsequent research and systematically improve the relevant experimental design and detection process. Furthermore, strengthening awareness of atypical pathogenic fungi and enhancing laboratory capacities in fungal culture and molecular identification will contribute to improved early diagnostic rates, optimized antifungal treatment strategies, and the prevention of misdiagnosis and inappropriate management.
Data Sharing Statement
The data underlying the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
The publication of case reports does not require ethical approval. We confirm that the publication of case details does not require institutional approval.
Consent Statement
The patient has provided written informed consent for the anonymous publication of their personal information in this article.
Acknowledgments
The authors would like to thank the patient for participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Doctoral Research Startup Foundation of the Affiliated Hospital of Guizhou Medical University (Grant Number: gyfybsky-2024-11); Guizhou Provincial Natural Science Foundation (Qiankehe Ji Chu-ZK[2022] General 449).
Disclosure
The authors declare that there are no conflicts of interest associated with this study.
References
1. Shah AA, Mirza R, Sattar A, et al. “Unveiling onychomycosis: pathogenesis, diagnosis, and innovative treatment strategies”. Microb Pathog. 2025;198:107–6. doi:10.1016/j.micpath.2024.107111
2. Leung AKC, Lam JM, Leong KF, et al. Onychomycosis: an Updated Review. Recent Pat Inflamm Allergy Drug Discov. 2020;14(1):32–45.
3. Álvarez-Salafranca M, Hernández-Ostiz S, Salvo Gonzalo S, et al. Proximal subungual onychomycosis due to aspergillus niger: a simulator of subungual malignant melanoma. Actas Dermosifiliogr. 2017;108:482–485. doi:10.1016/j.ad.2016.11.002
4. Andersen PL, Henning MAS, Jemec GBE, et al. Two cases of proximal subungual onychomycosis caused by trichophyton rubrum in hiv-negative patients during treatment with tnf-α inhibitors combined with methotrexate. Acta Dermatovenerol Croat. 2018;26:304–306.
5. Liang SE, Cohen DE, Rieder EA. Proximal Subungual Onychomycosis in the Immunocompetent: a Case Report and Review of the Literature. J Drugs Dermatol. 2018;17:475–478.
6. Phaitoonwattanakij S, Leeyaphan C, Bunyaratavej S, et al. Trichophyton erinacei onychomycosis: the first to evidence a proximal subungual onychomycosis pattern. Case Rep Dermatol. 2019;11:198–203. doi:10.1159/000501424
7. Mehta M, Sharma J, Bhardwaj SB. Proximal subungual onychomycosis of digitus minimus due to Aspergillus brasiliensis. Pan Afr Med J. 2020;35:79. doi:10.11604/pamj.2020.35.79.20762
8. Daniel CR 3rd, Norton LA, Scher RK. The spectrum of nail disease in patients with human immunodeficiency virus infection. J Am Acad Dermatol. 1992;27:93–97. doi:10.1016/0190-9622(92)70163-A
9. Gómez-Moyano E, Crespo-Erchiga V. HIV infection manifesting as proximal white onychomycosis. N Engl J Med. 2017;377(18):e26. doi:10.1056/NEJMicm1703082
10. Pitt JI, Hocking AD. Penicillium and Talaromyces. Fungi and Food Spoilage Springer, Cham. 2022;231–349.
11. Iacovelli R, Bovenberg RAL, Driessen AJM. Nonribosomal peptide synthetases and their biotechnological potential in Penicillium rubens. J Ind Microbiol Biotechnol. 2021;48(7–8):kuab045.
12. Ramani R, Ramani A, Shivananda PG. Penicillium species causing onychomycosis. J Postgrad Med. 1994;40(2):87–88.
13. Panggabean SD, Hustrini NM. A successful management of fungal peritonitis caused by Rhodotorula glutinis in CAPD patient, coincident with onychomycosis by Penicillium sp: case report. Medicine. 2023;102(28):e34199.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.