Back to Journals » Clinical Ophthalmology » Volume 8
An evidence-based review of unoprostone isopropyl ophthalmic solution 0.15% for glaucoma: place in therapy
Received 5 January 2014
Accepted for publication 7 February 2014
Published 10 March 2014 Volume 2014:8 Pages 543—554
DOI https://doi.org/10.2147/OPTH.S41562
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Derrick S Fung, Jess T Whitson
Department of Ophthalmology, University of Texas Southwestern Medical Center, Dallas, TX, USA
Abstract: Glaucoma is a progressive, neurodegenerative optic nerve disease that can cause significant visual morbidity and affects over 60 million people worldwide. The only known modifiable risk factor for glaucoma at this time is elevated intraocular pressure (IOP), which may be treated with medications, laser therapy, and/or incisional surgery. Topical ocular medications are commonly used as first-line therapy for glaucoma, although side effects may limit their use. Unoprostone is a novel 22-carbon ocular hypotensive agent that may be advantageous in treating some patients with open angle glaucoma or ocular hypertension. Unlike the 20-carbon prostanoids, such as latanoprost, that lower IOP primarily through an increase in uveoscleral outflow, unoprostone may lower IOP through increased aqueous outflow via the conventional trabecular meshwork pathway. Although not as efficacious as other prostanoids, unoprostone is effective for IOP reduction both as monotherapy and adjunctive therapy with timolol. Unoprostone has decreased affinity for the prostaglandin F2α receptor, which may explain its well tolerated ocular and systemic side effect profile compared with other prostanoids.
Keywords: unoprostone, Rescula®, prostaglandin, glaucoma, medication
Introduction
Glaucoma is defined as a group of diseases with a characteristic optic neuropathy and associated visual function changes. The visual loss that occurs from glaucoma is irreversible. It represents a significant public health problem, given that over 60 million people have glaucoma worldwide and this number is increasing.1 It is the second most common cause of blindness in the world following cataract, and the main cause of irreversible blindness.1,2 Risk factors for glaucoma include elevated intraocular pressure (IOP), family history, age, race, a thin central cornea, and low ocular perfusion pressure.3,4 Elevated IOP is currently the only known modifiable risk factor for glaucoma. Lowering IOP has been shown to slow visual field deterioration and is protective against both the development and progression of glaucoma.5–7 Current glaucoma treatment is focused on lowering IOP with medications, laser therapy, and/or incisional surgery.
Medical therapy is commonly employed as first-line treatment for glaucoma. Current options for topical therapy include alpha agonists, beta antagonists, carbonic anhydrase inhibitors, miotics, and prostaglandin analogs. Most topical ocular hypotensive agents used today are well tolerated, although side effects can limit their effectiveness due to poor patient compliance. Having a large selection of ocular hypotensive agents allows clinicians to better tailor medication regimens for glaucoma patients to balance clinical efficacy and side effects. With increasing medical treatment options, more invasive glaucoma therapy, such as laser or surgery, may be delayed or avoided altogether.
Unoprostone is an IOP-lowering docosanoid and part of a family of lipid IOP-lowering agents, or prostanoids. Under the trade name Rescula®, unoprostone isopropyl ophthalmic solution 0.12% was developed by R-Tech Ueno, Ltd (Tokyo, Japan) and has been marketed there since 1994.8 It first received approval as a second-line agent for the treatment of glaucoma and ocular hypertension by the US Food and Drug Administration (FDA) in 2000 as a prostaglandin analog and was marketed by Ciba Vision, a unit of Novartis (Basel, Switzerland), as a 0.15% solution.8 In 2009, Sucampo Pharmaceuticals, Inc. (Bethesda, MD, USA) acquired the commercialization rights for unoprostone in the USA and Canada.8 In 2011, these rights were expanded to include all territories worldwide, excluding parts of Asia.8 Last year, the FDA revised its formal label for unoprostone to include a first-line indication for the treatment of glaucoma and ocular hypertension.9 Also, the FDA removed its description of the drug as a prostaglandin analog. Unlike the prostaglandin analogs, which are 20-carbon derivatives of the eicosanoid prostaglandin F2α, unoprostone is a 22-carbon derivative of docosahexaenoic acid with little to no affinity for the prostaglandin receptor (see Figure 1).8,10 Additionally, recent studies show it may work, at least in part, by activating potassium (BK) and chloride (CIC-2 type) channels, leading to relaxation of the trabecular meshwork and increased outflow of aqueous humor though the conventional pathway.9
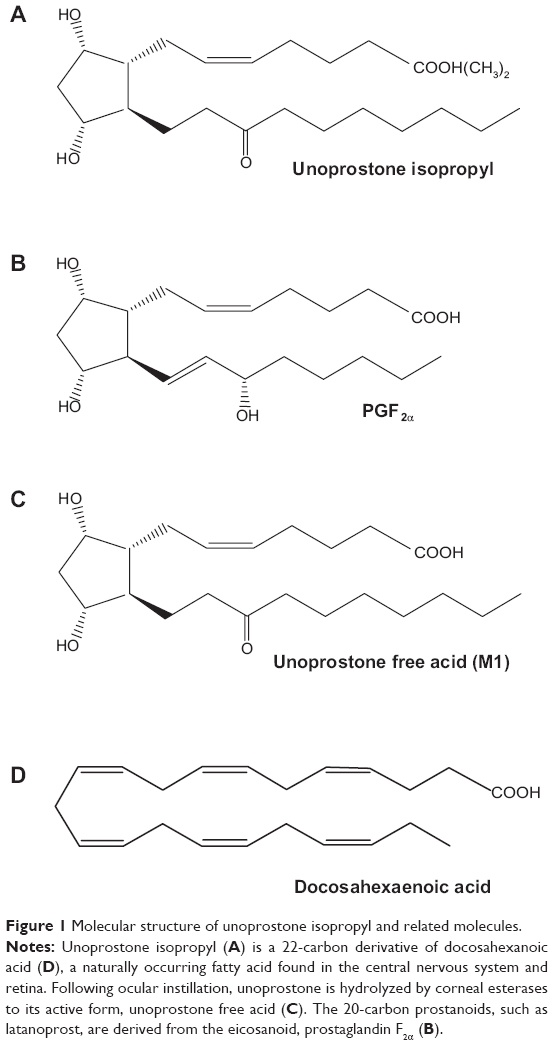 | Figure 1 Molecular structure of unoprostone isopropyl and related molecules. |
Description
Unoprostone isopropyl is a synthetic docosanoid molecule and a derivative of docosahexaenoic acid, which is a naturally occurring omega-3 polyunsaturated fatty acid endogenous to the central nervous system and retina.8,11 Its chemical name is isopropyl (+)-(Z)-7-[(1R,2R,3R,5S)-3,5-dihydroxy-2-(3-oxodecyl)cyclopentyl]-5-heptenoate, and its chemical formula is C25H44O5.9 Docosahexaenoic acid is essential for the development and proper functioning of photoreceptor cells, and has been shown to prevent photoreceptor apoptosis associated with oxidative stress in cell cultures.11–13 Unoprostone 0.15% (Rescula) is formulated as a sterile, isotonic, buffered aqueous solution of unoprostone isopropyl with a pH of 5.0–6.5 and preserved with 0.015% of benzalkonium chloride.9
Pharmacokinetics
Unoprostone isopropyl is readily hydrolyzed by esterases to its active form, unoprostone free acid (M1), (3-[(1R,2R,3R,5S)-3,5-dihydroxy-2-(3-oxodecyl)cyclopentyl]propionic acid), as shown in Figure 1.8 Unlike the prostaglandin analog latanoprost, which is metabolized only by corneal esterases, unoprostone undergoes additional metabolism once inside the eye by iris and ciliary body esterases.14 This effect may explain the shortened clinical efficacy of unoprostone when compared with latanoprost. In a study of 18 healthy volunteers given unoprostone isopropyl 0.15% ophthalmic solution twice daily in both eyes for 14 days, the mean peak unoprostone free acid plasma concentration was <1.5 ng/mL and dropped below the lower limit of quantitation (<0.250 ng/mL) 1 hour following instillation, indicating low systemic absorption and rapid plasma excretion.9 Excretion is rapid through the kidneys, with a half-life of 14 minutes. Unoprostone will begin to reduce IOP 30 minutes after ocular instillation.15 A clinically sustained effect, however, requires at least 2 weeks of twice-daily therapy.8
Mechanism
The mechanism of action for the IOP-lowering effect of unoprostone is controversial. Early studies showed that unoprostone increases aqueous humor outflow through the uveoscleral pathway similar to the 20-carbon prostaglandin analogs, such as latanoprost.8 More recent evidence, however, shows that it may work, at least in part, through stimulation of Ca2+-activated BK and CIC-2 type channels, leading to increased trabecular meshwork outflow. It is these later studies which have prompted the FDA to remove the prostaglandin designation from its formal label.9
The prostaglandin analogs, including prostaglandin F2α, latanoprost, and travoprost, mediate their ocular hypotensive effect by stimulating the prostaglandin F2α (FP) receptor.16–18 These medications have been confirmed in the literature as FP receptor agonists, and induce ciliary muscle relaxation leading to early IOP reduction via increased uveoscleral outflow.16–20 The early ocular hypotensive effect of prostaglandin F2α is blocked with concurrent use of pilocarpine, which contracts the longitudinal muscle of the ciliary body. This contraction counteracts prostaglandin-mediated ciliary muscle relaxation, thus blocking the early hypotensive effect.16,21
With long-term prostaglandin use, the ciliary muscle undergoes remodeling of the cytoskeletal proteins actin and vinculin via mediation of collagen turnover, further contributing to increased uveoscleral outflow and sustained IOP reduction.16 Other studies have suggested that some aqueous humor outflow may also occur at least in part through the trabecular meshwork pathway as well.22 The remodeling and turnover of the extracellular matrix in the ciliary muscle is believed to be related to the balance between matrix metalloproteinase (MMP) and tissue inhibitors of metalloproteinase (TIMP). Prostaglandin F2α showed increased c-Fos expression in human ciliary muscle cells, which induces expression of MMPs.16,23–25 Bimatoprost, latanoprost, and unoprostone all increase MMP activity in human ciliary body smooth muscle cells except for MMP-2.26 Unoprostone was found to decrease MMP-2 activity and increase TIMP activity. This difference in MMP/TIMP balance between the prostaglandin analogs may explain the lower clinical efficacy of unoprostone.
In contrast with latanoprost, unoprostone has only weak activity on the FP receptor, and its ocular hypotensive effect is believed to involve more than FP receptor activation alone. As opposed to increasing uveoscleral outflow, unoprostone has been shown to increase outflow facility through the trabecular meshwork.27
Unoprostone acts on BK channels that, upon activation, lead to cell hyperpolarization.28,29 Endothelin-1 (ET-1) is known to induce trabecular meshwork contractility mediated via glutamate-associated increases in intracellular Ca2+.28,30 Through BK channel activation, unoprostone is believed to block this increase in intracellular Ca2+ in trabecular meshwork cells and contribute to increased trabecular meshwork outflow and IOP reduction. This mechanism is supported by studies of iberiotoxin, a specific inhibitor of BK channel activation. Iberiotoxin was found to inhibit the hyperpolarization effect of unoprostone.13,28,30 Another study found that unoprostone also acts on L-type Ca2+ channel currents in the trabecular meshwork and that it reduced trabecular meshwork contractility independent of ET-1.31
The effect of unoprostone on ET-1 is also believed to mediate a possible neuroprotective benefit.8 ET-1 is believed to play a role in cell apoptosis and ocular blood flow. The glutamate-associated hypercalcemia that accompanies injury-induced retinal and ganglion cell apoptosis may be mediated by ET-1.13,28,29 ET-1 is known to cause vasoconstriction of vascular smooth muscle, and unoprostone may allow for increased ocular blood flow by blocking this vasoconstriction.32–36 This effect was studied in healthy subjects and patients with normal tension glaucoma using a scanning laser Doppler flowmeter, and measures of ocular microcirculation were found to be improved with unoprostone treatment.37 A study done in healthy individuals given intravenous ET-1 found that topical unoprostone significantly decreased the reduction in choroidal blood flow induced by ET-1.35
Several animal studies have found protective effects of unoprostone on nerve injury, specifically on retinal ganglion cell death,38–40 although one study did find that suppression of ET-1 occurred with travoprost and not unoprostone.41 These findings suggest possible neuroprotective properties associated with unoprostone. A recent study by Tawada et al evaluated the effect of twice-daily topical unoprostone on central retinal sensitivity in 30 patients with retinitis pigmentosa.42 After 6 months of therapy, retinal sensitivity improved significantly by fundus microperimetry and visual field mean deviation. Further research is needed to investigate the potential role of unoprostone as a neuroprotective agent in retinal disease.
Efficacy
Unoprostone as monotherapy
Early Japanese studies of unoprostone found modest IOP reduction with fewer ocular side effects compared with prostaglandins E2 and F2α.42–46 Unoprostone typically lowers IOP by 10%–25% from baseline, with a duration of effect of 2–5 hours compared with a 25%–30% reduction in IOP with latanoprost which may last up to 24 hours and beyond.47 Table 1 lists published randomized clinical trials of unoprostone when used as monotherapy.48–62 Most of these studies compared unoprostone with timolol and latanoprost as monotherapy. Many studies have documented the superior efficacy in IOP reduction of latanoprost compared with unoprostone in primary open angle glaucoma and normal tension glaucoma.52–59,63–66 Sponsel et al compared the IOP-lowering and hydrodynamic effects of unoprostone and latanoprost in paired eyes of 25 patients with open-angle glaucoma or ocular hypertension.59 Following one month of therapy, both agents produced significant reductions in IOP and increases in pulsatile ocular blood flow, although the changes seen with latanoprost were nearly two-fold greater than those seen with unoprostone, which was statistically significant. Although some studies have found equivalent IOP reduction between timolol and unoprostone,48–50 Nordmann et al in a 24-month multicenter, double-masked, randomized trial of 556 patients with glaucoma or ocular hypertension who received either twice-daily unoprostone, betaxolol, or timolol for 6 months, found similar mean diurnal IOP-lowering efficacy between betaxolol and unoprostone monotherapy.60 Both groups achieved an IOP reduction of 3–4 mmHg, or 18%–20%, from baseline. In this study, however, timolol monotherapy produced a significantly greater mean diurnal IOP reduction than either unoprostone or betaxolol (see Figure 2).
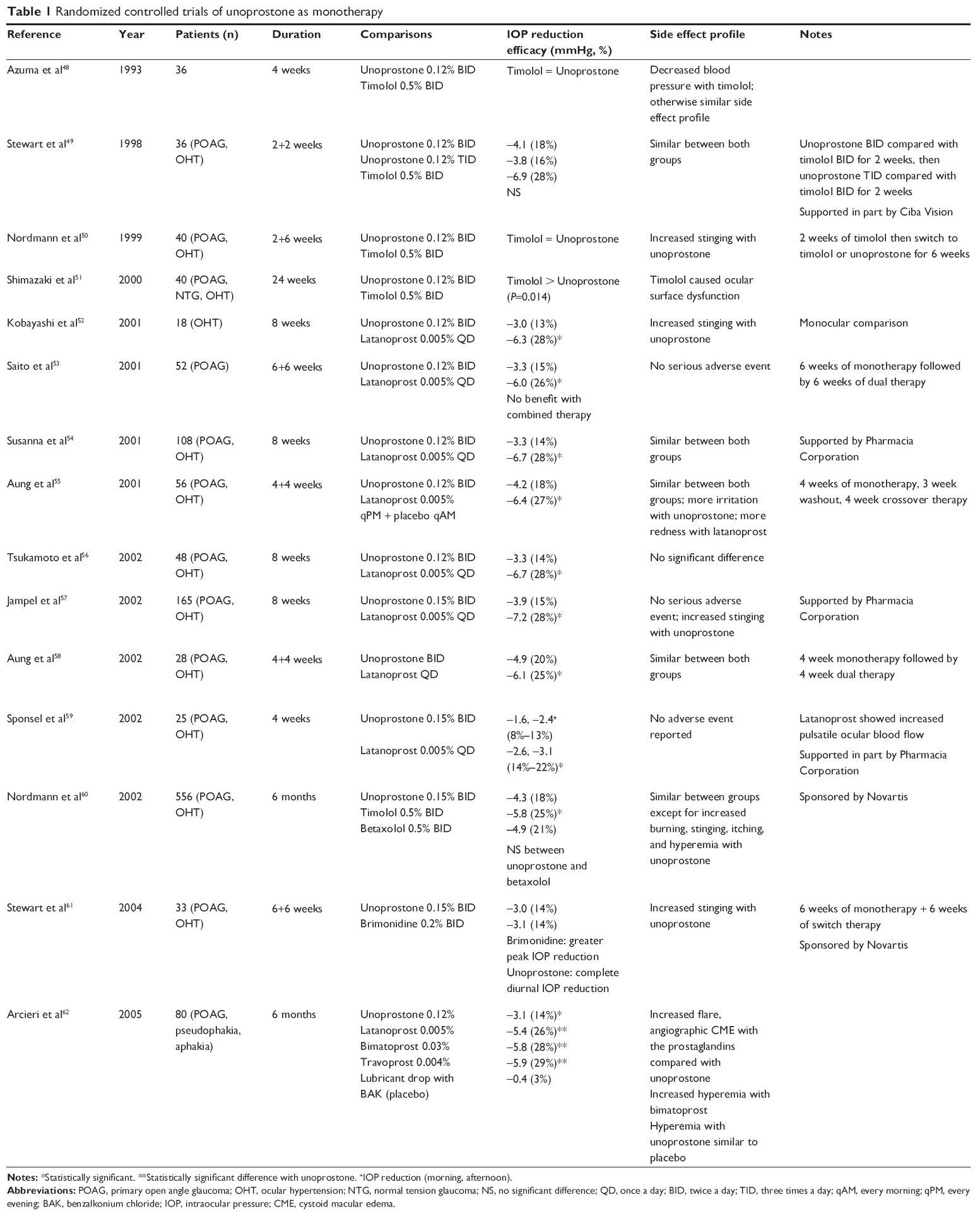 | Table 1 Randomized controlled trials of unoprostone as monotherapy |
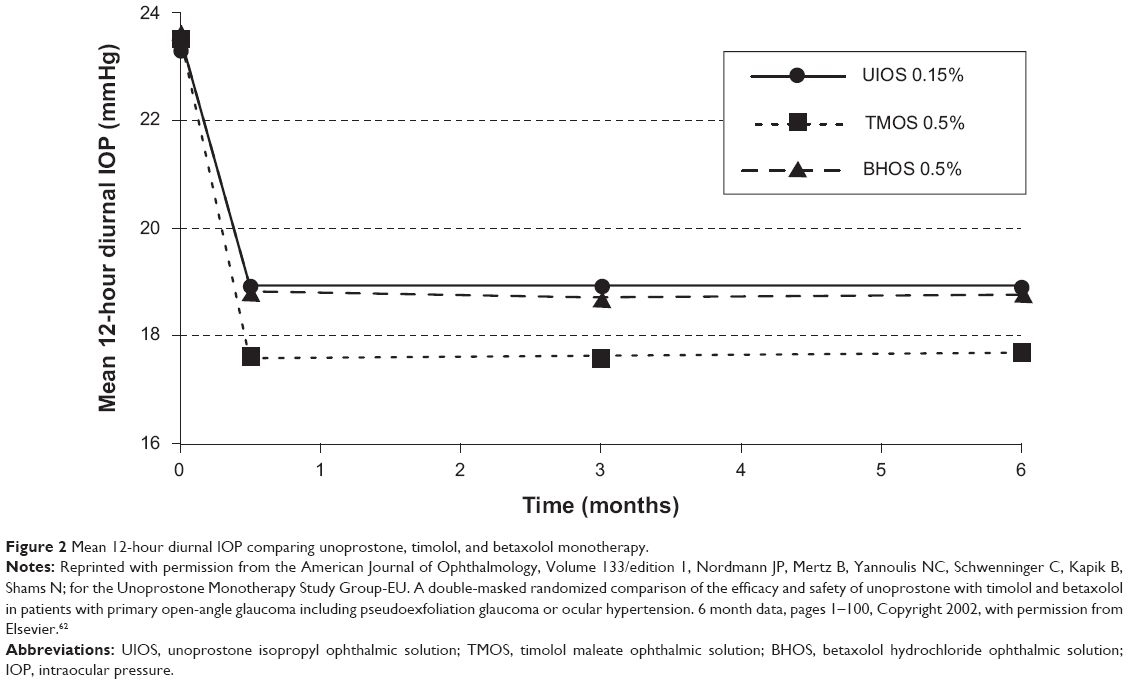 | Figure 2 Mean 12-hour diurnal IOP comparing unoprostone, timolol, and betaxolol monotherapy. |
Unoprostone as adjunctive therapy
Other studies have investigated the use of unoprostone as adjunctive therapy to timolol for the treatment of glaucoma or ocular hypertension (see Table 2).67–69 In a 12-week, multicenter, double-masked, randomized trial of 146 patients comparing unoprostone, brimonidine, and dorzolamide when added to timolol, Hommer et al found comparable efficacy in mean diurnal IOP reduction between all groups, with each adjunctive agent producing an additional drop in IOP of 2–3 mmHg from a timolol-treated baseline (see Figure 3).67 Similar results were found in two other studies comparing unoprostone, brimonidine, and dorzolamide as adjunctive therapy with timolol.68,69 A study by Saito et al involving 52 patients with primary open-angle glaucoma found no additional IOP-lowering effect when unoprostone was added to latanoprost following 12 weeks of therapy.53
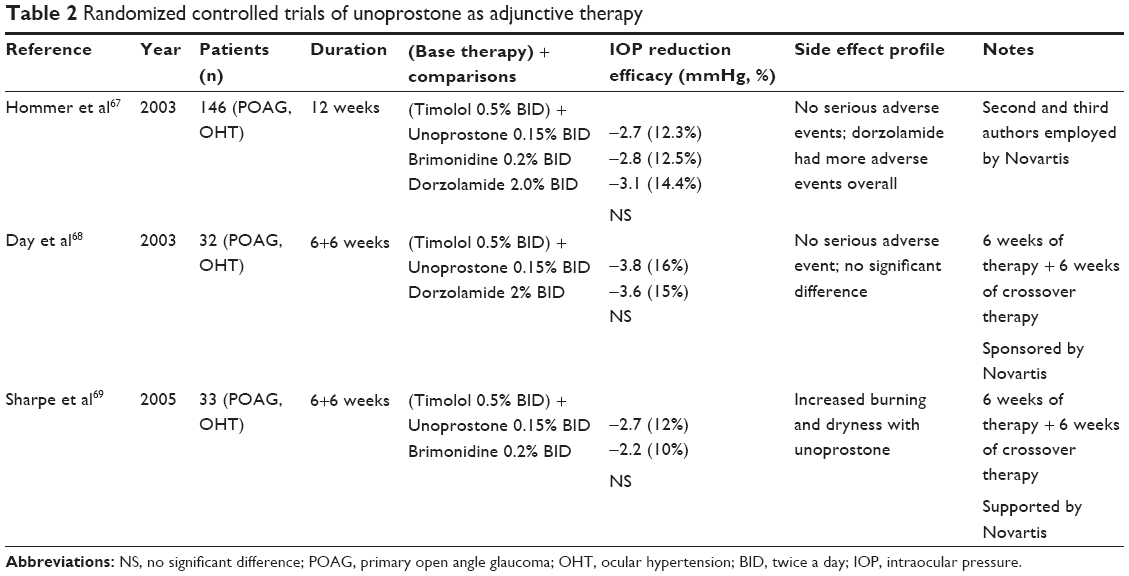 | Table 2 Randomized controlled trials of unoprostone as adjunctive therapy |
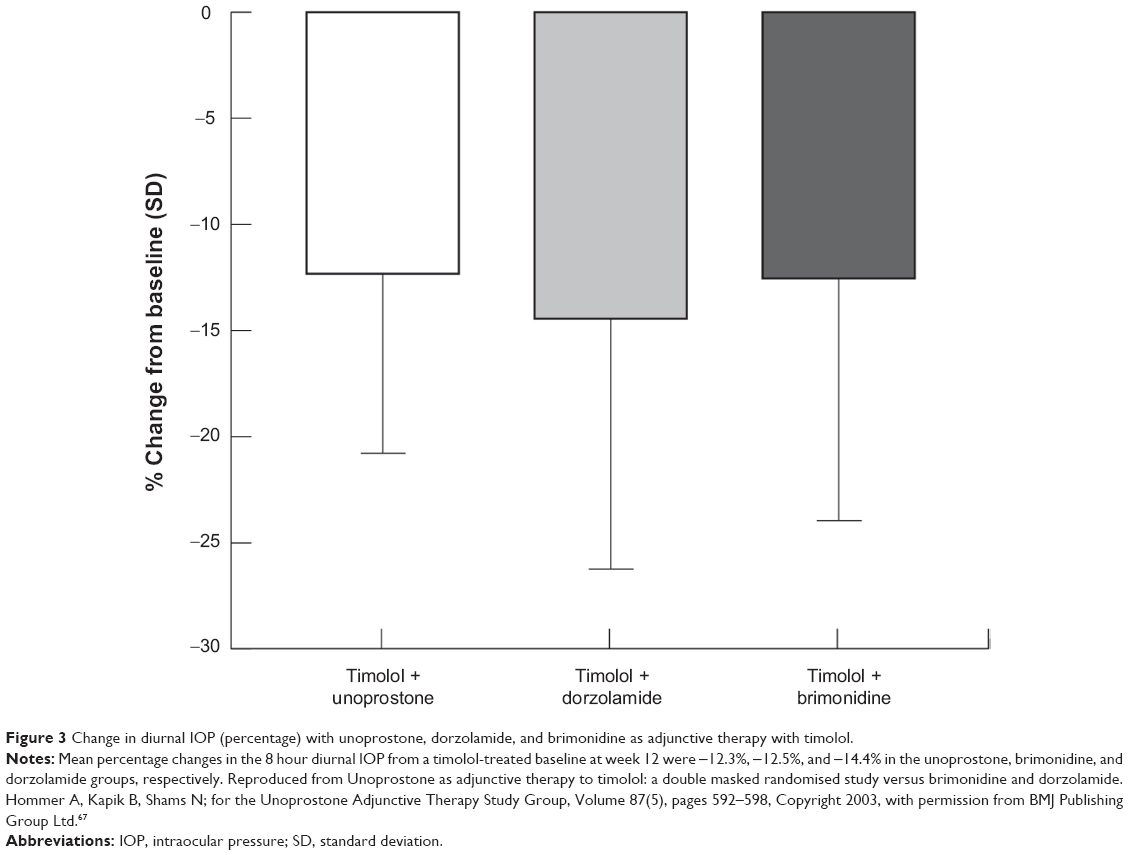 | Figure 3 Change in diurnal IOP (percentage) with unoprostone, dorzolamide, and brimonidine as adjunctive therapy with timolol. |
Safety and tolerability
The side effects of the lipid IOP-lowering agents are well described in the literature, and include conjunctival hyperemia, increased iris pigmentation, eyelash and eyelid changes, deepening of the upper eyelid sulcus, cystoid macular edema (CME), iris cysts, worsening of herpetic keratitis, and anterior uveitis.70–73 A summary of trials investigating the local and systemic safety profile of unoprostone is shown in Table 3.51,62,74–79 Many of these studies reported a favorable side effect profile of unoprostone when compared with timolol and placebo.51,74,75,77 When compared with other prostanoids, unoprostone tended to have a better ocular side effect profile.62,76,78,79
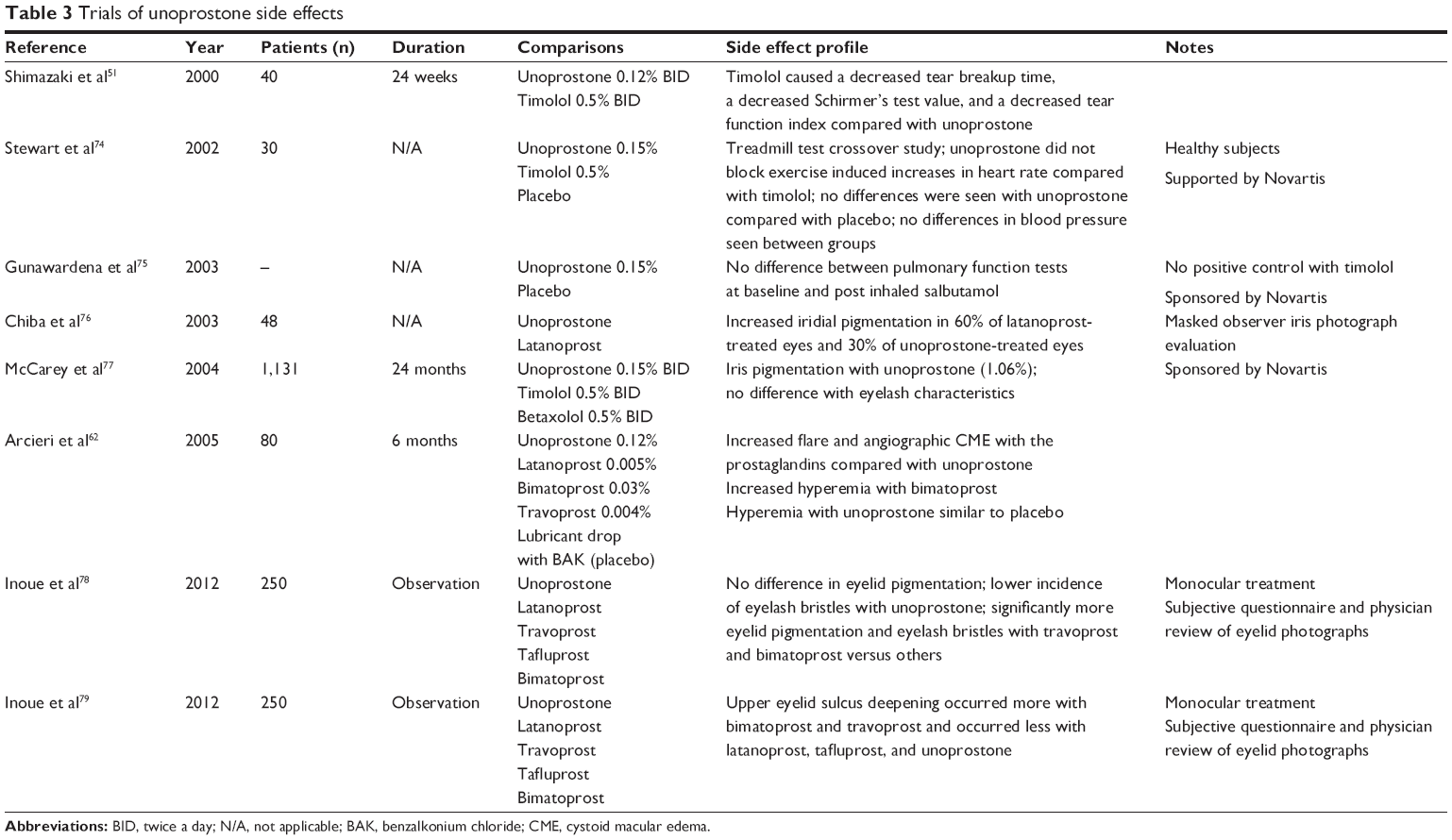 | Table 3 Trials of unoprostone side effects |
In the comparative trial of unoprostone, timolol, and betaxolol by Nordmann et al discussed in the Unoprostone as monotherapy section, adverse events were similar for the three treatment groups except for burning/stinging, burning/stinging upon drug instillation, and ocular itching, which were more common with unoprostone than with timolol but less common than with betaxolol.60 Hyperemia was also more common with unoprostone (10.8%) than with timolol (3.6%) or betaxolol (5.0%). Adverse events in this study were typically mild to moderate and transient in nature.
FP receptor activation is believed to lead to enhanced tyrosinase activity and melanogenesis in iridial melanocytes causing increased iris pigmentation.80 Mouse epidermal melanocytes were found to have enhanced tyrosinase activity with both latanoprost and unoprostone.81 A prospective study in Japan by Chiba et al compared iris pigmentation between 48 patients using either latanoprost or unoprostone as monotherapy.76 Patients included in this study all had glaucoma and were treated for over 30 months with one of the two agents. Photography was performed by the same slit-lamp camera with 45 degree illumination at 16× magnification. Photograph grading was performed by three glaucoma specialists who were masked to the patient and treatment characteristics. Only upon agreement among all three specialists was positive pigmentation documented. They found that 60% of latanoprost patients had increased iris pigmentation compared with 30% of unoprostone patients, which was statistically significant.
A multicenter, prospective, double-masked, randomized study by McCarey et al evaluated iris color and eyelash changes over 24 months in 1,131 patients randomized to twice-daily unoprostone, timolol, or betaxolol.77 Serial color photographs of the iris and eyelids were taken at baseline and over the course of the 24-month study. Photography was performed under standardized conditions, including equipment, camera settings, flash settings, slit-lamp settings, and environmental lighting. Seven views of each eye, a calibration photograph, and a patient identification photograph were used at each patient visit. Two masked, independent readers evaluated baseline and post-treatment photographs. Of the 659 patients on unoprostone, seven cases of iris color change (1.06%) were noted. There were no differences in eyelash density or length noted between the three treatment groups. The authors concluded that the incidence of iris pigmentation change was low with unoprostone and that eyelash changes were not clinically significant. The authors proposed that this may be related to the lower affinity of unoprostone for the FP receptor.
Deepening of the upper eyelid sulcus is a recently discovered ocular side effect observed with the prostanoids. Two hundred and fifty patients on various prostanoid medications were observed with eyelid photographs and subjective questionnaires.78,79 Bimatoprost and travoprost were found to have a higher incidence of deepening of the upper eyelid sulcus, eyelid pigmentation, and eyelid bristles compared with latanoprost, tafluprost, and unoprostone. Furthermore, unoprostone had a significantly lower incidence of abnormal lash growth compared with all other prostanoids.
A recent review by Arcieri et al investigated the effect of prostanoid use on the blood–aqueous barrier and on angiographic CME.62 Eighty patients with primary open angle glaucoma, pseudophakia, or aphakic glaucoma were randomized to treatment with bimatoprost (n=16), latanoprost (n=15), travoprost (n=17), unoprostone (n=16), or lubricant placebo drops (n=16) over 6 months. No patient had angiographic CME at baseline; however, four latanoprost-treated patients, one bimatoprost-treated patient, and one travoprost-treated patient developed CME on fluorescein angiography. The CME resolved in all patients with cessation of the prostanoid and use of a nonsteroidal anti-inflammatory medication. Of note, five of the six patients who developed CME had an absent or ruptured posterior capsule. No unoprostone-treated patients developed CME. The authors concluded that bimatoprost, latanoprost, and travoprost may disrupt the blood–aqueous barrier in pseudophakic or aphakic eyes and lead to the development of angiographic CME. They proposed that this may be related to higher affinity of these medications for the FP receptor compared with unoprostone.
Unoprostone is well tolerated systemically. Stewart et al compared the cardiovascular effects of unoprostone and timolol during exercise using a treadmill test in 30 healthy adults.74 Following 5 days of twice-daily dosing, timolol significantly reduced exercise-induced heart rate, while unoprostone showed no effect. In another study comparing unoprostone with placebo in patients with mild to moderate asthma, there were no changes in pulmonary function test parameters before or after administration of salbutamol.75
Conclusion
Unoprostone is a novel ocular hypotensive agent which may act, at least in part, to increase trabecular meshwork outflow, unlike the typical prostanoids which lower IOP primarily by increasing uveoscleral outflow. While it does not match the efficacy of the typical prostanoids, unoprostone does provide a modest IOP-lowering effect as monotherapy and is also an effective adjunctive agent when added to timolol. Although its mechanism of action is unclear, its relatively weak affinity for the prostaglandin FP receptor may help explain its more favorable local tolerability profile when compared with other prostanoids. Patients with ocular hypertension or early glaucoma who are intolerant of the typical prostanoids may benefit from unoprostone, either as monotherapy or adjunctive therapy, given its well tolerated side effect profile. It is also well tolerated systemically, demonstrating no effect on exercise-induced heart rate or pulmonary function. Unoprostone is a well-tolerated ocular hypotensive medication that can be considered for the treatment of glaucoma or ocular hypertension.
Disclosure
Dr Whitson is on the speaker’s bureau for Alcon, Allergan, and Sucampo. The authors have no other conflicts of interest in this work.
References
Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–267. | ||
Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82:844–851. | ||
Drance S, Anderson DR, Schulzer M; for the Collaborative Normal-Tension Glaucoma Study Group. Risk factors for progression of visual field abnormalities in normal-tension glaucoma. Am J Ophthalmol. 2001;131:699–708. | ||
Gordon MO, Beiser JA, Brandt JD, et al; for the Ocular Hypertension Treatment Study Group. The ocular hypertension treatment study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:714–720. | ||
The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130:429–440. | ||
Heijl A, Leske C, Bengtsson B, Hyman L, Bengtsson B, Hussein M; for the Early Manifest Glaucoma Trial Group. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120:1268–1279. | ||
Kass MA, Heuer DK, Higginbotham EJ, et al; for the Ocular Hypertension Treatment Study Group. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:701–713. | ||
Harms NV, Toris CB. Current status of unoprostone for the management of glaucoma and the future of its use in the treatment of retinal disease. Expert Opin Pharmacother. 2013;14:105–113. | ||
Rescula (unoprostone isopropyl ophthalmic solution) 0.15% package insert. Bethesda, MD, USA: Sucampo Pharma; November 2012. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/021214s006s007lbl.pdf. Accessed December 15, 2013. | ||
Bhattacherjee P, Paterson CA, Percicot C. Studies on receptor binding and signal transduction pathways of unoprostone ispropyl. J Ocul Pharmacol Ther. 2001;17:433–441. | ||
German OL, Insua MF, Gentili C, et al. Docosahexaenoic acid prevents apoptosis of retina photoreceptors by activating the ERK/MAPK pathway. J Neurochem. 2006;98:1507–1520. | ||
Rotstein NP, Politi LE, German OL, Girotti R. Protective effect of docosahexaenoic acid on oxidative stress-induced apoptosis of retina photoreceptors. Invest Ophthalmol Vis Sci. 2003;44:2252–2259. | ||
Tsuruma K, Tanaka Y, Shimazawa M, Mashima Y, Hara H. Unoprostone reduces oxidative stress- and light-induced retinal cell death, and phagocytotic dysfunction, by activating BK channels. Mol Vis. 2011;17:3556–3565. | ||
Kashiwagi K, Iizuka Y, Tsukahara S. Metabolites of isopropyl unoprostone as potential ophthalmic solutions to reduce intraocular pressure in pigmented rabbits. Jpn J Pharmacol. 1999;81:56–62. | ||
Takase M, Murao M, Koyano S, Okita M, Ueno R. [Ocular effects of topical instillation of UF-021 ophthalmic solution in healthy volunteers]. Nihon Ganka Gakkai Zasshi. 1992;96:1261–1267. Japanese. | ||
Alm A, Nilsson SF. Uveoscleral outflow – a review. Exp Eye Res. 2009;88:760–768. | ||
Sharif NA, Kelly CR, Crider JY. Human trabecular meshwork cell responses induced by bimatoprost, travoprost, unoprostone, and other FP prostaglandin receptor agonist analogues. Invest Ophthalmol Vis Sci. 2003;44:715–721. | ||
Ota T, Aihara M, Narumiya S, Araie M. The effects of prostaglandin analogues on IOP in prostanoid FP-receptor-deficient mice. Invest Ophthalmol Vis Sci. 2005;46:4159–4163. | ||
Gabelt BT, Kaufman PL. Prostaglandin F2 alpha increases uveoscleral outflow in the cynomolgus monkey. Exp Eye Res. 1989;49:389–402. | ||
Poyer JF, Millar C, Kaufman PL. Prostaglandin F2 alpha effects on isolated rhesus monkey ciliary muscle. Invest Ophthalmol Vis Sci. 1995;36:2461–2465. | ||
Crawford K, Kaufman PL. Pilocarpine antagonizes prostaglandin F2 alpha-induced ocular hypotension in monkeys. Evidence for enhancement of uveoscleral outflow by prostaglandin F2 alpha. Arch Ophthalmol. 1987;105:1112–1116. | ||
Lim KS, Nau CB, O’Byrne MM, et al. Mechanism of action of bimatoprost, latanoprost, and travoprost in healthy subjects: a crossover study. Ophthalmology. 2008;115:790–795. | ||
Kashiwagi K, Jin M, Suzuki M, Tanaka Y, Iizuka Y, Tsukahara S. Isopropyl unoprostone increases the activities of matrix matalloproteinases in cultured monkey ciliary muscle cells. J Glaucoma. 2001;10:271–276. | ||
Lindsey JD, Kashiwagi K, Boyle D, Kashiwagi F, Firestein GS, Weinreb RN. Prostaglandins increase proMMP-1 and proMMP-3 secretion by human ciliary smooth muscle cells. Curr Eye Res. 1996;15:869–875. | ||
Lindsey JD, To HD, Weinreb RN. Induction of c-fos by prostaglandin F2 alpha in human ciliary smooth muscle cells. Invest Ophthalmol Vis Sci. 1994;35:242–250. | ||
Ooi YH, Oh DJ, Rhee DJ. Effect of bimatoprost, latanoprost, and unoprostone on matrix metalloproteinases and their inhibitors in human ciliary body smooth muscle cells. Invest Ophthalmol Vis Sci. 2009;50:5259–5265. | ||
Toris CB, Zhan G, Camras CB. Increase in outflow facility with unoprostone treatment in ocular hypertensive patients. Arch Ophthalmol. 2004;122:1782–1787. | ||
Cuppoletti J, Malinowska DH, Tewari KP, Chakrabarti J, Ueno R. Unoprostone isopropyl and metabolite M1 activate BK channels and prevent ET-1-induced [Ca2+]i increases in human trabecular meshwork and smooth muscle. Invest Ophthalmol Vis Sci. 2012;53:5178–5189. | ||
Cuppoletti J, Malinowska DH, Tewari KP, Chakrabarti J, Ueno R. Cellular and molecular effects of unoprostone as a BK channel activator. Biochim Biophys Acta. 2007;1768:1083–1092. | ||
Thieme H, Stumpff F, Ottlecz A, Percicot CL, Lambrou GN, Wiederholt M. Mechanisms of action of unoprostone on trabecular meshwork contractility. Invest Ophthalmol Vis Sci. 2001;42:3193–3201. | ||
Thieme H, Steinhausen K, Ottlecz A, et al. Effects of unoprostone and endothelin 1 on L-type channel currents in human trabecular meshwork cells. Ophthalmic Res. 2005;37:293–300. | ||
Yu DY, Su EN, Cringle SJ, Schoch C, Percicot CP, Lambrou GN. Comparison of the vasoactive effects of the docosanoid unoprostone and selected prostanoids on isolated perfused retinal arterioles. Invest Ophthalmol Vis Sci. 2001;42:1499–1504. | ||
Tamaki Y, Araie M, Tomita K, Nagahara M, Sandoh S, Tomidokoro A. Effect of topical unoprostone on circulation of human optic nerve head and retina. J Ocul Pharmacol Ther. 2001;17:517–527. | ||
Makimoto Y, Sugiyama T, Kojima S, Azuma I. Long-term effect of topically applied isopropyl unoprostone on microcirculation in the human ocular fundus. Jpn J Ophthalmol. 2002;46:31–35. | ||
Polska E, Doelemeyer A, Luksch A, et al. Partial antagonism of endothelin 1-induced vasoconstriction in the human choroid by topical unoprostone isopropyl. Arch Ophthalmol. 2002;120:348–352. | ||
Yoshitomi T, Yamaji K, Ishikawa H, Ohnishi Y. Vasodilatory mechanism of unoprostone isopropyl on isolated rabbit ciliary artery. Curr Eye Res. 2004;28:167–174. | ||
Kimura I, Shinoda K, Tanino T, Ohtake Y, Mashima Y. Effect of topical unoprostone isopropyl on optic nerve head circulation in controls and in normal-tension glaucoma patients. Jpn J Ophthalmol. 2005;49:287–293. | ||
Munemasa Y, Kitaoka Y, Hayashi Y, et al. Effects of unoprostone on phosphorylated extracellular signal-regulated kinase expression in endothelin-1-induced retinal and optic nerve damage. Vis Neurosci. 2008;25:197–208. | ||
Sugiyama T, Mashima Y, Yoshioka Y, Oku H, Ikeda T. Effect of unoprostone on topographic and blood flow changes in the ischemic optic nerve head of rabbits. Arch Ophthalmol. 2009;127:454–459. | ||
Mukuno H, Nakamura M, Kanamori A, Nagai A, Negi A, Seigel G. Unoprostone isopropyl rescues retinal progenitor cells from apoptosis in vitro. Curr Eye Res. 2004;29:457–464. | ||
Ohashi M, Mayama C, Ishi K, Araie M. Local effect of topical FP-receptor agonists on retinal vessels of the ipsilateral posterior retina in normal rabbit eyes. Clin Experiment Ophthalmol. 2008;36:767–774. | ||
Tawada A, Sugawara T, Ogata K, Hagiwara A, Yamamoto S. Improvement of central retinal sensitivity six months after topical isopropyl unoprostone in patients with retinitis pigmentosa. Indian J Ophthalmol. 2013;61:95–99. | ||
Sakurai M, Araie M, Oshika T, et al. Effects of topical application of UF-021, a novel prostaglandin derivative, on aqueous humor dynamics in normal human eyes. Jpn J Ophthalmol. 1991;35:156–165. | ||
Ueno R, Yoshida S, Deguchi T, et al. [The intraocular pressure lowering effects of UF-021, a novel prostaglandin related compound, in animals]. Nihon Ganka Gakkai Zasshi. 1992;96:462–468. Japanese. | ||
Tetsuka H, Tsuchisaka H, Kin K, Takahashi Y, Takase M. [A mechanism for reducing intraocular pressure in normal volunteers using UF-021, a prostaglandin-related compound]. Nihon Ganka Gakkai Zasshi. 1992;96:496–500. Japanese. | ||
Inoue K, Noguchi K, Wakakura M, Tomita G. Effects of unoprostone on diurnal variation of intraocular pressure in healthy volunteers. Clin Ophthalmol. 2011;5:1003–1005. | ||
Camras CB, Alm A. Initial clinical studies with prostaglandins and their analogues. Surv Ophthalmol. 1997;41 Suppl 2:S61–S68. | ||
Azuma I, Masuda K, Kitazawa Y, Takase M, Yamamura H. Double-masked comparative study of UF-021 and timolol ophthalmic solutions in patients with primary open-angle glaucoma or ocular hypertension. Jpn J Ophthalmol. 1993;37:514–525. | ||
Stewart WC, Stewart JA, Kapik BM. The effects of unoprostone isopropyl 0.12% and timolol maleate 0.5% on diurnal intraocular pressure. J Glaucoma. 1998;7:388–394. | ||
Nordmann JP, Rouland JF, Mertz BP. A comparison of the intraocular pressure-lowering effect of 0.5% timolol maleate and the docosanoid derivative of a PGF2 alpha metabolite, 0.12% unoprostone, in subjects with chronic open-angle glaucoma or ocular hypertension. Curr Med Res Opin. 1999;15:87–93. | ||
Shimazaki J, Hanada K, Yagi Y, et al. Changes in ocular surface caused by antiglaucomatous eyedrops: prospective, randomized study for the comparison of 0.5% timolol v 0.12% unoprostone. Br J Ophthalmol. 2000;84:1250–1254. | ||
Kobayashi H, Kobayashi K, Okinami S. A comparison of intraocular pressure-lowering effect of prostaglandin F2-alpha analogues, latanoprost, and unoprostone isopropyl. J Glaucoma. 2001;10:487–492. | ||
Saito M, Takano R, Shirato S. Effects of latanoprost and unoprostone when used alone or in combination for open-angle glaucoma. Am J Ophthalmol. 2001;132:485–490. | ||
Susanna R Jr, Giampani J Jr, Borges AS, Vessani RM, Jordao ML. A double-masked, randomized clinical trial comparing latanoprost with unoprostone in patients with open-angle glaucoma or ocular hypertension. Ophthalmology. 2001;108:259–263. | ||
Aung T, Chew PT, Yip CC, et al. A randomized double-masked crossover study comparing latanoprost 0.005% with unoprostone 0.12% in patients with primary open-angle glaucoma and ocular hypertension. Am J Ophthalmol. 2001;131:636–642. | ||
Tsukamoto H, Mishima HK, Kitazawa Y, Araie M, Abe H, Negi A; for the Glaucoma Study Group. A comparative clinical study of latanoprost and isopropyl unoprostone in Japanese patients with primary open-angle glaucoma and ocular hypertension. J Glaucoma. 2002;11:497–501. | ||
Jampel HD, Bacharach J, Sheu WP, Wohl LG, Solish AM, Christie W; for the Latanoprost/Unoprostone Study Group. Randomized clinical trial of latanoprost and unoprostone in patients with elevated intraocular pressure. Am J Ophthalmol. 2002;134:863–871. | ||
Aung T, Chew PT, Oen FT, et al. Additive effect of unoprostone and latanoprost in patients with elevated intraocular pressure. Br J Ophthalmol. 2002;86:75–79. | ||
Sponsel WE, Paris G, Trigo Y, Pena M. Comparative effects of latanoprost (Xalatan) and unoprostone (Rescula) in patients with open-angle glaucoma and suspected glaucoma. Am J Ophthalmol. 2002;134:552–559. | ||
Nordmann JP, Mertz B, Yannoulis NC, Schwenninger C, Kapik B, Shams N; for the Unoprostone Monotherapy Study Group-EU. A double-masked randomized comparison of the efficacy and safety of unoprostone with timolol and betaxolol in patients with primary open-angle glaucoma including pseudoexfoliation glaucoma or ocular hypertension. 6 month data. Am J Ophthalmol. 2002;133:1–10. | ||
Stewart WC, Stewart JA, Day DG, Jenkins J. The safety and efficacy of unoprostone 0.15% versus brimonidine 0.2%. Acta Ophthalmol Scand. 2004;82:161–165. | ||
Arcieri ES, Santana A, Rocha FN, Guapo GL, Costa VP. Blood-aqueous barrier changes after the use of prostaglandin analogues in patients with pseudophakia and aphakia: a 6-month randomized trial. Arch Ophthalmol. 2005;123:186–192. | ||
[No authors listed]. Intraocular pressure-lowering efficacy of latanoprost in patients with normal-tension glaucoma or primary open-angle glaucoma. J Ocul Pharmacol Ther. 2001;17:19–25. | ||
Otori Y, Tokugawa H, Morimura H, et al. [The effect of substituting latanoprost 0.005% for unoprostone 0.12%]. Nihon Ganka Gakkai Zasshi. 2004;108:207–212. Japanese. | ||
Takahashi I, Tanaka M. Switching to latanoprost monotherapy for 24 weeks in glaucoma patients. Eur J Ophthalmol. 2004;14:401–406. | ||
Enoki M, Saito J, Hara M, Uchida T, Sagara T, Nishida T. Additional reduction in intraocular pressure achieved with latanoprost in normal-tension glaucoma patients previously treated with unoprostone. Jpn J Ophthalmol. 2006;5:334–337. | ||
Hommer A, Kapik B, Shams N; for the Unoprostone Adjunctive Therapy Study Group. Unoprostone as adjunctive therapy to timolol: a double masked randomised study versus brimonidine and dorzolamide. Br J Ophthalmol. 2003;87:592–598. | ||
Day DG, Schacknow PN, Wand M, et al. Timolol 0.5%/dorzolamide 2% fixed combination vs timolol maleate 0.5% and unoprostone 0.15% given twice daily to patients with primary open-angle glaucoma or ocular hypertension. Am J Ophthalmol. 2003;135:138–143. | ||
Sharpe ED, Henry CJ, Mundorf TK, et al. Brimonidine 0.2% vs unoprostone 0.15% both added to timolol maleate 0.5% given twice daily to patients with primary open-angle glaucoma or ocular hypertension. Eye (Lond). 2005;19:35–40. | ||
Alm A, Grierson I, Shields MB. Side effects associated with prostaglandin analog therapy. Surv Ophthalmol. 2008;53 Suppl:S93–S105. | ||
Yamamoto T, Kitazawa Y. Iris-color change developed after topical isopropyl unoprostone treatment. J Glaucoma. 1997;6:430–432. | ||
Kaufman HE, Varnell ED, Toshida H, Kanai A, Thompson HW, Bazan NG. Effects of topical unoprostone and latanoprost on acute and recurrent herpetic keratitis in the rabbit. Am J Ophthalmol. 2001;131:643–646. | ||
Wand M, Gaudio AR. Cystoid macular edema associated with ocular hypotensive lipids. Am J Ophthalmol. 2002;133:403–405. | ||
Stewart WC, Stewart JA, Crockett S, Kubilus C, Brown A, Shams N. Comparison of the cardiovascular effects of unoprostone 0.15%, timolol 0.5% and placebo in healthy adults during exercise using a treadmill test. Acta Ophthalmol Scand. 2002;80:272–276. | ||
Gunawardena KA, Crame N, Mertz B, Shams N. Safety of unoprostone isopropyl 0.15% ophthalmic solution in patients with mild to moderate asthma. Ophthalmologica. 2003;217:129–136. | ||
Chiba T, Kashiwagi K, Chiba N, et al. Comparison of iridial pigmentation between latanoprost and isopropyl unoprostone: a long term prospective comparative study. Br J Ophthalmol. 2003;87:956–959. | ||
McCarey BE, Kapik BM, Kane FE; for the Unoprostone Monotherapy Study Group. Low incidence of iris pigmentation and eyelash changes in 2 randomized clinical trials with unoprostone isopropyl 0.15%. Ophthalmology. 2004;111:1480–1488. | ||
Inoue K, Shiokawa M, Higa R, et al. Adverse periocular reactions to five types of prostaglandin analogs. Eye (Lond). 2012;26:1465–1472. | ||
Inoue K, Shiokawa M, Wakakura M, Tomita G. Deepening of the upper eyelid sulcus caused by 5 types of prostaglandin analogs. J Glaucoma. 2013;22:626–631. | ||
Stjernschantz JW, Albert DM, Hu DN, Drago F, Wistrand PJ. Mechanism and clinical significance of prostaglandin-induced iris pigmentation. Surv Ophthalmol. 2002;47 Suppl:S162–S175. | ||
Kashiwagi K, Tsukamoto K, Suzuki M, Tsukahara S. Effects of isopropyl unoprostone and latanoprost on melanogenesis in mouse epidermal melanocytes. J Glaucoma. 2002;11:57–64. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.