Back to Journals » Drug, Healthcare and Patient Safety » Volume 14
An Atypical Case of Extreme Polypharmacy
Authors Veronin MA
Received 11 August 2021
Accepted for publication 25 January 2022
Published 10 March 2022 Volume 2022:14 Pages 19—26
DOI https://doi.org/10.2147/DHPS.S332954
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajender Aparasu
Michael A Veronin
Social and Administrative Sciences, Department of Pharmaceutical Sciences and Health Outcomes, The University of Texas at Tyler, Ben and Maytee Fisch College of Pharmacy, Tyler, TX, 75799, USA
Correspondence: Michael A Veronin, Social and Administrative Sciences, Department of Pharmaceutical Sciences and Health Outcomes, The University of Texas at Tyler, Ben and Maytee Fisch College of Pharmacy, 3900 University Blvd., Tyler, TX, 75799, USA, Tel +1 903 566 6148, Fax +1 903 565 5598, Email [email protected]
Abstract: A commonly reported definition of polypharmacy is the numerical definition of 5 or more medications daily, and definitions have ranged from 2 or more to 11 or more medications. In this case report, an extreme case of polypharmacy is presented, highlighted by the inordinate number of drugs used over time throughout the patient’s care. A 48-year-old African American female with multiple comorbidities experienced a serious adverse drug event (ADE) prompting reporting to MedWatch, the US Food and Drug Administration’s adverse drug event reporting system. The patient’s concomitant medications included 146 drug entities, across 82 therapeutic drug categories. It is apparent that the greatest influence on the occurrence of polypharmacy was the presence of multiple comorbidities, and treatment centered around addressing each morbidity with drug therapy. This case illustrates the insidious nature of polypharmacy and raises questions as to the appropriate progression and limits on the use of multiple medications.
Keywords: polypharmacy, adverse drug event, comorbidity, multiple medications, food and drug administration, MedWatch
Introduction
Polypharmacy has been described as “one of the greatest prescribing challenges in general practice”.1 Several harmful consequences have been identified related to polypharmacy, which include, but are not limited to, greater health care costs, an increased risk of adverse drug events (ADEs), drug interactions, medication non-adherence, and reduced functional capacity.2 Aside from being a major problem in clinical practice, just identifying a uniform definition of polypharmacy has been challenging. In one report, a total of 138 definitions of polypharmacy and associated terms were obtained”.3 A commonly reported definition of polypharmacy is the numerical definition of 5 or more medications daily,4 and definitions have ranged from 2 or more to 11 or more medications.3
As well as the lack of congruence for the definition of polypharmacy, reporting on the prevalence of polypharmacy exists to varying degrees of consistency.
Quinna and Shah report that concomitant use of multiple prescription drugs is increasingly common, with 10% of the population and 30% of older adults in the US taking five or more drugs simultaneously.5
According to the Slone Epidemiology Center in Boston, MA (2006), in a given week, an average of 82% of adults in the US are taking at least one medication (prescription or nonprescription drug, vitamin/mineral, herbal/natural supplement), and 29% are taking five or more.6
As recently as August 2019, Hales et al reported that nearly 7 in 10 adults aged 40–79 used at least 1 prescription drug in the past 30 days in the US (69.0%) and Canada (65.5%), and approximately 1 in 5 used at least 5 prescription drugs (22.4% in the US and 18.8% in Canada).7
The occurrence of polypharmacy is more pronounced in older adults. Woodruff reports that 44% of men and 57% of women older than age 65 take five or more medications per week; about 12% of both men and women take 10 or more medications per week. These agents include both prescription and over-the-counter (OTC) preparations, such as vitamin and mineral supplements and herbal products.8 This coincides with a recent account by Nguyen et al who report an average rate of 40% to 50% in this population.9
In this case report, an atypical case of extreme polypharmacy is presented, highlighted by the inordinate number of drugs used over time throughout the patient’s care. The source of information for the case is MedWatch, the US Food and Drug Administration’s adverse drug event reporting system.10 The FDA Adverse Event Reporting System (FAERS) database includes the MedWatch narratives submitted by healthcare providers and patients with identifying details removed. Using the Freedom of Information Act (FOIA), a copy of the individual case report was obtained from the FDA, which includes a narrative where reporters describe the clinical (adverse) event in their own words.11 The polypharmacy in this case raises questions as to the appropriate use of drugs in patients with multiple comorbidities.
Case Report
A 48-year-old African American female with multiple comorbidities experienced a serious adverse drug event (ADE) prompting reporting to MedWatch. Possible nephrogenic systemic fibrosis (NSF) was observed in the patient after receiving contrast media. According to clinical notes, on eight different occasions from 1991 to 2008, the patient received Omniscan® (gadodiamide) for the indication of “fullness in the right neck”, a gadolinium agent (type not specified) for the indication of left breast mass and liver cancer, and Magnevist® (gadopentetate dimeglumine) for the indications of headache to rule out central nervous system Lupus, questionable stroke, and spasmatic weakness. On March 25, 2014, The FDA received an ADE report by clinicians through the FDA’s MedWatch surveillance reporting system. At the time the report was submitted, the patient’s history and medical condition were noted.
Relevant past medical history with year of occurrence included: end stage renal disease (ESRD) (1984, 1999), lupus nephritis (1984), first cadaveric kidney transplant (unspecified date), removal of first renal transplant (unspecified date), myocardial infarction (unspecified date), Lupus cerebritis (1999), bilateral femoral chondromalacia patellae (2000), partial parathyroidectomy (unspecified date), atrial fibrillation, second cadaveric renal transplant (unspecified date), chronic allograft nephropathy (2007), third renal transplant evaluation (unspecified date), transplant failure of second transplant (2008), and nontoxic multinodular goiter (2010).
At the time of the report, concurrent medical conditions with year of occurrence included uncontrolled hypertension, systemic lupus erythematosus with End-Stage Renal Disease (ESRD) (1984), various stages of chronic kidney disease (1998) peritoneal dialysis, hepatitis C (1995), seizures (1999), diabetes mellitus induced by Dapsone (diamino-diphenyl sulfone) (2002), overactive parathyroid (2003), nerve damage, poor circulation, rotator cuff disease in both shoulders, osteoporosis (both wrists and spine), arthritis (both wrist and spine), gout, human papilloma virus (HPV), peritoneal dialysis (1998 to 2002 and Jun 2008 onwards), cytomegalovirus (CMV), Hepatitis B, secondary hyperparathyroidism, sensory polyneuropathy axonal and Raynaud’s disease.
Concomitant medications included 146 drug entities, across 82 therapeutic drug categories. The medications listed included 8 duplicate entries, identified separately by brand and generic name. Dosage forms included oral, injectable, topical, nasal, ophthalmic, and intraocular drug products. In addition, the patient had been taking vitamins, minerals, and nutritional supplements. The information is presented in Table 1.
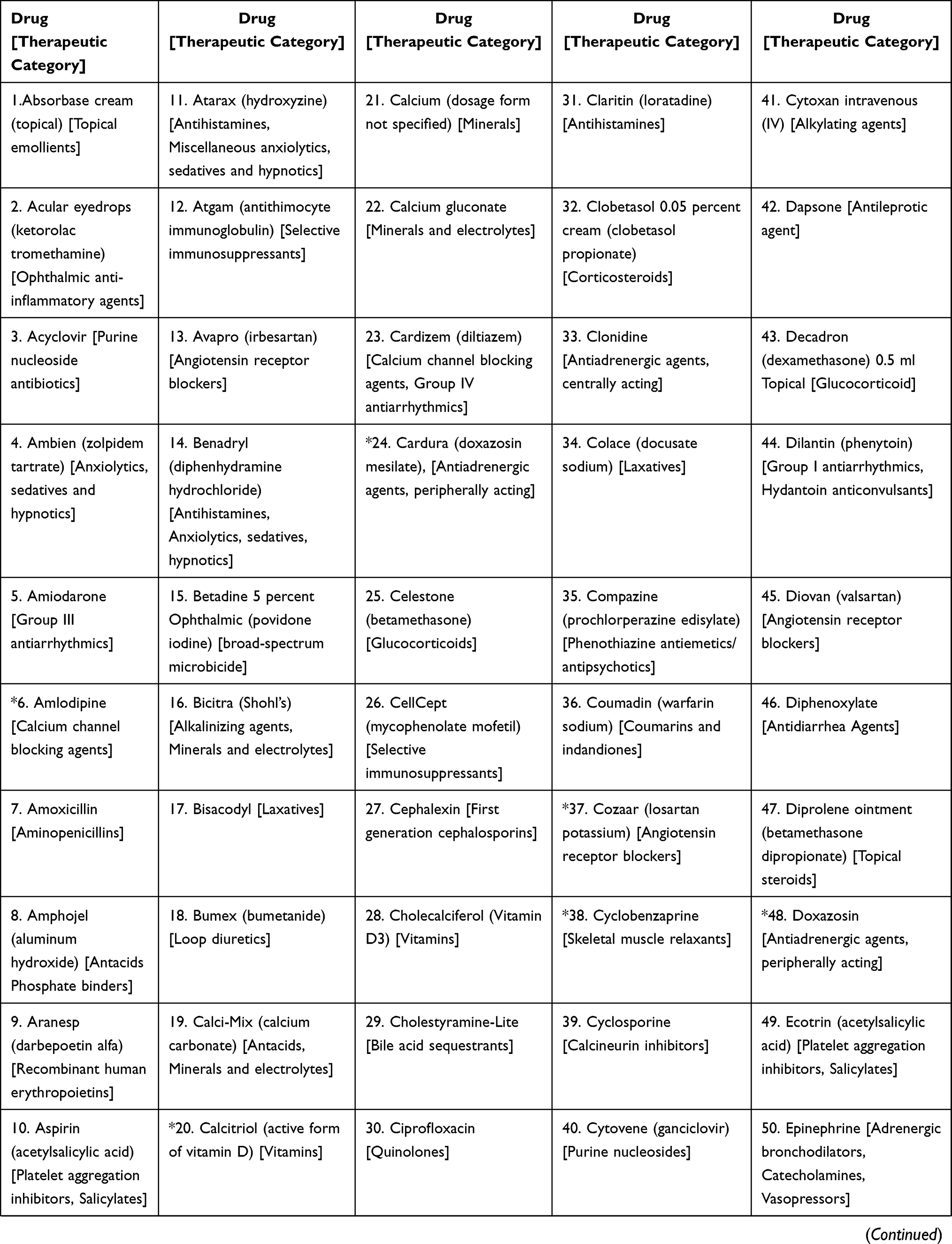 | 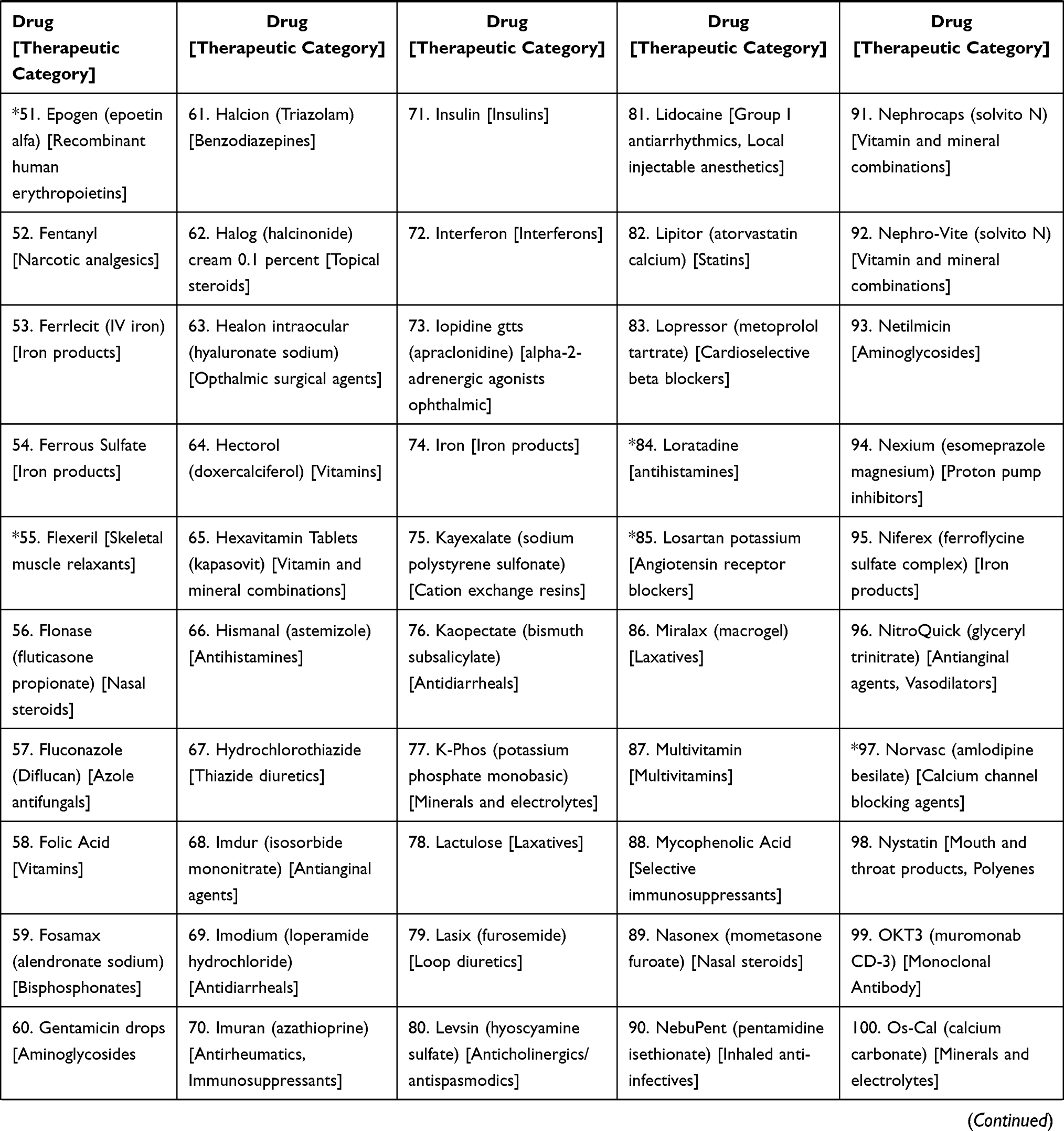 | 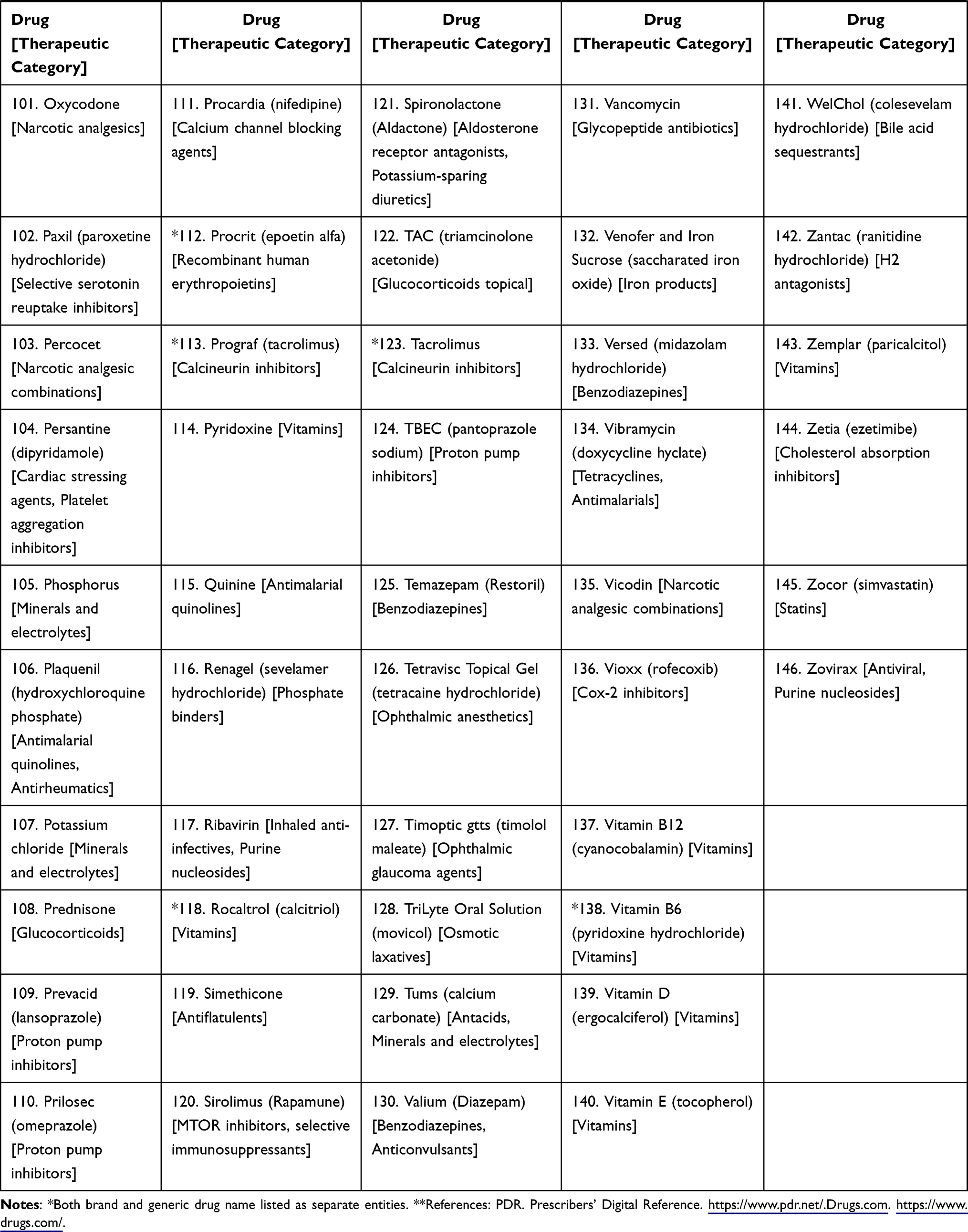 |
Table 1 Atypical Case of Extreme Polypharmacy: Concomitant Medications (Drug* and Therapeutic Category**) |
Discussion
This case illustrates the insidious nature of polypharmacy and raises questions as to the appropriate progression and limits on the use of multiple medications. In the context of patients afflicted by polypharmacy, the case described may be extreme, and perhaps even viewed as an outlier. Yet, the case illustrates several important issues that healthcare practitioners should consider when caring for patients on drug therapy for multiple health conditions.
The US Food and Drug Administration (FDA) maintains one of the largest government databases in the country, known as the FDA Adverse Event Reporting System, or FAERS. It is comprised of drug safety reports that have been submitted to the FDA through the “MedWatch” reporting program.12 Reports can be submitted to the FDA by consumers, health care providers, and drug manufacturers. A copy of an individual case report can be obtained from the FDA, which includes a narrative where reporters describe the adverse event in their own words based on observations.13 The original MedWatch report of this case is provided as Supplemental Online Material.
The focus of this case report is on polypharmacy specifically as it relates to the large quantity of prescription drugs used by an individual patient in their treatment. In the report, it is difficult to discern the presence of inappropriate use of medication(s), or use of medications without a clinical indication, which also have been used to define polypharmacy.4
Other similar cases on high numbers of prescribed drugs considered to be extreme have appeared in the medical literature.
Agarwal and Agarwal (2013) report an extreme case of polypharmacy in a patient with schizophrenia.14 A 67-year-old female patient was taking 32 different medications for various comorbid conditions. The patient’s drug regimen included 38 to 41 pills per day, oral liquid medication 2 to 5 per day and applying two lotions for a total of 4 times per day. The authors conclude that all of the medications appeared to be clinically warranted, although “runaway” polypharmacy can result from a patient’s comorbid conditions and seeing different specialists.
Nechba et al describe the case of an 85-year-old female who had been taking the 6 different drugs for an extended period of time: amlodipine, valsartan, hydrochlorothiazide, lysine acetylsalicylate, simvastatin, and trimetazidine.15 At a later time, she presented thoracic pain and received 3 more drugs: propranolol, tramadol, and paracetamol. One week later, she developed a diffuse skin lesion, which was treated with an oral corticosteroid. The authors conclude that consequences of polypharmacy can be serious, and as highlighted in this case, elderly patients with multiple comorbidities are at risk of experiencing adverse drug events, and perhaps iatrogeny.
In a case series study on patients seen in outpatient clinical practice, Finkelstein et al describe the case of a 74-year-old Dominican woman with a history of hypertension, diabetes, hyperlipidemia, diastolic heart failure, and asthma for 30 years on 26 different medications.16 The patient underwent pharmacogenetic (PGx) testing by a treating physician in order to optimize her therapy. The decision to change or eliminate potentially inappropriate medications in this patient was complicated by the complex interaction of polypharmacy and lack of clear evidence-based guidelines for optimal drug changes under such conditions.
Gareri et al report the case of an 81-year-old man with a clinical history of diabetes, blood hypertension, non-valvular atrial fibrillation, chronic obstructive pulmonary disease, osteoarthritis, anxiety, and depression.17 The patient was taking 11 different drugs daily. The authors conclude that prudent deprescribing in older adults is needed and avoiding potentially inappropriate drugs. The authors assert that drug-induced symptoms are the second most frequent medical problem that the geriatrician encounters, and collaboration with a pharmacologist can help to optimize pharmacotherapy by deprescribing inappropriate agents.
Similar cases of patients with multiple comorbidities on multiple medication regimens ranging from 11 to 28 different drugs can be found in the medical literature.9,18,19 In terms of sheer numbers, the case described here appears to exceed all others for excessive medication use.
Determinants of Polypharmacy
Polypharmacy is a multifaceted healthcare issue, and as illustrated in this case, several risk factors exist increasing a patient’s susceptibility to polypharmacy. Determinants of polypharmacy include patient-related factors such as having multiple medical conditions or comorbidities, in particular, chronic mental health conditions.20
Polypharmacy is more likely to take place in the elderly, particularly for individuals residing in a long-term care facility, although it has been observed to occur in younger, at-risk populations predisposed to medical conditions.20 With increasing numbers of older adults in the population, the prevalence of chronic medical conditions is also increasing. And an ageing population with increasing frailty often necessitates the use of multiple medications.21
Determinants of polypharmacy may also include medical conditions may be managed by multiple providers with different specialties and subspecialties who may prescribe similar medications.22
Healthcare systems where care is delivered have been observed to play a role in the occurrence of polypharmacy. Processes include operational factors such as fragmented care and a loss of accountability in medication management. Poorly updated medical records, automated refill services, and prescribing to meet disease-specific quality metrics have been implicated in occurrence of polypharmacy.23
Some, if not several, of these factors likely played a role in the occurrence of the patient’s polypharmacy. In this case, it is apparent that the greatest influence on the occurrence of polypharmacy was the presence of multiple comorbidities, and treatment centered around addressing each morbidity with drug therapy.
Many patients suffering from a chronic disease condition may also endure concomitant illnesses, or comorbidities.24 Clinical treatment guidelines mainly focus on single disease conditions and often do not take into account patients who have comorbidities.25 Using guidelines for single conditions can pose problems to clinicians treating, and patients with, comorbidities, as patients with multiple medical conditions often have different healthcare needs.26
Increasing numbers of patients are prescribed complicated prevention regimens not just to treat each condition, but to reduce their future risk of serious medical events such as diabetes, stroke, and coronary events.27,28 It is not uncommon for patients with multiple comorbidities to be prescribed multiple medications to reduce long-term risk for those conditions. Recommended guidelines for treating each condition often are associated with drug therapy management and once a patient starts a medication, it may not be discontinued even though it may no longer be of benefit.20,29
Conclusion
For this case report, the information source is MedWatch, and reports are limited in the amount of detail about a patient’s condition.30 The intent of this report is not necessarily to describe a rare condition, but to characterize a set of health problems remarkable for their occurrence and concomitant medication use. Based on the observations recounted by clinicians, it is not clear if any of the patient’s illnesses were caused by treatment with excessive medications.
This case illustrates extreme polypharmacy. Although all medications may be clinically warranted, co-morbid conditions and multiple prescribers can result in polypharmacy, which can be problematic to patients if left unchecked. Non-compliance, drug-drug interactions and serious side effects can result from extreme polypharmacy. This is best summed up by Rowhani and Iglseder, “Although clinicians are aware of multimorbidity and the risks of polypharmacy, the dilemma of how to treat the frail and multimorbid without subjecting patients to under-treatment, or indeed over-treatment, remains”.19
Acknowledgments
The study was funded by The University of Texas at Tyler Ben and Maytee Fisch College of Pharmacy, with no external sources of funding or support.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Payne RA, Avery AJ. Polypharmacy: one of the greatest prescribing challenges in general practice. Br J Gen Pract. 2011;61(583):83–84. doi:10.3399/bjgp11X556146
2. Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13(1):57–65. doi:10.1517/14740338.2013.827660
3. Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17(1):230. doi:10.1186/s12877-017-0621-2
4. Taghy N, Cambon L, Cohen JM, Dussart C. Failure to reach a consensus in polypharmacy definition: an obstacle to measuring risks and impacts-results of a literature review. Ther Clin Risk Manag. 2020;16:57–73. doi:10.2147/TCRM.S214187
5. Quinna KJ, Shah NH. A dataset quantifying polypharmacy in the United States. Sci Data. 2017;4:170167. doi:10.1038/sdata.2017.167
6. Slone Epidemiology Center. Patterns of medication use in the United States, 2006: a report from the slone survey. Available from: https://www.bu.edu/slone/files/2012/11/SloneSurveyReport2006.pdf.
7. Hales CM, Servais J, Martin CB, Kohen D. Prescription drug use among adults aged 40–79 in the United States and Canada. NCHS data brief, No. 347. Hyattsville, MD: National Center for Health Statistics; 2019. Available from: https://www.cdc.gov/nchs/products/databriefs/db347.htm.
8. Woodruff K. Preventing polypharmacy in older adults. Am Nurse Today. 2010;5(10). Available from: https://www.myamericannurse.com/preventing-polypharmacy-in-older-adults/.
9. Nguyen T, Wong E, Ciummo F. Polypharmacy in older adults: practical applications alongside a patient case. J Nurse Pract. 2020;16:205–209. doi:10.1016/j.nurpra.2019.11.017
10. U.S. Food and Drug Administration. MedWatch: the FDA safety information and adverse event reporting program. Available from: https://www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program.
11. U.S. Food and Drug Administration. How to make a FOIA request; 2020. Available from: https://www.fda.gov/regulatoryinformation/foi/howtomakeafoiarequest/default.htm.
12. U.S. Food and Drug Administration. Questions and answers on FDA’s Adverse Event Reporting System (FAERS). What is FAERS?; 2018. Available from: http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Surveillance/AdverseDrugEffects.
13. Bleakley A. Stories as data, data as stories: making sense of narrative inquiry in clinical education. Med Educ. 2005;39(5):534–540. doi:10.1111/j.1365-2929.2005.02126.x
14. Agarwal S, Agarwal NK. 1397 – extreme polypharmacy in a patient with schizophrenia. Eur Psychiatry. 2013;28(S1):1. doi:10.1016/S0924-9338(13)76439-3
15. Nechba RB, Kadiri MEM, Bennani-Ziatni M, Zeggwagh AA, Mesfioui A. Difficulty in managing polypharmacy in the elderly: case report and review of the literature. J Clin Gerontol Geriatr. 2015;6(1):30–33. doi:10.1016/j.jcgg.2014.06.002
16. Finkelstein J, Friedman C, Hripcsak G, Cabrera M. Potential utility of precision medicine for older adults with polypharmacy: a case series study. Pharmgenomics Pers Med. 2016;9:31–45. doi:10.2147/PGPM.S101474
17. Gareri P, Gallelli L, Cotroneo AM, Manfredi VGL, De Sarro G. The art of safe and judicious deprescribing in an elderly patient: a case report. Geriatrics. 2020;5(3):57. doi:10.3390/geriatrics5030057
18. Eibling D. Too many medications-not enough saliva. Ear Nose Throat J. 2019;98(5):263–264. doi:10.1177/0145561319839704
19. Rowhani M, Iglseder B. Polypharmacy in palliative care-COPD and multimorbidity: a case report. Wien Med Wochenschr. 2018;168(7–8):177–183. English. doi:10.1007/s10354-018-0633-3
20. Halli-Tierney AD, Scarbrough C, Carroll D. Polypharmacy: evaluating risks and deprescribing. Am Fam Physician. 2019;100(1):32–38.
21. Hilmer SN, Gnjidic D. Prescribing for frail older people. Aust Prescr. 2017;40(5):174–178. doi:10.18773/austprescr.2017.055
22. Doos L, Roberts EO, Corp N, Kadam UT. Multi-drug therapy in chronic condition multimorbidity: a systematic review. Fam Pract. 2014;31(6):654–663. doi:10.1093/fampra/cmu056
23. Khezrian M, McNeil CJ, Murray AD, Myint PK. An overview of prevalence, determinants and health outcomes of polypharmacy. Ther Adv Drug Saf. 2020;11:2042098620933741. doi:10.1177/2042098620933741
24. Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med. 2009;7(4):357–363. doi:10.1370/afm.983
25. Bayliss EA, Edwards AE, Steiner JF, Main DS. Processes of care desired by elderly patients with multimorbidities. Fam Pract. 2008;25:287–293. doi:10.1093/fampra/cmn040
26. Guthrie B, Payne K, Alderson P, McMurdo MET, Mercer SW. Adapting clinical guidelines to take account of multimorbidity. BMJ. 2012;345:e6341.
27. Wise J. Polypharmacy: a necessary evil. BMJ. 2013;347:f7033. doi:10.1136/bmj.f7033
28. Rambhade S, Chakarborty A, Shrivastava A, Patil UK, Rambhade A. A survey on polypharmacy and use of inappropriate medications. Toxicol Int. 2012;19(1):68–73. doi:10.4103/0971-6580.94506
29. Bushardt RL, Massey EB, Simpson TW, Ariail JC, Simpson KN. Polypharmacy: misleading, but manageable. Clin Interv Aging. 2008;3(2):383–389. doi:10.2147/cia.s2468
30. Veronin MA, Schumaker RP, Dixit R. The irony of MedWatch and the FAERS database: an assessment of data input errors and potential consequences. J Pharm Technol. 2020;36(4):164–167. doi:10.1177/8755122520928495
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.