Back to Journals » Clinical Ophthalmology » Volume 19
Altered Dynamic Functional Connectivity in High Myopia: Findings From Leading Eigenvector Dynamics Analysis
Authors Wei B ![]() , Shu BL, Cheng Y, Wu XR
, Shu BL, Cheng Y, Wu XR
Received 29 July 2025
Accepted for publication 19 November 2025
Published 1 December 2025 Volume 2025:19 Pages 4367—4372
DOI https://doi.org/10.2147/OPTH.S556941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bin Wei,* Ben-Liang Shu,* Yuan Cheng,* Xiao-Rong Wu
Department of Ophthalmology, The First Affiliated Hospital, Nanchang University, Nanchang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao-Rong Wu, Department of Ophthalmology, the 1 st affiliated hospital, Jiangxi Medical College, Nanchang University, Nanchang, Jiangxi, People’s Republic of China, Tel +86-136117093259, Email [email protected]
Aim: This study aims to investigate the impact of high myopia (HM) on brain functional connectivity (FC) using Leading Eigenvector Dynamics Analysis (LEiDA), focusing on the dynamic characteristics of brain networks and their potential neural mechanisms.
Methods: We recruited 141 participants, including 82 high myopia patients and 59 healthy controls (HCs), matched for gender, age, and education level. LEiDA was applied to analyze dynamic functional connectivity (DFC). Key metrics, such as Mean Dwell Time (MDT), Transition Probability (TP), and Switching Rate (SR), were compared between groups using a two-sample t-test with FDR correction.
Results: High myopia patients showed significantly shorter MDT in phase-locking (PL) states 1 and 2 compared to HCs (p = 0.012, p = 0.011). However, no significant differences were found in TP, SR, or occupancy rates between the two groups.
Conclusion: This study demonstrates that high myopia is associated with altered dynamic brain connectivity, particularly in local network stability. The findings suggest that high myopia affects not only the visual system but also broader brain networks, potentially offering insights for early diagnosis and intervention strategies. Further research is needed to explore the therapeutic implications of these connectivity changes.
Keywords: LEiDA, high myopia, brain networks
Introduction
Myopia is currently the most prevalent refractive error worldwide and has become a global public health issue.1 By 2020, nearly 30% of the global population was affected by myopia, and its prevalence continues to rise annually.2,3 High myopia is myopia with a refractive error of −6D or more. Without timely intervention, it not only leads to vision impairment but can also result in severe ocular conditions such as fundus lesions and choroidal neovascularization, ultimately diminishing the patient’s quality of life.4 Moreover, high myopia is closely linked to changes in brain function. Recently, neuroimaging techniques, such as functional magnetic resonance imaging (fMRI), have revealed significant alterations in the connectivity and neural network activity of various brain regions in high myopia patients.5–7 This research, through dynamic functional analysis, provides a new perspective for a deeper understanding of the neural mechanisms underlying high myopia.
Recent fMRI applications have revealed significant alterations in the FC patterns of patients with high myopia. Research indicates that high myopia impacts not only the visual system but may also disrupt connectivity across various brain networks, including reduced connectivity strength between the visual cortex and regions such as the parietal and prefrontal cortices.5,6 Moreover, resting-state fMRI studies have demonstrated widespread disruptions in the static FC (SFC) of high myopia patients, particularly in the connections between visual-related areas and the cognitive control network.7 As neuroimaging technology advances, DFC analysis has become an increasingly important tool for investigating neurological disorders.8 Traditional SFC analysis only reveals the brain’s average connectivity patterns over extended periods, overlooking the brain’s dynamic changes at different moments. To address this limitation, the LEiDA technique has been developed in recent years, aiming to capture the brain’s DFC over short time intervals.9 LEiDA extracts the leading eigenvector of the FC matrix to identify the brain’s dominant connectivity patterns at different time points, allowing for the detection of phase-locking states and their transition modes.10 This technique not only analyzes the brain’s instantaneous connectivity changes but also uses clustering analysis to summarize the brain’s common functional states. Compared to other methods, LEiDA provides a more flexible and effective tool to analyze the dynamic functional state of the brain and is particularly good at capturing dynamic changes over short time scales. While studies have shown significant changes in the static functional networks of high myopia patients,11,12 the dynamic characteristics of their brain networks remain underexplored. To date, no research has applied LEiDA to investigate DFC alterations in high myopia patients.
Therefore, this study introduces the LEiDA technique to explore the impact of high myopia on various brain functional states by capturing the dynamic changes in brain connectivity.
Materials and Methods
Participants
Between August and December 2021, 385 participants were recruited by the First Affiliated Hospital of Nanchang University, with 254 excluded based on eligibility criteria. The final group consisted of 141 participants: 82 high myopia patients and 59 HCs, matched for gender, age, and education level. The inclusion criteria for high myopia patients were myopia a spherical equivalent refractive error of ≤ −6.00 D in both eyes, corrected visual acuity greater than 1.0, normal ophthalmic examination results, and the ability to tolerate MRI. HCs were required to have normal visual acuity and no history of eye or systemic diseases. Subjects with significant eye diseases, prior surgeries, or brain conditions were excluded from the study.
Acquisition and Preprocessing of fMRI Data
MRI data were acquired using a 3-Tesla Trio magnetic resonance imaging system, with participants instructed to minimize movement, keep their eyes closed, and remain awake. Noise-canceling headphones were provided to reduce external noise. The T1-weighted imaging parameters included an echo time of 2.26 ms, a slice thickness of 1 mm, an acquisition matrix of 256 × 256, a repetition time of 1900 ms, a 240×240 mm2 field of view, and a 12° flip angle. Data preprocessing, conducted using DPABI toolboxes, MATLAB 2013b, and SPM12, involved discarding the initial 10 volumes, spatial smoothing, temporal correction, functional volume analysis, spatial normalization, and head motion correction.
Static Functional Connectome Analysis
First, based on the time series of each subject’s brain regions, the instantaneous functional connectivity matrix at each time point was calculated and the principal eigenvectors were extracted by eigenvalue decomposition to represent the main functional connectivity patterns at that time point. Then, the principal eigenvectors of all time points were constructed into a time series, and a k-means clustering algorithm was applied to cluster these principal eigenvectors into different PL states representing common functional connectivity patterns in the brain. In the LEiDA framework, each fMRI time frame is represented by the leading eigenvector of the BOLD phase-locking matrix, which captures the dominant pattern of instantaneous synchronization across all brain regions. Clustering these eigenvectors identifies a set of recurrent phase-locking states that characterize distinct configurations of large-scale brain networks. To describe the temporal properties of these states, four dynamic metrics were computed: fractional occupancy (FO), representing the proportion of time spent in each state; mean dwell time, reflecting the average duration that the brain remains in a given state; switching rate, indicating how frequently transitions occur between states; and transition probability, denoting the likelihood of moving from one state to another. Together, these measures provide a comprehensive characterization of the stability and flexibility of brain functional dynamics. Then, each state was characterized, including the calculation of FO, MDT, TP, and SR, to assess the occurrence of each state in the time series, frequency, stability, and dynamic transition patterns. Frequency, stability, and dynamic transition patterns.
Statistical Analysis
A two-sample t-test was used to compare DFC characteristics between the high myopia and HC groups, with a false-discovery rate (FDR)-corrected alpha threshold of 0.05.
Results
Participant Characterization
The study included a total of 82 high myopia patients (43 males and 39 females) with an average age of 26.53 ± 5.29 years, alongside 59 healthy controls (24 males and 35 females) with an average age of 25.67 ± 3.10 years. There were no significant differences in gender distribution (p = 0.17) or age (p = 0.27) between the two groups.
Dynamic Functional Connectivity Analysis
In the DFC, significant differences were detected in PL states 1 and 2 when the DFC was divided into 3 PL states, as illustrated by the spatial distribution of brain network nodes (Figure 1A) and their corresponding connectivity patterns (Figure 1B). The MDT was shorter in the high myopia group compared to the HC group (p = 0.012 and p = 0.011, FDR-corrected) (Figure 2A). However, there were no significant differences in fractional occupancy (Figure 2B), while the state-transition probabilities (Figure 2C) were calculated from an exploratory 5-state model to provide a more detailed view of state transitions, or switching rates (Figure 2D) between the two groups. Similarly, no significant group differences were observed in the transition matrices (Figure 2E) and mean transition probabilities (Figure 2F).
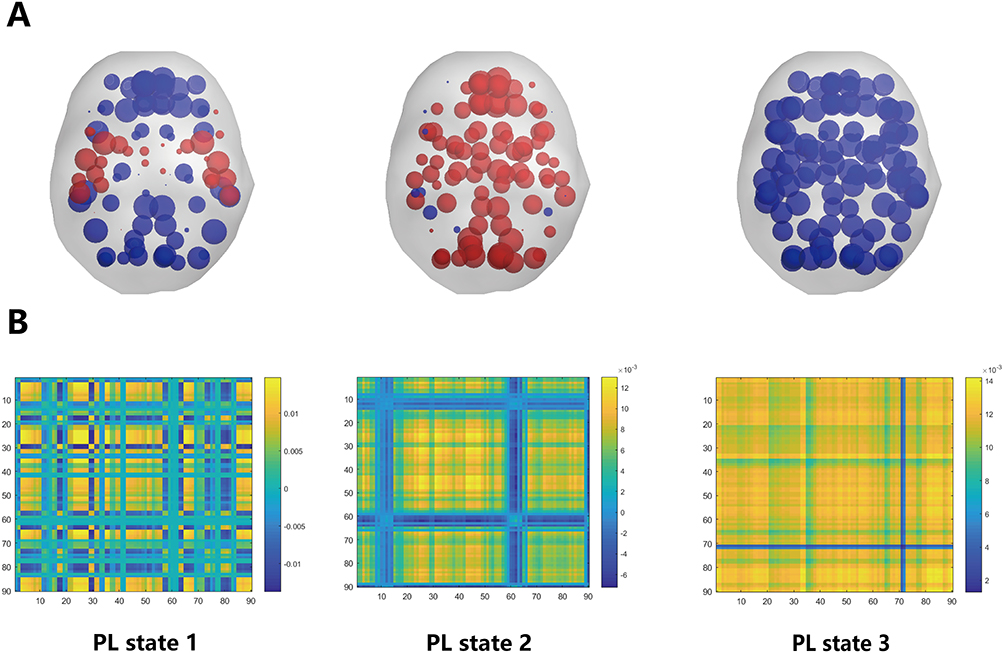 |
Figure 1 The patterns of 3 PL states detected by clustering the set of leading eigenvectors into 3 clusters. (A) The nodes in the brain network are represented by blue and red spheres, and the size and color shades of the nodes indicate the level of activity and strength of connectivity of different brain regions in this state. Red spheres indicate more active regions and blue spheres indicate less active regions. (B) The 90×90 connectivity pattern corresponding to each state. In these matrices, color intensity and line width indicate the strength of functional coupling between brain regions, where warmer colors and thicker lines represent stronger positive phase-locking relationships. |
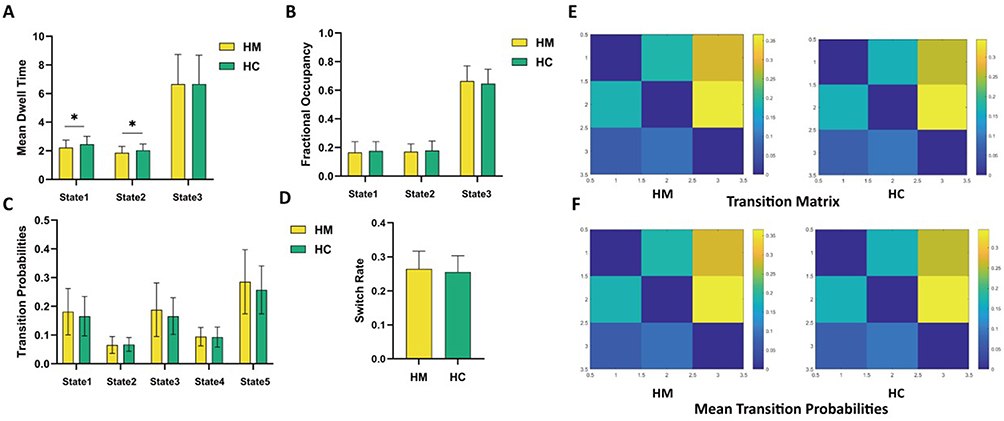 |
Figure 2 Comparison between dynamic functional connectivity in HM and HC groups. *indicate significant group differences between the two groups after mean dwell time correction (P < 0.05). (A–D) Comparison of mean dwell time, Fractional Occupancy, Transition Probability and switch rate between HM and HC groups (E and F) Transition Matrix and Mean Transition Probability for groups HM and HC. |
Discussion
In this study, LEiDA analysis categorized dynamic functional connectivity into three PL states. The results showed significant changes in the brain connectivity patterns of high myopia patients in PL state 1 and PL state 2. Compared to the HCs group, the high myopia group exhibited shorter MDT in these two states, indicating that the brains of high myopia patients switch between these functional states more rapidly, potentially suggesting reduced stability in their brain connectivity.
In previous research, Yang et al used LEiDA to study fMRI data from participants with Alzheimer’s disease, mild cognitive impairment, and cognitively normal individuals. Their findings revealed abnormal dynamic activity in the resting-state networks of AD and MCI patients, offering new insights into the dynamic analysis of brain networks.13 Cahart’s research group, using emotion dynamics and LEiDA data analysis, discovered that anhedonia-mediated depression influenced the relationship between attention network recruitment and emotional blunting.9 MDT is a key indicator in DFC analysis, reflecting the stability and flexibility of the brain in different functional states. By analyzing MDT, we can uncover how the brain transitions between various states and the association between the duration of these states and functional stability. Xie et al found a significant reduction in MDT in state 3 among chronic tinnitus patients (t = 2.039, P = 0.046), suggesting that abnormal brain network dynamics contribute to understanding the mechanisms of tinnitus and provide potential therapeutic implications.14 Similarly, Chen’s team observed that MDT increased in state 1 but decreased in state 3 for patients with residual dizziness after benign paroxysmal positional vertigo (BPPV), indicating altered global meta-states and temporal features in these patients.15 The reduction in MDT observed in high myopia patients may indicate an underlying instability in visual processing and cognitive integration, reinforcing the hypothesis that high myopia affects not only the visual system but also other brain networks. These findings could have implications for early diagnosis and treatment strategies, suggesting that neuroimaging markers of DFC changes could potentially be used to identify patients at risk for more complex neurological disruptions. This is consistent with our previous research findings.16
Additionally, although no significant differences were detected in transition probability, switching rate, or occupancy across the three states, this may suggest that high myopia primarily affects the stability of local functional networks, while the global dynamic functional connectivity patterns remain relatively stable Of course, it is also possible that the lack of detected differences could be due to insufficient statistical power or a small sample size, which could lead to discrepancies.
This study innovatively used the LEiDA technique to explore the DFC of the brain in patients with high myopia, which provides a more comprehensive view than static analysis, capturing fluctuations in brain networks over time. However, a limitation of the study was the small sample size and the relatively homogenous validation area. In addition, the study focused primarily on specific PL states, which limits the breadth of findings, and comparisons with other vision-related neurological disorders may further enrich the understanding of high myopia.
Conclusion
This study shows that high myopia alters DFC, particularly in local brain network stability. These findings highlight broader neural impacts of high myopia beyond the visual system, offering insights that could aid in early diagnosis and treatment.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
Ethical approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Medical Research Ethics Committee of The First Affliated Hospital of Nanchang University.
Consent to Participate
Written informed consents were provided by all the participants.
Acknowledgments
We would like to express our gratitude to Director Zeng of the Radiology Department and Dr. Wang Yuanyuan from The First Affiliated Hospital of Nanchang University for their significant contributions to this experiment. Their support ensured the smooth progress of our study and provided a solid foundation for future research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received support from the National Natural Science Foundation of China (Grant No. 82160207), the Technology Plan of Jiangxi Provincial Health and Health Commission (202130156), Young Scholar Project of the First Affiliated Hospital of Nanchang University (YFYPY202219), Jiangxi Science Education Society (2025KXJYS354), and the Science and Key Projects of Jiangxi Youth Science Fund (No. 20202ACBL216008).
Disclosure
The authors declare no competing interests.
References
1. Medina A. The cause of myopia development and progression: theory, evidence, and treatment. Survey Ophthalmol. 2022;67(2):488–509. doi:10.1016/j.survophthal.2021.06.005
2. Dolgin E. The myopia boom. Nature. 2015;519(7543):276–278. doi:10.1038/519276a
3. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
4. Ohno-Matsui K, Wu PC, Yamashiro K, et al. IMI pathologic myopia. Invest Ophthalmol Visual Sci. 2021;62(5):5. doi:10.1167/iovs.62.5.5
5. Ji Y, Shi L, Cheng Q, et al. Abnormal large-scale neuronal network in high myopia. Front Human Neurosci. 2022;16:870350. doi:10.3389/fnhum.2022.870350
6. Wu YJ, Wu N, Huang X, et al. Evidence of cortical thickness reduction and disconnection in high myopia. Sci Rep. 2020;10(1):16239. doi:10.1038/s41598-020-73415-3
7. Cheng Y, Chen XL, Shi L, et al. Abnormal functional connectivity between cerebral hemispheres in patients with high myopia: a resting FMRI study based on voxel-mirrored homotopic connectivity. Front Human Neurosci. 2022;16:910846. doi:10.3389/fnhum.2022.910846
8. Ma H, Xu Y, Tian L. RS-MAE: region-state masked autoencoder for neuropsychiatric disorder classifications based on resting-state fMRI. IEEE Trans Neural Net Learn Syst. 2024. doi:10.1109/TNNLS.2024.3449949
9. Cahart MS, Giampietro V, Naysmith L, et al. Anhedonia severity mediates the relationship between attentional networks recruitment and emotional blunting during music listening. Sci Rep. 2024;14(1):20040. doi:10.1038/s41598-024-70293-x
10. Cabral J, Vidaurre D, Marques P, Kringelbach ML. Cognitive performance in healthy older adults relates to spontaneous switching between states of functional connectivity during rest. Sci Rep. 2017;7(1):5135. doi:10.1038/s41598-017-05425-7
11. Wei B, Huang X, Ji Y, et al. Analyzing the topological properties of resting-state brain function network connectivity based on graph theoretical methods in patients with high myopia. BMC Ophthalmol. 2024;24(1):315. doi:10.1186/s12886-024-03592-6
12. Ji Y, Huang SQ, Cheng Q, et al. Exploration of static functional connectivity and dynamic functional connectivity alterations in the primary visual cortex among patients with high myopia via seed-based functional connectivity analysis. Front Neurosci. 2023;17:1126262. doi:10.3389/fnins.2023.1126262
13. Yang YL, Liu YX, Wei J, et al. Alterations of resting-state network dynamics in Alzheimer’s disease based on leading eigenvector dynamics analysis. J Neurophysiol. 2024;132(3):744–756. doi:10.1152/jn.00027.2024
14. Xie J, Zhang W, Yu C, et al. Abnormal static and dynamic brain network connectivity associated with chronic tinnitus. Neuroscience. 2024;554:26–33. doi:10.1016/j.neuroscience.2024.06.034
15. Chen Z, Cai Y, Xiao L, et al. Increased functional connectivity between default mode network and visual network potentially correlates with duration of residual dizziness in patients with benign paroxysmal positional vertigo. Front Neurol. 2024;15:1363869. doi:10.3389/fneur.2024.1363869
16. Wei B, Fu WW, Ji Y, et al. Exploration of hippocampal functional connectivity alterations in patients with high myopia via seed-based functional connectivity analysis. Clin Ophthalmol. 2023;17:3443–3451. doi:10.2147/OPTH.S434797
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.