Back to Journals » Psychology Research and Behavior Management » Volume 19
Altered Bilateral Motor Cortex Excitability and Peripheral Glutamate/GABA Imbalance in Generalized Anxiety Disorder: A TMS Investigation
Authors Zhou X, Zhang P ![]() , Chen R, Shi G, Liu W, Zhang P, Zhou P
, Chen R, Shi G, Liu W, Zhang P, Zhou P ![]()
Received 10 January 2026
Accepted for publication 13 May 2026
Published 10 June 2026 Volume 2026:19 595261
DOI https://doi.org/10.2147/PRBM.S595261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gabriela Topa
Xiayun Zhou,1,2 Pan Zhang,1 Ruiming Chen,1 Guoao Shi,1 Weiai Liu,2 Peng Zhang,2 Peng Zhou1
1The Seventh Clinical College of Guangzhou University of Chinese Medicine/Shenzhen Bao’an Traditional Chinese Medicine Hospital, Shenzhen, People’s Republic of China; 2Department of Acupuncture, The Second Affiliated Hospital of Hunan University of Traditional Chinese Medicine, Changsha, People’s Republic of China
Correspondence: Peng Zhou, Email [email protected]
Objective: Generalized anxiety disorder (GAD) imposes a substantial burden on individuals and society, yet its underlying neurophysiological mechanisms remain unclear. This study aimed to investigate whether GAD is associated with abnormalities in bilateral motor cortex excitability and peripheral neurochemical balance.
Methods: This case-control study compared 30 unmedicated GAD patients with 30 age- and gender-matched healthy controls. Cortical excitability indices—including resting motor threshold (rMT), motor evoked potential amplitude (MEP-A) and latency (MEP-L), and cortical silent period (CSP)—were assessed using single-pulse transcranial magnetic stimulation (spTMS). Peripheral serum levels of glutamate (Glu) and gamma-aminobutyric acid (GABA) were also measured. P-values for primary outcomes were corrected using the Bonferroni correction.
Results: Key findings revealed a pathological imbalance in bilateral motor cortex excitability in GAD patients. This was characterized by a significant increase in left rMT (the corrected p< 0.05) and a decrease in left MEP-A (the corrected p< 0.05), alongside an increase in right MEP-A (the corrected p< 0.05), resulting in a significantly reduced left-to-right MEP-A ratio (the corrected p< 0.001). No significant inter-group differences were found for MEP-L or CSP after Bonferroni correction
Conclusion: These results demonstrate that GAD involves systemic dysregulation across neurophysiological and neurochemical domains, featuring left-lateralized cortical hypoexcitability and right-lateralized hyperexcitability, coupled with altered peripheral glutamate-GABA balance. The combined use of TMS-derived excitability metrics and peripheral neurochemical markers may offer novel objective indicators to supplement clinical assessment in GAD. Further research is needed to establish the diagnostic specificity of these biomarkers. This study was registered with the Chinese Clinical Trial Registry (ChiCTR2200066311).
Keywords: generalized anxiety disorder, transcranial magnetic stimulation, cortical excitability, glutamate, gamma-aminobutyric acid, neurophysiology
Introduction
Generalized Anxiety Disorder (GAD) is a common chronic mental disorder that ranks among the top causes of mental health burden worldwide.1,2 As the most common subtype of anxiety disorders, its lifetime prevalence is approximately 3–6%.3 The core clinical features of GAD include persistent and uncontrollable excessive worry about daily life events (generalized worry),4,5 often accompanied by a series of psychological and physical symptoms such as restlessness, muscle tension, fatigue, difficulty concentrating, and sleep disorders.6–8 Due to its chronic and recurrent nature, GAD can significantly impair patients’ social functions and quality of life, and bring a heavy public health burden.9–12 However, the pathophysiological mechanism of GAD has not been fully elucidated yet. Clinical diagnosis mainly relies on the Diagnostic and Statistical Manual of Mental Disorders (DSM) or International Classification of Diseases (ICD) standards and subjective symptom assessment tools such as the Hamilton Anxiety Scale (HAMA), lacking objective and reliable biological markers, which to some extent limits the precise identification, mechanism analysis, and efficacy evaluation of this disease.13,14
In recent years, the development of non-invasive brain function detection technologies has provided a new approach for exploring the neural mechanisms of mental disorders. Single-pulse Transcranial Magnetic Stimulation (spTMS) is a mature neuroelectrophysiological technique.15 By stimulating the primary motor cortex (M1) and recording motor evoked potentials (MEPs) in the contralateral target muscle, spTMS can objectively and quantitatively assess the excitatory and inhibitory functions of the corticospinal pathway. The resting motor threshold (rMT) reflects the baseline excitability of the cortical neuronal population; MEP amplitude (MEP-A) and latency (MEP-L) respectively represent the overall excitatory state and nerve conduction velocity of the corticospinal pathway; and the cortical silent period (CSP) is mainly related to the inhibitory function mediated by GABA within the cortex.16 These indicators have been proven to sensitively reflect the excitation-inhibition (E/I) balance state of various mental disorders, including anxiety disorders and depression.17–21 Although M1 does not directly participate in advanced emotional processing, its excitatory state can indirectly reflect the E/I balance of a broader cortical network affected by the emotional regulation network of the prefrontal-amygdala system.22 Therefore, spTMS is a reliable tool for studying the neurophysiological basis of mental disorders. In GAD patients, spTMS can not only serve as an objective tool for assessing anxiety states,23 but also predict treatment responses based on baseline cortical excitability, providing theoretical basis for individualized intervention strategies.24 Current research is increasingly focusing on using the excitatory parameters derived from spTMS to explore the neurobiological mechanisms of anxiety-related symptoms.25 It is notable that healthy individuals typically exhibit a physiological asymmetry pattern of relatively lower excitability in the right hemisphere motor cortex, which is regulated by commissural fibers such as the corpus callosum.26–28 Neuroimaging studies suggest that GAD patients may have abnormal inter-hemispheric functional connections involving brain regions such as the prefrontal and temporal lobes,29 as well as a functional advantage or imbalance of the right hemisphere in emotional processing.21 This provides a theoretical basis for exploring whether GAD patients have pathological lateralization imbalance of cortical excitability.
At the neurochemical level, the normal function of the central nervous system highly depends on the dynamic balance between the excitatory neurotransmitter glutamate (Glu) and the inhibitory neurotransmitter Gama-aminobutyric acid (GABA). Glu/GABA system imbalance is considered one of the core pathological mechanisms of anxiety disorders.30,31 Studies have shown that although the levels of Glu and GABA in peripheral blood (serum or plasma) cannot directly equate to the concentrations in the central nervous system, they can to some extent reflect their metabolic status or be affected by systemic pathological physiological processes (such as chronic stress, inflammation). The GABA/Glu ratio is often used as a potential alternative indicator to assess the peripheral E/I balance status.32,33
Based on the above background, this study aims to integrate the two dimensions of neurophysiology and neurochemistry to systematically explore the cortical excitability characteristics of GAD patients and their association with the peripheral E/I system balance. We hypothesize that compared with healthy control groups, untreated GAD patients have pathological imbalance of bilateral motor cortex excitability (manifested as lateralized changes in specific spTMS indicators), and this imbalance may be associated with the deviation of the GABA/Glu ratio in peripheral serum. To this end, this study uses spTMS technology to quantify the rMT, MEP-A, MEP-L and CSP of the bilateral M1 area of the participants, and simultaneously detects the concentrations of Glu and GABA in peripheral serum and their ratios. By comparing the inter-group differences between GAD patients and healthy controls, this study aims to provide new empirical evidence for clarifying the pathophysiological mechanism of GAD and explore the potential value of these objective indicators as future clinical auxiliary assessment tools.
Materials and Methods
Ethical Declaration, Research Design and Participant Recruitment
This study is a case-control study. It has been approved by the Ethics Committee of Shenzhen Bao’an Traditional Chinese Medicine Hospital (Ethical Approval Number: KY-2022-035-01), and has been registered in the Chinese Clinical Trial Registry (Registration Number: ChiCTR2200066311). All research procedures follow the principles of the Helsinki Declaration. All participants were fully informed about the research purpose, process, potential risks and benefits by the researchers before participating in the study, and signed a written informed consent form before the assessment of enrollment.
Participants
The research participants were patients with GAD who visited the outpatient department of Shenzhen Bao’an Traditional Chinese Medicine Hospital affiliated to Guangzhou University of Chinese Medicine and its 18 community health centers from October 2022 to September 2023 (GAD group). At the same time, healthy control participants (HC group) with matching age and gender were recruited through hospital internal advertisements and social networks. A total of 60 participants were planned to be included, with 30 participants in each group. The TMS operators and laboratory analysts were unaware of the group assignment of the participants to minimize assessment bias.
Inclusion Criteria
GAD group: (1) They met the diagnostic criteria for GAD as stipulated in the “Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)” of the United States; (2) 14≤HAMA score <29; (3) Hamilton Depression Scale (HAMD) 17-item total score less than 7; (4) 18 years ≤Age ≤65 years; (5) Right-handed; (6) Able to cooperate with testing and treatment arrangements, and without communication and cognitive impairments; (7) No medication, psychological, or physical treatment in the past 3 weeks; (8) Signed an informed consent form and voluntarily participated in the study.
HC group: (1) 18 years≤Age≤65 years; (2)Right-handed; (3) Previously healthy, physically and mentally well, HAMA and HAMD both less than 7, no physical discomfort in the past month; (4) No central stimulation (rTMS, TDCS, etc.) or peripheral stimulation (acupuncture, transcutaneous electrical stimulation, etc.) in the past 3 months; (5) No history of illegal drug use or excessive alcohol consumption; (6) Sign an informed consent form and voluntarily participate in this study.
Exclusion Criteria
GAD group: (1) History of clear mental illness or other diseases that can present anxiety symptoms, such as schizophrenia, bipolar disorder, or other mental disorders, or somatic diseases; (2) History of brain injury, epilepsy, or accompanied by liver and kidney dysfunction, with metal implants or serious organic diseases of the cardiovascular, liver, or kidney; (3) Current or past self-harm or suicidal plans or behaviors, or psychotic symptoms; (4) Individuals with alcohol or drug abuse dependence or pregnant women.
HC group: (1) Individuals with speech disorders; (2) Individuals with hypertension, diabetes, or significant diseases of the heart, liver, kidney, etc.; (3) Individuals with a history of dementia, mental illness, epilepsy, or other neurological diseases; (4) History of cranial trauma or surgery; (5) Individuals with metal residues in the body (including dentures, pacemakers, neurostimulators, medical pumps, etc.); (6) Individuals who fear TMS or cannot undergo TMS stimulation for other reasons; (7) Pregnant women.
Dropout Criteria
Failure to detect the motor cortical hand area through TMS testing.
Observation Indicators and Detection Methods
Clinical Assessment
At enrollment, trained researchers used the HAMA to assess the severity of anxiety symptoms. The 14-item scale has a total score range of 0–56, with higher scores indicating greater symptom severity.
spTMS and Electromyography (EMG) Recording
The participants adjusted themselves to a comfortable sitting position, keeping their heads and arms relaxed. A long flexible ruler was used to measure and record the two midlines from the root of the nasal ridge to the posterior nuchal tubercle and from the anterior edge of the bilateral ear pinnae, marking the intersection point of the two lines as the Cz point. From the Cz point, 5 cm towards the bilateral ear pinnae gave the coordinates of left M1 and right M1. With the bilateral M1 as the center, a 9-grid pattern with a distance of 1 cm both horizontally and vertically was marked. The MagstimRapid2 transcranial magnetic stimulation device (from Magstim Company, UK) and the Nicolet Viking Quest physiological recorder (from Natus Neurology Company, USA) were turned on. The spTMS stimulation mode was selected and the stimulation output intensity was adjusted. According to the brain side to be tested, the recording electrode connected to the electromyography evoked potential recorder was pasted on the first dorsal interosseous muscle of the contralateral hand (FDI), the reference electrode was placed on the radial side in front of the second metacarpophalangeal joint of the same hand, and the ground electrode was pasted on the ulnar styloid process. Before pasting the electrode sheet, the local skin of the electrode placement area needed to be treated with a Weber abrasive gel to remove the dead skin. The TMS eight-shaped coil was placed at a 45 angle to the anterior midline and closely adhered to the scalp, with the cut surface being the motor cortex of the brain side, namely the M1 area. The stimulation intensity started from 50%, and the stimulation intensity was adjusted according to the individual differences of the participants. Each stimulation interval was 5–10 seconds. (1) Determine the optimal stimulation point: Stimulate each point in the 9-grid pattern centered on M1 and 1 cm apart both horizontally and vertically. If no obvious MEP amplitude appeared during the stimulation, the stimulation intensity could be increased according to the situation until the optimal position that could induce MEP in FDI was found, which was the optimal stimulation point. (2) Determine rMT: Perform 10 consecutive output stimulations at each bilateral optimal stimulation point, and the minimum stimulation intensity that could trigger MEPs with a≥50uV amplitude (MEP-A being the maximum, MEP-L being the shortest and having the best repeatability) at least 5 times or more was the rMT. (3) Determine the stimulation intensity: Apply 10 stimulations at each bilateral optimal stimulation point, setting the spTMS stimulation intensity at 120% of rMT. Each stimulation interval was 5–10 seconds. The MEP-A and MEP-L of the motor evoked potential induced by this stimulation were measured 10 times, and the average value was taken as the measurement value of MEP-A and MEP-L for this time. The CSP recorded at the optimal stimulation point when the bilateral FDI maintained 20% of the maximum force was detected, and the CSP measurement value was taken as the average value of 10 consecutive measurements. All EMG signal sampling rates were set at 48kHz, with a band-pass filter of 2–10KHz, and the data were stored and analyzed offline.
Detection of Peripheral Serum Glu and GABA Concentrations
Peripheral venous blood samples (6 mL) were collected from all participants in a fasting state between 8:00 and 9:00 AM. After clotting at room temperature for 30 minutes, samples were centrifuged at 3000 rpm (4°C) for 15 minutes to separate serum. Serum was immediately aliquoted and stored at −80°C until analysis. Serum concentrations of Glu and GABA were determined using commercial enzyme-linked immunosorbent assay (ELISA) kits (Human Glutamate ELISA Kit, AE91435Hu; Human GABA ELISA Kit, AE91068Hu; AMEKO, Shanghai Lianshou Biotechnology Co., Ltd., China). All assays were performed by Guangzhou Jin Yu Medical Laboratory Co., Ltd., following the manufacturer’s protocols. The GABA/Glu ratio was calculated as a potential peripheral index of excitation-inhibition (E/I) balance.
Statistical Analysis
Data were analyzed using SPSS software (version 25.0). Continuous variables were tested for normality (Shapiro–Wilk test) and homogeneity of variance (Levene’s test). Normally distributed data are presented as mean±standard deviation (Mean±SD) and were compared between groups using independent samples t-tests (with Welch’s correction if variances were unequal). Non-normally distributed data are presented as median (interquartile range) and were compared using the Mann–Whitney U-test. Categorical data are presented as counts (percentages) and were compared using the chi-square test.
The primary analyses compared the GAD and HC groups on bilateral rMT, MEP-A, MEP-L, CSP, serum Glu, serum GABA, and the GABA/Glu ratio. To control the Type I error rate due to multiple comparisons, the Bonferroni correction was applied separately for the two families of primary outcomes: 12 cortical excitability indices and 3 peripheral serum neurotransmitter levels. The corrected P<0.05 was considered statistically significant. All tests were two-sided with 0.05. A post-hoc power analysis will be conducted based on the observed effect sizes to evaluate the statistical power of this study.
Results
Participant Flow and Baseline Characteristics
A total of 60 participants were enrolled in this study, comprising 30 patients with GAD and 30 healthy people. All participants completed peripheral blood serum collection, spTMS assessment, and clinical evaluations, with no dropouts. The participant screening and enrollment flow is depicted in Figure 1.
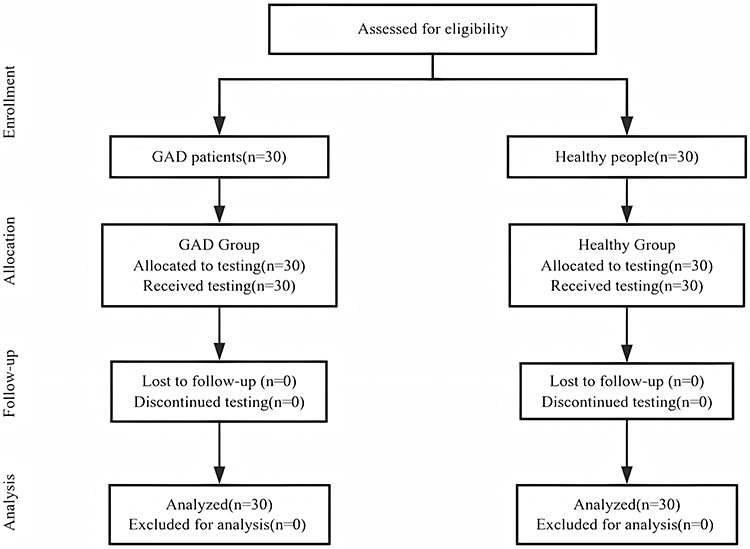 |
Figure 1 Flow Chart of the Research Participants. |
There were no statistically significant differences between the two groups in terms of age (p>0.05) and gender composition (p>0.05), indicating well-matched baseline characteristics and comparability. As expected, the total HAMA score was significantly higher in the GAD group compared to the HC group, with a highly statistically significant difference (p<0.001).
Comparison of Bilateral Motor Cortex Excitability Indices
Comparisons of bilateral primary motor cortex excitability indices between the two groups are presented in Table 1. The main findings are as follows:
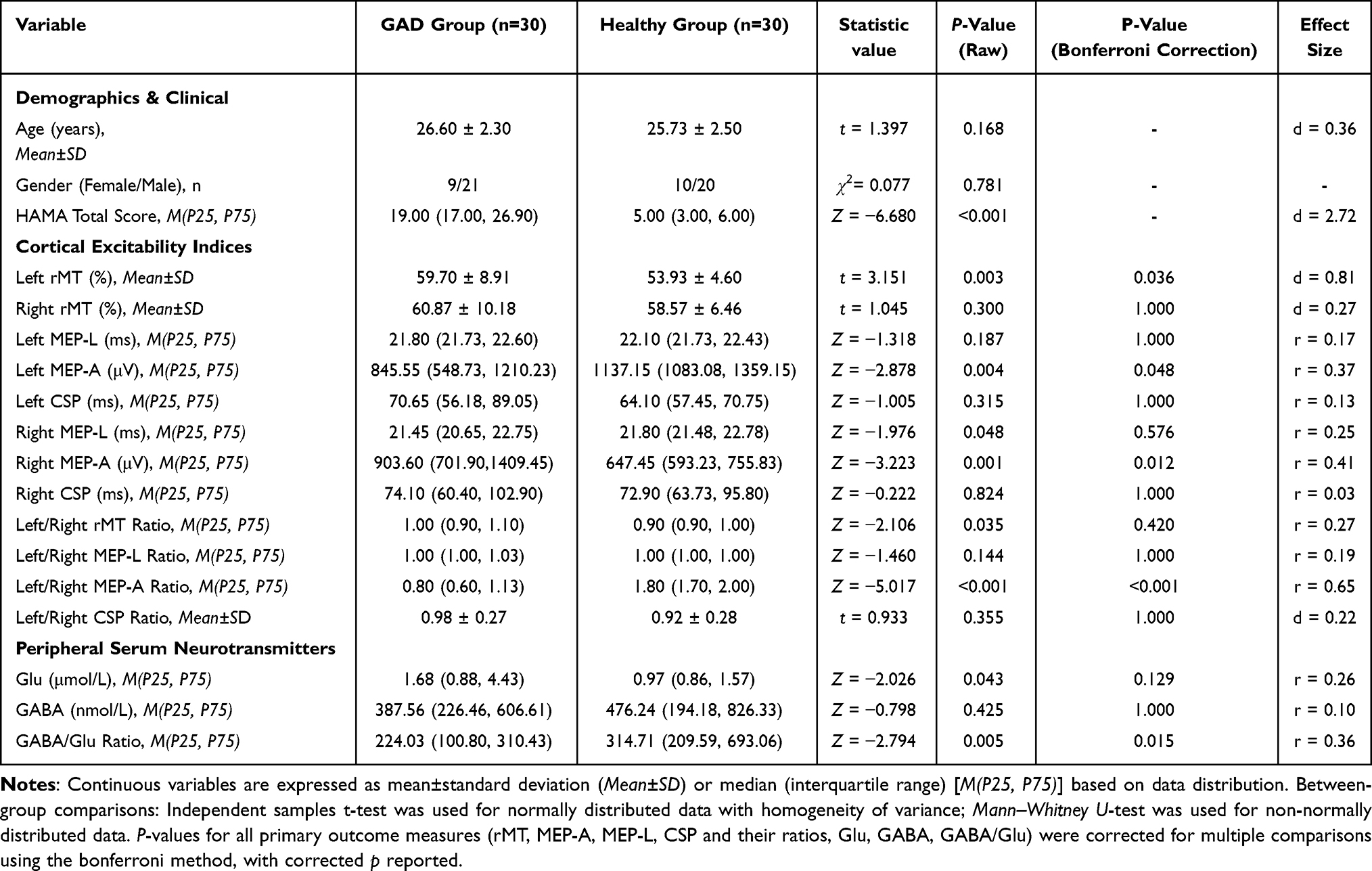 |
Table 1 The Demographic, Clinical and Neurophysiological Characteristics of Patients with GAD and Healthy Controls |
(1) rMT: The rMT of the left M1 was significantly higher in the GAD group compared to the HC group, with a statistically significant difference (p<0.01, the corrected p<0.05). There was no significant difference in the right M1 rMT between groups (p>0.05). The left/right rMT ratio showed no statistically significant difference between the GAD group and the HC group, although a trend was observed (p<0.05, the corrected p>0.05).
(2)MEP-A: The left MEP-A was significantly lower in the GAD group compared to the HC group, while the right MEP-A was significantly higher in the GAD group compared to the HC group. These differences were highly statistically significant (left: p<0.01, the corrected p<0.05; right: p<0.01, the corrected p<0.05). The left/right MEP-A ratio was significantly lower in the GAD group than in the HC group, with a highly statistically significant difference (p<0.001, the corrected p<0.001).
(3)MEP-L and CSP: No statistically significant differences were found between the two groups for left MEP-L, right MEP-L (p<0.05, the corrected p>0.05), bilateral CSP, or the left/right ratios of MEP-L and CSP (all p>0.05, the corrected p>0.05).
Comparison of Peripheral Serum Glutamate and GABA Levels
Analysis of peripheral serum neurotransmitter levels revealed: Serum Glu levels were higher in the GAD group than in the HC group in the raw analysis (p<0.05), but this difference did not remain statistically significant after FDR correction for multiple comparisons (the corrected p>0.05). There was no significant difference in serum GABA levels between the two groups (p>0.05). The GABA/Glu ratio was significantly lower in the GAD group compared to the HC group, with a statistically significant difference (p<0.01, the corrected p<0.05). As presented in Table 1.
Discussion
This study provides objective neurophysiological and neurochemical evidence for the pathophysiology of GAD. The key findings are that, compared to healthy controls, GAD patients exhibit a pathological imbalance in bilateral motor cortex excitability, characterized by an increase in the left rMT, a decrease in the left MEP-A, an increase in the right MEP-A, and a consequently significantly reduced left-to-right MEP-A ratio. Concurrently, GAD patients showed a decreased peripheral serum GABA/Glu ratio. These results suggest that GAD involves a systematic dysregulation spanning from cortical excitability to peripheral neurochemical balance.
The primary motor cortex is increasingly recognized for its role in emotional processing, with its state modulated by affective conditions such as anxiety.34,35 TMS offers a direct method to probe cortical physiology.36 The MEP-A specifically reflects the net excitatory output of the corticospinal pathway, influenced by the balance of intracortical facilitatory and inhibitory circuits.37–39 Our finding of reduced left MEP-A alongside elevated right MEP-A in GAD represents a clear deviation from the physiological asymmetry typically observed in healthy individuals, where the non-dominant (often right) hemisphere shows relatively lower excitability.26–28,40 This pattern of left-sided hypoexcitability and right-sided hyperexcitability provides objective support for theories of right-hemisphere functional dominance in anxiety.21 The observed right M1 hyperexcitability may be a neurophysiological correlate of the persistent hyperarousal central to GAD.
Furthermore, the observed increase in peripheral serum Glu and decrease in the GABA/Glu ratio align with the central hypothesis of E/I imbalance in anxiety disorders.41–47 The E/I balance is fundamental to neural circuit function and is governed by the dynamic interplay between glutamatergic and GABAergic transmission.48–60 While peripheral levels are influenced by systemic factors and do not directly equate to central synaptic concentrations,61–64 the co-occurrence of this peripheral neurochemical shift with the specific cortical excitability pattern suggests a multi-level systemic disturbance. This convergence hints that a widespread E/I dysregulation, potentially stemming from common pathophysiological processes like chronic stress, may underlie both the central excitability imbalance and peripheral biochemical changes observed in GAD.
However, several limitations must be considered. First, the relationship between peripheral neurochemistry and central cortical excitability is indirect and may be mediated by shared systemic factors. Second, the observed lateralized cortical excitability pattern, while prominent in GAD, may not be entirely specific and could be present in other high-arousal disorders such as depression or PTSD.40 This is a common challenge for cross-sectional biomarker studies. Finally, these objective indicators are currently exploratory. Their true value lies as potential supplementary tools to augment clinical assessment based on subjective scales, and their diagnostic specificity and clinical utility require validation in larger, prospective, and transdiagnostic cohorts.
Conclusion
In summary, this study utilized spTMS technology to demonstrate that unmedicated GAD patients exhibit a distinct imbalance in bilateral motor cortex excitability, characterized by left-sided hypoexcitability and right-sided hyperexcitability, alongside a concurrent shift in the peripheral serum glutamate-GABA system. These objective neurophysiological and neurochemical alterations provide new evidence for understanding the pathophysiology of GAD and may serve as auxiliary references for future clinical evaluations. However, the direct relationship between these peripheral indicators and central nervous system function, their diagnostic specificity for GAD, and their clinical applicability require further verification through multimodal neuroimaging techniques and cross-diagnostic research designs.
Trial Registration Number
ChiCTR2200066311.
Data Sharing Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request. No digital information was obtained. Other information that could expose a participant’s identity will not be released. The data will be unavailable after 5 years.
Ethical Approval
This research was registered at the China Clinical Trial Center (No.ChiCTR2200066311) and received approval from the Medical Ethics Committee of Shenzhen Bao’an Traditional Chinese Medicine Hospital (No.KY-2022-035-01).
Funding
This research received support from Special Project of Shenzhen Science and Technology Innovation Commission (JSGG20220226090205008).
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–10. doi:10.1016/S0140-6736(20)30925-9. [published correction appears in Lancet. 2020 Nov 14;396(10262):1562]
2. Lakhawat SS, Mech P, Kumar A, et al. Intricate mechanism of anxiety disorder, recognizing the potential role of gut microbiota and therapeutic interventions. Metab Brain Dis. 2024;40(1):64. doi:10.1007/s11011-024-01453-1
3. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593–602. doi:10.1001/archpsyc.62.6.593
4. Fagan HA, Baldwin DS. Pharmacological Treatment of Generalised Anxiety Disorder: current Practice and Future Directions. Expert Rev Neurother. 2023;23(6):535–548. doi:10.1080/14737175.2023.2211767
5. Mishra AK, Varma AR. A Comprehensive Review of the Generalized Anxiety Disorder. Cureus. 2023;15(9):e46115. doi:10.7759/cureus.46115
6. Munir S, Takov V. Generalized Anxiety Disorder. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
7. Fowler K. Generalized Anxiety Disorder in Canadian Adults: to what Extent Might Social Support Subdomains and Negative Social Interactions Predict Psychological Distress? Psychiatr Q. 2023;94(4):655–673. doi:10.1007/s11126-023-10055-6
8. Dugas MJ, Giguère Marchal K, Cormier S, et al. Pain catastrophizing and worry about health in generalized anxiety disorder. Clin Psychol Psychother. 2023;30(4):852–861. doi:10.1002/cpp.2843
9. DeMartini J, Patel G, Fancher TL. Generalized Anxiety Disorder. Ann Intern Med. 2019;170(7):ITC49–ITC64. doi:10.7326/AITC201904020
10. Wittchen H-U, Jacobi F. Size and burden of mental disorders in Europe—a critical review and appraisal of 27 studies. Eur Neuropsychopharmacol. 2005;15(4):357–376. doi:10.1016/j.euroneuro.2005.04.012
11. Xue Y, Wang WD, Liu YJ, et al. Sleep disturbances in generalized anxiety Disorder: the central role of insomnia. Sleep Med. 2025;132:106545. doi:10.1016/j.sleep.2025.106545
12. Cardoner N, Gutiérrez-Rojas L, Saiz P, et al. Does pregabalin offer potential as a first-line therapy for generalized anxiety disorder? A meta-analysis of efficacy, safety, and cost-effectiveness. Front Pharmacol. 2025;16:1483770. doi:10.3389/fphar.2025.1483770
13. Matsuyama S, Otsubo T, Nomoto K, et al. Prevalence of Generalized Anxiety Disorder in Japan: a General Population Survey. Neuropsychiatr Dis Treat. 2024;20:1355–1366. doi:10.2147/NDT.S456272
14. Harandi AA, Kimia N, Medghalchi A, et al. Cerebral hemodynamic response to generalized anxiety disorder. Psychiatry Res Neuroimaging. 2023;333:111654. doi:10.1016/j.pscychresns.2023.111654
15. Wanyun Z, Jiayi Y, Qingyi Q, et al. Clinical observation of 60 cases of patients with liver depression and fire type generalized anxiety disorder treated with transcranial magnetic stimulation and psychological basic therapy combined with intradermal acupuncture. J Traditional Chin Med. 2025;66(01):50–58.
16. Ziemann U, Reis J, Schwenkreis P, et al. TMS and drugs revisited 2014. Clin Neurophysiol. 2015;126(10):1847–1868. doi:10.1016/j.clinph.2014.08.028
17. Jinxin T, Yuxin Z, Tong H, et al. Network Meta-analysis of different modes of transcranial magnetic stimulation intervention for adult refractory depression. Chin J Tissue Eng Res. 2025;29(35):7639–7648.
18. Matsumoto H, Ugawa Y. Central and Peripheral Motor Conduction Studies by Single-Pulse Magnetic Stimulation. J Clin Neurol. 2024;20(3):241–255. doi:10.3988/jcn.2023.0520
19. Loyd JO, Chisholm KI, Oehle B, et al. Cortical Mechanisms of Single-Pulse Transcranial Magnetic Stimulation in Migraine. Neurotherapeutics. 2020;17(4):1973–1987. doi:10.1007/s13311-020-00879-6
20. Wiesman AI, da Silva Castanheira J, Fon EA, et al. Alterations of Cortical Structure and Neurophysiology in Parkinson’s Disease Are Aligned with Neurochemical Systems. Ann Neurol. 2024;95(4):802–816. doi:10.1002/ana.26871
21. Beck MM, Christiansen L, Madsen MAJ, et al. Transcranial magnetic stimulation of primary motor cortex elicits an immediate transcranial evoked potential. Brain Stimul. 2024;17(4):802–812. doi:10.1016/j.brs.2024.06.008
22. Bajbouj M, Lisanby SH, Lang UE, et al. Evidence for impaired cortical inhibition in patients with unipolar major depression. Biol Psychiatry. 2006;59(5):395–400. doi:10.1016/j.biopsych.2005.07.036
23. Fengmin L, Heng Z, Xiangjun Z, et al. Site-directed mutagenesis improves the practical application of L-glutamic acid decarboxylase in Escherichia coli. Eng Life Sci. 2023;23(4):e2200064. doi:10.1002/elsc.202200064
24. An HE, Park HS, Yin CS. Association of sarcopenia with generalized anxiety disorder in Korean middle-aged and older adults: results from the Korea National Health and Nutrition Examination Survey in 2022. PLoS One. 2025;20(5):e0323772. doi:10.1371/journal.pone.0323772
25. Glick C, Gajawelli N, Sun Y, et al. Concurrent single-pulse (sp) TMS/fMRI to reveal the causal connectome in healthy and patient populations. bioRxiv. 2024;2024:614833.
26. Maeda F, Keenan JP, Pascual-Leone A. Interhemispheric asymmetry of motor cortical excitability in major depression as measured by transcranial magnetic stimulation. Br J Psychiatry. 2000;177:169–173. doi:10.1192/bjp.177.2.169
27. Ping Z. Study on the Brain Function Regulation and Mechanisms of Electroacupuncture and Transcranial Direct Current Stimulation Based on Cortical Excitability. Shanghai University of Traditional Chinese Medicine; 2019.
28. Bingyou L, Guiyun J, Rongjiang J, et al. Mechanism study of sertraline combined with repetitive transcranial magnetic stimulation in the treatment of persistent somatoform pain disorder based on the theory of functional asymmetry of the cerebral hemisphere. Chin J Rehabil Med. 2018;33(08):934–939.
29. Duque J, Hummel F, Celnik P, et al. Transcallosal inhibition in chronic subcortical stroke. Neuroimage. 2005;28(4):940–946. doi:10.1016/j.neuroimage.2005.06.033
30. Luscher B, Fuchs T, Kilpatrick CL. GABAA receptor trafficking-mediated plasticity of inhibitory synapses. Neuron. 2011;70(3):385–409. doi:10.1016/j.neuron.2011.03.024
31. Nuss P. Anxiety disorders and GABA neurotransmission: a disturbance of modulation. Neuropsychiatr Dis Treat. 2015;11:165–175. doi:10.2147/NDT.S58841
32. Maddock RJ, Buonocore MH. MR spectroscopic studies of the brain in psychiatric disorders. Curr Top Behav Neurosci. 2012;11:199–251.
33. Houtepen LC, Schür RR, Wijnen JP, et al. Acute stress effects on GABA and glutamate levels in the prefrontal cortex: a 7T 1H magnetic resonance spectroscopy study. Neuroimage Clin. 2017;14:195–200. doi:10.1016/j.nicl.2017.01.001
34. van Loon AM, van den Wildenberg WP, van Stegeren AH, et al. Emotional stimuli modulate readiness for action: a transcranial magnetic stimulation study. Cogn Affect Behav Neurosci. 2010;10(2):174–181. doi:10.3758/CABN.10.2.174
35. Liu H, Wang L, Tan X, et al. Deficits in Emotional Perception-Related Motor Cortical Excitability in Individuals With Trait Anxiety: a Transcranial Magnetic Stimulation Study. Depress Anxiety. 2024;2024:5532347. doi:10.1155/2024/5532347
36. Theodore WH. Transcranial magnetic stimulation in epilepsy. Epilepsy Curr. 2003;3(6):191–197. doi:10.1046/j.1535-7597.2003.03607.x
37. Madsen MAJ, Christiansen L, Chung C, et al. Single and paired TMS pulses engage spatially distinct corticomotor representations in human pericentral cortex. J Neurophysiol. 2025;133(5):1423–1434. doi:10.1152/jn.00459.2024
38. Guerra A, Asci F, D’Onofrio V, et al. Enhancing Gamma Oscillations Restores Primary Motor Cortex Plasticity in Parkinson’s Disease. J Neurosci. 2020;40(24):4788–4796. doi:10.1523/JNEUROSCI.0357-20.2020
39. Ruhland S, Poeppl TB, Schoisswohl S, et al. Motor-evoked potentials as biomarkers for sexual arousal? J Sex Med. 2024;21(11):1004–1010. doi:10.1093/jsxmed/qdae122
40. Gökdemir S, Gündüz A, Özkara Ç, et al. Fear-conditioned alterations of motor cortex excitability: the role of amygdala. Neurosci Lett. 2018;662:346–350. doi:10.1016/j.neulet.2017.10.059
41. Nemeroff CB. The role of GABA in the pathophysiology and treatment of anxiety disorder. Psychopharmacol Bull. 2003;37(4):133–146. doi:10.64719/pb.4169
42. Chaves EMC, Honório-Júnior JER, Sousa CNS, et al. The anxiolytic-like effect of 6-styryl-2-pyrone in mice involves GABAergic mechanism of action. Metab Brain Dis. 2018;33(1):139–149. doi:10.1007/s11011-017-0139-5
43. Wang C, Gong B, Liu Y, et al. Agarwood essential oil inhalation exerts antianxiety and antidepressant effects via the regulation of Glu/GABA system homeostasis. Biomed Rep. 2023;18(2):16. doi:10.3892/br.2023.1598
44. Hartmann J, Dedic N, Hlmann ML, et al. Forebrain glutamatergic, but not GABAergic, neurons mediate anxiogenic effects of the glucocorticoid receptor. Mol Psychiat. 2016;22(3):466–467.
45. Lener MS, Niciu MJ, Ballard ED, et al. Glutamate and Gamma-Aminobutyric Acid Systems in the Pathophysiology of Major Depression and Antidepressant Response to Ketamine. Biol Psychiatry. 2017;81(10):886–897. doi:10.1016/j.biopsych.2016.05.005
46. Ren Z, Pribiag H, Jefferson SJ, et al. Bidirectional Homeostatic Regulation of a Depression-Related Brain State by Gamma-Aminobutyric Acidergic Deficits and Ketamine Treatment. Biol Psychiatry. 2016;80(6):457–468. doi:10.1016/j.biopsych.2016.02.009
47. Wierońska JM, Stachowicz K, Nowak G, et al. The Loss of Glutamate-GABA Harmony in Anxiety Disorders. Anxiety Disorders. 2011;8(24):135–158.
48. Cotovio G, Rodrigues da Silva D, Real Lage E, et al. Hemispheric asymmetry of motor cortex excitability in mood disorders - Evidence from a systematic review and meta-analysis. Clin Neurophysiol. 2022;137:25–37. doi:10.1016/j.clinph.2022.01.137
49. Barros-Barbosa AR, Oliveira Â, Lobo MG, Cordeiro JM, Correia-de-Sá P. Under stressful conditions activation of the ionotropic P2X7 receptor differentially regulates GABA and glutamate release from nerve terminals of the rat cerebral cortex. Neurochem Int. 2018;112:81–95. doi:10.1016/j.neuint.2017.11.005
50. Xu Y, Lian Y, Li J, et al. KangPiLao decoction modulates cognitive and emotional disorders in rats with central fatigue through the GABA/Glu pathway. Front Pharmacol. 2022;13:939169. doi:10.3389/fphar.2022.939169
51. Xiaoxiao H, Zhongli X, Mengyue X, et al. Exploring the mechanism of Qinggong Decoction against generalized anxiety disorder based on Glu/GABA metabolic balance. Chin J Experiment Formulae. 2024;30(24):28–35.
52. Yu W, Wang L, Yang L, et al. Activation of LXRβ Signaling in the Amygdala Confers Anxiolytic Effects Through Rebalancing Excitatory and Inhibitory Neurotransmission upon Acute Stress. Neurotherapeutics. 2020;17(3):1253–1270. doi:10.1007/s13311-020-00857-y
53. Klausberger T, Somogyi P. Neuronal diversity and temporal dynamics: the unity of hippocampal circuit operations. Science. 2008;321(5885):53–57. doi:10.1126/science.1149381
54. Bell TK, Craven AR, Hugdahl K, et al. Functional changes in GABA and Glutamate during motor learning. eNeuro. 2023;10(2):2373–2822. doi:10.1523/ENEURO.0356-20.2023
55. Wang M, Ho MS. Profiling neurotransmitter-evoked glial responses by RNA-sequencing analysis. Front Neural Circuits. 2023;17:1252759. doi:10.3389/fncir.2023.1252759
56. Ay H, Horata E, Öncü kaya EM, et al. Increased Serotonin Levels and Unchanged Glutamate and GABA Levels in Thalamic Microdialysates Despite Reduced Cell Numbers in a Valproic Acid-Induced Autism Model. Neurochem Res. 2024;50(1):45. doi:10.1007/s11064-024-04299-2
57. McKeon SD, Perica MI, Calabro FJ, et al. Prefrontal excitation/inhibition balance supports adolescent enhancements in circuit signal to noise ratio. Prog Neurobiol. 2024;243:102695. doi:10.1016/j.pneurobio.2024.102695
58. Mayeli A, Sonnenschein SF, Yushmanov VE, et al. Dorsolateral prefrontal cortex glutamate/gamma-aminobutyric acid(GABA)alterations in clinical high risk and first-episode schizophrenia:a preliminary 7-T magnetic resonance spectroscopy imaging study. Int J Mol Sci. 2022;23(24):1422–1467. doi:10.3390/ijms232415846
59. Sonnenschein SF, Mayeli A, Yushmanov VE. A longitudinal investigation of GABA, glutamate, and glutamine across the insula during antipsychotic treatment of first-episode schizophrenia. Schizophr Res. 2022;248:98–106. doi:10.1016/j.schres.2022.08.008
60. Mukerjee S, Gao H, Xu J, et al. ACE2 and ADAM17 Interaction Regulates the Activity of Presympathetic Neurons. Hypertension. 2019;74(5):1181–1191. doi:10.1161/HYPERTENSIONAHA.119.13133
61. Jiwu L, Sisi W, Haihua Y, et al. Comparative analysis of serum glutamate and gamma-aminobutyric acid levels in patients with bipolar disorder depressive episodes and depression. Chinese Med J. 2020;100(23):1800–1804. doi:10.3760/cma.j.cn112137-20191025-02319
62. Yujie Z. Detection value of serum Glu/GABA in patients with bipolar disorder depressive episodes. Modern Diagnosis Treatment. 2020;31(24):3932–3933.
63. Hawkins RA, O’Kane RL, Simpson IA, et al. Structure of the blood-brain barrier and its role in the transport of amino acids. J Nutr. 2006;136(1 Suppl):218S. doi:10.1093/jn/136.1.218S
64. Wise T, Taylor MJ, Herane-Vives A, et al. Glutamatergic hypofunction in medication-free major depression: secondary effects of affective diagnosis and relationship to peripheral glutaminase. J Affect Disord. 2018;234:214–219. doi:10.1016/j.jad.2018.02.059
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.