Back to Journals » Research and Reports in Urology » Volume 14
Alpha-Blocker Prescribing Trends for Ureteral Stones: A Single-Centre Study
Authors Qu LG ![]() , Chan G, Gani J
, Chan G, Gani J
Received 2 May 2022
Accepted for publication 4 August 2022
Published 29 August 2022 Volume 2022:14 Pages 297—303
DOI https://doi.org/10.2147/RRU.S372208
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Guglielmo Mantica
Liang G Qu,1,2,* Garson Chan,1– 3,* Johan Gani1,2,4
1Department of Urology, Austin Health, Heidelberg, Victoria, Australia; 2Department of Surgery, University of Melbourne, Melbourne, Victoria, Australia; 3Department of Surgery, Division of Urology, University of Saskatchewan, Saskatoon, SK, Canada; 4Department of Urology, Western Health, Footscray, Victoria, Australia
*These authors contributed equally to this work
Correspondence: Liang G Qu, Department of Urology, Austin Health, Heidelberg, Victoria, Australia, Tel +61 3 9496 5000, Email [email protected]
Purpose: Recommendations for alpha-blockers have shifted in the conservative management of ureteral stones. It is unknown whether real-life practices regarding alpha-blocker prescriptions reflect updates in evidence. This study aimed to characterise alpha-blocker prescriptions for conservatively managed ureteral stones and relate this to recent literature.
Methods: This was a retrospective audit, 01/01/2014 to 01/01/2019, of emergency acute renal colic presentations. Patients were included if they had a confirmed ureteral stone and were conservatively managed. The rates of alpha-blocker prescriptions were analysed using interrupted time-series analyses. May 2015 was selected as the cut-point to analyse before and after trend lines. Results were stratified by stone size and location. Tamsulosin and prazosin prescriptions were also compared.
Results: This study included 2163 presentations: 70.4% were stones ≤ 5 mm and 61.4% were proximal stones. Altogether, 24.7% of presentations were prescribed alpha-blockers. There was a fall in alpha-blocker prescription rates from before to after May 2015, regardless of stone size or location (p < 0.001). Since May 2015, however, there was a monthly rate increase of 0.5% for patients with stones > 5mm.
Conclusion: This study demonstrated a significant shift in rates of alpha-blocker prescriptions, possibly related to the influence of updates in available high-quality evidence.
Keywords: adrenergic alpha-antagonists, emergency medicine, renal colic, ureteric calculus
Plain Language Summary
There has been a shift in the evidence for using alpha-blockers for managing ureteric calculi over recent years. It is unclear if this change in research is reflected in practice. At our single institution, there was evidence of a shift in alpha-blocker prescribing practices, likely reflecting responsiveness to latest published high-quality literature in the field of renal colic. A difference in prescribing trends was not observed between proximal and distal stones. At our institution, prazosin prescriptions decreased relative to tamsulosin prescriptions, in later years of this study.
Introduction
Acute renal colic is a common emergency department (ED) presentation and may result in a trial of conservative management or plan for intervention. Stone disease is responsible for a significant impact on quality of life and presents a significant economic burden to health-care systems.1,2 Although several patient and stone factors influence the decision between management strategies,3–5 the choice and success of management plans is influenced by the use of adjunctive therapies such as alpha-blockers.6
The efficacy for alpha-blockers in ureteral stones has been extensively reported on and debated in recent years. Alpha-blockers are currently widely used, and was once previously recommended across all ureteric stones regardless of size or location.6 Subsequent recent evidence has put these recommendations into question.7–9 In particular, interest in publishing large-scale randomised-controlled trials (RCTs) has led to generating momentum for practitioners across the world to change prescribing for alpha-blockers in conservative management.6 Various high-quality studies report conflicting results, making interpretation difficult when it comes to real-life practice.
For instance, a RCT by Pickard et al suggested alpha-blockers demonstrated no benefit for both passage of stone or pain control. This lack of efficacy was shown regardless of stone location or stone size.7 A subsequent RCT by Furyk et al contrarily reported increase in stone passage for larger stones using tamsulosin compared to placebo.10 Systematic reviews have supported that a benefit may persist in certain stone subgroups.6,11,12 These conflicting conclusions from high-quality data make it difficult for clinicians to decide on appropriate practice for managing patients with ureteral stones.
It is currently unknown the extent of how real-life clinical practice is related to up-to-date literature and whether it reflects the evidence – and of note, the conflicting data varying between studies. Given the recent literature, this study sought to characterise trends in alpha-blocker prescriptions for patients presenting with ureteral stones in ED, and relate this to published literature.
Methods
This study was a retrospective audit conducted from 01/01/2014 to 01/01/2019, of ED presentations of acute renal colic, at a single institution. Data extraction involved all consecutive patient episodes with a coded diagnosis in ED for “acute renal colic” within the study time interval, producing 4320 events (Figure 1).
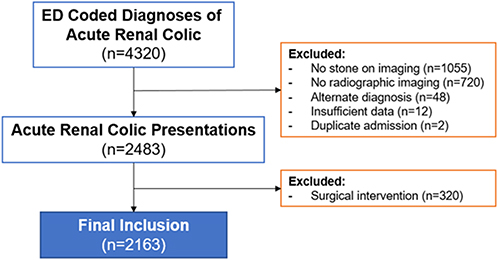 |
Figure 1 Study participant selection flowchart. Patients with acute renal colic presenting to emergency from 2014 to 2019 were extracted for data. Altogether, 2163 patients were included for final analysis. Abbreviation: ED, emergency department. |
Patients were included if they had radiographically confirmed ureteric calculi and were conservatively managed. Patients with multiple presentations were included, and each separate episode was analysed as a different entry. Radiographic imaging consisted of either: low-dose computerised tomography (CT), ultrasound, or X-ray. Imaging was required to be performed within 30 days of presentation. Conservative management was defined as a trial of spontaneous passage of the stone, with encouragement of increased fluid intake and offered prescription for analgesia with or without concurrent alpha-blockers. Patients were required to not be planned for subsequent surgical intervention at time of emergency department encounter, such as for stenting, nephrostomy, or ureteropyeloscopy. All patients undergoing trials of spontaneous passage were followed up in an outpatient setting with repeat imaging after 3 to 4 weeks. Regarding patient selection, study subjects elected for conservative management voluntarily after clinicians explained the various management options for obstructing ureteric calculi. Exclusion criteria included: misdiagnosis, insufficient data, or those who elected to undergo surgical intervention at the time of emergency presentation. A final count of 2163 presentations were included for this study.
Data were collected through extraction from the institutional electronic medical records system, on patient demographics, stone characteristics, and alpha-blocker prescriptions. Stone size was recorded as the maximal stone diameter reported by the radiologist, and this was then coded as a dichotomous variable of ≤5 mm or >5 mm, for reporting consistency alongside previous literature.7 Stone location was recorded and classified as either: “distal” (below level of sacro-iliac joint), or “proximal” (above sacro-iliac joint). Alpha-blockers prescribed by ED clinicians were recorded including the type of alpha-blocker – given the availability of medications in Australia, only tamsulosin or prazosin were prescribed.
This study was approved by the local human research ethics committee.
Statistical Analysis
Results were categorised primarily according to stones ≤5 mm or >5 mm. Chi-square and Wilcoxon rank-sum statistics compared groups, for age, sex, proportions of proximal versus distal stones, proportion receiving alpha-blockers, and use of imaging. Patients with missing field data were excluded from subsequent analyses.
The proportion of alpha-blocker prescriptions on discharge was analysed as a monthly time-series variable. Time-series variables were stratified by stone size ≤5 mm or >5 mm, and by proximal or distal stone location. A moving average smoothing function was applied (lag:current:lead = 1:1:1) to improve graph visualisation and reduce month-to-month variability.
It was expected that there would be a sharp decline in alpha-blocker prescriptions from May 2015, after evidence published at this time suggested lack of efficacy.7 Interrupted time-series analyses (ITSAs) were therefore conducted to assess for changes in level and trend before and after this time point, to highlight the potential effect towards clinical practice. Segmented ordinary least-squares regression models were used, with Newey-West standard errors calculated to adjust for autocorrelation. Comparison was not made between the different subgroups due to the anticipated difference in baseline levels and trends prior to May 2015.
Throughout this study, statistical significance was defined as p-value of <0.05. All statistical calculations were performed using StataIC v15.1 (Stata Statistical Software: Release 15. College Station, TX, USA: StataCorp LLC). The ITSA package by Linden et al was utilised in this study.13
Results
Altogether, 2163 acute renal colic presentations were included (median age: 50 years, 78.3% men) (Figure 1). Median number of presentations per year was 455 (range: 362–463). In total, 1530 patient episodes (70.4%) were of stones ≤5 mm, and 1327 (61.4%) were proximal stones (Table 1). Patients with stones >5 mm were more likely to have a proximal stone (74.6% vs 55.9%, p < 0.001). Alpha-blockers were prescribed in 534 (24.7%) episodes. Patients with stones >5mm were more likely to be prescribed alpha-blockers (33.2% vs 21.2%, p < 0.001). The majority of patients underwent CT as their diagnostic imaging (n = 2029, 93.8%).
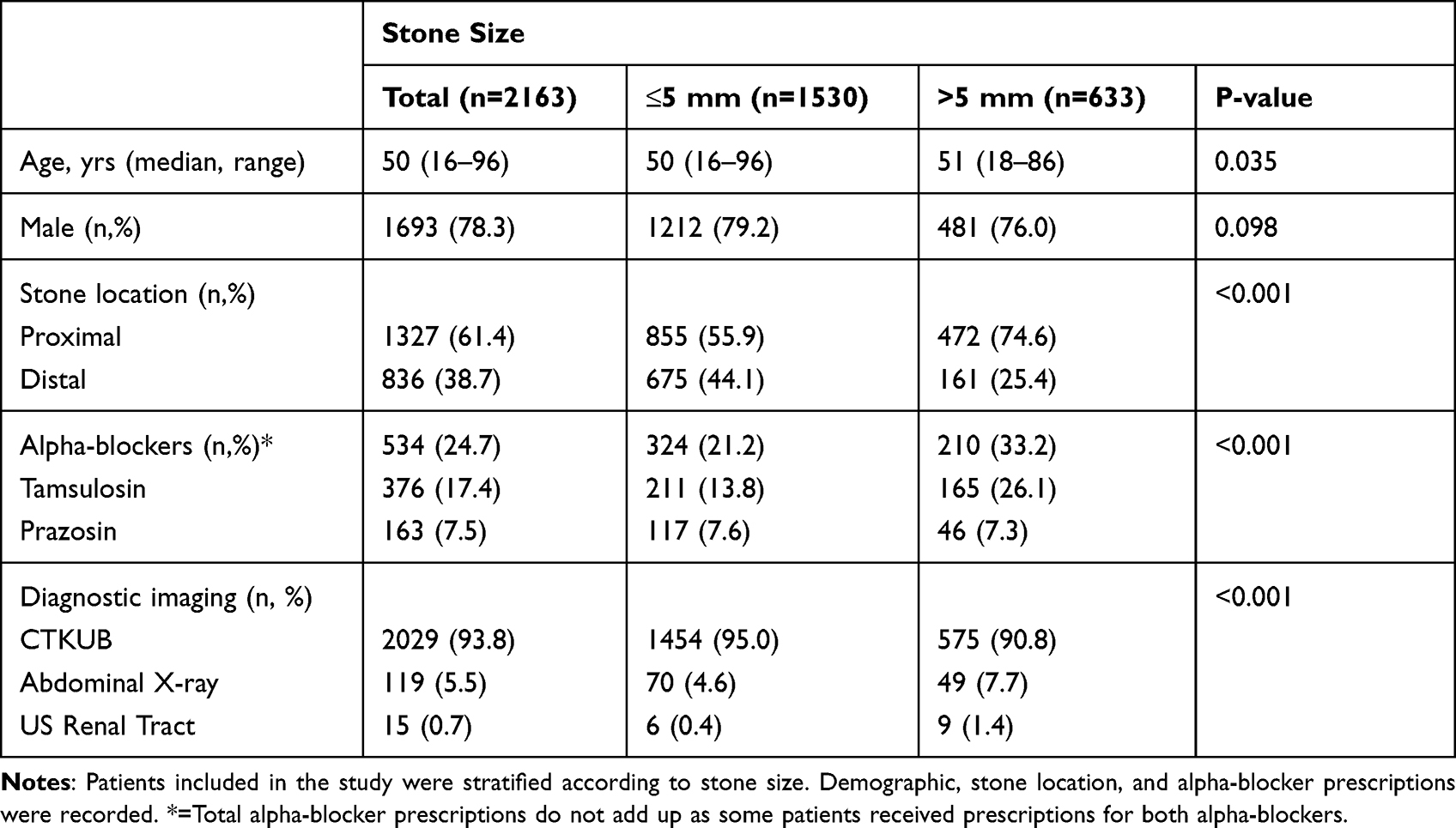 |
Table 1 Participant Baseline Characteristics |
Analysis by Stone Size
Proportion of alpha-blocker prescriptions was analysed as a time-series variable, stratified by stone size. On visual inspection, a sharp decline in alpha-blocker usage in all stone sizes was observed in May 2015 (Figure 2). For patients with stones >5 mm, there were local peaks in prescriptions in March 2016 (44.4%), February 2018 (49.7%), and subsequently December 2018 (56.3%). Meanwhile, proportions for stones ≤5 mm after May 2015 demonstrated consistently low rates of alpha-blocker prescription.
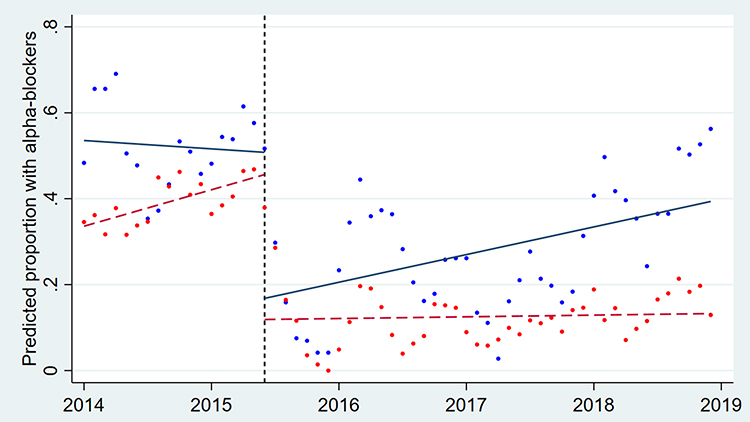 |
Figure 2 Interrupted time-series analyses for conservatively managed ureteral stones, by stone size. Patients with obstructing ureteric calculi of ≤5 mm [red] or >5 mm [blue] were assessed for rates of alpha-blocker prescriptions, with predicted trend lines shown. A sharp decline in overall prescriptions [vertical line] was observed in May 2015 across all subgroups, potentially related to published evidence at that time. |
Formal ITSAs were conducted (Table 2). For stones >5 mm, 53.5% of patients were prescribed alpha-blockers initially. At May 2015, there was a significant drop in level by 34.0% (p < 0.001). Despite the sudden drop, however, after May 2015, the monthly alpha-blocker prescription rate gradually rose by 0.5% per month thereafter (p = 0.035). For stones ≤5 mm, approximately 33.6% of patients were prescribed alpha-blockers initially. At May 2015, there was a significant drop in level by 33.7% (p < 0.001). Despite the sudden drop, however, after May 2015, there was a gradual trending decrease of 0.7% per month thereafter (p = 0.004).
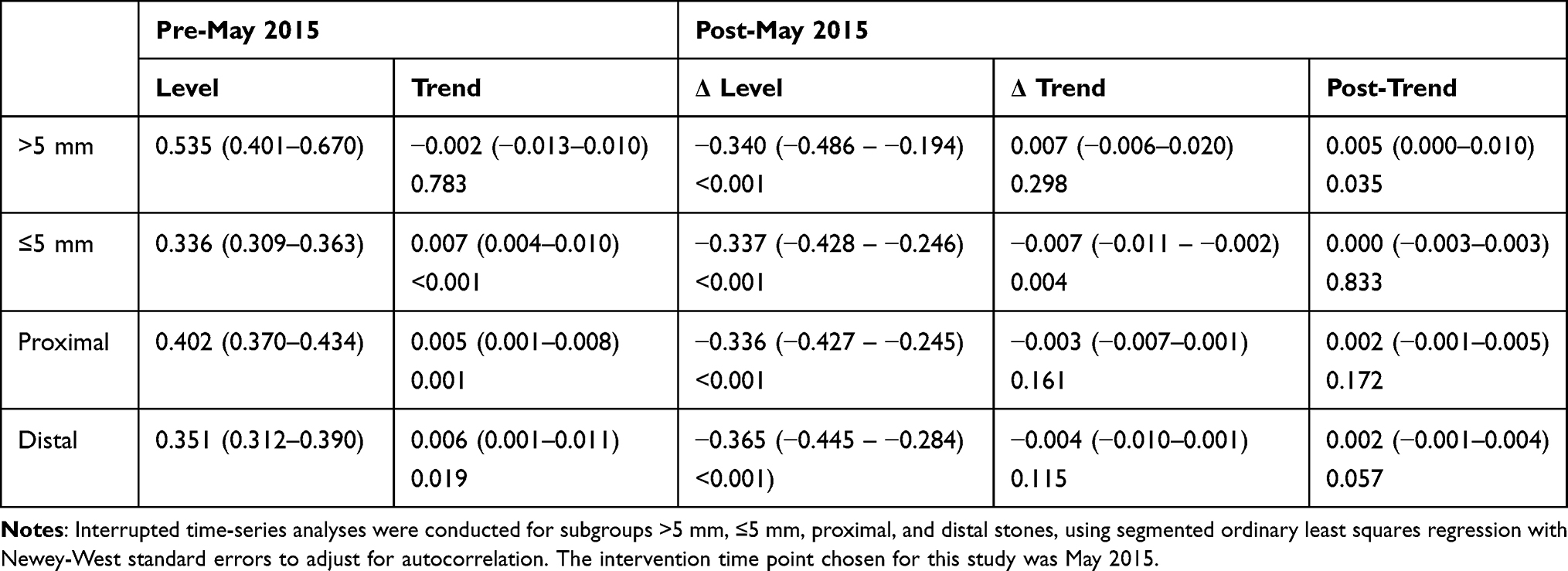 |
Table 2 Interrupted Time-Series Analyses for Stone Size and Stone Location Subgroups |
Analysis by Stone Location
Proportion of alpha-blocker prescriptions was analysed as a time-series variable, stratified by stone location. On visual inspection, there was a sharp decline in alpha-blocker usage in both subgroups observed in May 2015 (Figure 3).
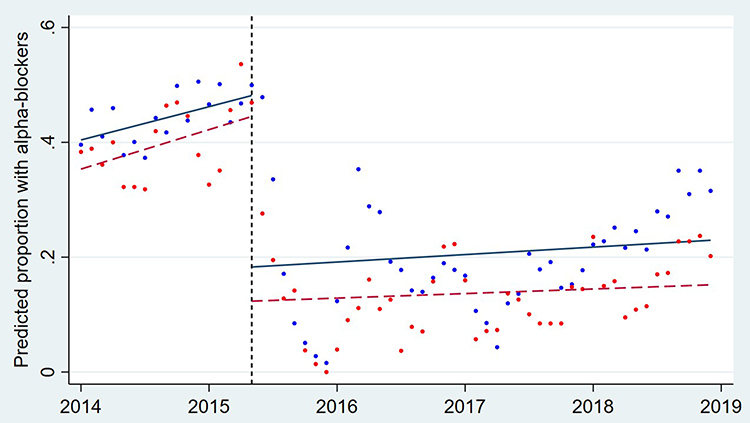 |
Figure 3 Interrupted time-series analyses for conservatively managed ureteral stones, by stone location. Patients with obstructing ureteric calculi, either proximal [blue] or distal [red] stones were assessed for rates of alpha-blocker prescriptions, with predicted trend lines shown. |
ITSAs were conducted to compare alpha-blocker prescriptions by stone location (Table 2). Alpha-blocker prescriptions for proximal stones demonstrated an initial proportion of 40.2%. A significant drop in proportion of 33.6% (p < 0.001) was observed at May 2015. For alpha-blocker prescriptions for distal stones, there was an initial proportion of 35.1%. A significant drop of 36.5% was observed in May 2015 (p < 0.001).
Discussion
In this study, alpha-blocker prescriptions for conservatively managed ureteric stones were characterised. This was a hypothesis-generating investigation to understand trends and how published literature may influence them, using May 2015 as an analysis time point. This study demonstrated a significant drop in alpha-blocker prescription for stones of all subgroup categories, including by stone size and by stone location.
The primary finding of this study was the sharp decrease in alpha-blocker prescription from May 2015. At this particular time point, the landmark RCT published in The Lancet by Pickard et al reported on the lack of effect of tamsulosin for improving stone clearance at four weeks.7 Despite sub-analysis by stone location or size, the authors reported no sub-group demonstrated improvements in any outcome with tamsulosin. Although other explanations may contribute to our findings observed in May 2015, it is likely that observant clinicians at our institution were able to implement changes to clinical practice and quickly adapt.
Despite the sudden drop in May 2015, there was a gradual rise in alpha-blocker usage again for stones >5 mm from May 2015 onwards, observed in our institution. This may be reflective of other studies that contributed to the subsequent increasing trend. A RCT in 2016 examined efficacy in larger stones.10 Furyk et al reported patients with stones of 5–10 mm experienced a higher likelihood of stone passage at 28 days with tamsulosin compared to placebo (83% vs 61%, p = 0.03). The further increase in alpha-blocker usage in early 2018 may also be contributed to by a study by Ye et al. The authors reported on the significantly higher expulsion rate with tamsulosin for stones >5 mm (odds ratio: 2.05, p < 0.001).14 Efficacy of tamsulosin for stones >5 mm was also demonstrated by the shorter time to expulsion, lower requirement for analgesics, and significant relief of renal colic. These studies may have continued the interest to clinicians for the growing support for tamsulosin therapy.
This study primarily served as a hypothesis-generating piece to suggest how literature influences practice, and various limitations exist. The ITSA employed in this study was limited to the study of only one intervention time point, when in reality, alpha-blocker prescription trends vary by a multiple number of potential factors. Furthermore, there may be additional influence by the implementation of local guidelines that may affect prescribing practices, and this is not examined here. The total number of physicians involved across all patient episodes was not examined due to limitations of the medical records, but this would be important to assess for trends over time as a potential confounder. The inclusion of patients with multiple presentations was for increasing the sensitivity and capture alpha-blockers prescribed at any presentations, whilst acknowledging that this may “dilute” our findings. The variability in diagnostic imaging modalities also influence the accuracy of stone characteristics recorded, where CT is generally considered the gold standard.15 However, patients in this audit were predominantly diagnosed through the use of CT scans (93.8%), and exclusion of non-CT patients was not done to reduce selection bias. Selection bias does however remain due to the retrospective single-centre study design, and not all variables were captured, such as baseline comorbidities,16 preadmission alpha-blocker usage or variations in clinician training. This single-centre study may also have limited generalisability to other health-care services, where clinician education and practice may vary. Nevertheless, this analysis suggests prescribing practices are associated and potentially responsive to updates in literature in the conservative management of patients with ureteral stones.
Conclusion
In this study, the effect of published literature on practice has been examined. In May 2015, a sharp drop in alpha-blocker prescriptions was observed. However subsequently, a steady increase in prescriptions for stones >5 mm followed. Future studies should investigate the difference in trends between stone size and location subgroups.
Abbreviations
ED, emergency department; ITSA, Interrupted time-series analysis; RCT, randomised-controlled trial.
Declarations
This study complies with the Declaration of Helsinki, and was approved by the Austin Health Human Research Ethics Committee (Audit/19/Austin/85).
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The authors declare no funding was used to support this study.
Disclosure
The authors declare no conflicts of interest relevant to this manuscript.
References
1. Maskal S, Jain R, Fedrigon D 3rd, Rose E, Monga M, Sivalingam S. The cost of operating room delays in an endourology center. Can Urol Assoc J. 2020;14(7):E304–E8. doi:10.5489/cuaj.6099
2. Liu Y, Chen Y, Liao B, et al. Epidemiology of urolithiasis in Asia. Asian J Urol. 2018;5(4):205–214. doi:10.1016/j.ajur.2018.08.007
3. Deng T, Chen Y, Liu B, et al. Systematic review and cumulative analysis of the managements for proximal impacted ureteral stones. World J Urol. 2019;37(8):1687–1701. doi:10.1007/s00345-018-2561-7
4. Shah TT, Gao C, Peters M, et al. Factors associated with spontaneous stone passage in a contemporary cohort of patients presenting with acute ureteric colic: results from the Multi-centre cohort study evaluating the role of Inflammatory Markers in patients presenting with acute ureteric Colic (MIMIC) study. BJU Int. 2019;124(3):504–513. doi:10.1111/bju.14777
5. Jain R, Maskal S, Milk J, Kahn L, Fedrigon D 3rd, Sivalingam S. Utility of stone volume estimated by software algorithm in predicting success of medical expulsive therapy. Can Urol Assoc J. 2020;15(3). doi:10.5489/cuaj.6491
6. Campschroer T, Zhu X, Vernooij RW, Lock MT. Alpha‐blockers as medical expulsive therapy for ureteral stones. Cochrane Database Syst Rev. 2018;2018(4). doi:10.1002/14651858.CD008509.pub3
7. Pickard R, Starr K, MacLennan G, et al. Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial. Lancet. 2015;386(9991):341–349. doi:10.1016/S0140-6736(15)60933-3
8. Meltzer AC, Burrows PK, Wolfson AB, et al. Effect of tamsulosin on passage of symptomatic ureteral stones: a randomized clinical trial. JAMA Intern Med. 2018;178(8):1051–1057. doi:10.1001/jamainternmed.2018.2259
9. Portis AJ, Portis JL, Borofsky MS, Neises SM. Beyond medical expulsive therapy: evolution to supported stone passage for ureteric stones. BJU Int. 2019;123(4):661–668. doi:10.1111/bju.14491
10. Furyk JS, Chu K, Banks C, et al. Distal ureteric stones and tamsulosin: a double-blind, placebo-controlled, randomized, multicenter trial. Ann Emerg Med. 2016;67(1):86–95. e2. doi:10.1016/j.annemergmed.2015.06.001
11. Wang RC, Smith-Bindman R, Whitaker E, et al. Effect of tamsulosin on stone passage for ureteral stones: a systematic review and meta-analysis. Ann Emerg Med. 2017;69(3):353–61 e3. doi:10.1016/j.annemergmed.2016.06.044
12. Cui Y, Chen J, Zeng F, et al. Tamsulosin as a medical expulsive therapy for ureteral stones: a systematic review and meta-analysis of randomized controlled trials. J Urol. 2019;201(5):950–955. doi:10.1097/JU.0000000000000029
13. Linden A. Conducting interrupted time-series analysis for single-and multiple-group comparisons. Stata J. 2015;15(2):480–500. doi:10.1177/1536867X1501500208
14. Ye Z, Zeng G, Yang H, et al. Efficacy and safety of tamsulosin in medical expulsive therapy for distal ureteral stones with renal colic: a multicenter, randomized, double-blind, placebo-controlled trial. Eur Urol. 2018;73(3):385–391. doi:10.1016/j.eururo.2017.10.033
15. Hanqi L, Fucai T, Caixia Z, Shuman Z, Guohua Z, Zhaohui H. Limited sensitivity and size over measurements of ultrasound affect medical decisions for ureteral stone compared to non-contrasted computed tomography. World J Urol. 2019;37(5):907–911. doi:10.1007/s00345-018-2444-y
16. Hesswani C, Iqbal S, Zand KR, et al. Identifying risk factors for development of nephrolithiasis in end-stage renal disease patients. Can Urol Assoc J. 2020;14(5):E185–E90. doi:10.5489/cuaj.6017
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.