Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Allergy – Patients with Atopic Dermatitis Express Themselves Through a Questionnaire
Authors Shourick J, Taïeb C ![]() , Seite S
, Seite S ![]()
Received 23 October 2020
Accepted for publication 8 December 2020
Published 5 January 2021 Volume 2020:13 Pages 1075—1077
DOI https://doi.org/10.2147/CCID.S285943
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Jason Shourick,1 Charles Taïeb,2 Sophie Seite3
1Département Epidémiologie, Hôpital de Toulouse, Toulouse, France; 2Patients Priority Department, European Market Maintenance Assessment, Fontenay Sous-bois, France; 3La Roche-Posay Dermatological Laboratories, Levallois Perret, France
Correspondence: Charles Taïeb
Patients Priority Department, European Market Maintenance Assessment, Fontenay Sous-bois, France
Tel +00 33 771772100
Email [email protected]
Introduction: Allergies are becoming more prevalent across the globe and can be linked to several skin diseases, particularly atopic dermatitis (AD). Disruption of the immune system in the skin can lead to inflammatory diseases such as atopic and contact dermatitis, skin infections, and allergies. This is especially evident in processes such as “atopic march”, where in childhood, the development of atopic dermatitis can later lead to food allergies, allergic rhinitis and asthma.
Objective: The aim of this international online survey is to study the link between self-reported doctor-diagnosed AD and allergy prevalence.
Methodology: Our survey queried a representative sample of the general population over the age of 18 from five countries (Brazil, China, Russia, the USA and France).
Results: A total of 9399 participants answered the entire online questionnaire. Among them, 2483 (26.4%) had an allergy diagnosed by a doctor (1243 with food allergies (13.2%), 1564 with respiratory allergies (16.6%) and 1669 with skin allergies (17.7%)). There were 794 (31.9%) participants with current AD in the allergy group and 640 (9.25%) in the group without allergies (p< 0.001), and there were 1299 (52.3%) participants with CAD in the allergy group versus 1368 (19.8%) in the group without allergies (p< 0.001). Multivariate analysis showed ORs of 3.24 [2.98, 3.63] (p< 0.001) for current AD and 2.4 [2.09, 2.74] (p< 0.001) for CAD. There was no significant interaction between AD and CAD (p=0.6).
Conclusion: A total of 26.4% of survey respondents reported having doctor-diagnosed allergies. Among these patients, half reported having AD during childhood, and 1/3 reported having a current AD. CAD and AD patients clearly have a higher risk of having an allergy than patients without CAD or AD.
Keywords: allergy, atopic dermatitis, patient centricity
Introduction
Allergies are becoming more prevalent across the globe and can be linked to several skin diseases, particularly atopic dermatitis (AD).1 While the cause of this increase is not entirely clear, it has been attributed to factors such as stress, use of antibiotics, poor nutrition, growing up in clean and urban homes and exposure to environmental pollution.2 It has been known for some time that the skin barrier plays a critical role in excluding allergens, irritants, and pathogens that have the potential to disrupt the immune system and cause allergic sensitization.2 Disruption of the immune system in the skin can lead to inflammatory diseases such as atopic and contact dermatitis, skin infections, and allergies. This is especially evident in processes such as “atopic march”, where in childhood, the development of atopic dermatitis can later lead to food allergies, allergic rhinitis and asthma.3
The aim of this international online survey is to study the link between self-reported doctor-diagnosed AD and allergy prevalence.
Methodology
Our study queried a representative sample of the general population over the age of 18 from five countries (Brazil, France and Russia: n=2000; United States: n=2050; China: n=3050). Participants were selected with the use of a stratified random sampling method from a database including several million Internet users who agreed to participate in various panel surveys.4
All participants were asked to complete a structured digital questionnaire. Because this study used completely anonymized data and did not involve patient contact, institutional review board approval was not required.
However, before answering the questionnaire, each respondent was informed of the nature of the survey, that anonymity would be respected and that no collected information would allow any identification.
The respondents could stop answering the questionnaire at the time of their choice without any explanation.
By answering the questionnaire, the respondent confirmed his or her agreement, and completion of the survey was deemed to be informed consent.
After collecting sociodemographic information, questions were asked about the presence of allergies and atopic dermatitis either currently (AD) or during childhood (CAD). Participants were then asked about the type of allergy they had and whether the allergy was diagnosed by a doctor. We defined an allergy patient only as a patient who had been diagnosed by a doctor. We then used global allergy and each type of allergy as the outcomes of univariate and multivariate logistic regression, adjusting for age and sex. We tested the presence of an interaction between childhood atopic dermatitis and/or current atopic dermatitis and allergy.
Results
A total of 9399 participants answered the entire online form (4787 women, age 40.9 ± 14.5). Among them, 2483 (26.4%) had an allergy diagnosed by a doctor (1243 with food allergies (13.2%), 1564 with respiratory allergies (16.6%) and 1669 with skin allergies (17.7%)). There were 794 (31.9%) participants with current AD in the allergy group and 640 (9.25%) in the group without allergies (p<0.001) and 1299 (52.3%) participants with CAD in the allergy group versus 1368 (19.8%) in the group without allergies (p<0.001).
Multivariate analysis for all allergies showed an odds ratio (OR) of 3.24 [2.98, 3.63] (p<0.001) for current AD and an OR of 2.4 [2.09, 2.74] (p<0.001) for CAD. There was no significant interaction between AD and CAD (p=0.6) (Table 1). The multivariate analysis with respiratory allergy as an outcome showed ORs of 3.51 [3.07, 4.01] for CDA and of 2.25 [1.95, 2.6] for current DA, without interaction (p=0.8) (Table 2). For food and skin allergies, there was a significant interaction between DA and CDA (p=0.004 for food allergies and p=0.009 for skin allergies). Therefore, we presented the results in four groups. For food allergies having neither AD nor CAD (N=6464, 68.7%) as the reference group, for AD without CAD (N=1166, 12.4%), the OR was 3.58 [2.56, 4.91] (p<0.001); for CAD without AD (N=1501, 15.9%), the OR was 4.65 [3.97, 4.46] (p<0.001); and for AD and CAD (N=268, 2.85%), the OR was 9.69 [8.27, 11.36] (p<0.001) (Table 3). For skin allergies having neither AD nor CAD as the reference group, for AD without CAD, the OR was 4.25 [3.17, 5.663] (p<0.001); for CAD without AD, the OR was 5.02 [4.34, 5.81]; and for AD and CAD, the OR was 13.8 [11.9, 16] (Table 4).
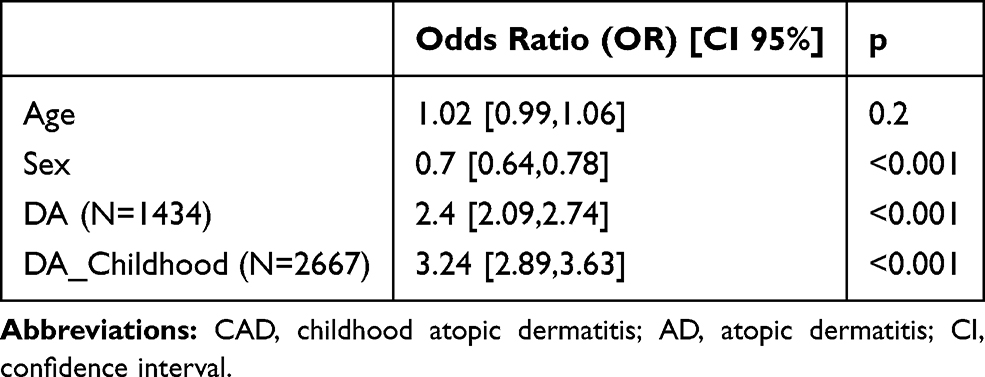 |
Table 1 Multivariate Analysis of the Association Between Any Allergy and Atopic Dermatitis |
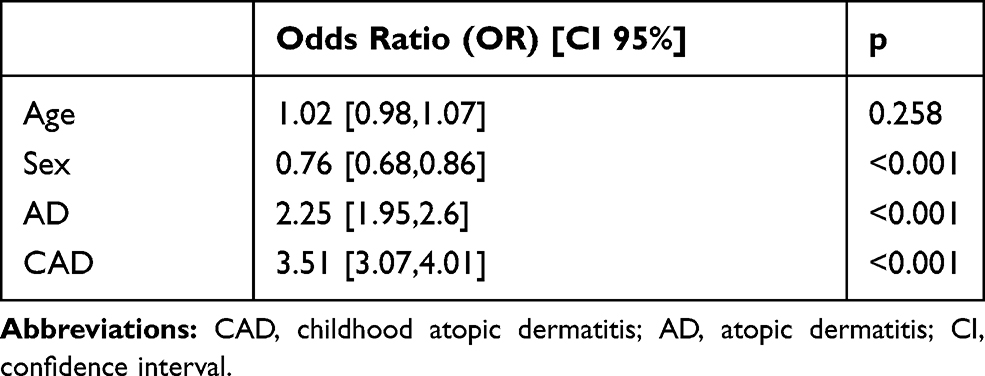 |
Table 2 Multivariate Analysis of the Association Between Respiratory Allergy and Atopic Dermatitis |
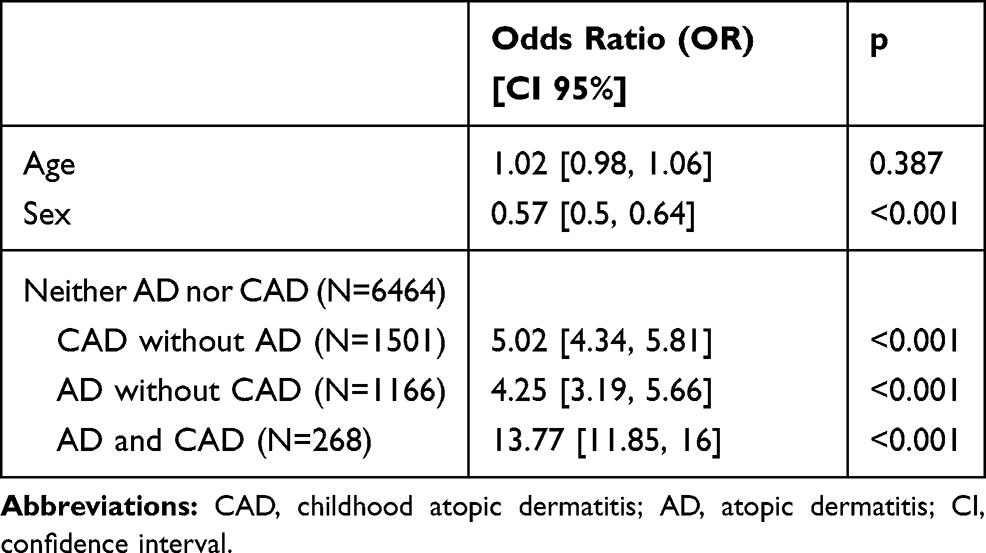 |
Table 3 Multivariate Analysis of the Association Between Food Allergies and Atopic Dermatitis |
 |
Table 4 Multivariate Analysis of the Association Between Skin Allergies and Atopic Dermatitis |
Conclusion
In this self-reported survey of a representative sample of the general populations of 5 different countries (Brazil, China, Russia, the USA and France), 26.4% of the survey respondents reported having doctor-diagnosed allergies. Among these patients, half reported having AD during childhood, and 1/3 reported having a current DA. These patients clearly have a higher risk of having an allergy than patients without CAD or AD. This is particularly true for allergies as a whole and for respiratory allergies where CAD and AD are independent risk factors for having an allergy. This confirmed the importance of the “atopic march” and the need for close follow-up by dermatologists of patients with CAD and AD (because there is a strong relationship between CAD and AD) to minimize their risk of developing allergies later in life. Furthermore, AD is frequently treated with corticosteroids, and minimizing skin barrier dysfunction may be one way to prevent future allergies.
Nevertheless, CAD and current AD are not the only risk factors for developing allergies; 44.1% of patients with diagnosed allergies have neither CAD nor current AD. Allergies can develop via transcutaneous sensitization; thus, taking care of primary barrier deficiency in at least some individuals with sensitive skin is of primary importance to limit the prevalence of allergies across the globe.2
With the rising prevalence of allergies, it is increasingly important to better characterize their nature and implications. Until the pathogenesis is fully understood, the skin and its barrier function remain important targets for preventive and curative strategies.
Funding
La Roche-Posay Dermatological Laboratories, France.
Disclosure
S. Seité is an employee of La Roche-Posay, France. The authors report no other conflicts of interest in this work.
References
1. Nettis E, Ortoncelli M, Pellacani G, et al. A multicentric study on prevalence of clinical patterns and clinical phenotypes in adult atopic dermatitis. J Investig Allergol Clin Immunol. 2020;30(6). doi:10.18176/jiaci.0519.
2. Strugar TL, Kuo A, Seité S, Lin M, Lio P. Connecting the dots: from skin barrier dysfunction to allergic sensitization, and the role of moisturizers in repairing the skin barrier. J Drugs Dermatol. 2019;18(6):581–586.
3. Bantz SK, Zhu Z, Zheng T. The atopic march: progression from atopic dermatitis to allergic rhinitis and asthma. J Clin Cell Immunol. 2014;5.
4. Seité S, Kuo AM, Taieb C, Strugar TL, Lio P. Self-reported prevalence of allergies in the USA and impact on skin-an epidemiological study on a representative sample of american adults. Int J Environ Res Public Health. 2020;17(10):3360. doi:10.3390/ijerph17103360
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.