Back to Journals » Journal of Asthma and Allergy » Volume 15
Allergen Management in Children with Type 2-High Asthma
Authors Gray-Ffrench M ![]() , Fernandes RM, Sinha IP, Abrams EM
, Fernandes RM, Sinha IP, Abrams EM
Received 3 December 2021
Accepted for publication 17 March 2022
Published 29 March 2022 Volume 2022:15 Pages 381—394
DOI https://doi.org/10.2147/JAA.S276994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Madeleine Gray-Ffrench,1 Ricardo M Fernandes,2,3 Ian P Sinha,4,5 Elissa M Abrams6,7
1University of Birmingham, Faculty of Medicine, Birmingham, UK; 2Clinical Pharmacology Unit, Faculty of Medicine and Instituto de Medicina Molecular, Universidade de Lisboa, Lisbon, Portugal; 3Department of Pediatrics, Hospital de Santa Maria, Centro Hospitalar Universitário de Lisboa Norte, Lisbon, Portugal; 4Alder Hey Children’s Hospital, Liverpool, UK; 5Department of Women’s and Children’s Health, Faculty of Health and Life Sciences, University of Liverpool, Liverpool, UK; 6Department of Pediatrics, Section of Allergy and Clinical Immunology, University of Manitoba, Winnipeg, Canada; 7Department of Pediatrics, Division of Allergy and Immunology, University of British Columbia, Vancouver, British Columbia, Canada
Correspondence: Elissa M Abrams, Department of Pediatrics, Section of Allergy and Clinical Immunology, University of Manitoba, FE125-685 William Avenue, Winnipeg, MB, R2A 5L9, Canada, Tel +1 204-255-7650, Fax +1 204-254-0730, Email [email protected]
Abstract: Children exposed to various indoor and outdoor allergens are placed at an increased risk of developing asthma in later life, with sensitization in these individuals being a strong predictor of disease morbidity. In addition, aeroallergen exposure influences asthma outcomes through an interplay with adverse determinants of health. The goal of this review is to provide an introductory overview of factors related to aeroallergen exposure in type 2-high childhood asthma. These include the relevance of exposure in asthma exacerbations and severity, and the evidence-base for avoidance and treatment for sensitization to these allergens. This review will focus on both indoor aeroallergens (house dust mite, pet, cockroach, mold, and rodent) and outdoor aeroallergens (pollens and molds). Treatment of aeroallergen sensitization in children with asthma includes avoidance and removal measures, although there is limited evidence of clinical benefit especially with single-strategy approaches. We will also address the interplay of aeroallergens and climate change, adverse social determinants, and the current COVID-19 pandemic, when we have seen a dramatic reduction in asthma exacerbations and emergency department visits among children. While there are many factors that are hypothesized to contribute to this reduction, among them is a reduced exposure to outdoor seasonal aeroallergens.
Keywords: asthma, aeroallergens, social determinants of health, COVID-19
Introduction
Asthma is one of the most common chronic conditions of childhood, impacting up to 10% of children in North America and over 7 million children in the United States.1–4 There is a substantial economic burden associated with asthma, with an estimated cost of $81.9 billion dollars in 2013 in the United States.5 In particular, poorly controlled asthma carries significant direct and indirect economic costs including healthcare utilization and school/work days lost.6
 |
Figure 1 There are three aspects to the cellular and chemical pathology of asthma: the epithelial and subepithelial response the subsequent inflammatory process; and the impact on airway mucus and bronchoconstriction. When children with asthma inhale an aeroirritant, there is a complex interplay of cells and chemical that is poorly understood. The main chemical players are called “alarmins”, and these link with cells such as Antigen-Presenting Cells and Dendritic Cells. These drive a shift in the types of T-cells that a person has. In most people with asthma there is an imbalance such that the undifferentiated T-helper cell (Th-0) is more likely to become a Th2, rather than Th1, cell. When this happens, people are said to have “Type 2-high” asthma; this is the usual phenotype in children. There are two main asthma endotypes in children with Type 2-high asthma - the eosinophilic pathway, and the IgE-mediated pathway. The key chemicals that drive these pathways include Interleukin 4/13 and Interleukin-5. Children exhibit these pathways and endotypes to varying degrees. There are other aspects of the pathogenesis, such as Th-17, which promote non-Type 2 inflammation. The consistent driver in children with Type 2-high asthma is that avoidance of aeroirritants in the first place significantly reduces the inflammatory load. |
Recognition of asthma heterogeneity across age ranges has led to the identification of Clinical and/or data-driven clusters of patients with similar observable traits (phenotypes) and increasing research on possible underlying pathophysiological and molecular mechanisms (endotypes).7,8 Whilst many challenges remain in disentangling the causal pathways, stability and implications of asthma heterogeneity, childhood asthma is mostly driven by type 2-high allergen-associated airway inflammation, albeit this may not be the case across levels of severity and treatment (Figure 1).9,10
Environmental allergies are the best predictor of persistence of asthma throughout childhood.2 In addition, exposure to aeroallergens in those who are sensitized is a significant cause of asthma exacerbations in children with asthma.11 The National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group (NAEPP) recommends allergy testing for aeroallergens (in particular indoor aeroallergens) in those with asthma who require daily anti-inflammatory therapy.12 However, the role of allergen avoidance as a general strategy in children with asthma remains controversial.2 The role of immunotherapy (both subcutaneous and sublingual) in asthma management is also an evolving conversation.2
There is an increasing recognition that the exposure to aeroallergens is and will continue to be impacted by key drivers of an era of global change such as climate change, evolving lifestyles and the current COVID-19 pandemic. Importantly, its consequences are most felt by those facing adverse social determinants of health.13,14 In addition, allergen exposure needs to be placed in the context of the multifactorial nature of asthma exacerbations and outcomes, in particularly given the major role of viral infections, as wells as other contributing factors such as microbiome and genetics.
The goal of this introductory review are to (i) explore the state of the art on the relevance of exposure to various indoor and outdoor aeroallergens in asthma exacerbations and severity; (ii) to briefly describe the evidence-base for avoidance and treatment for sensitization to these allergens, and (iii) to address the impact of climate change, adverse social determinants, and the current COVID-19 pandemic on allergen exposure.
Allergens and Asthma Outcomes
Indoor Allergens
Children exposed to various indoor allergens are placed at an increased risk of developing asthma in later life, with sensitization in these individuals being a strong predictor of disease morbidity.15–18 Common indoor exposures for infants include house dust mite, pet, cockroach, mold and rodent allergens.18 Sensitization to at least one indoor allergen, has been demonstrated to be present in 9 out of every 10 children Hospitalised with asthma.19,20
Recently, there has been a behavioural shift in modern society/families towards spending more time indoors, thereby increasing the amount of allergen exposure for children.21,22 To add to this, the current climate of the ongoing COVID19 pandemic has seen a huge increase in time spent at home due to lockdowns/quarantine. There is also growing evidence to suggest children are exposed in other environments where they spend large proportions of their day (such as school or daycare/nursery) as well as in their homes.23–27
In Table 1 we present risks of the development of childhood asthma in relation to exposure to aeroallergens discussed in this paper (based on a published systematic reviews – please note these relate to exposure, rather than sensitisation, to allergens).28
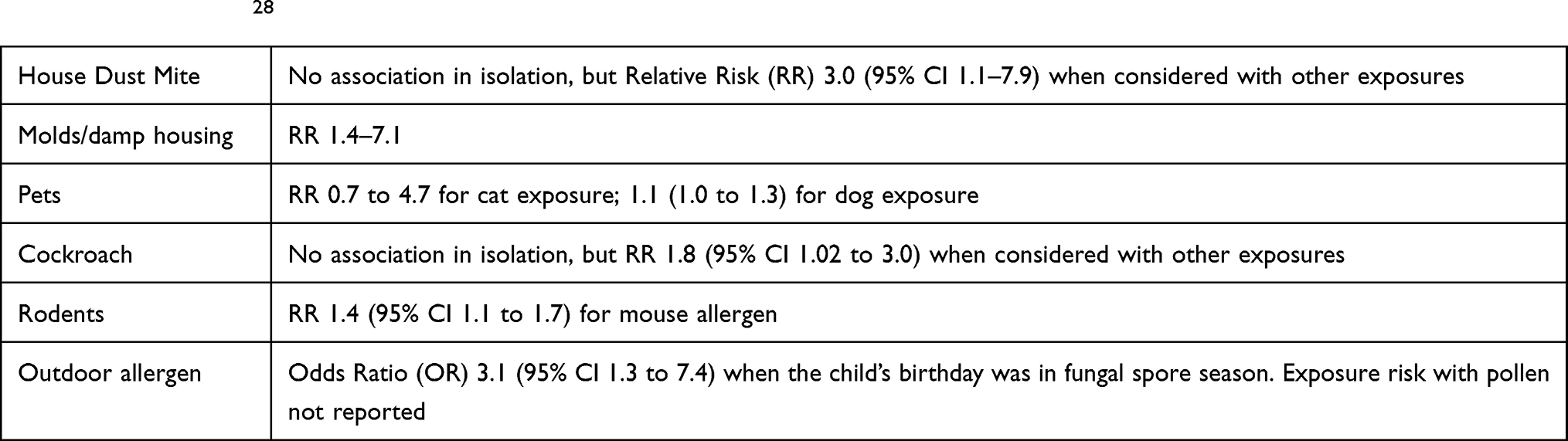 |
Table 1 A Summary of Risks for Development of Childhood Asthma in Relation to Exposure to Allergens Described in This Review. (Based on Dick et al)28 |
House Dust Mite
House dust mite (HDM) is one of the most prevalent indoor aeroallergens and commonly studied in the context of childhood asthma.29,30 It is believed that up to 85% of asthmatic children in temperate climates are sensitized to either one or both Dermatophagoides pteronyssinus or Dermatophagoides farinae species.31,32 Two main groups of allergens (1 and 2) usually found in dust mite faeces are predominantly responsible for allergen sensitization.
Dust mite allergens can be found in reservoirs present in various places throughout the home, such as soft furnishings and toys, beddings, carpets etc.27 One cross-Sectional study conducted across 831 United States (US) homes found that 84.2% had detectable levels of house dust mite allergens.32 It was further found that approximately half of the homes had levels equal to, or greater than, the supposed threshold for allergic sensitization (>2ug/g).33
Most of the literature available highlights the detrimental impact dust mite sensitization can have on paediatric asthma outcomes.29–31 Chronic exposure to HDM is associated with increased bronchial-hyperresponsiveness and airway inflammation; often resulting in poor lung function. One birth cohort study comprising of 620 babies noted associations between HDM sensitization and the prevalence of wheeze during infancy.34 The study concluded that children with a positive skin prick test for HDM at ages 1 or 2 years was a predictive factor for wheeze at age 12 years (adjusted odds ratio [aOR]: 1 year, 3.31 [95% CI 1.59–6.91]; 2 years, 6.37 [95% CI, 3.48–11.66]). The study further reported that one-year olds with wheeze who were HDM-sensitized had a 75% (95% CI 51% to 91%) greater probability of a wheeze present at 12 years of age.34 This was considerably lower compared to a 36% (95% CI 23% to 50%) probability amongst those infants who were not HDM sensitized. Similarly, this is echoed by another study which found a significant association between HDM sensitization in children (aged 2 to 5) with wheeze and the persistence of asthma in later childhood (P = 0.03).35 Symptom severity was also assessed by a study in Australia involving 174 children.36 They found a significant increase in daytime cough (relative rate [RR]; 1.64: 95% CI 1.14–2.36), nocturnal wheeze (RR; 3.62: 95% CI 1.49–8.77) and daytime asthma attacks (RR; 1.95: 95% CI 1.06–3.60).36
Indoor Molds
Fungal aeroallergens, commonly known as “molds”, are found extensively in both indoor and outdoor environments,21 often in association with damp and water damage.21 Out of the small number of species that have been identified, Penicillium and Aspergillus are the most prevalent types found indoors.29 However, some “outdoor” species, such as Alternaria can also be found indoors due to transfer via open windows or directly through clothing and pets.21,37
Sensitization rates for fungal allergens can be high amongst children with more asthma morbidity, with one inner-city US study reporting a prevalence of 50%.38 Another study involving UK children with severe symptoms presenting to hospital, demonstrate that up to 76% of participants were sensitised to such allergens.39 This emphasises the link between exposure in mold-sensitive children and severity of their asthma symptoms.
Several systematic reviews and meta-analyses have confirmed the associations between exposure to mold and damp with increased asthma morbidity in children.40,41 One study, investigating Penicillium exposure in asthmatic children found that high levels were associated with increased frequency of symptoms (an excess of 1.19 maximum symptom days at P=0.03) and healthcare visits (OR; 1.13: 95% CI 1.04–1.24).38 Similarly, Alternaria exposure has also been shown to worsen symptoms and bronchial hyper-responsiveness in sensitised asthmatic children.42 Results showed that children sensitised to the Alternaria mold species were more likely to suffer from airway hyperresponsiveness than other children (OR; 1.99: 95% CI: 1.45–2.70).42 Qualitative research has also demonstrated that merely the presence of visible mold, or its odour within the home is associated with overall poor infant asthma control.43
There is conflicting evidence regarding the associations between early life exposure to mold and asthma severity in later childhood. Some studies suggest that exposure to a diverse range of fungal allergens after birth can in fact be protective against allergen sensitisation and subsequently asthma symptoms.41 Yet most evidence supports the detrimental impact mold exposure can have on the development of asthma in children.21 For example, a Boston birth cohort study reported that high Alternaria exposure within the first 3 months of life is associated with increased frequency of wheezing in later childhood (OR; 1.83: 95% CI 1.07–3.14).
With regards to sensitisation, it can be difficult to fully assess the true extent of fungal allergens since many species remain unidentified.21 Furthermore, it is also noted that there is great variability in the methods used to quantify and assess fungal allergens.
Pets
Unsurprisingly, cats and dogs are the most common type of pets in US homes, and therefore are usually the primary focus in the context of asthma development in children.44 Fel d 1 and Can f 1, respectively, are major cat and dog allergens and specific markers for sensitisation.21 These allergens are found on the skin, hair and in the saliva of these furry pets and can be transferred to household members via clothing and surfaces.21 Such allergens can also remain airborne for a period of time, thereby causing airway irritation when inhaled by susceptible individuals (eg, atopic children). Although found in homes without pets, allergen concentrations are believed to be up to 1000 times greater in those households with pets.18 Sensitisation to Fel d 1 and Can f 1 is prevalent amongst asthmatic children and subsequently associated with poorer asthma-related outcomes. Sensitization rates reportedly range from between 25% to 65% amongst children with asthma.45
A prospective birth cohort conducted by the National Asthma Campaign Manchester Asthma and Allergy Study followed children from birth to 3 years of age.46 They measured skin-prick tests, airway resistance and allergen levels against pet ownership in the home. They concluded that the combination of allergic sensitization and high levels of pet allergen exposure were linked to significantly reduced lung function in children with asthma.46 The results from a US population-based survey emphasise the combined effect of allergic sensitisation and prolonged allergen exposure on asthma outcomes in children.44 For children sensitized to either cat or dog, there is a significant association with current asthma (reported sensitivity effect [SE] 17.3; 95% CI 9.3–25.4 and SE 14.5; 95% CI 8.8–20.1 respectively). Increased rates of asthma attacks amongst sensitized children were also reported, with 44.2% of attacks being attributable to high levels of dog allergens and 30.3% attributable to high levels of cat allergens.44 A similar effect is seen in adolescents enrolled in an Inner-City Asthma Control Evaluation; with higher cat IgE levels being associated with a greater risk of having an asthma exacerbation within the previous year.47
Conversely, there is some research to suggest that exposure to such pets can in fact be a protective factor against allergy sensitisation in asthmatic children.21 Yet, these findings may be need to be revisited given that a follow-up study revealed how the “protective nature” of this pet exposure during infancy usually diminishes by adulthood.48 Clearly, due to the degree of conflict across available literature, further evidence is required to confirm the role of pet exposure in early life in the context of asthma outcomes. It should also be noted other animals such as horse, may be have relevant asthma-related sensitizations including cross-reactive molecules.49
Cockroach
In the United States, the two main species of cockroach are the German (Blatella germanica) and American (Periplaneta americana). The major allergens derived from these cockroaches are Bla g 1, Bla g 2 and Per a 1 found in the saliva, secretions, debris and faecal material.18 A population-based cross-sectional survey including 831 U.S homes found that detectable levels of cockroach allergen concentrations (Bla g 1) were present in approximately 63% homes.50 The study further found that such allergens exceeded concentrations of > 2U/g in 11% of living rooms and 13% of kitchen floors.43 This threshold marks the hypothesised level of allergic sensitisation and is therefore associated with a potential increase in asthma morbidity.51 Generally, high allergen levels are linked to high-dense populations of lower socioeconomic status in urban environments.50 Sensitisation to cockroach allergens is common amongst children living in these areas, with prevalence rates ranging from 60% to 80% across the available literature.18
Children with asthma sensitised to cockroach allergens, who are exposed during their childhood often suffer from increased symptoms and poor overall asthma control.18 The Inner-City Asthma Study involving 939 children aged 5 to 11 with moderate to severely diagnosed asthma investigated the relationship between cockroach-allergen sensitization and asthma outcomes.52 They found that those children who were both sensitized to Bla g 1 (69%) and exposed, were significantly more likely to have more asthma symptom days (P = 0.02), more school days missed (P = 0.04), and an increased number of asthma-related unscheduled visits (RR 1.40; 95% CI: 1.02–1.92) than their non-sensitised unexposed counterparts.52 A birth cohort study within inner cities explored anti-cockroach IgE levels in children aged 2 to 3 years and their associated symptomology.53 The study reported an association between higher anti-cockroach IgE levels and increased frequency of wheeze (OR 3.3; 95% CI, 1.8–6.2). This dose-response relationship was significant (P<0.001) with early wheeze in infancy being linked to increasing cockroach IgE levels.53 Children sensitised to cockroach allergens are also reported to be at an increased risk of asthma morbidity and will often experience more hospitalisations than those who are not allergic.54 The National Cooperative Inner-City Asthma Study found a significant (P = 0.001) increase in the rate of asthma-related hospitalizations (0.37 per year) in those children who were both sensitised and exposed to cockroach allergens compared to others (0.11 hospitalisations per year).
Rodents
There are two mouse allergens, Mus m 1 and Mus m 2. Mus m 1 (the dominant mouse allergen), is found primarily in mouse urine, and in smaller amounts in mouse epithelium.55–57 Mus m 2 is found in mouse hair and dander.55−587 The major rat allergen is Rat n 1.58
Mouse allergen has been found primarily in inner-city homes and schools, although it is found in other demographics as well.59 While the concentration of mouse allergen varies as much as 1000-fold between inner-city and non-inner-city environments,60 Mus m 1 was found in 82% of homes in a cross-sectional survey of the United Stated (US) population.50 A study of predominantly high-income allergic children in Boston found mouse allergen in 42% of their homes.61 In addition to direct exposure in homes, mouse allergen can be passively transferred from adults who have occupational exposure.62 While less prevalent than mouse allergen, rat allergen is also common especially in inner-city homes. A prospective study of inner-city homes of the National Cooperative Inner-City Asthma Study Population found that 33% of inner city homes had detectable rat allergen.63
The majority of the literature regarding the role of rodent allergy in asthma derives from the US, where rodent sensitization has been associated with adverse clinical outcomes in children with asthma including poorer lung function and an increased risk of asthma exacerbations.58,59 A prospective study of 144 children with asthma noted a significant association between mouse sensitization and acute asthma care visits (prevalence ratio [PR] 1.33; 95% CI: 1.07–1.65), higher FENO levels (P<0.01), and increased bronchodilator reversibility (PR 1.54; 95% CI: 1.09–2.19), noting mouse allergen to be the “major allergen of public health relevance in Baltimore City”.64 A study of 645 predominantly minority and low-income children with uncontrolled asthma documented an association between mouse sensitization and higher asthma treatment step levels (P<0.001), as well as higher composite asthma severity index (CASI) (P=0.02), with a dose response noted.65 A prospective study of 127 school aged children in inner-city Baltimore with symptoms of asthma noted that mouse sensitization was associated with 50% more asthma symptom days (incidence rate ratio [IRR] 1.5; 95% CI: 1.1–2.1), 80% more days of beta-agonist use (IRR 1.9; 95% CI: 1.3–2.5), and increased emergency Department visits for asthma (OR 2.1; 95% CI: 1.1–4.1) and hospitalizations for asthma (OR 36.6; 95% CI: 4.1–327.3) than other children, noting mouse allergy to be “an important cause of asthma morbidity”.66 The study of homes through the National Cooperative Inner-City Asthma Study found that sensitization and rat exposure were associated with asthma-related hospitalizations, unscheduled medical visits and days with reduced activity as a result of asthma.63
Outdoor Allergens
Pollens
Outdoor pollens are mostly from tree, grasses and weeds.67 Cross-reactivity among pollens is common.68 More than 150 pollen allergens have been identified, and vary by region and time of year.69 Pollens have an annual periodicity, and symptoms related to sensitization and allergy to those pollens tend to occur at approximately the same time every year in a specific region, albeit with variations in timing, duration and intensity of each pollen season.70,71 Pollen allergen is released into the air as a result of humidity, heavy rain and pollutants but release also varies by pH, time and temperature outdoors.70
The literature has clearly and consistently identified outdoor pollens as playing a role in asthma exacerbations in children. A systematic review and meta-analysis on outdoor pollen as a trigger for asthma emergency department presentations in children (N=14 studies) found a statistically significant increase in the percentage change in the mean number of asthma emergency Department presentations for an increase in 10 grass pollen grains per cubic meter of exposure, with positive correlations between pollen concentrations and emergency department presentations.72 The strongest association was among children aged 5–17 years of age. A five year case-crossover study of 2098 children in Australia found that an increase from 75th to 90th percentile of grass (OR 1.03; 95% CI: 1.01–1.07), weed (OR 1.05; 95% CI: 1.01–1.10), and unclassified pollen (OR 1.05; 95% CI 1.00–1.09) levels were significantly associated with the odds of asthma-related hospitalizations.73 A time-stratified case-crossover study of pediatric asthma exacerbations in Philadelphia found an increased odds of asthma exacerbation in association with tree pollen, with a positive exposure-response pattern.74
Outdoor Molds
Outdoor molds include Alternaria and Cladosporium and peak seasonally in the mid-summer with a reduction by the winter season.75 In dry and warm climates Alternaria, found in soil, seeds and plants, is the most common outdoor mold and in temperate regions Cladosporium, found in plants and vegetable matter, is the most common outdoor mold.75
Both Alternaria and Cladosporium sensitization have been associated with asthma exacerbations.76 In fact, in a study of asthma-related deaths among children and young adults in Chicago, mean mold spore levels but not tree, grass, or ragweed pollen levels were significantly higher for days on which asthma-related death occurred than for days on which no deaths occurred (z = 2.80, p < 0.005).77 The association with mold spore levels remained significant on multivariate logistic regression with mold spore counts, with the odds of an asthma-related death occurring being 1.2 times higher (95% CI 1.07–1.34) for every increase of 1000 spores per cubic meter in daily mold spore levels.
Allergen Exposure in an Era of Global Change
Impact of Social Determinants of Health on Allergen Exposure
There are various social determinants of health, and many may have an impact on asthma prevalence and morbidity within specific populations including: income and social status, physical environments such as housing, and race/ethnicity.14,78–80 Many of these determinants exert their effects through a complex network of interdependences and direct and indirect mechanisms that limit access and adherence to medication. Social determinants may also influence patient outcomes, ie asthma control and risk of exacerbations, specifically through their impact on exposures, such as viral infections and aeroallergen exposure.
It has been suggested that the relationship between poverty and asthma is higher in the US than in other high income countries, and that this relationship may be related to surrogates of poverty, in particular urban living - housing and aeroallergen exposure - that is worsening asthma in inner cities in the US more so than in other parts of the world.81 Data from the NHIS (N=17,110 children) notes that while compared to nonurban children, urban children (both poor and not poor) were at significantly increased risk of asthma, nonurban poor children were not (adjusted OR 1.03; 95% CI 0.72–1.48).82 Mouse and cockroach exposure in inner-city homes has been described as endemic.59 Studies have found cockroach and mouse allergen to be present in up to 85–95% of inner-city homes within the US23,83 and up to 81% of school classrooms.84 In a study of 150 urban-dwelling children with asthma, every tenfold increase in bed mouse allergen level was associated with an 87% increase in the odds of any asthma-related health care use among mouse-sensitized (OR 1.87; 95% CI 1.21–2.88) but not non-mouse sensitized children.85
Access to environmental measures that may ameliorate the impact of aeroallergen exposure, such as dust mite covers, reductions in humidity, mold amelioration measures, and indoor climate control are also less accessible to those facing adverse social determinants of health.14,80
Impact of Climate Change on Allergen Exposure
It has been noted that over 90% of children worldwide “breath polluted air.”13 While the impact of climate change on aeroallergen exposure remains incompletely understood, there is increasing evidence that it may have an impact on outdoor aeroallergens, and by extension, asthma control in children.13,86 Global warming has been projected to influence the duration and intensity of pollen seasons, and may lead to increased pollen production, prolonged pollen seasons, and increased pollen protein allergenicity.13,86 The alterations in weather patterns including rainfall and wind may cause pollen species to reach environments in which they had not previously been present, contributing to a shift in geographic pollen distributions.13 In addition, increasing air pollutants as a result of climate change have the potential to interact with outdoor aeroallergens in a number of ways including increasing pollen allergenicity, increasing peripheral airway binding and distribution, and enhancing and irritative and pro-inflammatory effect.13
Extreme weather events, such as thunderstorms, are increased as a result of climate change. These also have profound impacts on aeroallergen distribution and effect, and its impact on asthma. One such example is “thunderstorm asthma,” in which there is an increase in acute asthma attacks following a thunderstorm during pollen seasons (with those who remain indoors, and hence not exposed to pollens, less likely to be impacted).87 These events have been associated with thunderstorms all over the world, including in children.88 In a retrospective review of pediatric patients during September 2018 noted a 2.7 times increase in daily visits to the emergency department and 16 times increase in hospitalizations during a thunderstorm compared to other days in September.89 It has been hypothesized that the mechanism for these asthma exacerbations relates to high levels of pollen aeroallergens (in particular grass pollen, but also outdoor molds) swirling in the early parts of the thunderstorm, pulled up by the air current, ruptured due to humidity, and then impacting the respiratory tract in high concentrations.88,90 Another extreme weather event, flooding, can also impact aeroallergen distribution and exposure. In particular, houses will be exposed to more indoor molds.91 Wildfires, which have plagued the United States, Canada and Australia (among others), increase particulate matter (in particular PM2.5) and increase the risk of asthma exacerbations and hospitalizations.92,93
As with all elements of asthma, the impact of climate change is most poignantly felt in those facing other adverse determinants of health. It has been noted that adverse determinants (poverty, homelessness, race, social disparities) influence climate exposures, exacerbate their health impacts, and ultimately cause worse health outcomes (due to increased likelihood of other underlying chronic medical conditions, and reduced healthcare access).13
Impact of the COVID-19 Pandemic on Allergen Exposure
During the COVID-19 pandemic, there has been a dramatic reduction in asthma exacerbations and emergency department visits among children.94–96 There are many factors that are hypothesized to contribute to this reduction, including social distancing measures, use of masks and a decrease in infectious triggers. Another possible contributor is is a reduced exposure to outdoor seasonal aeroallergens.97 This may be compounded by the considerable reduction in outdoor air pollution that has been noted during the pandemic. Declines in outdoor ground-level nitrogen dioxide (NO2), and PM2.5 have been noted in over 30 countries during the early phases of the pandemic, attributed in part to reductions in vehicle emissions.98 A network of over 10,000 air quality stations in over 34 countries noted dramatic reductions in PM2.5. It was estimated that there were a net total of 89,000 pediatric emergency room visits avoided during lockdowns as a result of this reduction in outdoor air pollution, which
illustrate the potential health benefits gained by reducing ‘business as usual’ air pollutant emissions from economic activities primarily through finding alternative transportation solutions.99
The flip side of the COVID-19 pandemic is the increased time indoors, and as a result exposure to indoor aeroallergens such as HDM, and indoor air pollutants.100 Some studies have demonstrated that, even in children with HDM sensitization and asthma, there remains reductions in respiratory tract infections and asthma exacerbations despite increased indoor aeroallergen exposure.100 However others have noted that HDM exposure and COVID-19 can create “the perfect storm,” with a noted worsening in allergic symptoms during the lockdowns among HDM sensitized individuals.101 However, other factors may influence the impact of increased indoor time as well. For example, increased indoor time can result in increased exposure to second-hand smoke and indoor air pollutants.97 In addition, with increased use of household cleaning products and disinfectants there has been a significant increase in volatile organic compound concentrations within the home including indoor total volatile organic compound concentration and PM2.5 concentrations.102
Principles of Treatment
Avoidance and Removal Measures
For indoor allergens, the Global Initiative for Asthma (GINA) strategy does not recommend allergen avoidance as a general strategy,2 noting limited evidence of clinical benefit especially with a single-strategy indoor aeroallergen avoidance approach. GINA also notes that allergen avoidance strategies can be both “complicated and expensive, and there are no validated methods for identifying those who are likely to benefit.”2 If an approach is taken, especially if there are multiple allergies, a comprehensive approach is most likely to be beneficial.75
Measures to remove HDM within the home include mattress and pillow covers (pore diameter no more than 10 microns), regular washing of bedding in hot water, removal of stuffed toys upholstered furniture and carpeting, regular vacuuming, and keeping the humidity low in the home (<50%).75 In a systematic review of 20 studies in children and adolescents, multicomponent dust mite interventions reduced the number of asthma symptoms by 0.8 days per 2 weeks (21.0 symptom days per year) and reduced the number of asthma acute care visits by 0.57 visits per year.103 However, as noted by the GINA guidance, “this approach is complicated, expensive and is not generally recommended.”2 Reduction in humidity has the potential to reduce indoor mold exposure such as dehumidifiers and air conditioners. In addition, removing obvious mold from the home may play a role as well.75
The optimal approach to remove pet allergen from the home is removal of the pet itself from the home. However, even with pet removal it can take months for the pet aeroallergen to reduce to baseline. In a study of 15 homes during a 9-to 43-week period after cat removal, Fel d 1 levels declined gradually in most homes and by 20 to 24 weeks after cat removal, 8/15 were consistent with levels found in control homes without cats.104 Whether or not the pet is removed from the home, thoroughly cleaning the home and removal of any reservoirs for the allergen (upholstered furniture and carpeting) may be beneficial.75 Use of high-efficiency particulate air (HEPA) filters, mattress and pillow covers, and regular washing (in particular for dogs but only if twice a week or more)104 can be helpful if the pet remains in the home.77 However, whether or not this reduction in airborne allergen levels impacts asthma disease activity remains controversial.105 The GINA strategy notes limited evidence of clinical benefit for asthma with pet avoidance strategies.2 This may be partly because exposure to pet allergens occurs in schools, public buildings and public transportation even if the pet is removed from the home.2
Integrated pest management (IPM) strategies have demonstrated effectiveness in removing cockroach, mouse and rat allergen from the home.106 IPM includes sealing all cracks/holes in the home, cleaning surfaces with detergent, vacuuming with HEPA filtration, tracking powder (pesticide) on wall voids/pipe chases, snap traps, and familial education about food storage and kitchen cleaning.59,60 Simple interventions, such as insecticides, can make a significant difference. A recent study of 122 children with moderate to severe asthma noted that insecticidal bait in the homes resulted in few cockroaches within the homes (P<0.01); children in control homes without the bait had more asthma symptoms (P=0.03), unscheduled health care utilization (P=0.03) and worsening lung function (P=0.01) compared to children in the intervention group.107 Rodenticide can be considered in accordance with their Environmental Protection Agency-approved label indications if other measures of IPM are unsuccessful.58
For outdoor allergens, GINA notes that these are impossible to avoid completely.2
Closing doors and windows and remaining indoors when pollen and/or mold counts are highest may have a role in reducing exposure (although there is low quality evidence to support this intervention).2 Pollen calendars and monitoring of pollen and mold counts may be helpful at the individual and population level, as correlations are found between the pattern of pollen load and allergen content with asthma symptoms.108,109 Novel methods to predict pollen counts including mobile solutions are ongoing.110
Allergen Immunotherapy
Allergen immunotherapy (AIT) is a key treatment option for children with aeroallergen-induced IgE-mediated disease. The mechanisms underpinning the induction and maintenance of allergen-specific tolerance involve several immunologic pathways, including both innate and adaptive immune responses.111 There are two main types of AIT available – subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT).2 A range of aeroallergens are available, using purified extracts or recombinant allergens, unmodified or modified, in increasingly diverse and heterogeneously available commercial products.
Whilst a robust body of evidence supports the efficacy and safety of AIT in pediatric allergic rhinitis and rhinoconjunctivitis over 5 years of age, the knowledge base for asthma is less solid.111 Most data for this indication comes from children with mild-to-moderate asthma, with several systematic reviews supporting the efficacy and safety of AIT in these asthmatic children. Immunotherapy has been considered safe, effective in reducing asthma medication burden, and has the potential to have a disease progression preventative effect.112 Guidelines differ in their recommendation for use in pediatric asthma, based on age, asthma severity and specific allergens.2,111,114,
Shortcomings in available evidence include the diversity in selected populations (eg single or polysensitized), the sources and types of single/combined allergen products used with differing standardization and quality, the absence of validated biomarkers and clinically relevant outcomes, as well as the scarcity of comparative data between SCIT and SLIT. Differences in the evidence base between distinct allergens are particularly relevant, with more confidence in the benefits of AIT for selected pollens and HDM, lower strength of evidence supporting the use in selected molds (ie Alternaria), and considerable gaps regarding effectiveness of AIT for dogs, cats, horses and rodents, as well as other allergens.
Mitigating the Impact of Climate Change, Adverse Social Determinants, and COVID-19
The Global Alliance against Chronic Respiratory Diseases (GRD) which was initiated by the World Health Organization (WHO) has identified climate change prevention (or amelioration) as a respiratory public health priority.13 A position statement by the European Respiratory Society (ERS) on climate change and respiratory disease notes that “awareness and appropriate actions with respect to climate change” are a necessary and urgent intervention.91 A recent review article on the impact of climate change and allergic disease noted
We must take a moment and reflect on our role during this unique moment in the history of humanity. It is up to us reading this journal to step up, educate, create awareness, and advocate for the future of our patients and every person in the world … The medical profession is a trusted source of knowledge and can promote equitable climate solutions and health policies.13
In addition, this review article noted the impact of individual-level choices as they relate to our personal carbon footprint, can have a profound impact on climate change.13 The ERS provides a series of specific recommendations to reduce the impact of climate change including reducing emissions, improving home insulation and temperature control and reducing indoor pollution, although acknowledging that many gaps in the literature exist and that for certain exposures – such as pollens – little can be done.91
Determinants of health need to be increasingly considered in working with children with asthma and their families. As noted in a recent viewpoint, “to foster health at the population level, population health is best seen as a hybrid of public health and clinical Medicine, drawing from the traditions of both approaches.”114 Ongoing advocacy is required to reduce the impact that determinants of health have on the prevalence, and morbidity, of asthma in childhood moving forward, both at a clinical and at a policy level. Various solutions to maintain “healthy housing” have been proposed during the pandemic, to mitigate any impact of increased exposure to indoor aeroallergens and pollutants.97 These include smoking avoidance and cessation, keeping windows open frequently (unless it is high pollen season), and avoiding burning solid fuels for cooking.97
Conclusion and Future Steps
Allergens have an important and long-lasting role in the development of asthma, and asthma control. Despite individual variances in asthma endotype and phenotype, the role of allergens, as an important driver of Type-2 high disease, is likely to remain constant. There are societal and socioeconomic factors that increase the risk and impact of allergen sensitisation.
Currently the evidence around allergen avoidance and mitigation measures – including clinical and cost-effectiveness outcomes – is variable. Notwithstanding this, there is a need for further education about the impact of particular problems, for example rodent allergy. Currently, there is no mention of evaluation of rodent sensitization in either the Global Initiative for Asthma (GINA)115 or National Asthma Education and Prevention Program (Expert Panel Report, 3) guidelines.59,116 Advocacy efforts to provide affordable pest management strategies are necessary.59 Further research efforts are necessary to determine which pest management strategies are most effective in these communities.59 A consensus approach is required, and this should start with a. detailed process mapping international guidance around allergens.
Alongside this there is a need to consider allergens and climate change. The ERS position statement has identified several steps that are required moving forward, largely focused on research priorities. For example, they note research is needed on the clinical efficacy of interventions to mitigate the impact of climate change, the role of housing systems in respiratory disease including asthma, and identifying which children are most at risk due to the impacts of climate change.91
Regarding the impact of social determinants, moving forward, there remains much to learn. As we increasingly understand the various phenotypic and endotypic differences in pediatric asthma, and the role of personalized medicine, this evolving and exciting research may further guide our approach to some of these determinants such as access to care. The results of studies in inner cities may further inform approach. The role of these determinants in shaping policy and research needs moving forward remains to be seen, as does how policy and healthcare spending should reflect the role of these determinants.
Disclosure
RM Fernandes is/has been a member of DMCs and CECs of clinical trials by Ablynx, Janssen and Reviral. EM Abrams is an employee of Public Health Agency of Canada (PHAC); the views expressed are her own and not those of PHAC. Dr Ian P Sinha reports being a paid consult from Astra Zeneca. The authors report no other conflicts of interest in this work.
References
1. Abrams E, Becker A, Szefler S. Current state and future of biologic therapies in the treatment of asthma in children. Pediatr Allergy Immunol Pulmonol. 2018;31(3):119–131. doi:10.1089/ped.2018.0901
2. GINA. GINA Guidance about COVID-19 and Asthma; 30 March 2021. Available from: https://ginasthma.org/wp-content/uploads/2021/03/21_03_30-GINA-COVID-19-and-asthma.pdf.
3. Akinbami LJ, Moorman JE, Bailey C, et al. Trends in asthma prevalence, health care use, and mortality in the United States, 2001–2010. NCHS Data Brief. 2012;94:1–8.
4. Zahran H, Bailey C, Damon S, Garbe P, Breysse P. Vital signs: asthma in children — UNITED STATES, 2001–2016. MMWR Morb Mortal Wkly Rep. 2018;67(5):149–155. doi:10.15585/mmwr.mm6705e1
5. Nurmagambetov T, Kuwahara R, Garbe P. The economic burden of asthma in the United States, 2008–2013. Ann Am Thorac Soc. 2018;15(3):348–356. doi:10.1513/AnnalsATS.201703-259OC
6. Szefler S, Zeiger R, Haselkorn T, et al. Economic burden of impairment in children with severe or difficult-to-treat asthma. Ann Allergy Asthma Immunol. 2011;107(2):110–119.e1. doi:10.1016/j.anai.2011.04.008
7. Saglani S, Custovic A. Childhood asthma: advances using machine learning and mechanistic studies. Am J Respir Crit Care Med. 2019;199(4):414–422. doi:10.1164/rccm.201810-1956CI
8. Oksel C, Haider S, Fontanella S, Frainay C, Custovic A. Classification of pediatric asthma: from phenotype discovery to clinical practice. J Asthma. 2018;6. doi:10.3389/fped.2018.00258
9. Licari A, Castagnoli R, Brambilla I, et al. Asthma endotyping and biomarkers in childhood asthma. Pediatr Allergy Immunol Pulmonol. 2018;31(2):44–55. doi:10.1089/ped.2018.0886
10. Bush A. Which child with asthma is a candidate for biological therapies? J Clin Med. 2020;9(4):1237. doi:10.3390/jcm9041237
11. Platts-Mills T, Leung DYM, Schatz M. The role of allergens in asthma. Am Fam Physician. 2007;76(5):675–680.
12. Cloutier M, Baptist A, Blake K, et al. 2020 focused updates to the asthma management guidelines: a report from the National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group. J Allergy Clin Immunol. 2020;146(6):1217–1270.
13. Pacheco S, Guidos-Fogelbach G, Annesi-Maesano I, et al. Climate change and global issues in allergy and immunology. J Allergy Clin Immunol. 2021;148(6):1366–1377. doi:10.1016/j.jaci.2021.10.011
14. Federico M, McFarlane A, Szefler S, Abrams E. The impact of social determinants of health on children with asthma. J Allergy Clin Immunol Pract. 2020;8(6):1808–1814. doi:10.1016/j.jaip.2020.03.028
15. Sporik R, Holgate S, Platts-Mills T, Cogswell J. Exposure to house-dust mite allergen (der pI) and the development of asthma in childhood. N Engl J Med. 1990;323(8):502–507. doi:10.1056/NEJM199008233230802
16. Squillance S, Sporik R, Rakes G, et al. Sensitization to dust mites as a dominant risk factor for asthma among adolescents living in Central Virginia. Am J Respir Crit Care Med. 1997;156(6):1760–1764. doi:10.1164/ajrccm.156.6.9704026
17. Call R, Smith T, Morris E, Chapman M, Platts-Mills T. Risk factors for asthma in inner city children. J Pediatr. 1992;121(6):862–866. doi:10.1016/S0022-3476(05)80329-4
18. Ahluwalia S, Matsui E. The indoor environment and its effects on childhood asthma. Curr Opin Allergy Clin Immunol. 2011;11(2):137–143. doi:10.1097/ACI.0b013e3283445921
19. Sheehan W, Permaul P, Petty C, et al. Association between allergen exposure in inner-city schools and asthma morbidity among students. JAMA Pediatr. 2017;171(1):31. doi:10.1001/jamaPediatrics.2016.2543
20. Beck A, Huang B, Kercsmar C, et al. Allergen sensitization profiles in a population-based cohort of children hospitalized for asthma. Ann Am Thorac Soc. 2015;12(3):376–384. doi:10.1513/AnnalsATS.201408-376OC
21. Ahluwalia S, Matsui E. Indoor environmental interventions for furry pet allergens, pest allergens, and mold: looking to the future. J Allergy Clin Immunol Pract. 2018;6(1):9–19. doi:10.1016/j.jaip.2017.10.009
22. US Environmental Protection Agency. Report to Congress on Indoor Air Quality. Vol. 2. Washington, DC: US Environmental Protection Agency; 1989.
23. Permaul P, Hoffman E, Fu C, et al. Allergens in urban schools and homes of children with asthma. Pediatr Allergy Immunol. 2012;23(6):543–549. doi:10.1111/j.1399-3038.2012.01327.x
24. Carreiro-Martins P, Papoila A, Caires I, et al. Effect of indoor air quality of day care centers in children with different predisposition for asthma. Pediatr Allergy Immunol. 2016;27(3):299–306. doi:10.1111/pai.12521
25. Holst G, Høst A, Doekes G, et al. Allergy and respiratory health effects of dampness and dampness-related agents in schools and homes: a cross-sectional study in Danish pupils. Indoor Air. 2016;26(6):880–891. doi:10.1111/ina.12275
26. Chen C, Chao H, Chan C, Chen B, Guo Y. Current asthma in schoolchildren is related to fungal spores in classrooms. Chest. 2014;146(1):123–134. doi:10.1378/chest.13-2129
27. Abramson S. Reducing environmental allergic triggers: policy issues. J Allergy Clin Immunol Pract. 2018;6(1):32–35. doi:10.1016/j.jaip.2017.10.027
28. Dick S, Friend A, Dynes K, et al. A systematic review of associations between environmental exposures and development of asthma in children aged up to 9 years. BMJ Open. 2014;4(11):e006554. doi:10.1136/bmjopen-2014-006554
29. Wilson J, Platts-Mills T. Home environmental interventions for house dust mite. J Allergy Clin Immunol Pract. 2018;6(1):1–7. doi:10.1016/j.jaip.2017.10.003
30. Portnoy J, Miller J, Williams P, et al. Environmental assessment and exposure control of dust mites: a practice parameter. Ann Allergy Asthma Immunol. 2013;111(6):465–507.
31. Louisias M, Ramadan A, Naja A, Phipatanakul W. The effects of the environment on asthma disease activity. Immunol Allergy Clin North Am. 2019;39(2):163–175. doi:10.1016/j.iac.2018.12.005
32. Wang J. The innate immune response in house dust mite-induced allergic inflammation. Allergy Asthma Immunol Res. 2013;5(2):68. doi:10.4168/aair.2013.5.2.68
33. Arbes S, Cohn R, Yin M, et al. House dust mite allergen in US beds: results from the first national survey of lead and allergens in housing. J Allergy Clin Immunol. 2003;111(2):408–414. doi:10.1067/mai.2003.16
34. Lodge C, Lowe A, Gurrin L, et al. House dust mite sensitization in toddlers predicts current wheeze at age 12 years. J Allergy Clin Immunol. 2011;128(4):782–788.e9. doi:10.1016/j.jaci.2011.06.038
35. Llanora G, Ming L, Wei L, van Bever H. House dust mite sensitization in toddlers predict persistent wheeze in children between eight to fourteen years old. Asia Pac Allergy. 2012;2(3):181. doi:10.5415/apallergy.2012.2.3.181
36. Nitschke M, Pilotto L, Attewell R, et al. A cohort study of indoor nitrogen dioxide and house dust mite exposure in asthmatic children. J Occup Environ Med. 2006;48(5):462–469. doi:10.1097/01.jom.0000215802.43229.62
37. Sheehan W, Phipatanakul W. Indoor allergen exposure and asthma outcomes. Curr Opin Pediatr. 2016;28(6):772–777. doi:10.1097/MOP.0000000000000421
38. Pongracic J, O’Connor G, Muilenberg M, et al. Differential effects of outdoor versus indoor fungal spores on asthma morbidity in inner-city children. J Allergy Clin Immunol. 2010;125(3):593–599. doi:10.1016/j.jaci.2009.10.036
39. O’Driscoll B, Hopkinson L, Denning D. Mold sensitization is common amongst patients with severe asthma requiring multiple hospital admissions. BMC Pulm Med. 2005;5(1). doi:10.1186/1471-2466-5-4
40. Caillaud D, Leynaert B, Keirsbulck M, Nadif R. Indoor mould exposure, asthma and rhinitis: findings from systematic reviews and recent longitudinal studies. Eur Respir Rev. 2018;27(148):170137. doi:10.1183/16000617.0137-2017
41. Baxi S, Portnoy J, Larenas-Linnemann D, et al. Exposure and health effects of fungi on humans. J Allergy Clin Immunol Pract. 2016;4(3):396–404. doi:10.1016/j.jaip.2016.01.008
42. Downs S, Mitakakis T, Marks G, et al. Clinical importance of Alternaria exposure in children. Am J Respir Crit Care Med. 2001;164(3):455–459. doi:10.1164/ajrccm.164.3.2008042
43. Değer L, Plante C, Goudreau S, et al. Home environmental factors associated with poor asthma control in Montreal children: a population-based study. J Asthma. 2010;47(5):513–520. doi:10.3109/02770901003615778
44. Gergen P, Mitchell H, Calatroni A, et al. Sensitization and exposure to pets: the effect on asthma morbidity in the US population. J Allergy Clin Immunol Pract. 2018;6(1):101–107.e2. doi:10.1016/j.jaip.2017.05.019
45. Weiss S, Horner A, Shapiro G, Sternberg A. The prevalence of environmental exposure to perceived asthma triggers in children with mild-to-moderate asthma: data from the Childhood Asthma Management Program (CAMP). J Allergy Clin Immunol. 2001;107(4):634–640. doi:10.1067/mai.2001.113869
46. Lowe L, Woodcock A, Murray C, et al. Lung function at age 3 years. Arch Pediatr Adolesc Med. 2004;158(10):996. doi:10.1001/archpedi.158.10.996
47. Matsui E, Sampson H, Bahnson H, et al. Allergen-specific IgE as a biomarker of exposure plus sensitization in inner-city adolescents with asthma. Allergy. 2010;65(11):1414–1422. doi:10.1111/j.1398-9995.2010.02412.x
48. Wegienka G, Johnson C, Havstad S, Ownby D, Zoratti E. Indoor pet exposure and the outcomes of total IgE and sensitization at age 18 years. J Allergy Clin Immunol. 2010;126(2):274–279.e5. doi:10.1016/j.jaci.2010.05.001
49. Schoos A, Nwaru B, Borres M. Component-resolved diagnostics in pet allergy: current perspectives and future directions. J Allergy Clin Immunol. 2021;147(4):1164–1173. doi:10.1016/j.jaci.2020.12.640
50. Cohn R, Arbes Jr. S
51. Eggleston P, Rosenstreich D, Lynn H, et al. Relationship of indoor allergen exposure to skin test sensitivity in inner-city children with asthma. J Allergy Clin Immunol. 1998;102(4):563–570. doi:10.1016/S0091-6749(98)70272-6
52. Gruchalla R, Pongracic J, Plaut M, et al. Inner city asthma study: relationships among sensitivity, allergen exposure, and asthma morbidity. J Allergy Clin Immunol. 2005;115(3):478–485. doi:10.1016/j.jaci.2004.12.006
53. Donohue K, Al-alem U, Perzanowski M, et al. Anti-cockroach and anti-mouse IgE are associated with early wheeze and atopy in an inner-city birth cohort. J Allergy Clin Immunol. 2008;122(5):914–920. doi:10.1016/j.jaci.2008.08.034
54. Rosenstreich D, Eggleston P, Kattan M, et al. The role of cockroach allergy and exposure to cockroach allergen in causing morbidity among inner-city children with asthma. N Engl J Med. 1997;336(19):1356–1363. doi:10.1056/NEJM199705083361904
55. Twiggs J, Agarwal M, Dahlberg M, Yunginger J. Immunochemical measurement of airborne mouse allergens in a laboratory animal facility. J Allergy Clin Immunol. 1982;69(6):522–526. doi:10.1016/0091-6749(82)90177-4
56. Schumacher M. Characterization of allergens from urine and pelts of laboratory mice. Mol Immunol. 1980;17(9):1087–1095. doi:10.1016/0161-5890(80)90105-4
57. Sakaguchi M, Inouye S, Miyazawa H, et al. Particle size of airborne mouse crude and defined allergens. Lab Anim Sci. 1989;39(3):234–236.
58. Phipatanakul W, Matsui E, Portnoy J, et al. Environmental assessment and exposure reduction of rodents: a practice parameter. Ann Allergy Asthma Immunol. 2012;109(6):375–387. doi:10.1016/j.anai.2012.09.019
59. Abrams E, Szefler S, Becker A. Time for allergists to consider the role of mouse allergy in non-inner city children with asthma. J Allergy Clin Immunol Pract. 2019;7(6):1778–1782. doi:10.1016/j.jaip.2019.03.004
60. Matsui E. Management of rodent exposure and allergy in the pediatric population. Curr Allergy Asthma Rep. 2013;13(6):681–686. doi:10.1007/s11882-013-0378-4
61. Phipatanakul W, Gold D, Muilenberg M, et al. Predictors of indoor exposure to mouse allergen in urban and suburban homes in Boston. Allergy. 2005;60(5):697–701. doi:10.1111/j.1398-9995.2005.00825.x
62. Krakowiak A, Szulc B, Górski P. Allergy to laboratory animals in children of parents occupationally exposed to mice, rats and hamsters. Eur Respir J. 1999;14(2):347–351. doi:10.1183/09031936.99.14235299
63. Perry T, Matsui E, Merriman B, Duong T, Eggleston P. The prevalence of rat allergen in inner-city homes and its relationship to sensitization and asthma morbidity. J Allergy Clin Immunol. 2003;112(2):346–352. doi:10.1067/mai.2003.1640
64. Ahluwalia S, Peng R, Breysse P, et al. Mouse allergen is the major allergen of public health relevance in Baltimore City. J Allergy Clin Immunol. 2013;132(4):830–835.e2. doi:10.1016/j.jaci.2013.05.005
65. Grant T, Aloe C, Perzanowski M, et al. Mouse sensitization and exposure are associated with asthma severity in urban children. J Allergy Clin Immunol Pract. 2017;5(4):1008–1014.e1. doi:10.1016/j.jaip.2016.10.020
66. Matsui E, Eggleston P, Buckley T, et al. Household mouse allergen exposure and asthma morbidity in inner-city preschool children. Ann Allergy Asthma Immunol. 2006;97(4):514–520. doi:10.1016/S1081-1206(10)60943-X
67. Baldacci S, Maio S, Cerrai S, et al. Allergy and asthma: effects of the exposure to particulate matter and biological allergens. Respir Med. 2015;109(9):1089–1104. doi:10.1016/j.rmed.2015.05.017
68. Ansotegui I, Melioli G, Canonica G, et al. IgE allergy diagnostics and other relevant tests in allergy, a World Allergy Organization position paper. World Allergy Organ J. 2020;13(2):100080.
69. Xie ZJ, Guan K, Yin J. Advances in the clinical and mechanism research of pollen induced seasonal allergic asthma. Am J Clin Exp Immunol. 2019;8(1):1–8.
70. Taketomi E, Sopelete M, de Sousa Moreira P, de Assis Machado Vieira F. Pollen allergic disease: pollens and its major allergens. Braz J Otorhinolaryngol. 2006;72(4):562–567. doi:10.1016/S1808-8694(15)31005-3
71. Bastl K, Kmenta M, Berger U. Defining pollen seasons: background and recommendations. Curr Allergy Asthma Rep. 2018;18(12):12. doi:10.1007/s11882-018-0829-z
72. Erbas B, Jazayeri M, Lambert K, et al. Outdoor pollen is a trigger of child and adolescent asthma emergency department presentations: a systematic review and meta-analysis. Allergy. 2018;73(8):1632–1641. doi:10.1111/all.13407
73. Shrestha S, Katelaris C, Dharmage S, et al. High ambient levels of grass, weed and other pollen are associated with asthma admissions in children and adolescents: a large 5-year case-crossover study. Clin Exper Allergy. 2018;48(11):1421–1428. doi:10.1111/cea.13225
74. De Roos A, Kenyon C, Zhao Y, et al. Ambient daily pollen levels in association with asthma exacerbation among children in Philadelphia, Pennsylvania. Environ Int. 2020;145:106138. doi:10.1016/j.envint.2020.106138
75. Baxi SN, Phipatanakul W. The role of allergen exposure and avoidance in asthma. Adolesc Med State Art Rev. 2010;21(1):
76. Pulimood T, Corden J, Bryden C, Sharples L, Nasser S. Epidemic asthma and the role of the fungal mold Alternaria alternata. J Allergy Clin Immunol. 2007;120(3):610–617. doi:10.1016/j.jaci.2007.04.045
77. Targonski P, Persky V, Ramekrishnan V. Effect of environmental molds on risk of death from asthma during the pollen season. J Allergy Clin Immunol. 1995;95(5):955–961. doi:10.1016/S0091-6749(95)70095-1
78. Government of Canada. Social determinants of health and health inequalities [Internet]; 2020. Available from: https://www.canada.ca/en/public-health/services/health-promotion/population-health/what-determines-health.html.
79. World Health Organization. The determinants of health [Internet]; 2022. Available from: https://www.who.int/hia/evidence/doh/en/.
80. Grant T, Croce E, Matsui EC. Asthma and the social determinants of health. Ann Allergy Asthma Immunol. 2021;128:5–11
81. Platts-Mills T, Carter M. Asthma and Indoor Exposure to Allergens. N Engl J Med. 1997;336(19):1382–1384. doi:10.1056/NEJM199705083361909
82. Andrew Aligne C, Auinger P, Byrd R, Weitzman M. Risk factors for pediatric asthma. Am J Respir Crit Care Med. 2000;162(3):873–877. doi:10.1164/ajrccm.162.3.9908085
83. Sohn M, Kim K. The cockroach and allergic diseases. Allergy Asthma Immunol Res. 2012;4(5):264. doi:10.4168/aair.2012.4.5.264
84. Chew G, Correa J, Perzanowski M. Mouse and cockroach allergens in the dust and air in northeastern United States inner-city public high schools. Indoor Air. 2005;15(4):228–234. doi:10.1111/j.1600-0668.2005.00363.x
85. Torjusen E, Diette G, Breysse P, et al. Dose-response relationships between mouse allergen exposure and asthma morbidity among urban children and adolescents. Indoor Air. 2012;23(4):268–274. doi:10.1111/ina.12009
86. Schmier J, Ebi K. The impact of climate change and aeroallergens on children’s health. Allergy Asthma Proc. 2009;30(3):229–237. doi:10.2500/aap.2009.30.3229
87. D’Amato G, Annesi Maesano I, Molino A, Vitale C, D’Amato M. Thunderstorm-related asthma attacks. J Allergy Clin Immunol. 2017;139(6):1786–1787. doi:10.1016/j.jaci.2017.03.003
88. D’Amato G, Annesi-Maesano I, Vaghi A, Cecchi L, D’Amato M. How do storms affect asthma? Curr Allergy Asthma Rep. 2018;18(4). doi:10.1007/s11882-018-0775-9
89. Xu Y, Xue T, Li H, Guan K. Retrospective analysis of epidemic thunderstorm asthma in children in Yulin, northwest China. Pediatr Res. 2020;89(4):958–961. doi:10.1038/s41390-020-0980-9
90. Rorie A, Poole J. The role of extreme weather and climate-related events on asthma outcomes. Immunol Allergy Clin North Am. 2021;41(1):73–84. doi:10.1016/j.iac.2020.09.009
91. Ayres J, Forsberg B, Annesi-Maesano I, et al. Climate change and respiratory disease: European Respiratory Society position statement. Eur Respir J. 2009;34(2):295–302. doi:10.1183/09031936.00003409
92. Kiser D, Metcalf W, Elhanan G, et al. Particulate matter and emergency visits for asthma: a time-series study of their association in the presence and absence of wildfire smoke in Reno, Nevada, 2013–2018. Environ Health. 2020;19(1). doi:10.1186/s12940-020-00646-2.
93. Tse K, Chen L, Tse M, Zuraw B, Christiansen S. Effect of catastrophic wildfires on asthmatic outcomes in obese children: breathing fire. Ann Allergy Asthma Immunol. 2015;114(4):308–311.e4. doi:10.1016/j.anai.2015.01.018
94. Ruano F, Somoza Álvarez M, Haroun-Díaz E, et al. Impact of the COVID-19 pandemic in children with allergic asthma. J Allergy Clin Immunol Pract. 2020;8(9):3172–3174.e1. doi:10.1016/j.jaip.2020.07.019
95. Krivec U, Kofol Seliger A, Tursic J. COVID-19 lockdown dropped the rate of paediatric asthma admissions. Arch Dis Child. 2020;105(8):809–810. doi:10.1136/archdischild-2020-319522
96. Kenyon C, Hill D, Henrickson S, Bryant-Stephens T, Zorc J. Initial effects of the COVID-19 pandemic on pediatric asthma emergency department utilization. J Allergy Clin Immunol Pract. 2020;8(8):2774–2776.e1. doi:10.1016/j.jaip.2020.05.045
97. Ferrante G, Mollicone D, Cazzato S, et al. COVID-19 pandemic and reduced physical activity: Is there an impact on healthy and asthmatic children? J Asthma. 2021;9. doi:10.3389/fped.2021.695703
98. Venter Z, Aunan K, Chowdhury S, Lelieveld J. COVID-19 lockdowns cause global air pollution declines. Proc Nat Acad Sci. 2020;117(32):18984–18990. doi:10.1073/pnas.2006853117
99. Venter Z, Aunan K, Chowdhury S, Lelieveld J. Air pollution declines during COVID-19 lockdowns mitigate the global health burden. Environ Res. 2021;192:110403. doi:10.1016/j.envres.2020.110403
100. Yucel E, Suleyman A, Hizli Demirkale Z, et al. ‘Stay at home’: is it good or not for house dust mite sensitized children with respiratory allergies? Pediatr Allergy Immunol. 2021;32(5):963–970. doi:10.1111/pai.13477
101. Gelardi M, Trecca E, Fortunato F, et al. COVID‐19: when dust mites and lockdown create the perfect storm. Laryngoscope Investig Otolaryngol. 2020;5(5):788–790. doi:10.1002/lio2.439
102. Domínguez-Amarillo S, Fernández-Agüera J, Cesteros-García S, González-Lezcano R. Bad air can also kill: residential indoor air quality and pollutant exposure risk during the COVID-19 crisis. Int J Environ Res Public Health. 2020;17(19):7183. doi:10.3390/ijerph17197183
103. Crocker D, Kinyota S, Dumitru G, et al. Effectiveness of home-based, multi-trigger, multicomponent interventions with an environmental focus for reducing asthma morbidity. Am J Prev Med. 2011;41(2):S5–S32. doi:10.1016/j.amepre.2011.05.012
104. Wood R, Chapman M, Adkinson N, Eggleston P. The effect of cat removal on allergen content in household-dust samples. J Allergy Clin Immunol. 1989;83(4):730–734. doi:10.1016/0091-6749(89)90006-7
105. Wood R, Johnson E, Van Natta M, Chen P, Eggleston P. A placebo-controlled trial of a HEPA air cleaner in the treatment of cat allergy. Am J Respir Crit Care Med. 1998;158(1):115–120. doi:10.1164/ajrccm.158.1.9712110
106. Phipatanakul W, Cronin B, Wood R, et al. Effect of environmental intervention on mouse allergen levels in homes of inner-city Boston children with asthma. Ann Allergy Asthma Immunol. 2004;92(4):420–425. doi:10.1016/S1081-1206(10)61777-2
107. Rabito F, Carlson J, He H, Werthmann D, Schal C. A single intervention for cockroach control reduces cockroach exposure and asthma morbidity in children. J Allergy Clin Immunol. 2017;140(2):565–570. doi:10.1016/j.jaci.2016.10.019
108. Suanno C, Aloisi I, Fernández-González D, Del Duca S. Pollen forecasting and its relevance in pollen allergen avoidance. Environ Res. 2021;200:111150. doi:10.1016/j.envres.2021.111150
109. Bastl K, Kmenta M, Pessi A, et al. First comparison of symptom data with allergen content (Bet v 1 and Phl p 5 measurements) and pollen data from four European regions during 2009–2011. Sci Total Environ. 2016;548–549:229–235. doi:10.1016/j.scitotenv.2016.01.014
110. Sofiev M, Palamarchuk Y, Bédard A, et al. A demonstration project of global alliance against chronic respiratory diseases: prediction of interactions between air pollution and allergen exposure—the mobile airways sentinel network-impact of air pollution on asthma and rhinitis approach. Chin Med J. 2020;133(13):1561–1567. doi:10.1097/CM9.0000000000000916
111. Alvaro‐Lozano M, Akdis C, Akdis M, et al. Allergen immunotherapy in children user’s guide. Pediatr Allergy Immunol. 2020;31(S25):1–101. doi:10.1111/pai.13189
112. Tosca M, Licari A, Olcese R, et al. Immunotherapy and asthma in children. J Asthma. 2018;6. doi:10.3389/fped.2018.00231
113. Cox L, Li J, Nelson H, Lockey R. Allergen immunotherapy: a practice parameter second update. J Allergy Clin Immunol. 2007;120(3):S25–S85.
114. Silverstein M, Hsu H, Bell A. Addressing social determinants to improve population health. JAMA. 2019;322(24):2379. doi:10.1001/jama.2019.18055
115. Bateman E, Hurd S, Barnes P, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2018;51(2):0751387.
116. National Heart Lung and Blood Institute. Expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma–Summary report 2007. J Allergy Clin Immunol. 2007;120(5):S94–S138. doi:10.1016/j.jaci.2007.09.029
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.