Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
ALK-Negative Systemic Anaplastic Large Cell Lymphoma with Cutaneous Involvement Initially Mimicking Primary Cutaneous Disease: A Case Report
Authors Wang H ![]() , Li Z, Zhuang S
, Li Z, Zhuang S
Received 1 May 2026
Accepted for publication 8 July 2026
Published 13 July 2026 Volume 2026:19 618913
DOI https://doi.org/10.2147/CCID.S618913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Huijing Wang, Zongyang Li, Shubo Zhuang
Department of Cosmetic Dermatology, The First Hospital of Tsinghua University, School of Clinical Medicine, Tsinghua Medicine, Tsinghua University, Beijing, People’s Republic of China
Correspondence: Shubo Zhuang, Department of Cosmetic Dermatology, The First Hospital of Tsinghua University, School of Clinical Medicine, Tsinghua Medicine, Tsinghua University, Beijing, People’s Republic of China, Tel +8613910889011, Email [email protected]
Abstract: Anaplastic large cell lymphoma (ALCL), a subgroup of T-cell non-Hodgkin’s lymphoma, is a relatively uncommon malignancy with a highly variable prognosis. Systemic ALK-negative status and high Ki-67 expression are generally associated with poor outcomes in ALCL patients. Systemic ALK-negative ALCL presenting initially with cutaneous involvement is rare, with only a few cases reported in the literature. The aggressive clinical course of systemic ALK-negative ALCL with cutaneous lesions contrasts sharply with the indolent behavior of primary cutaneous ALCL (C-ALCL). Accurate distinction requires integration of histopathological and immunophenotypic findings. In particular, negativity for cutaneous lymphocyte antigen (CLA) is a useful discriminator, as primary C-ALCL typically expresses CLA while systemic cases often do not. Accumulating more clinical data is essential to better characterize this entity and guide therapeutic decisions. Here, we report a case of aggressive ALK-negative systemic ALCL that presented with cutaneous nodules as the initial manifestation, clinically mimicking primary C-ALCL.
Keywords: anaplastic large cell lymphoma, ALK-negative, cutaneous involvement, case report, poor prognosis
Introduction
Anaplastic large cell lymphoma (ALCL) is a distinct subtype of T-cell non-Hodgkin lymphoma characterized by variable clinical behavior.1 According to the expression of anaplastic lymphoma kinase (ALK), ALCL is classified into ALK-positive and ALK-negative groups, with the latter typically occurring in older adults and often associated with a more aggressive course and poorer prognosis.1,2 ALK-negative ALCL is a genetically heterogeneous disease, and its clinical outcomes are widely disparate, underscoring the need for precise diagnosis and risk stratification.2 Cutaneous presentation in systemic ALCL is rare, and its frequency has not been well established in large epidemiological studies. Although systemic ALCL primarily involves lymph nodes, cutaneous manifestations can occasionally be the initial presenting feature, posing a diagnostic challenge. In particular, ALK-negative systemic ALCL presenting with skin lesions may closely mimic primary cutaneous ALCL (C-ALCL), a clinically indolent entity with an excellent prognosis — approximately 90% 5-year overall survival.3 Primary C-ALCL typically expresses CLA, whereas systemic ALCL often lacks it, providing a valuable immunophenotypic clue. This morphological and immunophenotypic overlap can lead to misdiagnosis and inappropriate management, as treatment strategies differ substantially between localized cutaneous disease and systemic lymphoma. Therefore, a high index of suspicion and a thorough systemic workup are mandatory for any patient presenting with CD30-positive lymphoproliferative skin lesions. Herein, we report a case of ALK-negative systemic ALCL that first manifested with multiple cutaneous nodules, highlighting the importance of comprehensive clinicopathological evaluation to distinguish systemic involvement from primary cutaneous disease and to guide timely, appropriate therapy.
Case Report
A 50-year-old female presented with a 40-day history of multiple cutaneous nodules. She reported no fever or night sweats but had experienced unintentional weight loss of approximately 10 kg. Her medical history was notable only for schizophrenia, and her family history was unremarkable. Physical examination revealed multiple purplish-red nodules on the left lower extremity and abdomen, the largest measuring 4.5×2.8 cm (Figure 1).
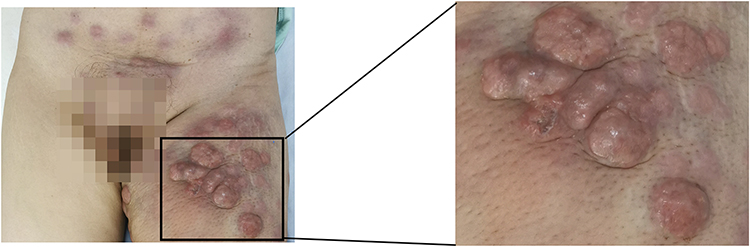 |
Figure 1 Multiple purplish-red nodules on the left lower extremity and abdomen. |
Laboratory tests showed elevated levels of several tumor markers, including carcinoembryonic antigen (16.5 ng/mL), human epididymal protein 4 (75.19 pmol/L), neuron-specific enolase (108 ng/mL), and carbohydrate antigen 15–3 (27 U/mL). These non-specific elevations were considered a reactive phenomenon in the setting of aggressive malignancy and did not contribute diagnostically. Complete blood count and comprehensive metabolic panel were within normal limits.
Imaging studies confirmed widespread systemic disease. Superficial lymph node ultrasonography revealed multiple enlarged lymph nodes in bilateral supraclavicular, axillary, and inguinal regions. Thoracoabdominal CT demonstrated generalized lymphadenopathy involving the axillae, mediastinum, retroperitoneum, and pelvis, along with multiple subcutaneous soft-tissue lesions in the abdominopelvic wall and bilateral inguinal region. PET/CT further delineated the extent of disease. It revealed multiple hypermetabolic lymph nodes of varying sizes. Hypermetabolic nodules or masses were also identified in the subcutaneous tissue, skeletal muscles, nasopharynx, right upper lung lobe, left breast, and uterus. These findings were consistent with disseminated extranodal involvement by lymphoma. Additionally, the PET/CT showed left-sided pneumothorax with incomplete lung expansion and bilateral small pleural effusions, with a left chest tube in situ. Diffuse subcutaneous edema was noted, likely attributable to impaired lymphatic drainage. Diffuse cerebral hypometabolism was also observed, presumably related to the patient’s underlying schizophrenia.
Histopathological examination of a skin biopsy specimen showed dermal infiltrate of large, pleomorphic lymphoid cells. Frequent mitotic figures, including atypical forms, were observed (Figure 2A and B). Immunohistochemistry demonstrated strong and uniform positivity for CD30 (Figure 2C) and a very high proliferation index (Ki-67 approximately 90%, Figure 2E), with focal staining for CD3 and CD4. Crucially, the tumor cells were negative for ALK (Figure 2D), cutaneous lymphocyte antigen (CLA, Figure 2F). Other negative markers included EMA, CD20, CD21, CD56, CD117, CD123, TIA-1, Granzyme B, MPO, CK, and Lysozyme. The immunophenotype (CD30+, ALK-, CLA-) in conjunction with the systemic distribution strongly supports a diagnosis of systemic ALK-negative ALCL rather than primary cutaneous disease.
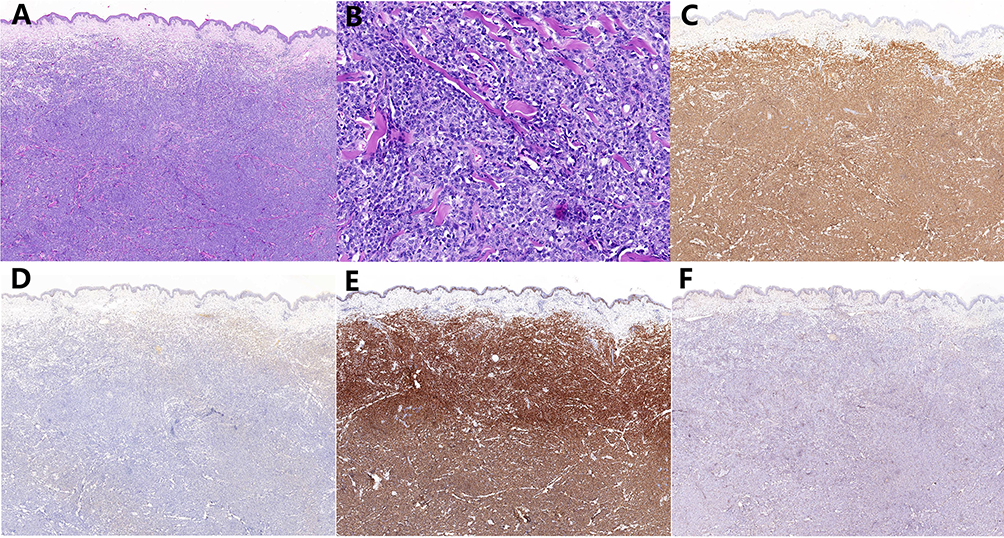 |
Figure 2 (A) Large, pleomorphic lymphoid cells infiltrated in dermis, (HE×20). (B) Large areas exhibited marked cellular atypia, with high nucleocytoplasmic ratio, enlarged cells, and frequent mitotic figures, (HE×200). (C) CD30 (positive, IHC×20). (D) ALK (negative, IHC×20). (E) Ki-67 (~90% positive, IHC×20). (F) CLA (negative, IHC×20). |
Based on these findings, the patient was diagnosed with ALK-negative systemic anaplastic large cell lymphoma, staged as IVB with an International Prognostic Index (IPI) score of 4, indicating high-risk disease. Given her poor performance status and the extensive, rapidly progressive nature of her disease, palliative treatment was initiated with oral prednisone (50 mg daily) and chidamide (30 mg twice weekly) for symptom palliation. Unfortunately, the disease progressed rapidly, and the patient died two months later.
This case report was prepared in accordance with the CARE (CAse REport) guidelines.
Discussion
Anaplastic large cell lymphoma (ALCL) is a CD30-positive T-cell neoplasm that primarily involves lymph nodes.1 According to ALK expression, ALCL is categorized as ALK-positive or ALK-negative. ALK-negative ALCL is genetically heterogeneous, harboring various molecular alterations such as rearrangements in DUSP22, TP63, or lacking any specific drivers (triple-negative), each associated with distinct prognostic implications.2 It typically affects older adults (median age 58 years).1,2 Systemic symptoms such as weight loss and night sweats are common.4 While the prognosis of ALK-negative ALCL is generally considered poorer than its ALK-positive counterpart, it is now recognized that outcomes are highly variable and not uniformly adverse, largely depending on the underlying genetic subtype.2,5 Although cutaneous involvement is uncommon in ALCL, its presence often signals a higher risk of adverse outcomes and necessitates a careful diagnostic approach.
The differential diagnosis for a CD30-positive lymphoproliferation with skin involvement is broad and clinically critical. Beyond primary C-ALCL and ALK-positive ALCL, other entities must be considered. These include lymphomatoid papulosis (LyP), particularly its type C form, which can be histologically indistinguishable from ALCL but has a benign, recurrent clinical course. Additionally, peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS), and classical Hodgkin lymphoma (particularly in cases with extranodal presentation) should be ruled out. Although breast implant-associated malignancies represent an important differential in patients with peri-breast lesions and implant history, this was not relevant to our patient and is therefore not discussed in detail.6 Accurate differential diagnosis is crucial because management differs substantially: localized skin tumors are often managed with surgical excision or radiotherapy, whereas systemic lymphomas require multi-agent chemotherapy or targeted agents.
The distinction between primary C-ALCL and systemic ALK-negative ALCL with secondary cutaneous involvement is paramount. Primary C-ALCL is almost always ALK-negative but follows an indolent course and is confined to the skin at the time of diagnosis. In contrast, ALK-negative systemic ALCL with cutaneous involvement often behaves aggressively.7 The 5-year overall survival is approximately 90% for primary C-ALCL versus around 49% for ALK-negative systemic ALCL, highlighting the prognostic divergence.3 Immunohistochemistry provides useful clues, as primary C-ALCL typically expresses CLA, whereas systemic ALCL often lacks it, as seen in our case. This CLA negativity, combined with systemic staging, was the key to correctly classifying our patient’s disease. Only a few reported cases of localized cutaneous ALK-negative systemic ALCL have shown an indolent course, representing rare exceptions.8–10 Several recent case reports have similarly underscored the diagnostic challenge posed by ALK-negative systemic ALCL with initial cutaneous manifestations.11,12 Meanwhile, even primary cutaneous ALCL can present with unusual clinical features, such as penile involvement, and may require individualized treatment approaches, further emphasizing the importance of accurate distinction between primary and systemic disease.13
The aggressive course in our patient aligns with the generally poor prognosis associated with systemic ALK-negative ALCL. Common causes of mortality in this context include rapid disease progression, infectious complications secondary to immunosuppression, and organ failure due to lymphomatous infiltration.5 Current treatment options for systemic ALK-negative ALCL include frontline multi-agent chemotherapy regimens such as CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) or CHOEP (CHOP plus etoposide). For relapsed or refractory disease, novel targeted therapies, most notably the anti-CD30 antibody-drug conjugate brentuximab vedotin, have demonstrated significant efficacy and are now incorporated into treatment paradigms.14 Regrettably, our patient’s poor performance status precluded the use of intensive multi-agent chemotherapy. This should be acknowledged as a factor that may have influenced the clinical outcome, as definitive systemic therapy could not be administered.
This case has several limitations that should be acknowledged. Notably, additional molecular characterization—including analysis of DUSP22 and TP63 rearrangement status as well as Epstein-Barr virus (EBV)-encoded small RNA (EBER) in situ hybridization—was not performed. The absence of these data precludes precise genetic subclassification of the ALK-negative ALCL, which is increasingly relevant for prognostication and may have therapeutic implications. Furthermore, the aggressive and rapidly progressive disease course limited the opportunity for more comprehensive diagnostic workup and prevented the administration of intensive chemotherapy, which may have influenced the outcome.
Conclusion
In summary, cutaneous involvement in systemic ALCL is rare but clinically significant. Even when skin lesions dominate, determining whether the disease is primary cutaneous or systemic in origin is critical, particularly in ALK-negative cases. Our case illustrates an aggressive, rapidly progressive form of ALK-negative systemic ALCL that presented initially with skin lesions and followed a fatal course with rapid progression despite treatment. Misclassification of such cases as primary cutaneous ALCL may lead to underestimation of disease severity and the selection of suboptimal treatment strategies. This underscores the importance of combining clinical suspicion with thorough histopathological evaluation to ensure accurate diagnosis and appropriate treatment.
Abbreviations
ALCL, anaplastic large cell lymphoma; C-ALCL, primary cutaneous anaplastic large cell lymphoma; ALK, anaplastic lymphoma kinase; CT, computed tomography; PET-CT, positron emission tomography – computed tomography.
Ethics Approval and Informed Consent
Written informed consent for the publication of the case details and accompanying images was signed by the patient when she had full decision-making capacity, prior to her death. Publication of the case details was approved by The First Hospital of Tsinghua University.
Acknowledgments
We thank the patient and physicians for participating in our study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang X, Zhou J, Han X, et al. Update on the classification of and diagnostic approaches to mature T-cell lymphomas. Arch Pathol Lab Med. 2022;146(8):947–5. doi:10.5858/arpa.2021-0143-RA
2. R PCE, S JE, W SJ, et al. ALK-negative anaplastic large cell lymphoma is a genetically heterogeneous disease with widely disparate clinical outcomes. Blood. 2014;124(9):1473–1480. doi:10.1182/blood-2014-04-571091
3. Savage KJ, Harris NL, Vose JM, et al. ALK- anaplastic large cell lymphoma is clinically and immunophenotypically different from both ALK+ ALCL and peripheral T-cell lymphoma, not otherwise specified: report from the international peripheral T-cell lymphoma project. Blood. 2008;111:5496. doi:10.1182/blood-2008-01-134270
4. Abdul Rahman S, Loutfi K, Turk T, et al. A challenging case of ALK-negative anaplastic large cell lymphoma in a 12-year-old boy: a rare case report from Syria. Ann Med Surg. 2022;79:104085. doi:10.1016/j.amsu.2022.104085
5. Pina-Oviedo S, Ortiz-Hidalgo C, A C-ZA, et al. ALK-negative anaplastic large cell lymphoma: current concepts and molecular pathogenesis of a heterogeneous group of large T-cell lymphomas. Cancers. 2021;13(18):4667. doi:10.3390/cancers13184667
6. D’Orsi G, Giacalone M, Calicchia A, et al. BIA-ALCL and BIA-SCC: updates on clinical features and genetic mutations for latest recommendations. Medicina. 2024;60(5):793. doi:10.3390/medicina60050793
7. Querfeld C, Khan I, Mahon B, et al. Primary cutaneous and systemic anaplastic large cell lymphoma: clinicopathologic aspects and therapeutic options. Oncology. 2010;24(7):574–587.
8. Metcalf RA, Bashey S, Wysong A, et al. Intravascular ALK-negative anaplastic large cell lymphoma with localized cutaneous involvement and an indolent clinical course: toward recognition of a distinct clinicopathologic entity. Am J Surg Pathol. 2013;37(4):617–623. doi:10.1097/PAS.0b013e318280aa9c
9. Wang L, Li C, Gao T. Cutaneous intravascular anaplastic large cell lymphoma. J Cutan Pathol. 2011;38(2):221–226. doi:10.1111/j.1600-0560.2010.01538.x
10. Iacobelli J, V SD, Tesfai Y, et al. Cutaneous intravascular anaplastic large T-cell lymphoma: a case report and review of the literature. Am J Dermatopathol. 2012;34(8):e133–e138. doi:10.1097/DAD.0b013e31824fec43
11. Ahuja R, Patel V, Mallick S, et al. Anaplastic Lymphoma Kinase (ALK)-negative systemic anaplastic large cell lymphoma presenting as zosteriform skin nodules. Ind J Dermatol Venereol Leprol. 2024;90(3):358–362. doi:10.25259/IJDVL_1166_2022
12. Abdallah J, Jabareen M, Alhroub W, et al. ALK-negative anaplastic large cell lymphoma with rare scalp involvement: a case report and literature review. J Investig Med High Impact Case Rep. 2025;13:23247096251388258. doi:10.1177/23247096251388258
13. Al-Bitar A, Alomar Albrazi A. Anaplastic large cell lymphoma in the penis: a case report and review of literature. J Med Case Rep. 2025;19:586. doi:10.1186/s13256-025-05520-8
14. Domingo-Domènech E, Pro B, Illidge T, et al. Brentuximab vedotin plus chemotherapy for the treatment of front-line systemic anaplastic large cell lymphoma: subgroup analysis of the ECHELON-2 study at 5 years’ follow-up. Blood Cancer J. 2025;15(1):129. doi:10.1038/s41408-025-01329-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.