Back to Journals » Psychology Research and Behavior Management » Volume 13
Alcohol Use Disorder and Associated Factors Among Jimma University Undergraduate Students
Authors Alemu D, Soboka M, Tesfaye E ![]() , Ahmed G
, Ahmed G ![]() , Tesfaye Y
, Tesfaye Y ![]()
Received 27 February 2020
Accepted for publication 10 July 2020
Published 27 July 2020 Volume 2020:13 Pages 609—618
DOI https://doi.org/10.2147/PRBM.S251510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Einar Thorsteinsson
Daniel Alemu,1 Matiwos Soboka,2 Elias Tesfaye,2 Gutema Ahmed,2 Yonas Tesfaye2
1Department of Psychiatry, Haramaya University, Harar, Harari, Ethiopia; 2Department of Psychiatry, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Yonas Tesfaye Tel +251910107507
Email [email protected]
Purpose: Harmful alcohol use among University students is a problem throughout the world. However, little is known about alcohol use disorders among JFD university students in Ethiopia. Therefore, this study aimed to assess the prevalence and associated factors of alcohol use disorder (AUD) among Jimma University undergraduate students.
Methods: Institution-based cross-sectional study was conducted among Jimma university students. Data were collected from 741 sampled students who were selected through a multi-stage stratified sampling technique. Alcohol Use Disorder Identification Test (AUDIT), Oslo 3 items social support scale (OSS-3), and Kessler-6 (K6) tools were used to assess alcohol use disorders, social support, and psychological distress, respectively. Data were analyzed through SPSS version 20.0. Bivariate and multivariate logistic regression analyses were conducted and adjusted odds ratio (AOR) at a 95% confidence interval (CI) was used to determine the independently associated factors of AUD.
Results: The overall prevalence of AUD among Jimma University undergraduate students was 26.5%. There was a positive and independent association between AUDs and being single AOR= 1.98, 95% CI [1.21, 3.22], having a history of mental illness AOR= 1.98, 95% CI [1.04, 3.75], having a history of suicidal attempt AOR= 3.63, 95% CI [1.18, 11.11], smoking cigarette AOR= 5.04, 95% CI [2.02, 12.57], having peer pressure to drink alcohol AOR= 2.72, 95% CI [1.76, 4.19] and presence of mental distress AOR= 2.81, 95% CI [1.83, 4.32].
Conclusion: The findings of this study showed that the prevalence of AUD was high in the sampled undergraduate students of Jimma University. AUD was positively associated with mental, substance, and behavioral risk factors. Therefore, concerted actions needed to emplace to increase the student’s awareness of the effect of harmful alcohol use. Moreover, it is recommended that further studies need to be conducted to develop strategies for evidence-based interventions.
Keywords: substance use disorder, alcohol use disorders, mental distress, risky sexual behavior, Jimma, Ethiopia
Introduction
Alcohol use disorder is a problem among university students worldwide.1,2 Across the world, it has been reported that university students’ alcohol consumption is higher than their non-university peers3,4 Alcohol misuse was also reported as a strong predictor of students’ mental health in which, it was attributable to increased depressive symptoms and attempted suicide.5,6 Tobacco and alcohol use were in the 2nd and 6th place in a 2013 ranking of the top 25 leading health risk factors in the world, respectively.6,7 More than 27 million, which is 0.6% of the world adult population currently believed to have alcohol and other drugs such as Khat (amphetamine-like local stimulant abused drug) and tobacco-related health problems.8,9
The use of substances such as alcohol, chewing khat leaves, and smoking cigarettes have become one of the rising major public health and socio-economic problems worldwide10,11 Alcohol use disorder was attributed to about 3.8% of all deaths (2.5 million) and about 4.5% of disability-adjusted life years lost (DALYs) (69.4 million).12,13
A study done in the US and Canadian showed a prevalence of lifetime and past-year alcohol use among university students to be 87% versus 81%, and 92% versus 86%, respectively.14 The prevalence of hazardous use of alcohol among undergraduate students at a public university in Brazil was 24%.15 Patterns of alcohol use on a South African university campus showed 8.5% of the undergraduate students have harmful alcohol consumption.16
The relationship between alcohol consumption and perceived social support (PSS) is complex; perhaps even more so among those with AUD. Epidemiological data suggest that social network size and diversity are smaller among those with alcohol dependence.17 Moreover, lower levels of perceived social support can influence drinking rates. PSS has been also shown to be associated with reduced rates of alcohol use and alcohol-related problems in non-treatment seeking adolescents and adults.17,18
Excessive alcohol intake among college and University students found to be associated with a variety of adverse consequences like poor academic achievement, drop out, violence, rape, assault, increased level of mental distress, and sexually transmitted diseases including Acquired Immunodeficiency Syndrome (AIDS).19–22
However, information is scarce regarding the prevalence of alcohol use disorders and its associated factors among Ethiopian University students. Thus, this study was attempted to generate information that helps for evidence-based intervention and further assists interested researchers in the topic area as baseline data for future studies.
Participants and Methods
Participants
The study was conducted at Jimma University, which is located 352 km southwest of the capital city of Ethiopia, Addis Ababa. Jimma University’s main campus has four colleges (“College of Natural and Computational Science,” “College of Medicine and Health Science,” “College of Social Science and Humanity” and “College of Law and Governance”). A total of 31 departments and 6155 regular undergraduate students were enrolled on the main campus. Sampled regular undergraduate main campus students who were enrolled in the 2016/17 academic calendar were the study population. The study was conducted from April 1–20, 2016.
Materials
Measures
The questionnaire consists of five sections; demographic, alcohol use disorder, social support, mental distress, and risky sexual behaviors.
Demographics include gender, age, marital status, ethnicity, religion, academic year, colleges, and current living status.
Alcohol use disorder was measured by the alcohol use disorder identification test (AUDIT). The AUDIT was developed by the World Health Organization (WHO) as a simple method of screening for the excessive or pathological pattern of alcohol drinking and to assist in brief assessment, AUDIT is a screening instrument and not diagnostic interview.23 The AUDIT has proven to be accurate in detecting pathological alcohol use in the University students.24 The measurements of local alcoholic beverages were converted to milliliters based on previous studies.25 Then, the measured amount of alcohol was converted to a standard drink after calculating the mass and volume of the alcohol. Beer, “draft” and wine (bottle/big/small) were converted to standard drinks based on their alcoholic content. Local drinks such as “Tella” (one of the Ethiopian traditional beverages, brewed from various grains and different cereals which includes; barely, corn, wheat, sorghum, maize, and Gesho (Rhamnus prinioid))26,27 “Areke” (a local colorless, traditional alcoholic beverage that is distilled from the fermentation of different grains)26 and “Tej” (A local home processed, fermented alcoholic beverage, prepared from honey, sugar, water, and leaves of Gesho (Rhamnus prepoides)26 were also considered as alcohol drinks in the study. A total AUDIT score of eight or more was used to define alcohol use disorders.25,28
Oslo 3 items social support scale (OSS-3) was used to measure the level of social support, the scale has good psychometric properties. A score ranging between 3 and 8 is classified as poor social support, a score between 9 and 11 as intermediate (moderate) social support, and a score between 12 and 14 indicates strong social support.29
Mental distress was measured by the Kessler-6 mental distress scale, cut-off points 5 or more was used to screen mental distress.30
Substance use was measured by current alcohol use (when the respondents used alcohol in the last 3 months) and lifetime alcohol use (when the respondents used alcohol even once in their lifetime) additionally, family history of drinking alcohol considered if any of the respondent’s family members (father, mother, brother or sister) drinks alcohol. History of mental illness assessed through a question, have you ever diagnosed with mental health problems?
Risky sexual behaviors (RSB) questions were developed by reviewing different literature in the topic area. RSB was considered if the respondents engaged in behaviors that include engaging in sexual activity from an early age, inconsistent use of condoms during sexual intercourse, having sex with commercial sex workers, and the tendency to have multiple sexual partners. An individual with at least one of these behaviors was considered to have risky sexual behavior.19,22,31
Design
A quantitative cross-sectional study was conducted.
Procedures
Sampling
The sample size was calculated using the single population proportion formula. Cochran (1977) developed a formula to calculate a representative sample for proportions as n0= Z2 pq/e2 where n0 is the sample size, z is the selected critical value of desired confidence level, p is the estimated proportion of alcohol use disorder 50%; to get the maximum sample size, q= 1-p and e is the desired level of precision p = 0.5. Hence, q= 1–0.5 = 0.5; e = 0.05; z =1.96,32 therefore n= (1.96)2*0.5 (1–0.5)/(0.05)2 = 384. Since the study design was a multistage sampling technique, the design effect of 2 was taken to multiply the calculated sample size. Finally, with the addition of 5% of contingency for non-response, the final sample size becomes 806.
Jimma University has three campuses (“Main campus”, “Jimma Institute of Technology”, “Business and economics campus”). The main campus was selected by the lottery method. Out of the total 31 departments in the four colleges, 18 departments were selected by using the lottery method. Then, the samples were further stratified proportionally by the number students in each department and year of study, finally, a total of 806 students were selected through a simple random sampling technique, taking the student registry list as a frame. Figure 1
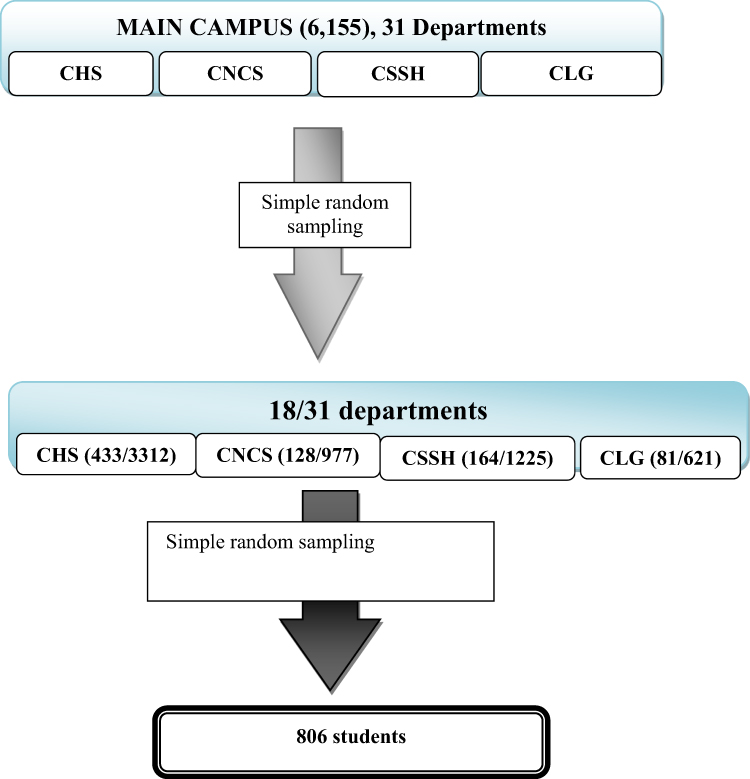 |
Figure 1 Schematic presentation of the sampling procedure, Jimma University’s main campus students, May 2016. A total of 6155 regular undergraduate students were in the main campus. The main campus comprised, College of health science (CHS), college of natural and computational science (CNCS), college of social science and Humanities (CSSH) and the college of law and governance (CLG). Out of the total of 31 departments in four colleges in the campus, 18 departments were selected by using simple random sampling lottery method, accordingly 433 respondents from a total of 3312 students in CHS, 128 from 977 in CNCS,164 from 1225 in CSSH and 81 from 621 in CLG included considering proportional allocation to the number of student in the college. Finally, simple random sampling method was used to get the final sample size of 806. Abbreviations: CNCS, College of Natural and Computational Science; CMHS, College of Medicine and Health Science; CSSH, College of Social Science and Humanity; CLG, College of Law and Governance. |
Data
Data were collected through a structured, pretested, and self-administered questionnaire. The data collection process was supervised by three professionals with a bachelor of science degree in psychiatry nursing after 1 day of training on administration of the study instruments, consent form, and maintaining confidentiality. The questionnaire was developed in English and then translated into local languages Amharic and Afan Oromo then back-translation into the English language was undertaken by blinded experts of the languages, respectively. The pretest was conducted on 5% of the sample size in the college of Agriculture and veterinary medicine campus students 1 week before the actual data collection period. Based on the pretest, unclear and ambiguous questions were revised, edited, and those found to be unclear or confusing were modified. In this study, the AUDIT tool has 0.81 Cronbach’s alpha scores. Moreover, the data collection process was closely followed by data collection supervisors.
Statistical Analysis
Data were entered into Epi data version 3.1 data entry software and exported to statistical package for social science (SPSS) version 20.0 for analysis. Bivariate and multivariate logistic regression analyses were done to determine the associated factors of AUD. First, each independent variable was entered into bivariate regression analysis; then, variables associated with the outcome variable were entered into a multivariable logistic regression to control the confounders. The degree of association between dependent and independent variables was assessed using the adjusted odds ratio with 95% CI. Moreover, the effect size was measured to determine the relationship between the outcome and explanatory variables.
Ethical Considerations
The study protocol was approved by the Institutional Review Board of Jimma University, Institute of Health (reference number IHRPGP/64/2016). The ethical review board of Jimma University also approved participants under the age of 18 years to be able to provide informed consent on their behalf. The letter of Permission was obtained from all relevant authorities of the colleges and sampled departments. The involvement of the study participants was voluntarily and participants were informed of the right to withdraw anytime from the study, moreover written informed consent was obtained from every study participant before data collection. The students were not paid or received any credit for participating in the survey. The data collection was undertaken confidentially and responses were kept private and anonymous. The study was conducted as per the Helsinki declaration.
Result
Socio-Demographic Characteristics of the Participants
Out of 806 sampled participants, 741 of them returned the properly filled questionnaires, making a response rate of 91.93%.
Of the total participants (62.1%, n= 460) were male. The mean age of the respondents was 22.68. Most (56%, n= 415) of the study participants were orthodox Christian religion followers and belong to the Oromo ethnic groups (42.2%, n= 313). Almost all (91.9%, n= 681) of the study participants were living in a University dormitory. Out of the total participants, the majority (28.6%, n= 212) were first-year students and from the college of health science (55.2%, n= 409). See Table 1 for more detail.
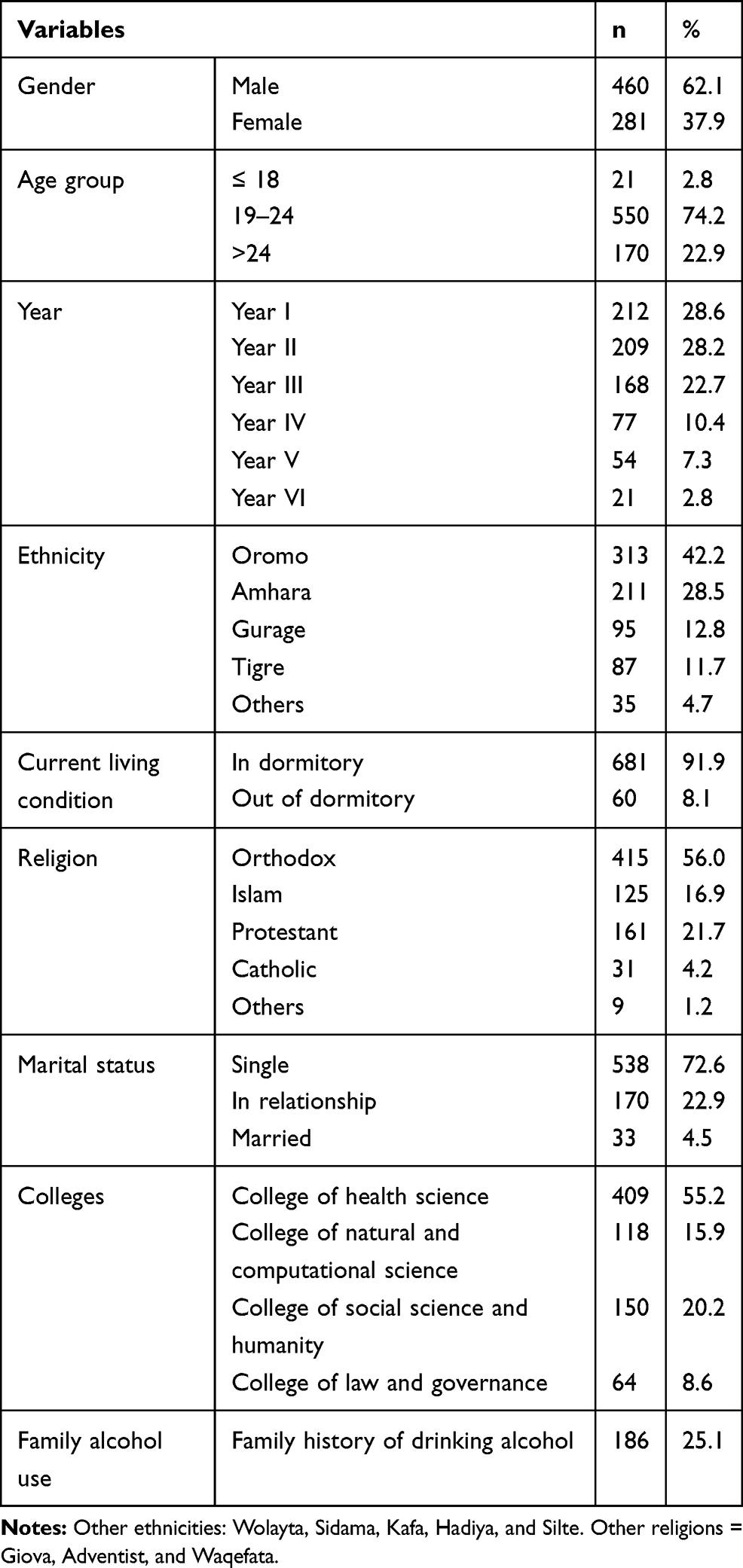 |
Table 1 Socio-Demographic, Economic and Family Alcohol Use Characteristics of Jimma University Main Campus Undergraduate Students, April 2016 |
Reasons for Starting Alcohol Use
Out of the total participants with AUDs, the majority started drinking alcohol due to peer pressure (54.6%, n= 107), followed by to enhance social interaction/social gathering (24.5%, n= 48) and easy availability of alcohol (11.7%, n= 23). A quarter of the study participants (25.1%, n= 186) had a family history of drinking alcohol. See Table 2 for more detail.
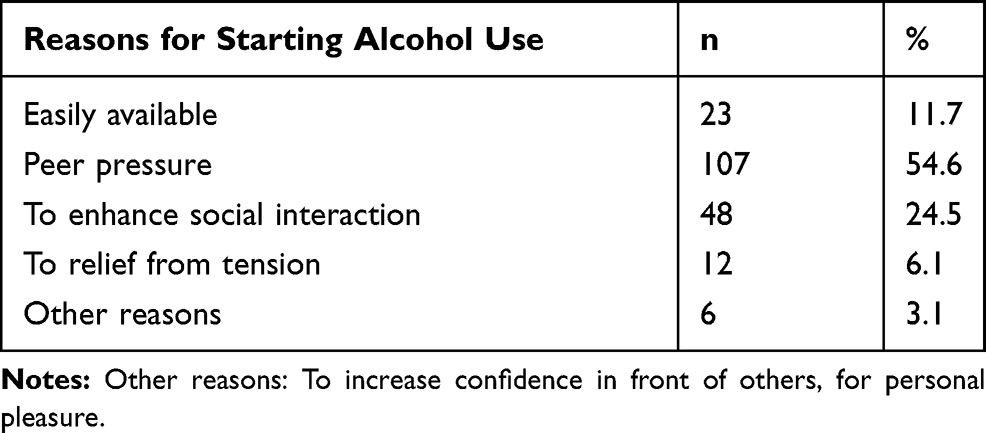 |
Table 2 Reasons for Drinking Alcohol Among Participants Who Had AUDs, Jimma University Main Campus Undergraduate Students, April 2016 |
Prevalence of Alcohol Uses Disorders
The prevalence of alcohol use disorder among Jimma University undergraduate students was (26.5%, n= 196). The prevalence of AUDs among males and females’ students was (32.6%, n= 150), and (16.4%, n= 46) respectively. A total of (28.1%, n = 75) study participants who earned higher monthly pocket money (≥ 500 Ethiopian birr) had AUD. The prevalence of AUDs among the study participants who lived in the University dormitory and outside the campus was (25.4%, n = 173), and (38.3%, n = 23) respectively. Out of (32.5%, n= 242) study participants who had poor social support, (41.3%, n= 81) had AUDs. A total of (40.75%, n= 302) respondents were reported to have risky sexual behavior, of this (64.6%, n= 195) had AUD. See Table 3 for more detail.
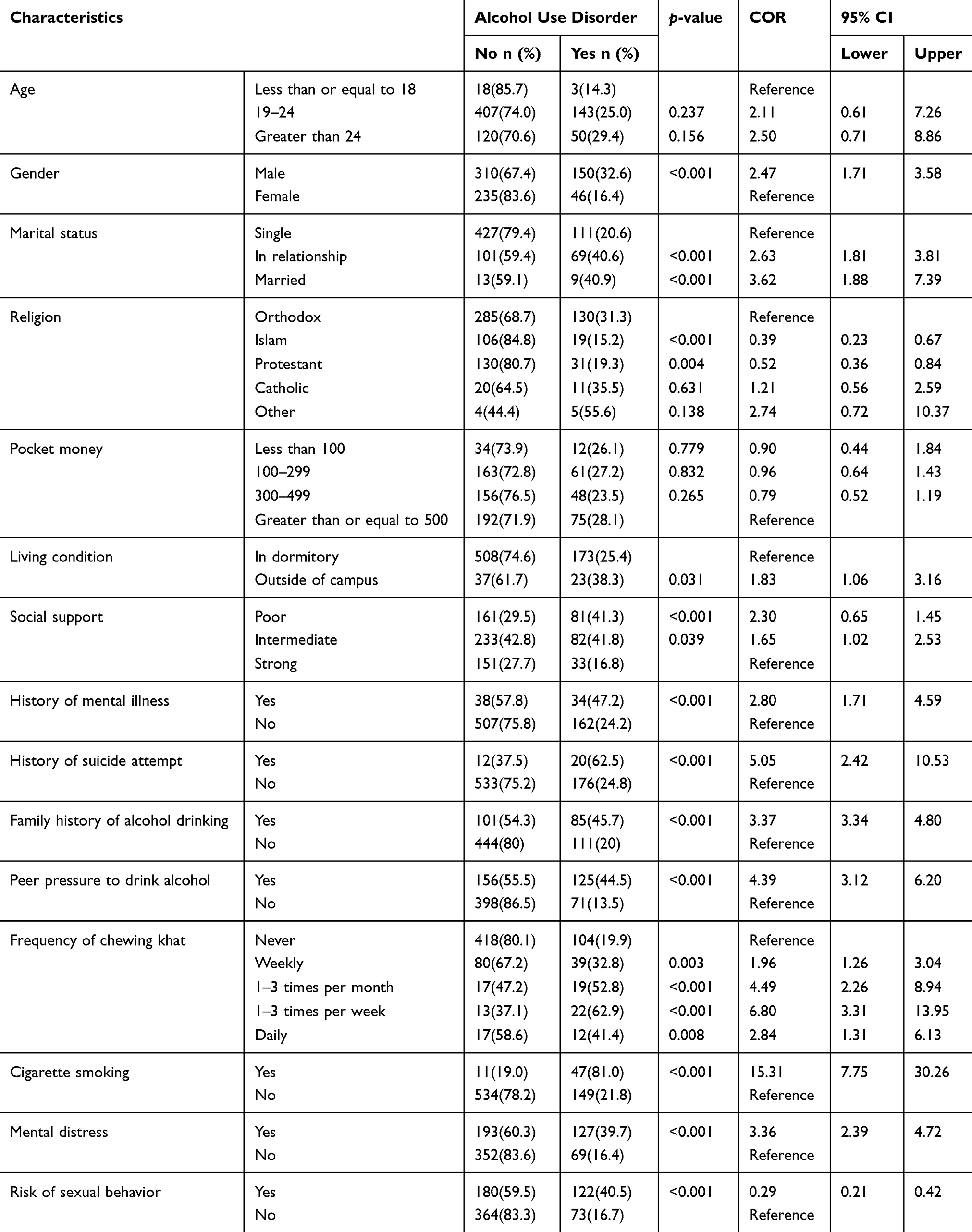 |
Table 3 Bivariate Analysis of Factors Associated with AUDs Among Jimma University Main Campus Undergraduate Students, April 2016 |
Associated Factors of Alcohol Use Disorder
In bivariate logistic regression analysis, gender, marital status, religion, living condition, social support, history of suicide attempt, history of mental illness, family history of alcohol drinking, presence of peer pressure to drink alcohol, frequency of chewing khat, cigarette smoking level of mental distress and risk of sexual behavior were found to be associated with alcohol use disorder. See Table 3 for more detail.
After adjusting for the potential confounders, multivariate logistic regression analysis showed, being male was approximately two time more likely to have AUD than female counterpart AOR = 2.27, 95% CI [0.37, 3.76], likewise being in relationship was nearly twice increased having AUD than single counterpart AOR= 1.98, 95% CI [1.21, 3.22], similarly being married was nearly three time increased the risk of AUD than single counterpart AOR= 2.88, 95% CI [1.17, 7.09]. Additionally having history of mental illness nearly two times increased the risk of AUD than its counterpart AOR= 1.98, 95% CI [1.04, 3.75], likewise history of attempting suicide increased the odd of having AUD more than three and half times AOR= 3.63, 95% CI [1.18, 11.11], similarly having peer pressure to drink alcohol increased the risk of AUD by approximately three times than its counterpart AOR= 2.72, 95% CI [1.76, 4.19], moreover chewing khat 1–3 times per week increased the odds of having AUD by nearly three times compared to the never chewed counterpart AOR= 2.82, 95% CI [1.16, 6.83], likewise cigarette smoking increased acquiring AUD by five times compared to the non-smoker counterpart AOR= 5.04, 95% CI [2.02, 12.57] and finally presence of mental distress increased having AUD by approximately three time than its counterpart AOR= 2.81, 95% CI [1.83, 4.32]. Moreover, the effect size association analysis showed; sex, marital status, history of mental illness, peer pressure to drink alcohol, chewing Khat 1–3 times a week and mental distress had medium effect size association with AUD (OR≥ 1.44 and < 4.27), whereas cigarette smoking had strong effect size association with AUD (OR≥ 4.27). See Table 4 for more detail.
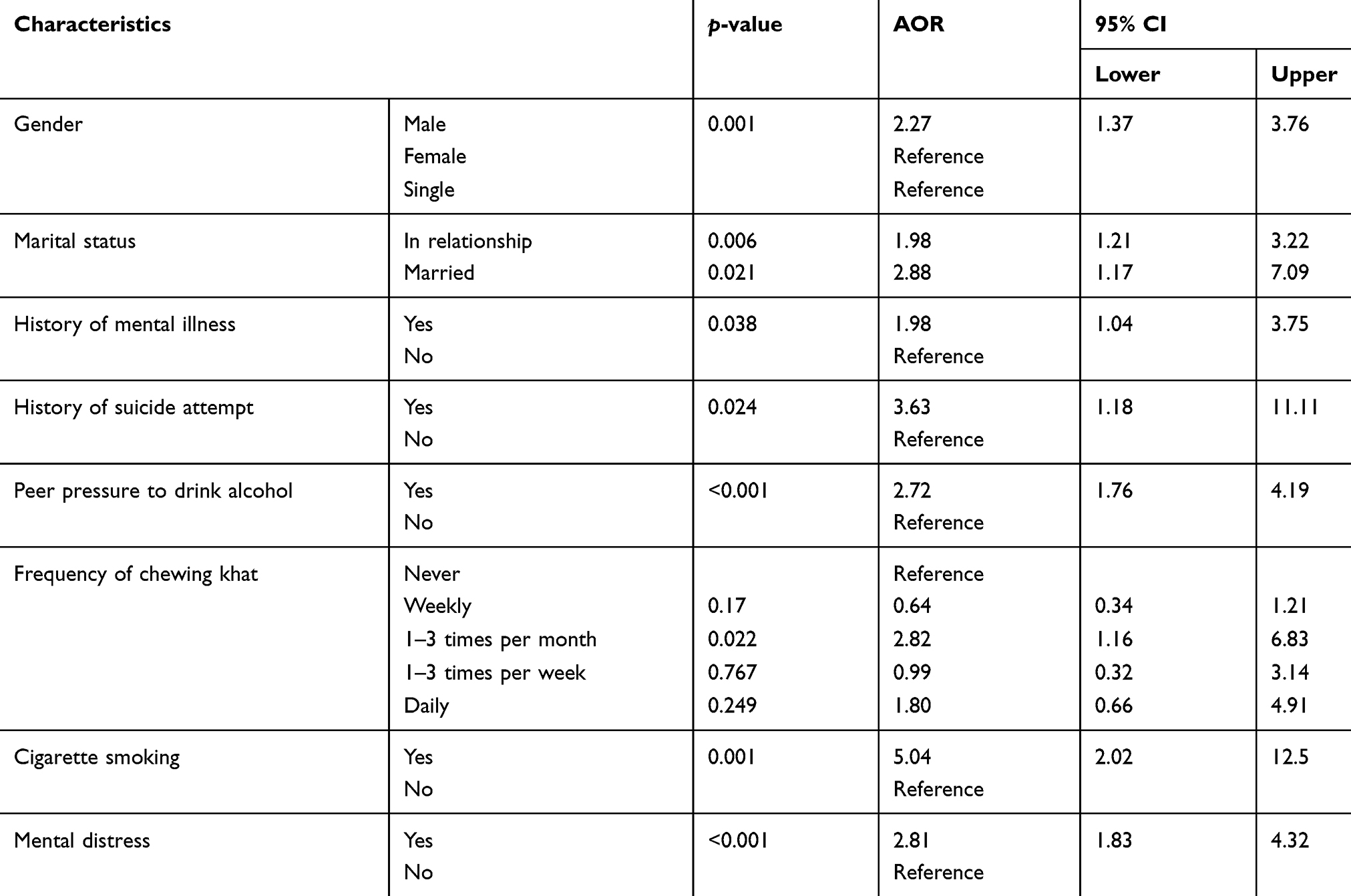 |
Table 4 Multivariate Logistic Regression Analysis of Factors Independently Associated Factors with AUDs Among, Jimma University Main Campus Undergraduate Students, April 2016 |
Discussion
In this study, the prevalence of alcohol use disorder was 26.5%, the finding was supported by the study done in Colombia university students, in which 20.5% of the respondents had harmful consumption and 14.9% were at risk of dependence,33 likewise a study done in the USA showed 18% of US college students suffered from AUD.34 Similar findings were also reported from the studies done in Wolaita University Students and Morocco high school students 8.5%,35 however, the finding was by far lower than the studies done in Undergraduates at English Universities, in which 61% of the students had AUD36 and Eldoret, western Kenya 51.9%.37 The discrepancy could be due to the variation in the study tools to assess AUD and alcohol use regulation policy differences among the countries. Nevertheless, the study result was higher than the study done in Nigeria (4.3%).38 Despite the similarity of the study population, the difference in the prevalence of AUDs between the studies may be due to the variation in the screening tools used in Nigeria (DSM-IV-TR) and for this study (AUDIT). AUDIT is a screening instrument and not a diagnostic interview. Moreover, the difference in alcohol drinking cultural perspective may also be the other reason for the discrepancy.
The current research found that being male had a strong association with AUDs, which is in agreement with similar studies done in Nigeria,38 South Africa,16 and general population surveys in 35 countries.39 This could be because of the gender differences in drinking behavior linked with many aspects of biological differences, women’s and men’s differing needs, reasons and motivations about drinking, gender-specific roles in other areas of life and of ways in which societies regulate peoples’ behavior, often giving women the role of warden or moderator of others’ drinking.40–42
In this study, peer pressure to drink alcohol was found to be an independent predictor of an alcohol use disorder, which is similar to the study findings from Gondar University,43 Nigeria University,38 and Haramaya University.31 This might be due to the strongest influence of peer norms on students’ drinking behavior, with the more socially integrated students typically drinking most heavily.44 The other reason could be students tend to drink more alcohol during social gatherings in the virtue of social interaction.45
In the current study, a high level of mental distress doubles the odds of having AUDs among university students, this is also in agreement with the studies done in Australia,2 Amanuel mental specialized hospital,46 and Haramaya University.31 This could be because alcohol use considered a coping mechanism against stress, anxiety, and depression, so it may take as a self-treatment to feel good.47
In the present study, the finding revealed that having a history of diagnosed mental illness was an independent predictor for AUD. This is in agreement with the studies done in Debre Markos University,48 Jimma University,49 and Haramaya University.50 The possible reason for these similarities could be because people with mental illnesses may indulge themselves in alcohol either to deal with their painful emotional disturbances or as a part of the psychopathology.51
This study revealed that students with khat chewing habit had nearly three times increased the odds of having AUDs compared to non-chewers, this is in line with the studies done in Jimma University22 Debre Markos University48,52 and Mekelle University.53 This could be because of that most khat chewers drink alcohol after chewing to terminate the sustained stimulation effect of khat.
Conclusion
AUDs were high among Jimma University Student and positively associated with mental, behavioral, and substance-related factors. Therefore, concerted actions needed to emplace to increase the student’s awareness of the effect of harmful alcohol use. Moreover, it is recommended that further studies needed to be conducted to develop strategies for evidence-based interventions.
Acknowledgments
We would like to extend our gratitude to Jimma University for funding this research project. We also thank the study participants for their willingness to participate in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Davoren MP, Cronin M, Perry IJ, O’Connor K. Alcohol consumption among university students: A typology of consumption to aid the tailoring of effective public health policy. BMJ Open. 2016;6(11):1–9. doi:10.1136/bmjopen-2016-011815
2. Reavley NJ, Jorm AF, Mccann TV, Lubman DI. Alcohol consumption in tertiary education students. BMC Public Health. 2011;11(1):545. doi:10.1186/1471-2458-11-545
3. Kypri K, Cronin M, Wright CS. Do university students drink more hazardously than their non-student peers? Addiction. 2005;100(5):713–714. doi:10.1111/j.1360-0443.2005.01116.x
4. Htet H, Saw YM, Saw TN, et al. Prevalence of alcohol consumption and its risk factors among university students: A cross-sectional study across six universities in Myanmar. PLoS One. 2020;15(2):1–14. doi:10.1371/journal.pone.0229329
5. Mekonen T, Fekadu W, Chane T, Bitew S. Problematic alcohol use among university students. Front Psychiatry. 2017;8:
6. Zadarko-Domaradzka M, Barabasz Z, Sobolewski M, et al. Alcohol consumption and risky drinking patterns among college students from selected countries of the Carpathian Euroregion. Biomed Res Int. 2018;2018.
7. World Health Organization. Global health risks: Mortality and burden of disease attributable to selected major risks. 2009. Available in: https://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf?ua.
8. Fedotov Y Who drug report 2012. New Directions for Youth Development. 2012.
9. Gizaw AT, Amdisa D, Lemu YK. Predictors of substance use among Jimma University instructors, Southwest Ethiopia. Subst Abus Treat Prev Policy. 2020;15(1):1–10.
10. Fufa G, Kinati T, Shiferaw D, Desalegn M. The role of indigenous social institutions on pastoral and the nexus between khat and other drug use among undergraduate students of Jigjiga University in Ethiopia; contributing factors and prevalence rates. Public Heal Res. 2017;7(2):49–54.
11. Kassim S, Jawad M, Croucher R, Akl EA. The epidemiology of tobacco use among khat users: A systematic review. Biomed Res Int. 2015;2015.
12. Wakeman SE, Saitz R. Alcohol, and drug use disorders. Chronic Illn Care Princ Pract. 2018;83–94.
13. Foroud T, Phillips TJ. Assessing the genetic risk for alcohol use disorders. Alcohol Res. 2012;34(3):266–272.
14. Kuo M, Adlaf EM, Lee H, Gliksman L, Demers A, Wechsler H. Erratum: more Canadian students drink but American students drink more: comparing college alcohol use in two countries. Addiction.2002;97:1583–1592. doi:10.1046/j.1360-0443.2002.00240.x
15. Santos A, Neves MCC, Azevedo RCS, et al. Hazardous use of alcohol among undergraduate students at a public university. Rev Psiquiatr Clin. 2014;41(6):150–155. doi:10.1590/0101-60830000000033
16. Young C, De Klerk V. Patterns of alcohol use on a South African university campus: the findings of two annual drinking surveys. Afr J Drug Alcohol Stud. 2009;7:2.
17. Brooks AT, Lòpez MM, Ranucci A, Krumlauf M, Wallen GR. A qualitative exploration of social support during treatment for severe alcohol use disorder and recovery. Addict Behav Reports. 2017;6:76–82. doi:10.1016/j.abrep.2017.08.002
18. Lee SB, Chung S, Seo JS, Jung WM, Park IH. Socioeconomic resources and quality of life in alcohol use disorder patients: the mediating effects of social support and depression. Subst Abuse Treat Prev Policy. 2020;15(1):13. doi:10.1186/s13011-020-00258-6
19. Gebremedhin AT, Gesesew HA, Demissie TD, Kerie MW, Sudhakar M. Khat chewing and risky sexual behavior in Sub-Saharan Africa: a systematic review protocol. JBI Database Syst Rev Implement Rep. 2013;11(12):59–67. doi:10.11124/jbisrir-2013-877
20. Choudhry V, Agardh A, Stafström M, Östergren P. Patterns of alcohol consumption and risky sexual behavior: a cross-sectional study among Ugandan university students. BMC Public Health. 2014;14(128):1–11. doi:10.1186/1471-2458-14-128
21. White A, Hingson R. The burden of alcohol use: excessive alcohol consumption and related consequences among college students. Alcohol Res Curr Rev. 2013;35(2):201–218.
22. Tesfaye Y, Negash A, Gebrehiwot TT, et al. Is there association between risky sexual behaviors and depression symptoms among youth? A case of Jimma university students, Ethiopia. Psychiatry J. 2019;2019:1–12. doi:10.1155/2019/3757656
23. Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. Alcohol Use Disorders Identification Test (AUDIT). 2. World Health Organization; 2001:1–39.
24. Reinert DF, Allen JP. (AUDIT): a review of recent research. Alcohol Clin Exp Res. 2002;26(2):272–279. doi:10.1111/j.1530-0277.2002.tb02534.x
25. Soboka M, Tesfaye M, Feyissa GT, Hanlon C. Alcohol use disorders and associated factors among people living with HIV who are attending services in south west Ethiopia. BMC Res Notes. 2014;7(1):1–9. doi:10.1186/1756-0500-7-828
26. Yohannes T. Preparation and physicochemical analysis of some Ethiopian traditional alcoholic beverages. African J Food Sci. 2013;7(11):399–403. doi:10.5897/AJFS2013.1066
27. Lee M, Regu M, Seleshe S. Uniqueness of Ethiopian traditional alcoholic beverage of plant origin, tella. J Ethn Foods. 2015;2(3):110–114. doi:10.1016/j.jef.2015.08.002
28. Saunders JB, Babor TF. AUDIT questionnaire: screen for. Addiction. 1993;88(791–803):1–2.
29. Kocalevent RD, Berg L, Beutel ME, et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. 2018;6(1):4–11. doi:10.1186/s40359-018-0249-9
30. Judith J. Prochaska, Hai-Yen Sung, Wendy Max Yanling Shi & Michael Ong. Validity study of the K6 scale as a measure of moderate mental distress based on mental health treatment need and utilization. Int J Methods Psychiatr Res. 2012;21(2):88–97. doi:10.1002/mpr.1349
31. Derese A, Seme A, Misganaw C. Assessment of substance use and risky sexual behaviour among Haramaya University Students, Ethiopia. Sci J Public Heal. 2020;2(2):102–110.
32. Cochran WG. Sampling Techniques.
33. Castaño-Perez GA, Calderon-Vallejo GA. Problems associated with alcohol consumption by university students. Rev Lat Am Enfermagem. 2014;22(5):739–746. doi:10.1590/0104-1169.3579.2475
34. Slutske WS. Alcohol use disorders among US college students and their non-college-attending peers. Arch Gen Psychiatry. 2005;62(3):321–327. doi:10.1001/archpsyc.62.3.321
35. Ben El Jilali L, Benazzouz B, El HA, Ouichou A, Mesfioui A. Prevalence of alcohol consumption and alcohol use disorders among middle and high school students in the province of Khemisset, Morocco: a cross-sectional study. Int J Adolesc Youth. 2020;25(1):638–648. doi:10.1080/02673843.2019.1700807
36. Heather N, Partington S, Partington E, et al. Alcohol use disorders and hazardous drinking among undergraduates at English universities. Alcohol Alcohol. 2011;46(3):270–277. doi:10.1093/alcalc/agr024
37. Atwoli L, Mungla PA, Ndung’u MN, Kinoti KC, Ogot EM. Prevalence of substance use among college students in Eldoret, western Kenya. BMC Psychiatry. 2011;11.
38. Adewuya AO, Ola BA, Aloba OO, Mapayi BM, Ibigbami OI, Adewumi TA. Alcohol use disorders among Nigerian University students: prevalence and Sociodemographic correlates. Niger J Psychiatry. 2008;5:1.
39. Gmel G. Gender and alcohol consumption: patterns from the multinational genacis project. Addiction. 2010;104(9):1487–1500.
40. Holmila M, Raitasalo K. Gender differences in drinking: why do they still exist? Addiction. 2005;100(12):1763–1769. doi:10.1111/j.1360-0443.2005.01249.x
41. Ceylan-isik AF, Mcbride SM, Ren J. Sex difference in alcoholism: who is at a greater risk for. Life Sci. 2011;87:133–138. doi:10.1016/j.lfs.2010.06.002
42. Hardy R. Gender differences in the relationship between alcohol consumption and drink problems are largely accounted for by body water. Alcohol Alcohol. 1999;34(6):894–902. doi:10.1093/alcalc/34.6.894
43. Yismaw S. Prevalence and associated factors of alcohol consumption among college students in Gondar Town, Northwest Ethiopia. Sci J Public Heal. 2015;3(4):453. doi:10.11648/j.sjph.20150304.12
44. Perkins HW. Social norms and the prevention of alcohol misuse in collegiate contexts. J Stud Alcohol, Suppl. 2002;1(s14):164–172. doi:10.15288/jsas.2002.s14.164
45. Lorant V, Nicaise P, Soto VE, D’Hoore W. Alcohol drinking among college students: college responsibility for personal troubles. BMC Public Health. 2013;13:1. doi:10.1186/1471-2458-13-615
46. Sintayehu M, Mulat H, Yohannis Z, Adera T, Fekade M. Prevalence of mental distress and associated factors among caregivers of patients with severe mental illness in the outpatient unit of Amanuel Hospital, Addis Ababa, Ethiopia, 2013: cross-sectional study. J Mol Psychiatry. 2015;3(1):1–10. doi:10.1186/s40303-015-0014-4
47. Beccaria A, Berger SE, Lopez T. Alcohol as a coping mechanism for social anxiety. Open Access J Addict Psychol. 2019;3(1):1–10.
48. Esmael A. Psychoactive substances use (khat, alcohol, and tobacco) and associated factors among debre Markos University Students, North-West Ethiopia, 2013. J Def Manag. 2014;04(01):1–7. doi:10.4172/2167-0374.1000118
49. Birhanu Y, Mossie A. Effect of substance use on academic achievement of health officer and medical students of Jimma University, Southwest Ethiopia. Ethiop J Health Sci. 2009;19:3.
50. Tesfaye G, Derese A, Hambisa MT. Substance use and associated factors among University students in Ethiopia: a cross-sectional study. J Addict. 2014;2014.
51. American Psychiatric Association. Diagnostic and Statistical Manual for Mental Disorders (DSM-5). Fifth edition. Arlington, VA, American Psychiatric Association, 2013.
52. Tesfaye G, Derese A, Hambisa MT. Assessment of substance abuse and associated factors among students of Debre Markos Poly Technique College In Debre Markos Town, East Gojjam Zone, Amhara Regional State, Ethiopia,2013. Glob J Med Res Pharma, Drug Discov Toxicol Med. 2013;13:4.
53. Tulu SK, Keskis W. Assessment of causes, prevalence, and consequences of alcohol and drug abuse among Mekelle University, CSSL 2 nd year students. Am J Appl Psychol. 2015;3(3):47–56.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.