Back to Journals » Clinical Ophthalmology » Volume 19
Ahmed Glaucoma Valve in Aniridia
Authors Ahmed AA ![]() , Netland PA
, Netland PA ![]()
Received 2 April 2025
Accepted for publication 27 June 2025
Published 29 July 2025 Volume 2025:19 Pages 2487—2493
DOI https://doi.org/10.2147/OPTH.S531997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ahmed A Ahmed,1– 3 Peter A Netland3,4
1Department of Ophthalmology, Case Western Reserve University School of Medicine, Cleveland, OH, USA; 2Department of Ophthalmology, Assiut University, Assiut, Egypt; 3Department of Ophthalmology, University of Virginia School of Medicine, Charlottesville, VA, USA; 4Department of Ophthalmology, Eastern Virginia Medical School, Norfolk, VA, USA
Correspondence: Peter A Netland, Department of Ophthalmology, Eastern Virginia Medical School, P.O. Box 180, Norfolk, VA, 23501, USA, Tel +1 757-388-2473, Email [email protected]; [email protected]
Purpose: To evaluate long-term clinical outcomes after Ahmed Glaucoma Valve implantation in glaucoma associated with aniridia.
Methods: This was a retrospective, noncomparative, consecutive, interventional case series of 20 eyes in 15 patients with aniridic glaucoma treated with the Ahmed Glaucoma Valve (Model FP7, New World Medical, Rancho Cucamonga, CA). Patient records were reviewed for intraocular pressure (IOP), number of glaucoma medications, surgical success (5 mmHg ≤ IOP ≤ 21 mmHg and ≥ 20% from baseline, without additional glaucoma surgery, and without loss of light perception vision), and complications.
Results: The IOP and number of glaucoma medications were significantly reduced at all time points after surgery. The mean IOP was 31.6 ± 8.4 and 15.6 ± 3.0 mmHg at baseline and 7 years after surgery, respectively (P< 0.0005). At baseline and 7 years after surgery, the average number of medications was 3.0 ± 0.7 and 0.8 ± 0.8, respectively (P< 0.0005). The cumulative probability of success was 95% at 7 years after surgery. Transient postoperative complications included shallow anterior chamber in 1 eye (5%) and choroidal effusion in 2 eyes (10%). Complications in the late postoperative period included tube repositioning in 4 eyes (20%), patch graft for tube exposure in 3 eyes (15%), and cataract in 1 eye (5%). Complications were resolved without vision loss in all patients.
Conclusion: Ahmed Glaucoma Valve implantation is effective for long-term control of IOP in patients with aniridic glaucoma. Complications were not associated with vision loss.
Keywords: aniridia, aniridic glaucoma, glaucoma drainage implant, Ahmed Glaucoma Valve, glaucoma surgery
Introduction
Aniridia is a pan ocular congenital malformation of the eye, which includes complete or partial iris hypoplasia and foveal hypoplasia, resulting in reduced visual acuity.1,2 The majority of cases of aniridia and associated disorders are caused by heterozygous loss-of-function mutations of the PAX6 gene or associated regulatory regions, causing haploinsufficiency of the PAX6 protein,3,4 which can be sporadic or familial. Mutations in PAX6 gene disrupt development, leading to the characteristic ocular and systemic features of aniridia. Aniridia syndrome has been associated with ocular and systemic problems, including aniridia, foveal hypoplasia, nystagmus, glaucoma, cataract, keratopathy, and obesity.5,6
Aniridia has been associated with glaucoma, which often develops during childhood to early adulthood.5,7,8 Approximately half of aniridia patients develop glaucoma, with a median onset at age 8.5 years.5 In patients presenting with aniridia and glaucoma, most have open anterior chamber angles, similar to patients with aniridia without glaucoma.9 A small percentage of eyes with aniridia and glaucoma with closed angles had prior history of ocular surgery,9 which likely contributed to development of angle closure. Aniridia is a pro‐fibrotic syndrome,10 which may account for the small percentage (7%) of patients with aniridic glaucoma and angle-closure.9 Medical therapy is often useful for treatment of aniridic glaucoma, but the majority (58%) of patients require surgical treatment of glaucoma.5 Several small case series have reported success with the Ahmed Glaucoma Valve in surgical treatment of aniridic glaucoma.11–15 In this study we evaluated the long-term clinical outcomes after Ahmed Glaucoma Valve implantation in the surgical management of glaucoma associated with aniridia.
Methods
This was a retrospective, noncomparative, consecutive, interventional case series of 20 eyes in 15 patients with aniridic glaucoma treated with the Ahmed Glaucoma Valve (Model FP7, New World Medical, Rancho Cucamonga, CA). Consecutive patients with congenital aniridia treated by a single surgeon (PAN) with the Ahmed Glaucoma Valve were identified from surgical logs and electronic medical records. All eligible patients were included in the study, and no eligible subjects were excluded from the analysis. The surgical technique was as described previously (www.newworldmedical.com, instructions for use, Ahmed Glaucoma Valve, FP7).
Patient records were reviewed for intraocular pressure (IOP), number of glaucoma medications, surgical success and complications for 7 years after surgery. Success was defined as 5 mmHg ≤ intraocular pressure ≤ 21 mmHg and ≥ 20% lowering of IOP, with or without medications, no loss of light perception vision, and without further glaucoma surgery. The study was approved by the University of Virginia Institutional Review Board and performed according to the tenets of the Declaration of Helsinki. Consent was waived due to the retrospective nature of the review, and the data was anonymized prior to data analysis and maintained with confidentiality. Groups were compared using the non-paired t-test. Kaplan-Meier survival analysis was used for success rates. P values less than 0.05 were considered statistically significant. Data were collected and stored in compliance with Health Insurance Portability and Privacy Act guidelines.
Results
The study included 20 eyes in 15 patients with aniridic glaucoma. The mean ± SD age at the time of surgery was 34 ± 19 years. Of the treated eyes, 17 (85%) were in female and 3 (15%) were in male patients. All eyes treated (100%) were in Caucasian patients. Patients had a history of prior ocular surgery in 11 eyes (55%), with cataract surgery in 8 (40%) eyes, artificial iris surgery in 2 (10%) eyes, corneal surgery in 3 (15%) eyes, and glaucoma surgery in 3 (15%) eyes (3 eyes had more than one prior procedure, thus the number of eyes was less than the sum of the number of procedures). The three eyes with a history of glaucoma procedure had been treated with trabeculectomy with mitomycin C, glaucoma drainage implant, and goniotomy. The majority of the eyes (17/20, 85%) were treated with the Ahmed Glaucoma Valve as primary (initial) surgery for glaucoma.
During surgery, the tube was placed in the sulcus in 7 eyes (35%), and 13 (65%) were placed in the anterior chamber. A 7–0 polyglactin flow-restriction suture was tied around the tube intraoperatively in 5 eyes (25%). One surgeon (PAN) performed the procedures. Tube placement and flow-restriction were used at the discretion of the surgeon, depending on the potential risk for complications for individual patients. In a patient with aniridic keratopathy, a central superficial keratectomy was performed in one eye (5%) during the procedure, to improve the view of the anterior chamber during tube placement.
As shown in Figure 1, the mean intraocular pressure was significantly reduced after Ahmed Glaucoma Valve implantation compared with baseline (P < 0.0005 at all the postoperative time points). At baseline, the mean IOP was 31.6 ± 8.4 and, at 7 years, the mean IOP was 15.6 ± 3.0 mmHg (P<0.0005). At 7 years follow-up, the percent reduction IOP from baseline was 51%. The numbers of patients with follow-up information at baseline, 1, 3, 5, and 7 years were 20, 19, 17, 16, and 11. At 3 and 4 years after surgery, 2 eyes in 1 patient were lost to follow up when the patient died.
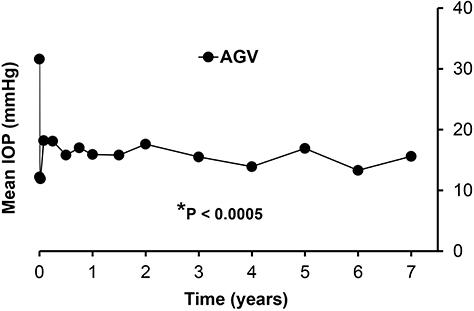 |
Figure 1 Mean intraocular pressure. The intraocular pressure was significantly reduced after Ahmed Glaucoma Valve implantation compared with baseline (*P < 0.0005) at all of the postoperative time points. At 7 years, the mean IOP was 15.6 ± 3.0 mmHg. N values at baseline, 1, 3, 5, and 7 years were 20, 19, 17, 16, and 11. Time 0 was the baseline (preoperative) IOP. Abbreviations: IOP, intraocular pressure; AGV, Ahmed Glaucoma Valve. |
The average number of medications was significantly lower compared with baseline (P < 0.0005) at all time points after implantation of the Ahmed Glaucoma Valve (Figure 2). At baseline and 7 years after surgery, the average ± SD number of medications was 3.0 ± 0.7 and 0.8 ± 0.8, respectively (P<0.0005). At 7 years follow-up, the percent reduction of number of medications from baseline was 73%. At baseline, all patients (100%) required glaucoma medications. At the last follow-up visit, 8 (40%) patients were on no glaucoma medications, and 19 (95%) had reduced the number of glaucoma medications. Success was defined as 5 mmHg ≤ intraocular pressure ≤ 21 mmHg and ≥ 20% lowering of IOP, with or without medications, no loss of light perception vision, and without further glaucoma surgery. At 7 years after surgery, the success rate was 95% (Figure 3). The failure was due to increased intraocular pressure despite medical therapy, which was improved after treatment with cyclophotocoagulation.
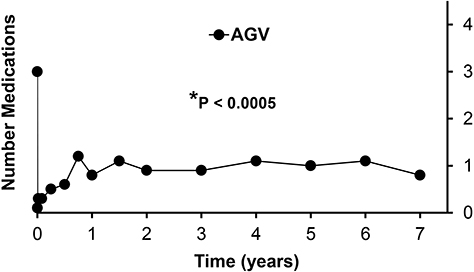 |
Figure 2 Mean number glaucoma medications. The average number of medications was significantly lower compared with baseline (*P < 0.0005) at all time points after implantation of the Ahmed Glaucoma Valve (AGV). At 7 years after surgery, the average number of medications was 0.8 ± 0.8. Time 0 was the baseline (preoperative) number of glaucoma medications. |
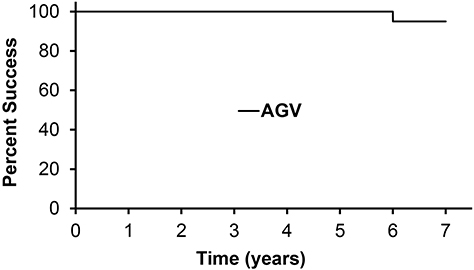 |
Figure 3 Cumulative probability of success. Success was defined as 5 mmHg ≤ intraocular pressure ≤ 21 mmHg and ≥ 20% lowering of IOP, with or without medications, no loss of light perception vision, and without further glaucoma surgery. At 7 years, the success rate was 95% after Ahmed Glaucoma (AGV) implantation. |
Postoperative complications are shown in Table 1. Transient early postoperative complications (≤ 3 months) included shallow anterior chamber in 1 eye (5%) and choroidal effusion in 2 eyes (10%). The patient with a shallow anterior chamber was treated with a single injection of an ophthalmic viscosurgical device (Healon, sodium hyaluronate 1% solution) to transiently deepen the anterior chamber. These early postoperative complications resolved without surgical treatment. Complications in the late postoperative period (> 3 months) included tube malposition treated with repositioning in 4 eyes (20%). One of these eyes had pre-existing aniridic keratopathy, which was treated with keratoprosthesis after the intraocular pressure was reduced, requiring repositioning of the tube posterior to the backplate of the keratoprosthesis. None of the other eyes treated with tube repositioning required additional corneal surgery during the postoperative follow up period. Two additional eyes had progression of aniridic keratopathy, likely unrelated to glaucoma drainage implant surgery. Three eyes (15%) required patch graft for tube exposure. One eye (5%) developed cataract during the postoperative follow up period, which was treated with cataract surgery. No complications were associated with vision loss.
 |
Table 1 Complications After Ahmed Glaucoma Valve Implantation in Aniridic Glaucoma (N=20 Eyes) |
Discussion
Glaucoma in aniridia is often poorly controlled with medical therapy and may lead to irreversible vision loss.5 In aniridia patients, therapeutic goniotomy, trabeculotomy, and cyclodestructive procedures have been associated with high intermediate- and long-term failure.14,16–18 Trabeculectomy for aniridic glaucoma has been associated with poor surgical success rates (ranging from 0% to 42%)11,14,18–23 and vision-threatening complications,24 although some success has been reported.25,26 Aniridia is a pro‐fibrotic syndrome,10 which may account for the low success rates reported for these options for primary surgery in aniridia patients. In our study, we assessed the clinical outcomes after implantation of the Ahmed Glaucoma Valve in 20 eyes with aniridia and glaucoma after long-term (7 years) follow up. The majority of eyes (85%) were treated with the Ahmed Glaucoma Valve as initial (primary) surgery for glaucoma. In patients with aniridic glaucoma, we found that Ahmed Glaucoma Valve implantation was effective for long-term control of intraocular pressure, and that early-and late-postoperative complications were not associated with vision loss.
Different glaucoma drainage implants have been used for treatment of aniridic glaucoma (Table 2). In aniridia patients, success rates reported for the non-valved Molteno implant have ranged from 67% to 100%.18,21,27,28 The number of eyes in these studies was small, ranging from 2 to 6. While the results of these early studies are difficult to compare to our results, our success rates are within the range reported for the Molteno implant.
 |
Table 2 Glaucoma Drainage Implant Results in Aniridic Glaucoma |
Arroyave et al described their results with the non-valved Baerveldt Glaucoma Implant.29 In this study, the success rate was 88% at 1 year for 8 eyes treated with the Baerveldt Glaucoma Implant. The Aurolab Aqueous Drainage Implant (AADI) is a non-valved implant similar to the Baerveldt implant. Durai et al found an 89% success rate at two years after treatment with the AADI in 18 aniridic eyes.23 In this study, the cumulative probability of failure was significantly higher in a comparison group of 12 aniridic eyes treated with trabeculectomy with mitomycin C. Cataract surgery was performed in 5 eyes in the trabeculectomy group and no eyes in the AADI group (P=0.01). Jacobson et al reported 87% success for 23 aniridic eyes treated with the Baerveldt Glaucoma Implant compared with 88% success for 8 aniridic eyes treated with the AGV.14 Complications were not described in this study, which included valved and non-valved glaucoma drainage implants.
In this study, we treated patients with the Ahmed Glaucoma Valve. Lee et al reported success in all 6 aniridic eyes treated with the Ahmed glaucoma Valve.11 Almousa and Lake reported 88% success in 8 aniridic eyes after implantation of the Ahmed Glaucoma Valve, with more than 3 years follow-up.12 In the study by Almousa and Lake, one patient experienced vision loss due to retinal detachment after drainage implant surgery. Demirok et al reported success in 67% of aniridic eyes at 1 year after implantation of the Ahmed Glaucoma Valve.13 There was a low frequency on non-vision-threatening complications, as described in our study. Jacobson and co-investigators found 88% success in 8 aniridic eyes treated with the Ahmed Glaucoma Valve after average 17.5 ± 20.1 years follow-up.14 Bolek et al reported 86% success at 3 years after implantation of Ahmed Glaucoma Valve and no vision-threatening complications in 6 aniridia patients (7 eyes).15 Our success rates were within the range of success reported in the previous studies of the Ahmed Glaucoma Valve in aniridia (Table 2, N = 6 studies, average success ± standard deviation = 87 ± 11%, median success = 88%). In our study, we found a similar high success rate up to 7 years after surgery.
In our study, complications occurred at low frequency and were not vision-threatening. One eye (5%) developed a shallow anterior chamber, and choroidal effusion was found in 2 eyes (10%) during the early postoperative period. These early postoperative complications resolved without surgical treatment. Complications in the late postoperative period (> 3 months) included tube repositioning in 4 eyes (20%) and cataract in 1 eye (5%). Three eyes (15%) required patch graft for tube exposure. Younger age and inflammation are significant risk factors for tube exposure after glaucoma drainage implant surgery.30 In our patients with tube exposure, two were young age (1.6 and 15 years old) and one was a 44-year-old with chronic inflammation associated with advanced aniridic keratopathy, which may have increased their risk for this complication. Although sample size limited our analysis of complications, we were able to describe late postoperative complications in our study because of the long-term follow up.
Complications were not associated with vision loss in this study. Visual acuity in aniridia is variable, ranging from logMAR 0.5 to 1.0 (Snellen equivalent 20/60 to 20/200 or worse.31 Visual acuity in aniridia is limited by foveal hypoplasia and nystagmus, as well as other progressive problems, including aniridic keratopathy, cataract, and glaucoma. In our aniridia patients, the average visual acuity was logMAR 0.95 ± 0.53, with both eyes and 0.78 ± 0.15 in the better seeing eye (20/125 Snellen equivalent).31 In this study, the visual acuity at last follow-up was not decreased from the pre-operative level, although we did not do a detailed analysis of the influence of the Ahmed Glaucoma Valve procedure on visual acuity. Limitations of this study include the limitations of retrospective analysis, including potential biases. Another limitation is the small sample size, especially in the analysis of complications. Small sample size often is a limitation of studies of rare diseases such as aniridia. Future studies may be able to analyze larger data sets or multicenter studies to address sample size problems in this population.
Conclusion
Ahmed Glaucoma Valve implantation is effective for long-term control of IOP in Caucasian eyes with aniridic glaucoma. Complications were not associated with vision loss, suggesting that the procedure is relatively safe in eyes with aniridic glaucoma. In our study, the Ahmed Glaucoma Valve was implanted as an initial (primary) glaucoma surgical treatment in the majority of patients.
Acknowledgment
This paper was presented in part at the 2024 American Ophthalmological Society (AOS) Annual Meeting in La Jolla, California on May 18, 2024.
Funding
The authors have no financial interest in this study, and there was no financial support for this study.
Disclosure
The authors declare no competing interests in this study.
References
1. Landsend ECS, Lagali N, Utheim TP. Congenital aniridia – a comprehensive review of clinical features and therapeutic approaches. Surv Ophthalmol. 2021;66:1031–1050. doi:10.1016/j.survophthal.2021.02.011
2. Netland PA. Management of glaucoma in congenital aniridia. In: Parekh M, Poli B, Ferrari S, Teofili C, Ponzin D, editors. Aniridia: Recent Developments in Scientific and Clinical Research. London: Springer; 2015:27–37.
3. Bobilev AM, McDougal ME, Taylor WL, Geisert EE, Netland PA, Lauderdale JD. Assessment of PAX6 alleles in 66 families with aniridia. Clin Genet. 2016;1–9. doi:10.1111/cge.12708
4. Hingorani M, Hanson I, Van Heyningen V. Aniridia. Eur J Hum Genet. 2012;20:1011–1017. doi:10.1038/ejhg.2012.100
5. Netland PA, Scott ML, Boyle JW, Lauderdale JD. Ocular and systemic findings in a survey of aniridia subjects. JAAPOS. 2011;15:562–566.
6. Shiple D, Finklea B, Lauderdale JD, Netland PA. Keratopathy, cataract, and dry eye in a survey of aniridia subjects. Clin Ophthalmol. 2015;9:291–295. doi:10.2147/OPTH.S74648
7. Balekudaru S, Sankaranarayanan N, Agarkar S. Prevalence, incidence, and risk factors for the development of glaucoma in patients with aniridia. J Pediatr Ophthalmol Strabismus. 2017;54:250–255. doi:10.3928/01913913-20170322-01
8. Gramer E, Reiter C, Gramer G. Glaucoma and frequency of ocular and general diseases in 30 patients with aniridia: a clinical study. Eur J Ophthalmol. 2012;22:104–110. doi:10.5301/EJO.2011.8318
9. Bajwa A, Burstein E, Grainger RM, Netland PA. Anterior chamber angle in aniridia with and without glaucoma. Clin Ophthalmol. 2019;13:1469–1473. doi:10.2147/OPTH.S217930
10. Tsai JH, Freeman JM, Chan CC, et al. A progressive anterior fibrosis syndrome in patients with postsurgical congenital aniridia. Am J Ophthalmol. 2005;140:1075–1079. doi:10.1016/j.ajo.2005.07.035
11. Lee H, Meyers K, Lanigan B, O’Keefe M. Complications and visual prognosis in children with aniridia. J Pediatr Ophthalmol Strabismus. 2010;47:205–210. doi:10.3928/01913913-20090818-07
12. Almousa R, Lake DB. Intraocular pressure control with Ahmed glaucoma drainage device in patients with cicatricial ocular surface disease-associated or aniridia-related glaucoma. Int Ophthalmol. 2014;34:753–760. doi:10.1007/s10792-013-9868-6
13. Demirok GS, Ekşioğlu Ü, Yakın M, Kaderli A, Kaderli ST, Örnek F. Short- and long-term results of glaucoma valve implantation for aniridia-related glaucoma: a case series and literature review. Turk J Ophthalmol. 2019;49:183–187. doi:10.4274/tjo.galenos.2019.07348
14. Jacobson A, Mian SI, Bohnsack BL. Clinical outcomes and visual prognostic factors in congenital aniridia. BMC Ophthalmol. 2022;22:235. doi:10.1186/s12886-022-02460-5
15. Bolek B, Wylegala E, Tarnawska D. Long-term clinical outcomes of Ahmed Valve implantation in aniridic glaucoma. Biomedicines. 2023;11:2996. doi:10.3390/biomedicines11112996
16. Walton DS. Aniridic glaucoma: the results of gonio-surgery to prevent and treat this problem. Trans Am Ophthalmol Soc. 1986;84:59–70.
17. Magan T, Tanner A, Fajardo-Sanchez J, et al. Long-term outcomes in primary congenital glaucoma, aniridia and anterior segment dysgenesis. Eur J Ophthalmol. 2022;32:2920–2927. doi:10.1177/11206721211073208
18. Wiggins RE, Tomey KF. The results of glaucoma surgery in aniridia. Arch Ophthalmol. 1992;110:503–505. doi:10.1001/archopht.1992.01080160081036
19. Grant WM, Walton DS. Progressive changes in the angle in congenital aniridia, with development of glaucoma. Trans Am Ophthalmol Soc. 1974;72:207–228.
20. Nelson LB, Spaeth GL, Nowinski TS, Margo CE, Jackson L. Aniridia. A review. Surv Ophthalmol. 1984;28:621–642. doi:10.1016/0039-6257(84)90184-X
21. Adachi M, Dickens CJ, Hetherington J, et al. Clinical experience of trabeculotomy for the surgical treatment of aniridic glaucoma. Ophthalmology. 1997;104:2121–2125. doi:10.1016/S0161-6420(97)30041-4
22. Okada K, Mishima HK, Masumoto M, Tsumamoto Y, Tsukamoto H, Takamatsu M. Results of filtering surgery in young patients with aniridia. Hiroshima J Med Sci. 2000;49(3):135–138.
23. Durai I, Pallamparthy S, Puthuran GV, et al. Outcomes of glaucoma drainage Device implantation and trabeculectomy with mitomycin C in glaucoma secondary to aniridia. Am J Ophthalmol. 2021;227:173–181. doi:10.1016/j.ajo.2021.03.008
24. Shakrawal J, Temkar S, Sihota R, Venkatesh P. Suprachoroidal hemorrhage after removal of releasable suture with globe massage post-trabeculectomy. Indian J Ophthalmol. 2019;67:287–289. doi:10.4103/ijo.IJO_452_18
25. Senthil S, Nkechinyere JU, Mohamed A, et al. Outcomes of primary combined trabeculotomy and trabeculectomy in early-onset glaucoma in children with congenital aniridia. Ophthalmol Glaucoma. 2021;4:305–311. doi:10.1016/j.ogla.2020.09.012
26. Sihota R, Selvan H, Azmira K, et al. Improving long-term intraocular pressure and visual outcomes in eyes with aniridic glaucoma. Graefes Arch Clin Exp Ophthalmol. 2021;259:3749–3755. doi:10.1007/s00417-021-05335-5
27. Molteno AC, Ancker E, Van Biljon G. Surgical technique for advanced juvenile glaucoma. Arch Ophthalmol. 1984;102:51–57. doi:10.1001/archopht.1984.01040030035030
28. Billson F, Thomas R, Aylward W. The use of two-stage Molteno implants in developmental glaucoma. J Pediatr Ophthalmol Strabismus. 1989;26:3–8. doi:10.3928/0191-3913-19890101-03
29. Arroyave CP, Scott IU, Gedde SJ, Parrish RK, Feuer WJ. Use of glaucoma drainage devices in the management of glaucoma associated with aniridia. Am J Ophthalmol. 2003;135:155–159. doi:10.1016/S0002-9394(02)01934-7
30. Chaku M, Netland PA, Ishida K, Rhee DJ. Risk factors for tube exposure as a late complication of glaucoma drainage implant surgery. Clin Ophthalmol. 2016;10:547–553. doi:10.2147/OPTH.S104029
31. Krause MA, Trout KL, Lauderdale JD, Netland PA. Visual acuity in aniridia and WAGR syndrome. Clin Ophthalmol. 2023;17:1255–1261. doi:10.2147/OPTH.S405003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Comparison of the Efficacy and Safety of Modified Baerveldt Drainage Implants versus Ahmed Glaucoma Valves After 1 Year of Follow-Up
Davis KL, Christensen QH, VandeLune JA, Pellack DR, Donegan PJ, Meyer MD, Singh RS, Al-Kaylani HM, Boese EA, Pouw AE
Clinical Ophthalmology 2026, 20:588163
Published Date: 8 July 2026