Back to Journals » Clinical Optometry » Volume 13
Agreement Between Retinoscopy, Autorefractometry and Subjective Refraction for Determining Refractive Errors in Congolese Children
Authors Mukash SN ![]() , Kayembe DL, Mwanza JC
, Kayembe DL, Mwanza JC
Received 25 January 2021
Accepted for publication 25 March 2021
Published 21 April 2021 Volume 2021:13 Pages 129—136
DOI https://doi.org/10.2147/OPTO.S303286
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Mr Simon Berry
Sabrina N Mukash,1 David L Kayembe,1 Jean-Claude Mwanza1,2
1Department of Ophthalmology, School of Medicine, Kinshasa University Hospital, Kinshasa, Democratic Republic of Congo; 2Department of Ophthalmology, School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA
Correspondence: Sabrina N Mukash
Department of Ophthalmology, School of Medicine, Kinshasa University Hospital, Kinshasa, Democratic Republic of Congo
Tel +243 816917089
Email [email protected]
Objective: To assess the agreement between retinoscopy and autorefractometry and between subjective refraction and both retinoscopy and autorefractometry in Congolese children.
Patients and Methods: Fifty-four children (6– 17 years old) were enrolled consecutively in this cross-sectional study. Refraction was evaluated before and after cycloplegia (1% cyclopentolate) with retinoscopy and autorefractometry. Readings were compared (paired t-test) and agreement assessed with Bland–Altman plots. Subjective refraction was compared with the two methods to determine which one provides better reference estimates for subjective refraction.
Results: Under cycloplegia, the spherical power was comparable between retinoscopy and autorefractometry (1.12 ± 1.37 D vs 1.22 ± 1.06D, P = 0.70), cylinder power was significantly more myopic on retinoscopy than autorefractometry (0.80 ± 1.10D vs − 0.62 ± 0.66, P = 0.019), and SE was greater on autorefractometry than retinoscopy (0.91 ± 1.10D vs 0.72 ± 1.00D, P = 0.014). Retinoscopy and autorefractometry overestimated the power of spherical (P = 0.022 and 0.002, respectively) and cylindrical components (all P < 0.001). There was an agreement between retinoscopy and autorefractometry in measuring spherical (bias: 0.09 ± 0.16D; limit of agreement, LoA: − 0.40 to 0.22D) and cylindrical power (bias: − 0.18 ± 0.20D; LoA: − 0.57 to 0.21D). Subjective refraction agreed with cycloplegic retinoscopy for determining SE power (bias: 0.11D; LoA: − 0.51 to 0.73D).
Conclusion: Retinoscopy and autorefractometry can be used interchangeably in children for determining the power of spherical and cylindrical components. Cycloplegic retinoscopy is better than autorefractometry to obtain SE reference values for subjective refraction in children.
Keywords: retinoscopy, autorefractometry, subjective refraction, agreement
Introduction
Uncorrected refractive errors are an important cause of avoidable visual impairment. A recent systemic review and meta-analysis based on global data estimated that in 2015 uncorrected refractive errors were the second leading cause of global blindness behind cataract. The same analysis also estimated that there are currently approximately 237.1 million people with moderate to severe visual impairment worldwide, of whom a little more than half have uncorrected refractive errors.1 Accurate measurement of refractive errors is required for satisfactory correction and vision improvement. Several methods for measuring refractive errors have been introduced in clinic over the years, including subjective refraction, retinoscopy, autorefractometry and photorefraction.
Both retinoscopy and autorefractometry are reliable methods for assessing refractive errors. However, retinoscopy requires a good training and patience as it is time-consuming and suffers from some degree of interobserver variability.2 Autorefraction appears currently to be used more frequently than retinoscopy because it is less time-consuming, easy to use, and well tolerated by patients. Studies comparing retinoscopy and autorefraction have produced conflicting findings, particularly in children.3–9 Upon review, it transpires that the discrepancies likely result from a combination of factors, including the difference in autorefractors used, the experience level of the examiner performing retinoscopy, the type and regimen of the cycloplegic used, and the age of the study population.10
Although autorefractometry has been used in high-income settings for more than three decades, it is only 4 years ago that the technique has been introduced in our department. This has led to an increasing trend among ophthalmology residents to favor autorefractometry over retinoscopy. While most available data on the comparison between refractive errors measured by autorefractometry, retinoscopy, and subjective refraction have come from South and East Asia, there is a contrasting dearth of such data in sub-Saharan Africa (SSA). Thus, establishing whether the two methods provide interchangeable measurements in our setting is clinically relevant. The present study was designed to determine the agreement between retinoscopy, autorefractometry and subjective refraction in Congolese children.
Patients and Methods
Patients
Participants were 54 children attending the Department of Ophthalmology at the University Hospital of Kinshasa. All of them were attending the clinic with visual symptoms commonly associated with refractive errors, such as asthenopia, blurred vision, headache, history of heterophoria. They were recruited and then consecutively enrolled in the study from November 2018 to March 2019. They had to be aged 6 to 17 years and were required to have clear ocular media. They were excluded from participation if they had ocular pathology, including media opacity, ocular misalignment, nystagmus, amblyopia, aphakia, pseudophakia, subluxated lens, congenital or acquired optic nerve and/or retinal disease, mental instability or if they were unable to follow instructions during the examination. Informed consent was obtained from the parents following study approval by the Institutional Review Board of the Kinshasa School of Public Health, a branch of the Kinshasa University School of Medicine. The study execution complied with the tenets of the Declaration of Helsinki.
Retinoscopy and Autorefractometry
All participants underwent a standard ophthalmologic assessment. This notably included Snellen visual acuity determination, non-cycloplegic retinoscopy using a Heine Beta 200 streak retinoscope (Heine Optotechnik GmbH, Herrsching, Germany) and a retinoscopy rack lens set, non-cycloplegic autorefractometry using a table-top TOPCON KR-9200 autorefractor (Topcon, Tokyo, Japan), slit-lamp biomicroscopy and fundus examination. At the end of this assessment, children also underwent cycloplegic retinoscopy and autorefraction. Retinoscopy and autorefractometry were performed in all study participants by the same examiner (S.N.M), who was an experienced third year ophthalmology resident. Cycloplegia was achieved with three drops of 1% cyclopentolate administered 5 minutes apart, after which retinoscopy and autorefractometry were performed 30 minutes after the last drop. Retinoscopy and autorefractometry data were ultimately used as starting points for subjective refraction, which was progressively refined until the best corrected visual acuity (BCVA) was achieved at patient’s satisfaction. Subjective refraction was performed at least 72 hours after cycloplegia.
Statistical Analysis
Spherical error, cylindrical error, and spherical equivalent (SE) were used to compare retinoscopy, autorefractometry and subjective refraction. J0 and J45 vectors for cylindrical axis were not used in this analysis because axis could not be determined with retinoscopy using rack lens set. SE refraction (SE in diopters, D) was calculated using the formula  . Refraction values were expresses as mean ± standard deviation (SD). The comparison between proportions was made with Pearson chi-square test. Retinoscopy, autorefractometry and subjective refraction data were compared using paired-sample Student’s t-test. Agreement between retinoscopy and autorefraction was assessed by calculating the bias, defined as the mean difference of refractive values of the two methods, and both the upper and lower limits of agreement (LoA) by determining its 95% confidence interval (CI) as follows: mean difference ± 1.96 (SD of the mean difference).11 The difference between measurements of the two methods was obtained by subtracting autorefraction-generated values from retinoscopic measurements. Agreement analyses were also performed in a similar way between subjective refraction and retinoscopy and autorefractometry. The statistical significance level was set at <0.05. All analyses were performed using SPSS version 26.0 (SPSS Inc., Chicago, IL, USA).
. Refraction values were expresses as mean ± standard deviation (SD). The comparison between proportions was made with Pearson chi-square test. Retinoscopy, autorefractometry and subjective refraction data were compared using paired-sample Student’s t-test. Agreement between retinoscopy and autorefraction was assessed by calculating the bias, defined as the mean difference of refractive values of the two methods, and both the upper and lower limits of agreement (LoA) by determining its 95% confidence interval (CI) as follows: mean difference ± 1.96 (SD of the mean difference).11 The difference between measurements of the two methods was obtained by subtracting autorefraction-generated values from retinoscopic measurements. Agreement analyses were also performed in a similar way between subjective refraction and retinoscopy and autorefractometry. The statistical significance level was set at <0.05. All analyses were performed using SPSS version 26.0 (SPSS Inc., Chicago, IL, USA).
Results
Children (17 boys and 37 girls,  ) mean age was 11.7 ± 3.0 years (range: 6.0–15.3 years). Because refraction of fellow eyes correlated strongly (r = 0.84 for retinoscopy and r = 0.93 for autorefraction), only data for right eyes was randomly chosen through a single coin toss for further statistical analyses.
) mean age was 11.7 ± 3.0 years (range: 6.0–15.3 years). Because refraction of fellow eyes correlated strongly (r = 0.84 for retinoscopy and r = 0.93 for autorefraction), only data for right eyes was randomly chosen through a single coin toss for further statistical analyses.
Table 1 shows spherical, cylindrical and SE values obtained with the two methods. Spherical power was significantly more hyperopic after than before cycloplegia on both retinoscopy and autorefractometry (all P < 0.05). Cylindrical power estimated by retinoscopy was significantly more myopic before than after cycloplegia (P <0.001); a similar observation was made for autorefractometry (P = 0.021). The power of the spherical and cylindrical components measured with retinoscopy and autorefractometry under cycloplegic conditions were significantly greater than corresponding values obtained with subjective refraction (all P < 0.05). Non-cycloplegic retinoscopy and autorefraction yielded comparable SE values (P = 0.58) although the latter tended to produce higher values. Cycloplegic refraction yielded greater SE values with autorefraction than retinoscopy (P = 0.014). Relative to refraction before cycloplegia, both cycloplegic retinoscopy and autorefraction shifted the refraction from myopic to hyperopic (all P < 0.05). The difference in SE was significant in both cases (all P < 0.001). The shift was greater with autorefraction (1.26D) than retinoscopy (0.96D). The mean SE of subjective refraction was comparable with the one obtained after cycloplegic retinoscopy (P = 0.051), but was significantly lower than cycloplegic autorefraction-based measurement (P < 0.001).
 |
Table 1 Comparison of Retinoscopy, Autorefractometry and Subjective Refraction Before and After Cycloplegia |
Data in Table 2 show the frequency of misclassification of refractive errors as well as underestimation and overestimation of the severity of hyperopia and myopia by non-cycloplegic retinoscopy and autorefractometry based on SE values. Compared to cycloplegic refraction, non-cycloplegic retinoscopy and autorefractometry misclassified as myopic or emmetrope 54.8% and 46.7% ( and underestimated 40.4% and 40.9% (
and underestimated 40.4% and 40.9% ( of hyperopic children, respectively. In myopic children, non-cycloplegic retinoscopy and autorefractometry overestimated the severity of myopia in 60.0% and 66.6% (
of hyperopic children, respectively. In myopic children, non-cycloplegic retinoscopy and autorefractometry overestimated the severity of myopia in 60.0% and 66.6% ( and underestimated it in 30.0% and 11.1% (
and underestimated it in 30.0% and 11.1% ( .
.
 |
Table 2 Frequency of Misclassification, Underestimation and Overestimation of Refractive Errors After Cycloplegic Retinoscopy and Autorefractometry |
Data from agreement analysis between retinoscopy, autorefractometry, and subjective refraction is given in Table 3 and related Bland–Altman plots shown in Figure 1. Cycloplegic retinoscopy and autorefractometry agreed on spherical and cylindrical power values, with non-significant biases of −0.09 ± 0.16D and −0.18 ± 0.20D, respectively. SE values derived from subjective refraction agreed with those from retinoscopy (bias: 0.11D), but not autorefractometry. No agreement was found between subjective refraction and either retinoscopy or autorefractometry regarding spherical (bias: 0.51 ± 0.32D and 0.60 ± 0.24D, respectively) and cylindrical power (bias: −0.57 ± 0.36D and −0.39 ± 0.21D, respectively).
 |
Table 3 Agreement Data Between Cycloplegic Retinoscopy, Autorefractometry and Subjective Refraction |
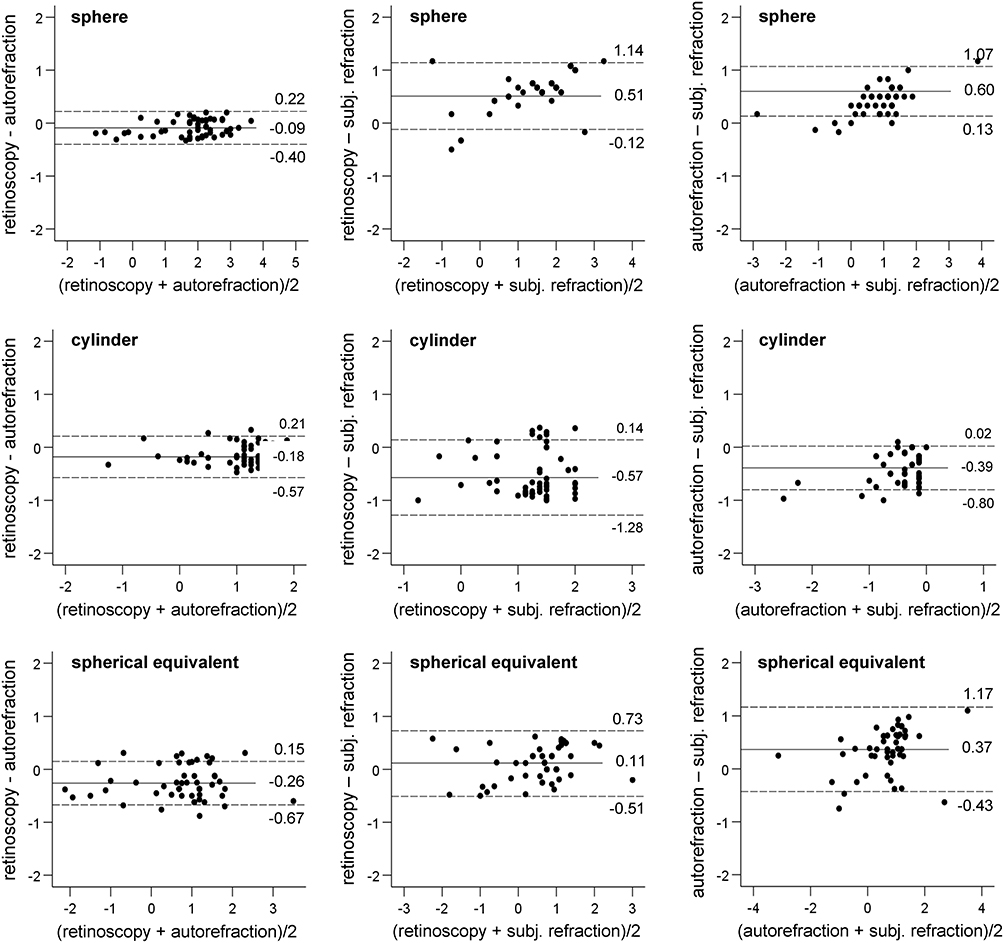 |
Figure 1 Bland–Altman plots of the agreement between retinoscopy and autorefractometry refraction, between subjective refraction and retinoscopy and between subjective refraction and autorefraction for measuring the power of spherical, cylindrical and SE in children. |
Discussion
Our findings indicated that relative to cycloplegic retinoscopy and autorefractometry, both methods significantly underestimated positive spherical power, under non-cycloplegic conditions. Non-cycloplegic retinoscopy also overestimated the power of negative cylindrical component. Underestimation of positive spherical and both over- and underestimation of spherical negative power by autorefractometry under non-cycloplegic conditions has been reported previously.12–15 These studies also showed that non-cycloplegic autorefractometry tended to either underestimate13,14 or overestimate negative cylindrical power.12 On the contrary, SE values determined with non-cycloplegic retinoscopy and autorefractometry produced more myopic measurements than the same method under cycloplegic conditions. Although the differences in measurements obtained under non-cycloplegic and cycloplegic conditions were statistically significant with both methods, it was greater with refractometry than retinoscopy. There was a shift in refraction under cycloplegic conditions, indicating that without cycloplegia both retinoscopy and autorefractometry underestimated the severity of hyperopia and misclassified hyperopic eyes in comparable proportions of eyes. The two refraction methods also overestimated the severity of myopia in similar proportions. Such a shift has been described previously with autorefractometry and retinoscopy, both in clinical-12–14,16–22 and population-based studies.14,23–29 Specifically, non-cycloplegic refraction has been reported to overestimate the severity of myopia and underestimate that of hyperopia. In population-based studies, performing refraction in children without cycloplegia erroneously increased the prevalence of myopia while decreasing that of hyperopia. The data above show consistency across studies regarding the difference between non-cycloplegic and cycloplegic refraction. They suggest that in children refraction should be assessed under cycloplegic conditions, to avoid misclassification of refractive errors. A plausible explanation for this shift is that in non-cycloplegic conditions, accommodation effort in hyperopes helps suppress the blurriness in order to achieve clear vision. On the contrary, such an effort is not present or is negligible in myopes due to weaker accommodation requirements. This could be the reason why the positive shift in refraction is greater in hyperopic than myopic children. More importantly, imaging studies have provided evidence that this shift results from an increased anterior chamber depth and anterior lens radius of curvature as well as a reduced lens thickness following treatment with muscarinic antagonists.30–32
Our observation that under cycloplegia autorefractometry and retinoscopy produced comparable values of the spherical component aligns with findings of two previous studies.33,34 Contrary to significant differences between subjective refraction with both retinoscopy and autorefractometry in spherical and cylindrical values, as also reported by Pokupec et al,7 similar comparisons showed no significant differences in Ozdemir et al’s study.34 SE values from subjective refraction being significantly lower than those from autorefractometry in the present study corroborates Demirci et al15 findings, but differs from the lack of significant difference reported previously by both Ganger et al33 as well as Ozdemir et al.34 While the discrepancies across studies are likely multifactorial, one of the key contributing factors may be the profile of refractive errors in study populations and the fundamental difference between manual retinoscopy and automated refraction.
Retinoscopy and autorefractometry showed agreement only for measuring the power of the spherical, but not the cylindrical and SE components. While the bias of −0.18D for measuring the cylindrical component was mathmatically significant, it is clearly clinically insignificant. Thus, retinoscopy and autorefractometry may be used conversely for determining the power of the cylindrical component. On the other hand, though the −0.26 D bias between the two methods in determining the SE component was mathematically small, it is important to remember that even a ±0.25D difference can be clinically significant for some patients, in whom such a change will be easily perceived as improvement or deterioration of visual sensitivity. Alternatively, some patients with reduced visual sensitivity will not perceive a change in visual sensitivity even with a ±0.5D difference. In the Shahroud Children Cohort Study,5 cycloplegic autorefractometry produced significantly greater spherical, cylindrical and SE values than retinoscopy. However, the biases were deemed clinically meaningless, suggesting that the two methods could be interchanged to measure the power of the three refractive components. Other studies in children have reported similar spherical, cylindrical, and SE power between retinoscopy and refractometry under cycloplegia.4,8,15,16,35,36
The ultimate goal of objective refraction, regardless of the method used, is to determine the starting point for subjective refraction. Relative to retinoscopy- and autorefractometry-based refraction in the present study, subjective refraction agreed with retinoscopy-based refraction only for measuring the SE component of the refraction. From the management standpoint, our findings suggest that in children whose acceptance during subjective refraction shows preference of SE, data obtained from cycloplegic retinoscopy should be given preference and be used for subjective refraction. Past studies have produced varying findings. Among studies that investigated the agreement of subjective refraction with cycloplegic retinoscopy and/or autorefractometry, Adyanthaya and Abhilash37 noted that autorefractometry significantly overestimated spherical power in myopic eyes, but underestimated it in hyperopic eyes. However, retinoscopy was better for determining the spherical power, whereas autorefractometry was suitable for quantifying the cylindrical power of subjective refraction. Among other studies, two reported that the two methods were in agreement when quantifying the spherical power,16,33 one found that patients were more likely to accept correction based on retinoscopic than autorefractometric testing although no significant difference was discovered between the three methods with regard to spherical and cylindrical power,38 and another one revealed that subjective refraction significantly differed from the other two methods of refraction.17 In studies that used only cycloplegic autorefractometry and subjective refraction, the comparison of the two methods yielded similar refractive values for sphere and SE,14 suggested that preference be given to cycloplegic autorefraction because it was more accurate,39 or determined that autorefractometry significantly overcorrected refractive errors and therefore was less accurate than subjective refraction in children.40 Since the children in our study were predominantly hyperopic, it is possible that the residual accommodation was likely stronger during autorefractometry than retinoscopy. The distance from the eye to the fixation target inside the autorefractometer is shorter during refractometry than the distance at which retinoscopy is usually performed. Consequently, the residual accommodation effort would be stronger with autorefractometry than retinoscopy. Moreover, the reading distance during subjective refraction is likely to mimic the retinoscopy than autorefractometry scenario, which could account for the similarity observed between subjective refraction and retinoscopy. Because most of past studies were performed in South and East Asians in whom the prevalence of myopia is higher than in blacks,41–43 the lack of or negligible accommodation in these populations may explain, at least partly, some of the differences between their findings and ours.
The subjects in the present study were all recruited from an eye department rather than a random sample of the general population. This selection bias could limit the generalizability of the findings. Another limitation of this study is its relatively small sample size. Notwithstanding, our sample size can be considered adequate since several studies8,16,17,38 comparing refraction techniques used similar or smaller sample sizes compared to ours. Furthermore, our findings were mostly compared to those obtained in South East Asian children despite obvious differences in ocular biometric profiles, because of the scarcity of similar information within SSA. Thus, the difference in ocular biometric features may account for the difference in findings.
In conclusion, retinoscopy and autorefractometry were in agreement for determining the power of the spherical component. Although the difference between the two methods in determining the power of the cylindrical component was statistically significant, it was clinically negligible, suggesting the two methods could be used interchangeably. Data provided by cycloplegic retinoscopy are preferable for quantifying the power of SE to be used for subjective refraction.
Data Sharing Statement
The data will be available upon request from the corresponding author.
Ethics Statement
The Kinshasa School of Public Health at the University of Kinshasa Institutional Ethical Review Board approved the study as per the tenets of the Declaration of Helsinki. Participation in the study required each participant to provide a written informed consent after a brief explanation of the objectives of the study. Participation in the study was voluntary without any type of coercion. Information collected was kept confidential.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. doi:10.1016/S2214-109X(17)30393-5
2. Safir A, Hyams L, Philpot J, Jagerman LS. Studies in refraction. I. The precision of retinoscopy. Arch Ophthalmol. 1970;84(1):49–61. doi:10.1001/archopht.1970.00990040051013
3. Asiedu K, Kyei S, Ampiah EE. Autorefraction, retinoscopy, javal’s rule, and Grosvenor’s modified javal’s rule: the best predictor of refractive astigmatism. J Ophthalmol. 2016;2016:3584137. doi:10.1155/2016/3584137
4. Guha S, Shah S, Shah K, Hurakadli P, Majee D, Gandhi S. A comparison of cycloplegic autorefraction and retinoscopy in Indian children. Clin Exp Optom. 2017;100(1):73–78. doi:10.1111/cxo.12375
5. Hashemi H, Khabazkhoob M, Asharlous A, Yekta A, Emamian MH, Fotouhi A. Overestimation of hyperopia with autorefraction compared with retinoscopy under cycloplegia in school-age children. Br J Ophthalmol. 2018;102(12):1717–1722. doi:10.1136/bjophthalmol-2017-311594
6. Naidoo KS, Raghunandan A, Mashige KP, et al. Refractive error and visual impairment in African children in South Africa. Invest Ophthalmol Vis Sci. 2003;44(9):3764–3770. doi:10.1167/iovs.03-0283
7. Pokupec R, Mrazovac D, Popovic-Suic S, Mrazovac V, Kordic R, Petricek I. Comparison between refractometer and retinoscopy in determining refractive errors in children–false doubt. Coll Antropol. 2013;37(Suppl 1):205–208.
8. Prabakaran S, Dirani M, Chia A, et al. Cycloplegic refraction in preschool children: comparisons between the hand-held autorefractor, table-mounted autorefractor and retinoscopy. Ophthal Physiol Opt. 2009;29(4):422–426. doi:10.1111/j.1475-1313.2008.00616.x
9. Rotsos T, Grigoriou D, Kokkolaki A, Manios N. A comparison of manifest refractions, cycloplegic refractions and retinoscopy on the RMA-3000 autorefractometer in children aged 3 to 15 years. Clin Ophthalmol. 2009;3:429–431. doi:10.2147/OPTH.S5145
10. Jorge J, Queiros A, Almeida JB, Parafita MA. Retinoscopy/autorefraction: which is the best starting point for a noncycloplegic refraction? Optom Vis Sci. 2005;82(1):64–68.
11. Bland JM, Altman DG. Comparing methods of measurement: why plotting difference against standard method is misleading. Lancet. 1995;346(8982):1085–1087. doi:10.1016/S0140-6736(95)91748-9
12. Bamdad S, Momeni-Moghaddam H, Abdolahian M, Pinero DP. Agreement of wavefront-based refraction, dry and cycloplegic autorefraction with subjective refraction. J Optom. 2020. doi:10.1016/j.optom.2020.08.008
13. Bogdanici CM, Sandulache CM, Vasiliu R, Obada O. Difference of refraction values between standard autorefractometry and plusoptix. Rom J Ophthalmol. 2016;60(4):249–254.
14. Choong YF, Chen AH, Goh PP. A comparison of autorefraction and subjective refraction with and without cycloplegia in primary school children. Am J Ophthalmol. 2006;142(1):68–74. doi:10.1016/j.ajo.2006.01.084
15. Demirci G, Arslan B, Ozsutcu M, Eliacik M, Gulkilik G. Comparison of photorefraction, autorefractometry and retinoscopy in children. Int Ophthalmol. 2014;34(4):739–746. doi:10.1007/s10792-013-9864-x
16. Egashira SM, Kish LL, Twelker JD, Mutti DO, Zadnik K, Adams AJ. Comparison of cyclopentolate versus tropicamide cycloplegia in children. Optom Vis Sci. 1993;70(12):1019–1026. doi:10.1097/00006324-199312000-00005
17. Honglertnapakul W, Jindarak P, Praneeprachachon P, Pukrushpan P. The difference of refraction between the cycloplegic retinoscopy and non-cycloplegic subjective refraction in children aged 6 to 15 years. J Med Assoc Thai. 2020;103(6):566–571.
18. Lowery JP, Joachim A, Olson R, Peel J, Pearce NN. Autorefraction vs. retinoscopy: a comparison of non-cycloplegic measures in a pediatric sample. J Behav Optom. 2005;16(1):4–8.
19. Jorge J, Queiros A, Gonzalez-Meijome J, Fernandes P, Almeida JB, Parafita MA. The influence of cycloplegia in objective refraction. Ophthal Physiol Opt. 2005;25(4):340–345. doi:10.1111/j.1475-1313.2005.00277.x
20. Rauscher FG, Lange H, Yahiaoui-Doktor M, et al. Agreement and repeatability of noncycloplegic and cycloplegic wavefront-based autorefraction in children. Optom Vis Sci. 2019;96(11):879–889. doi:10.1097/OPX.0000000000001444
21. Yoo SG, Cho MJ, Kim US, Baek SH. Cycloplegic refraction in hyperopic children: effectiveness of a 0.5% tropicamide and 0.5% phenylephrine addition to 1% cyclopentolate regimen. Korean J Ophthalmol. 2017;31(3):249–256. doi:10.3341/kjo.2016.0007
22. Li T, Zhou X, Zhu J, Tang X, Gu X. Effect of cycloplegia on the measurement of refractive error in Chinese children. Clin Exp Optom. 2019;102(2):160–165. doi:10.1111/cxo.12829
23. Fotedar R, Rochtchina E, Morgan I, Wang JJ, Mitchell P, Rose KA. Necessity of cycloplegia for assessing refractive error in 12-year-old children: a population-based study. Am J Ophthalmol. 2007;144(2):307–309. doi:10.1016/j.ajo.2007.03.041
24. Fotouhi A, Morgan IG, Iribarren R, Khabazkhoob M, Hashemi H. Validity of noncycloplegic refraction in the assessment of refractive errors: the Tehran Eye Study. Acta Ophthalmol. 2012;90(4):380–386. doi:10.1111/j.1755-3768.2010.01983.x
25. Hu YY, Wu JF, Lu TL, et al. Effect of cycloplegia on the refractive status of children: the Shandong children eye study. PLoS One. 2015;10(2):e0117482. doi:10.1371/journal.pone.0117482
26. Liu X, Ye L, Chen C, Chen M, Wen S, Mao X. Evaluation of the necessity for cycloplegia during refraction of Chinese children between 4 and 10 years old. J Pediatr Ophthalmol Strabismus. 2020;57(4):257–263. doi:10.3928/01913913-20200407-01
27. Sankaridurg P, He X, Naduvilath T, et al. Comparison of noncycloplegic and cycloplegic autorefraction in categorizing refractive error data in children. Acta Ophthalmol. 2017;95(7):e633–e640. doi:10.1111/aos.13569
28. Zhao J, Mao J, Luo R, Li F, Pokharel GP, Ellwein LB. Accuracy of noncycloplegic autorefraction in school-age children in China. Optom Vis Sci. 2004;81(1):49–55. doi:10.1097/00006324-200401000-00010
29. Zhu D, Wang Y, Yang X, et al. Pre- and postcycloplegic refractions in children and adolescents. PLoS One. 2016;11(12):e0167628. doi:10.1371/journal.pone.0167628
30. Cheng HC, Hsieh YT. Short-term refractive change and ocular parameter changes after cycloplegia. Optom Vis Sci. 2014;91(9):1113–1117. doi:10.1097/OPX.0000000000000339
31. Huang F, Huang S, Xie R, et al. The effect of topical administration of cyclopentolate on ocular biometry: an analysis for mouse and human models. Sci Rep. 2017;7(1):9952. doi:10.1038/s41598-017-09924-5
32. Marchini G, Babighian S, Tosi R, Perfetti S, Bonomi L. Comparative study of the effects of 2% ibopamine, 10% phenylephrine, and 1% tropicamide on the anterior segment. Invest Ophthalmol Vis Sci. 2003;44(1):281–289. doi:10.1167/iovs.02-0221
33. Ganger A, Bala S, Kaur I, Satpal KP. Comparison of autorefractometer, retinoscope and subjective method ni myopic and hypermetropic patients. Int J Contemp Med Res. 2017;4(3):740–743.
34. Ozdemir O, Ozen Tunay Z, Petricli IS, Erginturk Acar D, Erol MK. Comparison of non-cycloplegic photorefraction, cycloplegic photorefraction and cycloplegic retinoscopy in children. Int J Ophthalmol. 2015;8(1):128–131. doi:10.3980/j.issn.2222-3959.2015.01.24
35. Iuorno JD, Grant WD, Noel LP. Clinical comparison of the welch allyn SureSight handheld autorefractor versus cycloplegic autorefraction and retinoscopic refraction. J AAPOS. 2004;8(2):123–127. doi:10.1016/j.jaapos.2003.10.006
36. Pedamallu S, Reddy K, Pedamallu R, Pedamallu C. Reliability of cycloplegic autorefractor measurements to determine spherical and astigmatism refractive errors in young children. Internet J Ophthalmol Vis Sci. 2008;6(1):1–5.
37. Adyanthaya S, Abhilash B. A comparison between retinoscopy and autorefraction in acceptance of subjective correction in school age children. Indian J Clin Exp Ophthalmol. 2020;6(3):418–421. doi:10.18231/j.ijceo.2020.090
38. Deepikadevi SN, Sundararajan D, Bhuvaneshwari K, Krishnan M. Comparing the effect of conventional method of retinoscopic refraction with computerized automated refraction in various refractive error patients. IJAM. 2017;4(10):104–110.
39. Hashemi H, Khabazkhoob M, Asharlous A, et al. Cycloplegic autorefraction versus subjective refraction: the Tehran Eye Study. Br J Ophthalmol. 2016;100(8):1122–1127. doi:10.1136/bjophthalmol-2015-307871
40. Joubert L, Harris WF. Excess of autorefraction over subjective refraction: dependence on age. Optom Vis Sci. 1997;74(6):439–444. doi:10.1097/00006324-199706000-00029
41. Kleinstein RN, Jones LA, Hullett S, et al. Refractive error and ethnicity in children. Arch Ophthalmol. 2003;121(8):1141–1147. doi:10.1001/archopht.121.8.1141
42. Rudnicka AR, Kapetanakis VV, Wathern AK, et al. Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis: implications for aetiology and early prevention. Br J Ophthalmol. 2016;100(7):882–890. doi:10.1136/bjophthalmol-2015-307724
43. Rudnicka AR, Owen CG, Nightingale CM, Cook DG, Whincup PH. Ethnic differences in the prevalence of myopia and ocular biometry in 10- and 11-year-old children: the Child Heart and Health Study in England (CHASE). Invest Ophthalmol Vis Sci. 2010;51(12):6270–6276. doi:10.1167/iovs.10-5528
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.