Back to Journals » Psychology Research and Behavior Management » Volume 18
Ageism and Career Motivation Toward Gerontological Nursing in the Post-Pandemic Era: A Sequential-Parallel Mediation Analysis Among Early-Stage Nursing Students
Received 1 June 2025
Accepted for publication 31 August 2025
Published 16 September 2025 Volume 2025:18 Pages 2009—2028
DOI https://doi.org/10.2147/PRBM.S539792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Bao-Liang Zhong
Se Chen,1 Zhonglei Wan2
1School of International Education, Jiangxi Science and Technology Normal University, Nanchang, Jiangxi, People’s Republic of China; 2Department of General Education, Jiangxi Youth Vocational College, Nanchang, Jiangxi, People’s Republic of China
Correspondence: Se Chen, School of International Education, Jiangxi Science and Technology Normal University, 589 Xuefu Avenue, Nanchang, Jiangxi, 330038, People’s Republic of China, Tel +8618679059130, Email [email protected]
Background: The growing aging population has led to escalating demands for gerontological nursing, further intensified by the COVID-19 pandemic. While ageism is a recognized barrier to nursing students’ career motivation toward gerontological nursing (CMGN), the underlying mechanisms through which it exerts influence remain underexplored. Moreover, empirical research on CMGN and related factors in the post-pandemic context is limited.
Objective: This study examined the levels and predictors of CMGN among early-stage nursing students in the post-pandemic context and explored how ageism influences CMGN directly and indirectly through a sequential-parallel mediation model.
Methods: A cross-sectional online survey was conducted at a medical university in Jiangxi Province, China. A total of 1,192 completed questionnaires from nursing students (mean age = 18.44; 90.3% female; 85.6% first-year students) across two academic tracks (bachelor’s and diploma programs) were included in the analysis. T-tests, ANOVA, regression, and structural equation modeling were used to identify key predictors and mediating pathways.
Results: Students reported a moderate overall level of CMGN (M = 64.12, SD = 12.86; range = 20– 100). Key predictors of both CMGN subscales—Expectancy and Value—with β > 0.1 and p < 0.01 included empathy, intergenerational contact quality, and learning experiences in gerontological nursing. Ageism was a dimension-specific negative predictor, affecting only the Value subscale (β = − 0.212, p < 0.001). Mediation analysis further showed that ageism influenced Value both directly (β = − 0.200, p < 0.001) and indirectly (β = − 0.124, p < 0.001) through a sequential pathway involving contact quality and Expectancy, as well as a parallel pathway mediated by gratitude.
Conclusion: The multifaceted negative impact of ageism on CMGN underscores the need for a holistic curriculum strategy. Key recommendations include integrated gerontological nursing education, anti-ageism instruction, interventions to foster gratitude and empathy, and interpersonal communication training tailored to geriatric care.
Keywords: gerontological nursing, ageism, career motivation, intergenerational contact, gratitude
Introduction
The rapid global aging trend is becoming increasingly pressing. According to the World Health Organization (WHO), by 2030, one in six people worldwide will be aged 60 years or older. By 2050, the global population of individuals aged 60 years and older is projected to double to 2.1 billion, and the number of persons aged 80 years or older is expected to triple, reaching 426 million. 1,2 This demographic shift poses unique challenges to healthcare systems worldwide, particularly in providing competent and compassionate care for older adults. This is especially significant in low- and middle-income countries, where 80% of older adults will reside by 2050. 2
Simultaneously, the nursing workforce is facing severe strain. The International Council of Nurses has reported that the COVID-19 pandemic has had a devastating impact on the global nursing workforce. Despite efforts to recover, the nursing sector remains in the early stages of recuperation, highlighting the worldwide shortage of nurses as a global health emergency. 3 This situation exacerbates the significant workforce shortage in gerontological nursing, further compounded by a longstanding lack of interest among nursing students in pursuing careers in this field across the world.4–9
Career motivation toward gerontological nursing (CMGN) among students is shaped by a complex interplay of psychological and structural factors. Although a substantial body of research has explored the factors influencing CMGN, findings have been inconsistent, and a consensus has yet to be established within the field. Among the various factors previously examined, several have consistently emerged as significant influencers. These include psychological attributes such as ageism and attitudes toward older adults, aging anxiety, empathy, and gratitude.6,10–19 Additionally, socio-demographic characteristics such as the frequency and quality of inter-generational interactions, gerontological nursing education experience, experience in caring for older adults, and the clinical practice environment have also been suggested as influential.6,11,13,14,16,20–24
In the Chinese cultural context, traditional Confucian values emphasize filial piety, respect for elders, and gratitude toward older generations.25,26 However, rapid modernization, urbanization, and demographic shifts—including declining family sizes, fewer multigenerational households, and increased geographic mobility—have weakened traditional family structures and reduced intergenerational contact, challenging the transmission of longstanding cultural values.27–29 Coupled with the accelerating pace of population aging—which may exacerbate intergenerational tensions—these structural changes, interacting with enduring filial norms, can foster ambivalent perceptions of older adults and gerontological care among younger generations.27,30–33
One manifestation of this ambivalence is “respectful ageism”, a China-specific phenomenon in which genuine cultural respect for older adults coexists with implicit discriminatory attitudes and practices, arising when traditional norms of honoring elders intersect with modern institutional structures that inadvertently marginalize them.27,33,34 Such ambivalence has implications not only for everyday intergenerational relationships but also for the younger generation’s professional attitudes toward gerontological care.
Given this context, it is essential to examine the relationship between socio-demographic and psychological factors—such as ageism and intergenerational contact—and CMGN through a nuanced lens that considers the mechanisms by which these factors operate. This focus is particularly relevant for early-stage nursing students, whose professional values remain malleable and responsive to educational influence, and whose formative experiences may shape their long-term career trajectories.5,23,35,36
Despite its significance, empirical research on CMGN in Chinese nursing students—especially those at early stages of training—remains limited in the post-2023 era, following the stabilization of disruptions caused by the COVID-19 pandemic. The pandemic exerted multifaceted impacts: it heightened vulnerabilities among older adults—increasing susceptibility to serious health complications, social isolation, and mental health decline—thereby escalating demand for gerontological healthcare.37–39 Concurrently, it intensified workforce strain through nurse burnout, stress, and accelerated retirements, further exacerbating preexisting staffing shortages.3,40 These intersecting challenges highlight an urgent need to investigate the factors and pathways shaping CMGN in the post-COVID context. In particular, the mechanisms underlying ageism warrant closer examination, given its role as a central psychological barrier in gerontological nursing.
Background
Ageism, a term introduced by Robert Butler in 1969, describes prejudice and discrimination directed toward individuals based on age.41,42 The WHO defines ageism as a multifaceted phenomenon comprising three dimensions—stereotypes (thoughts), prejudice (feelings), and discrimination (actions)—which can manifest at institutional, interpersonal, or self-directed levels and operate through explicit (conscious) or implicit (unconscious) mechanisms.43 In the context of nursing education, ageism is widely recognized as a significant barrier contributing to the persistent global shortage of interest among nursing students in pursuing gerontological nursing.4–6,9 Gherman et al further identified ageism as a mediating factor linking insufficient knowledge of aging, aging anxiety, and poor-quality intergenerational contact to nursing students’ reluctance to work with older adults.6
Despite these insights, there remains a considerable research gap concerning the complex mechanisms through which ageism influences nursing students’ willingness to engage in gerontological care. This includes exploring both direct and indirect effects, particularly how socio-demographic characteristics and psychological attributes act as intermediary variables.
Allport’s contact theory suggests that intergroup contact has the potential to mitigate prejudice among diverse social groups.44 Subsequent research has expanded the applicability of this theory beyond racial and ethnic encounters to include various intergroup contexts, such as interactions between different age groups.45 Empirical evidence supporting this notion suggests that positive interactions with older adults can diminish nursing students’ ageism and foster positive attitudes toward this demographic.46–49
The Expectancy-Value Theory suggests that individuals are more likely to engage in activities or goals when they believe in their ability to succeed and when they perceive the outcomes as valuable.50,51 Drawing on this theory, Cheng et al proposed that nursing students’ motivation for gerontological nursing consists of two components: “Expectancy”, which refers to their expectations of success in gerontological nursing, and “Value”, which pertains to their perceived worth and benefits of a career in this field.13
Previous research has demonstrated that the quality of intergenerational contact significantly predicts nursing students’ intentions to work with older adults.6,20,52 Building on this evidence and the previously discussed negative association between ageism and contact quality, we hypothesize a sequential pathway: higher levels of ageism reduce the quality of contact with older adults, which in turn lowers nursing students’ expectations of success in gerontological nursing, ultimately diminishing the value they place on this career path.
Furthermore, gratitude—defined as a psychological attribute characterized by a general tendency to acknowledge and emotionally respond with thankfulness to the benevolence of others—may also serve as a mediator in the relationship between ageism and valuation of gerontological nursing.53 A grateful disposition has been shown to foster more positive views of the aging process and may help counteract ageist beliefs.46 In addition, individuals with higher levels of gratitude are more likely to demonstrate a stronger willingness to care for older adults.5,18 This relationship may be particularly salient in the Chinese sociocultural context, where gratitude is deeply embedded in traditional values such as filial piety and respect for elders—core tenets of Confucianism that emphasize honoring older adults for their past contributions to family and society.25,26,54 These cultural norms are often reinforced through lived experiences; for example, many Chinese children are partially raised by grandparents, and such intergenerational caregiving has been empirically linked to increased gratitude and more positive attitudes toward older adults.13,15,18,31 Therefore, gratitude is also included as a key mediator in our conceptual framework.
Building on these insights, we propose a mediation model. Following Cheng et al, CMGN was deconstructed into two subscales: Expectancy and Value.13 The model explores the indirect effects of ageism on Value through two pathways: a sequential pathway involving two mediators—contact quality and Expectancy—and a parallel pathway with gratitude as the single mediator (see Figure 1).
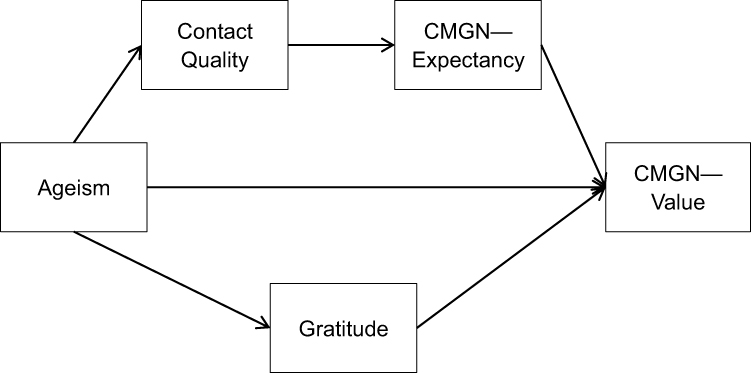 |
Figure 1 Proposed Sequential and Parallel Mediation Model. |
In summary, given the importance of better understanding early-stage nursing students’ CMGN and its influencing factors in the post-COVID-19 context, as well as the need to explore the multifaceted impacts of ageism and the mechanisms through which it operates, this study formulated three research questions (RQs):
RQ1: What are the current levels of CMGN among the nursing students in the sample?
RQ2: Which socio-demographic, psychological, or contact-related factors significantly influence nursing students’ CMGN?
RQ3: How does ageism directly and indirectly influence nursing students’ CMGN through the mediating effects of contact quality and gratitude?
Methods
Study Design and Participants
Research Setting
This study was conducted at a medical university in Jiangxi Province, China. Participants were nursing students enrolled in either a four-year bachelor’s degree program or a three-year diploma program. The university regularly updates its nursing curricula to align with evolving societal and healthcare demands. This research contributes to ongoing curriculum development in gerontological nursing, driven by the increasing care needs of an aging population.
Sample Size Planning
To determine the minimum sample size required to ensure sufficient statistical power for structural equation modeling (SEM), we conducted an “a priori power analysis” using the semPower R package.55 The degrees of freedom (df) for our hypothesized model (Figure 1) were calculated to be 4. Required sample sizes were estimated based on two commonly recommended thresholds for the Root Mean Square Error of Approximation (RMSEA), namely 0.06 and 0.08, which reflect benchmarks for close and reasonable model fit, respectively.56,57 Assuming an alpha level of 0.05 and a desired power of 0.80, the minimum sample size needed to detect moderate model misspecification (RMSEA = 0.08) was N = 467. To detect more subtle misspecification (RMSEA = 0.06), the required sample size increased to N = 831.
To account for potential invalid or incomplete responses—estimated at up to 15%—we applied an adjustment, yielding a conservative target sample size of approximately N = 978 (ie, 831 ÷ 0.85). This target was intended to ensure adequate statistical power even under more stringent model fit criteria.
Data Collection
A cross-sectional survey design was employed. Data were collected between October and November 2023 via an online questionnaire administered on the Chinese survey platform wjx.cn. A convenience sampling approach was adopted. Inclusion criteria were: (1) enrollment in either the bachelor’s or diploma nursing program at the target university at the time of data collection; (2) access to relevant class communication platforms (eg, WeChat or QQ) through which the survey link was distributed; and (3) voluntary participation. No explicit exclusion criteria were applied, in order to maximize inclusiveness and minimize selection bias within the accessible population.
The survey link was disseminated via class-based group chats by student counselors known to the researchers. Participation was entirely voluntary and anonymous. No personally identifiable information was collected. Ethical considerations related to participant protection are discussed in a later section.
Sample Overview and Data Quality
A total of 1,192 completed questionnaires were received. To minimize potential coercion and safeguard student autonomy, no direct invitations were sent. As a result, the total number of students reached and the response rate could not be determined.
All collected responses were initially screened for completeness and response patterns. To evaluate potential straight-lining behavior, we followed Collier’s recommendation to compute the standard deviation across all Likert-type scale items (excluding socio-demographic variables) for each respondent.58 The resulting within-respondent standard deviations ranged from 0.394 to 2.159 (Mean = 1.251, N = 1,192), all well above the 0.25 threshold commonly used to flag disengaged cases—indicating sufficient response variability and no evidence of flat-response patterns.58 Additional data quality checks were conducted to assess the item-level distribution of all scale items (also excluding socio-demographic variables). Skewness values ranged from −1.095 to +1.038, kurtosis from −0.784 to +0.915, and standard deviations from 0.595 to 1.554. Furthermore, no item had more than 70% of responses concentrated in a single category.
Together, these diagnostics suggest that the dataset does not exhibit problematic response characteristics and demonstrates sufficient variability and approximate normality to support further analysis.58–60 Therefore, all 1,192 responses were retained for analysis. The final sample had a mean age of 18.44 years (SD = 0.89). Of the respondents, 90.3% (n = 1,076) were female and 9.7% (n = 116) were male. In terms of academic year, 85.6% (n = 1,020) were first-year students, 13.6% (n = 162) were in their second year, and only 0.8% (n = 10) were in their third year or above. Information on academic track (ie, Bachelor’s vs Diploma) was not collected during the survey; therefore, program-level subgroup analyses could not be conducted. This point is further discussed in the Limitations section.
Ethical Considerations
This study received ethical approval from the Ethics Committee at Jiangxi Science and Technology Normal University (Reference No. 113182023080309) on August 3, 2023, and adhered to the ethical principles outlined in the Declaration of Helsinki. Informed consent was obtained through a consent form presented on the front page of the online questionnaire. The form provided detailed information about the study’s purpose, content, number of questions, estimated completion time, the researchers’ affiliations and contact information, and assurances regarding anonymity, voluntariness, and the right to withdraw at any time without consequences. No personally identifiable information—such as names or contact details—was collected, and participation was entirely voluntary. No monetary or material incentives were provided.
None of the researchers held teaching, administrative, or employment roles at the medical university where the study was conducted. Although university staff helped disseminate the survey, participants were repeatedly reminded of the voluntary and anonymous nature of their participation to minimize any perceived coercion. Data were collected anonymously using a secure online platform, and responses were submitted directly to the researchers without any identifying information, ensuring that individual students could not be linked to their responses.
Measurements
A self-designed questionnaire was used to collect demographic and contextual information. For key psychological constructs—including CMGN, ageism, aging anxiety, gratitude, and empathy—established scales were employed. For scales that were translated or adapted by the researchers of this study, additional validation analyses (eg, EFA and CFA) were conducted and reported to ensure construct validity in our sample. Below is a detailed description of the measurement tools used:
Career Motivation Toward Gerontological Nursing (CMGN)
To measure participants’ CMGN, we used the Motivations for Choosing Gerontological Nursing as a Career Questionnaire.13 This 20-item instrument, originally developed in Chinese and widely used in studies involving Chinese nursing students, comprises two subscales: Expectancy (uni-dimensional with 6 items) and Value (14 items).11,13,15,23 The Expectancy Subscale evaluates students’ perceptions of their capabilities and self-efficacy regarding a career in gerontological nursing. The Value Subscale assesses students’ valuation of such a career through four dimensions: interest (3 items), utility (3 items), attainment value (5 items), and cost (3 items). Responses were recorded on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), with higher scores indicating a stronger CMGN. The scale exhibited a Cronbach’s Alpha of 0.94 in this study, while the subscales showed Alpha values between 0.86 and 0.91.
Negatively worded items were reversed according to the original scale’s instructions, a detail consistently applied across all measurements and will not be reiterated in subsequent sections.
Ageism
Ageism was measured using the Chinese version of the Fraboni Scale of Ageism (CV-FSA).41,61 Originally conceptualized by Fraboni et al and translated and adapted by Fan et al, the CV-FSA comprises 22 items across three dimensions: Avoidance, Exclusion, and Stereotyping, rated on a 4-point Likert scale (1 = strongly disagree to 4 = strongly agree). Higher scores indicate stronger level of ageism. In this study, the overall Cronbach’s alpha was 0.92, with subscales ranging from 0.81 to 0.83.
Aging Anxiety
Aging anxiety was assessed using the revised Kafer Aging Anxiety Scale (KAS) adapted by Yan et al.62 This six-item unidimensional scale measures concerns about personal aging, with responses rated on a four-point Likert scale (1 = strongly disagree to 4 = strongly agree), where higher scores indicate greater aging anxiety. The translation of the KAS was conducted by the researchers and underwent independent translation, back-translation, and review by English language professionals to ensure linguistic and conceptual accuracy.
Exploratory factor analysis (EFA) supported a single-factor structure for the adapted KAS, consistent with the original scale. However, initial confirmatory factor analysis (CFA) indicated the need for modifications due to localized dependencies. The final CFA model incorporated correlated error terms for Questions 1 and 2 (both related to physical decline) and Questions 5 and 6 (both related to loss of autonomy). These adjustments improved model fit while preserving the scale’s unidimensional structure. The modified CFA demonstrated excellent fit (CFI = 0.99, TLI = 0.99, RMSEA = 0.06, SRMR = 0.02), with factor loadings ranging from moderate to strong (λ = 0.56–0.87, all p < 0.01). Internal consistency was high (α = 0.88), confirming the reliability of the adapted scale.
Gratitude
Gratitude was assessed using the Chinese version of the Gratitude Questionnaire-6 (GQ-6), originally developed by McCullough et al and translated and validated by Wei et al53,63 To better align with our participants, minor wording adjustments were made to the Chinese version of the GQ-6 based on feedback from a pilot study conducted prior to formal data collection. Participants responded on a seven-point Likert scale (1 = strongly disagree, 7 = strongly agree), with higher scores indicating greater levels of gratitude. The adapted GQ-6 demonstrated acceptable internal consistency in this study (Cronbach’s α = 0.75).
Empathy
Empathy was assessed using an adapted version of the Toronto Empathy Questionnaire (TEQ).64 This unidimensional instrument originally contained 16 items, evenly split between positively and negatively worded statements. In this study, the eight positively worded items were retained to reduce redundancy and minimize participant fatigue. Participants rated the frequency of their empathetic responses across various scenarios on a five-point Likert scale (1 = never to 5 = always), with higher scores indicating greater empathy.
The TEQ was translated into Chinese by the researchers following the same process described for the KAS. EFA supported a unidimensional structure; however, initial CFA indicated localized dependencies, suggesting the need to incorporate correlated error terms between Questions 8 and 9 (both related to implicit emotional detection) and Questions 13 and 16 (both related to proactive protective responses) of the original TEQ. The final CFA model for the adapted TEQ demonstrated good fit (CFI = 0.98, TLI = 0.97, RMSEA = 0.07, SRMR = 0.02), with strong factor loadings (λ = 0.67–0.86, all p < 0.01). Internal consistency was excellent (α = 0.93), confirming the reliability of the adapted scale.
Contact Frequency and Quality
Contact frequency with older adults was assessed using a single self-reported item developed by the researchers: “How often have you been in contact with older adults recently?” Responses were recorded on a 5-point Likert scale ranging from 1 (“Rarely”) to 5 (“Very Frequently”). Similarly, contact quality was measured with the item: “How would you rate the quality of your interactions with older adults?” using a 5-point Likert scale ranging from 1 (“Terrible”) to 5 (“Excellent”). These items were intentionally broad and did not specify the context or formality of contact (eg, informal vs clinical, everyday vs structured), allowing for a wide range of intergenerational experiences to be captured. This approach aligns with the study’s focus on general intergenerational contact rather than structured clinical exposure.
Socio-Demographic Factors
This study incorporates ten socio-demographic factors, with shorter names (provided in parentheses) used throughout the article for clarity and conciseness. These factors include: “gender”, “age”, “academic year”, whether participants are an only child at home (“only-child status”), self-rated health status (“health”), the frequency of receiving care from older relatives during childhood (“childhood care-receiving”), the frequency of co-residing with older people at home (“co-residence frequency”), self-reported level of exposure to gerontological nursing knowledge and courses (“learning experience”), the frequency of engaging in practice-based gerontological nursing training (“training experience”), and the frequency of participating in care for older adults (“caregiving frequency”). Each factor was measured using a single-item question specifically designed by the researchers to capture the relevant aspect of the participant’s background.
Data Analysis
Analytical Strategy by Research Question
The study addressed three RQs using distinct analytical approaches. RQ1 concerns the current levels of CMGN among nursing students. To address this and to characterize the psychological and contact-related variables of interest, descriptive statistics were used, including means, standard deviations (SD), possible score ranges, and Cronbach’s α coefficients to assess internal consistency.
RQ2, which examines factors influencing CMGN, was addressed using regression analysis. Prior to this, preliminary variable screening was conducted to inform predictor selection. Independent-samples t-tests and ANOVA (with Bonferroni correction for multiple comparisons) were used to assess differences in CMGN across categorical socio-demographic variables. Pearson correlation analyses were conducted to examine associations between CMGN and psychological/contact-related variables. Only variables demonstrating statistically significant differences or correlations were included as predictors in a multiple linear regression model.
RQ3, which explores both the direct effects of ageism on CMGN and the indirect effects mediated by contact quality and gratitude, was addressed using structural equation modeling (SEM) conducted in R. The model incorporated both sequential and parallel mediation pathways, with ageism as the independent variable and the Value subscale of CMGN as the dependent variable. In the sequential mediation pathway, contact quality served as the first mediator, followed by the Expectancy subscale. In the parallel pathway, gratitude functioned as an independent mediator (see Figure 1).
Statistical Thresholds and Interpretive Criteria
To ensure consistency and clarity in interpreting results, the following threshold criteria were applied:
- Statistical significance: All hypothesis tests were two-tailed, with statistical significance determined at α = 0.05.
- Descriptive categorization of Likert-based variables: Scales composed of Likert-type items were trichotomized for descriptive interpretation by dividing their theoretical score ranges into equal thirds and labeling them as low, moderate, and high. For example, for a scale ranging from 22 to 88, scores from 22–43.99 were classified as low, 44–65.99 as moderate, and 66–88 as high. This proportional tertile approach is commonly used in social science research to facilitate interpretation across measures.65,66
- Correlation magnitude: Following Cohen’s guidelines, Pearson correlation coefficients were interpreted as follows: |r| ≈ 0.10–0.29 = small, 0.30–0.49 = medium, and ≥ 0.50 = large.67
- Indirect effect estimation: In the SEM, indirect, direct, and total effects were estimated using bootstrapping with 5,000 iterations to generate 95% bias-corrected bootstrap confidence intervals (95% BCCI). Effects were considered statistically significant if the 95% BCCI did not include zero. Fully standardized path coefficients (β) were reported to support interpretation.68
- Model fit for SEM: Model fit was evaluated using the Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), Root Mean Square Error of Approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR). Thresholds for acceptable and excellent fit were as follows: CFI and TLI ≥ 0.90 (acceptable) or ≥ 0.95 (excellent), RMSEA ≤ 0.08 (acceptable) or ≤ 0.06 (excellent), and SRMR ≤ 0.08.56,57
Results
Sample Characteristics and Descriptive Statistics for RQ1
A total of 1,192 valid responses were included in the analysis. Participants had a mean age of 18.44 years (SD = 0.89), with females comprising 90.3% (n = 1,076) of the sample and males 9.7% (n = 116). Most were first-year students (85.6%, n = 1,020), followed by second-year (13.6%, n = 162) and third year or above (0.8%, n = 10). The majority (88.7%) reported that they were not an only child at home. Most participants (88.1%) rated their health as “fair” or “good.”
Childhood care-receiving from older relatives was reported as rare (15.4%), occasional (27.5%), frequent (32.9%), or constant (24.2%). Co-residence with older adults followed a similar distribution: rare (24.6%), occasional (30.3%), frequent (17.3%), and constant (27.8%). In terms of recent involvement in caring for older adults, 36.7% were rarely engaged, 54.0% occasionally participated, 8.1% frequently participated, and 1.2% were constantly engaged.
Given the predominance of early-year students, most had limited exposure to formal gerontological coursework or clinical placements at the time of the survey. Overall, 59.6% reported no gerontological nursing learning experience, 35.9% had brief exposure, and 4.5% had systematic instruction. Practical training experience was even less common, with 87.0% reporting none, 11.5% occasional, and 1.5% systematic training.
Descriptive statistics for the main study variables showed a moderate level of CMGN overall (M = 64.12, SD = 12.86, range 20–100). The Expectancy subscale averaged 18.69 (SD = 4.96, range 6–30) and the Value subscale 45.42 (SD = 8.68, range 14–70). Participants exhibited a moderate overall level of ageism, with a total mean score of 46.59 (SD = 9.96, range 22–88). The ageism subscales recorded the following means: Avoidance at 15.51 (SD = 3.72, range 8–32), Excluded at 14.63 (SD = 3.58, range 7–28), and Stereotype at 16.45 (SD = 3.71, range 7–28).
Aging Anxiety among participants was moderate, with a mean score of 15.72 (SD = 4.05, range 6–24). Gratitude and Empathy scores fell within the high range but were close to the moderate–high cutoff, with means of 31.46 (SD = 5.37, range 6–42) and 30.54 (SD = 5.54, range 8–40), respectively. Participants reported moderate contact frequency with older adults, with a mean score of 2.96 (SD = 1.21, range 1–5), and somewhat more favorable contact quality, with a mean of 3.50 (SD = 0.75, range 1–5), though both remained within the moderate range.
Table 1 presents the descriptive statistics for CMGN, psychological, and contact variables, and Table 2 presents the distribution of socio-demographic factors.
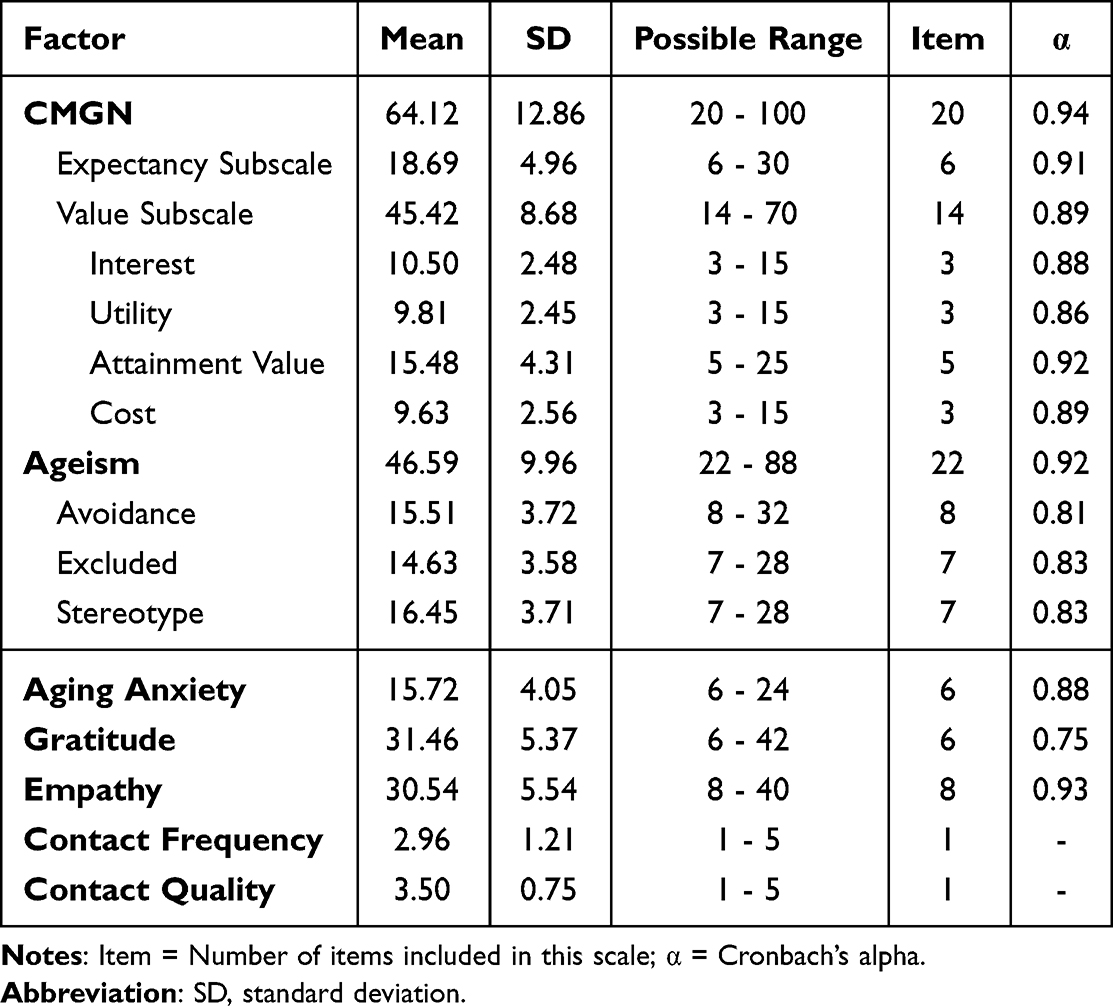 |
Table 1 Descriptive Analysis of CMGN, Psychological, and Contact Variables (N = 1192) |
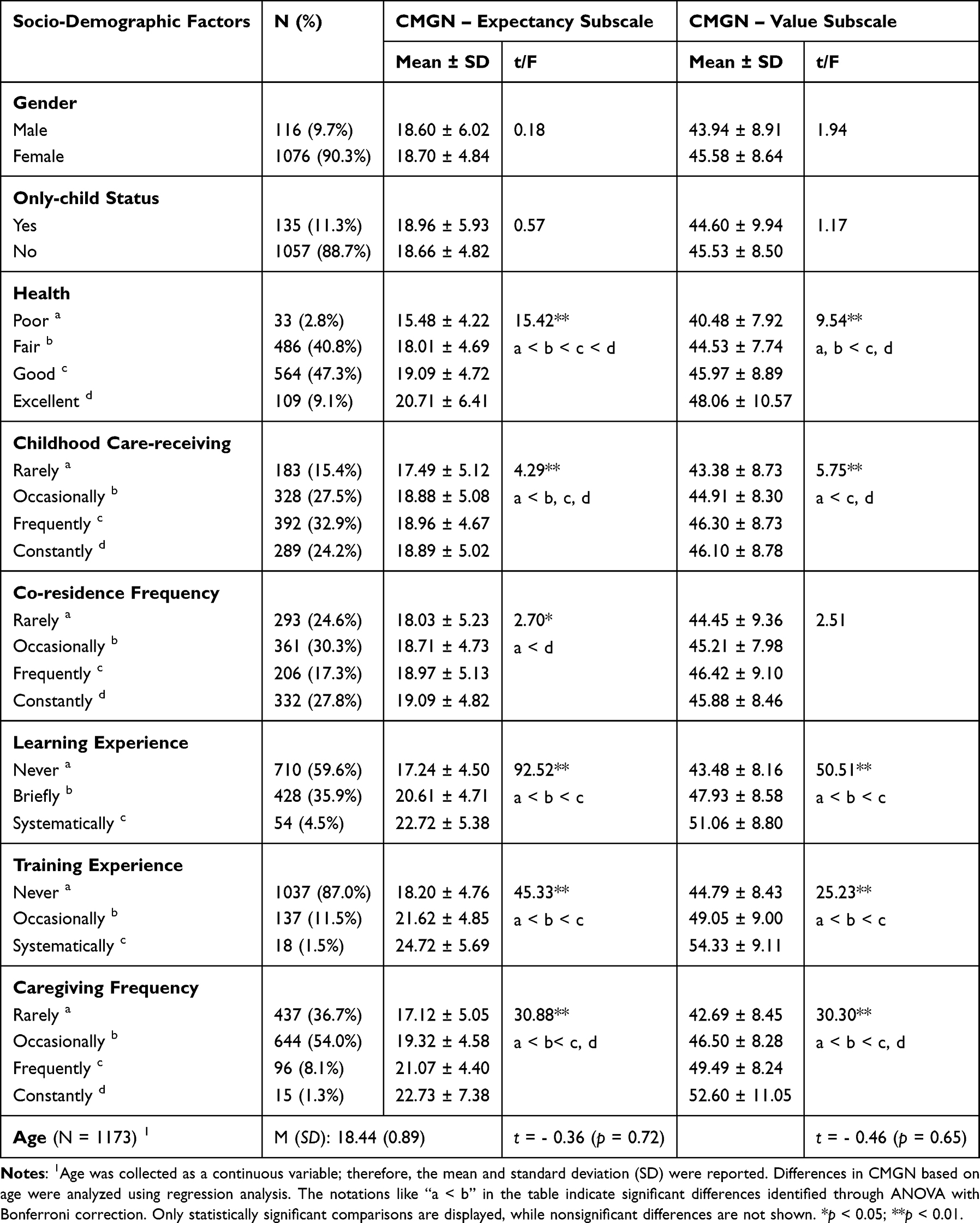 |
Table 2 Socio-Demographic Factors, and Variation in CMGN Sub-Scales by Factors (N = 1192) |
Results for RQ2: Factors Influencing CMGN
Differences in CMGN Across Demographic Variables
Differences in CMGN—measured through the Expectancy and Value subscales—across the socio-demographic variables are also presented in Table 2. Significant differences were identified for six factors: self-rated health, childhood care-receiving, learning experience, training experience, caregiving frequency, and co-residence frequency.
Students with better self-rated health reported significantly higher scores on both the Expectancy and Value subscales compared to those with poorer health (p < 0.01). Similarly, students who had more frequent care-receiving experiences from older relatives during childhood scored higher on both subscales than those with limited or no such experience (p < 0.01).
Notable differences were also found based on gerontological learning and training. Students with greater exposure to gerontological nursing—whether through theoretical learning or practical training—consistently reported higher levels on both the Expectancy and Value subscales compared to those with limited exposure (p < 0.01).
A comparable trend was observed in relation to caregiving experience: students who more frequently provided care to older adults reported significantly stronger career motivation across both subscales (p < 0.01), suggesting a cumulative benefit from real-world involvement.
Co-residence with older adults had a smaller but statistically significant effect on Expectancy (p < 0.05), with higher scores observed among students who co-resided constantly. However, its effect on the Value subscale was not significant (p > 0.05).
In contrast, gender, only-child status, and age did not yield significant differences on either subscale (p > 0.05), indicating that these demographic characteristics may have limited influence on early-stage students’ CMGN.
Correlations Between CMGN and Psychological and Contact Variables
Table 3 presents the correlation analysis results between CMGN and psychological and contact variables.
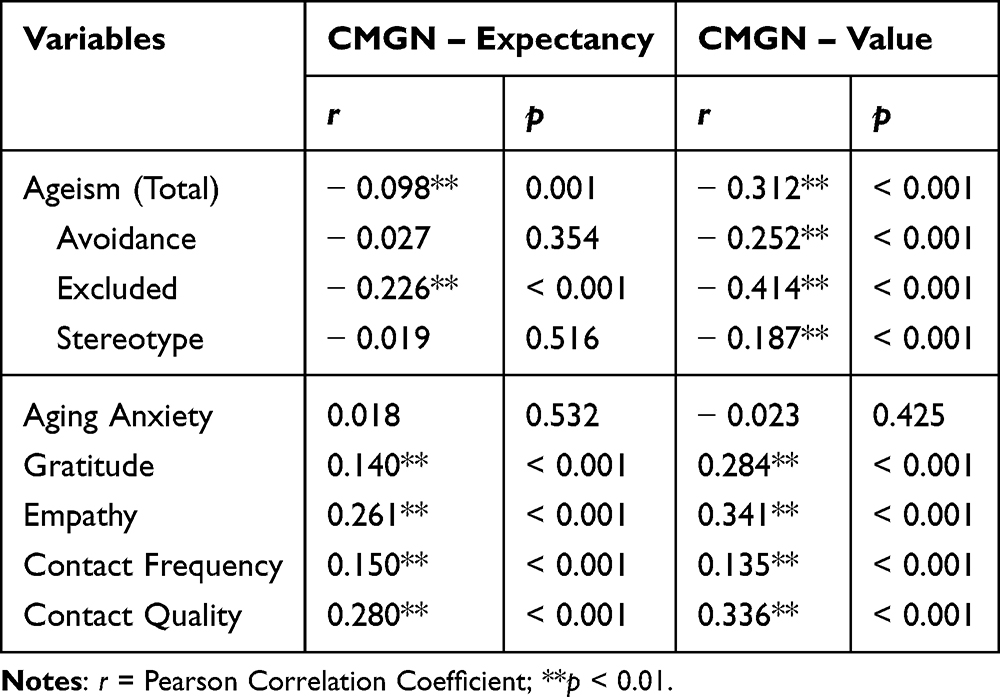 |
Table 3 Correlations Between CMGN and Psychological and Contact Variables |
A very small but statistically significant negative correlation was observed between total ageism and the CMGN Expectancy subscale (r = –0.098, p = 0.001). However, the effect size suggests that this association is negligible in practical terms. In contrast, a moderate negative correlation was found with the Value subscale (r = –0.312, p < 0.001), suggesting a more substantial relationship.
Gratitude and Empathy were both positively associated with the CMGN subscales. For Expectancy, Gratitude showed a small correlation (r = 0.140, p < 0.001), and Empathy a small-to-moderate correlation (r = 0.261, p < 0.001). For Value, Gratitude showed a small correlation, nearing moderate strength (r = 0.284, p < 0.001), while Empathy showed a moderate correlation (r = 0.341, p < 0.001).
Both the frequency (r = 0.150, p < 0.001) and quality (r = 0.280, p < 0.001) of contact with older adults were positively correlated with the Expectancy subscale. Similarly, frequency (r = 0.135, p < 0.001) and quality (r = 0.336, p < 0.001) of contact were positively associated with the Value subscale. These correlations ranged from small to moderate in strength.
In contrast, aging anxiety did not demonstrate any significant correlation with either Expectancy (r = 0.018, p = 0.532) or Value (r = −0.023, p = 0.425), indicating a negligible linear relationship.
Predictors of CMGN
To identify predictors of CMGN, multiple linear regression analyses were conducted using the two subscales of CMGN—Expectancy and Value—as dependent variables in two separate regression models. A total of 11 independent variables were selected based on their varied impact on CMGN or their significant correlations with CMGN. These variables included ageism, gratitude, empathy, contact frequency, contact quality, health, childhood care-receiving, co-residence frequency, learning experience, training experience, and caregiving frequency. Table 4 presents the regression results.
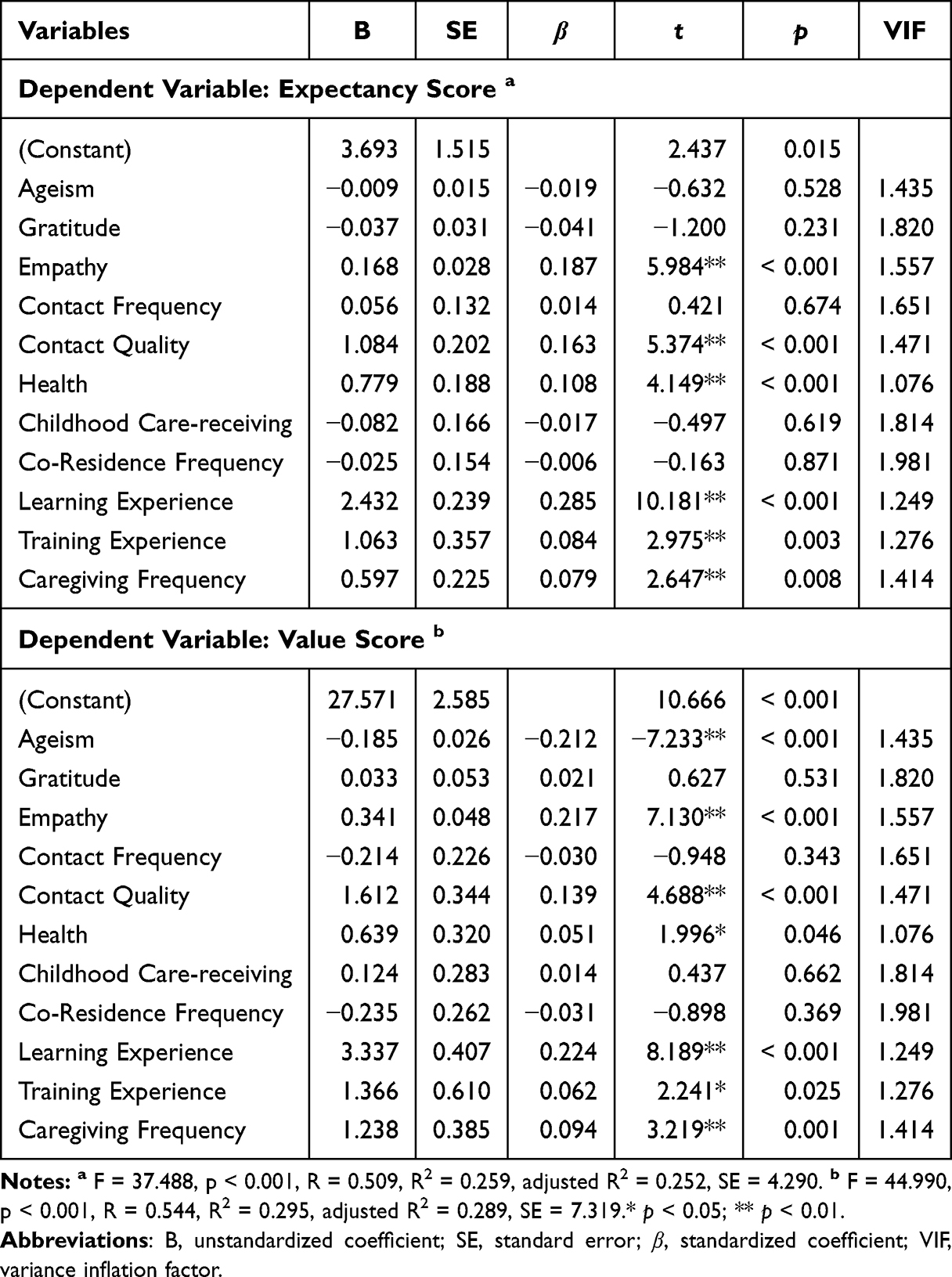 |
Table 4 Predictors of CMGN (N = 1192) |
For the Expectancy score, significant predictors included empathy (β = 0.187, p < 0.001), contact quality (β = 0.163, p < 0.001), health (β = 0.108, p < 0.001), learning experience (β = 0.285, p < 0.001), training experience (β = 0.084, p = 0.003), and caregiving frequency (β = 0.079, p = 0.008). For the Value score, ageism showed a significant negative influence (β = −0.212, p < 0.001), whereas positive influences were noted for empathy (β = 0.217, p < 0.001), contact quality (β = 0.139, p < 0.001), health (β = 0.051, p = 0.046), learning experience (β = 0.224, p < 0.001), training experience (β = 0.062, p = 0.025), and caregiving frequency (β = 0.094, p = 0.001).
Learning experience, empathy, and contact quality emerged as the most significant predictors for both Expectancy and Value scores, with learning experience being the strongest predictor across all evaluated independent variables, highlighting the essential role of educational exposure in shaping students’ CMGN. Ageism, although not a significant predictor for the Expectancy score, emerged as a notable negative influencer for the Value score, suggesting that ageism considerably diminish students’ valuation of gerontological nursing as a career path.
Gratitude, contact frequency, childhood care-receiving, and co-residence frequency did not significantly predict either subscale. The regression models demonstrated substantial explanatory power, with adjusted R2 values of 0.252 for Expectancy, and 0.289 for Value. The models’ integrity is further supported by Variance Inflation Factor (VIF) values ranging from 1.076 to 1.981, indicating a minimal presence of multicollinearity.
Results for RQ3: Mediation Pathways from Ageism to CMGN
Figure 2 presents an overview of the mediation SEM model, and Table 5 summarizes the detailed results of the mediation analysis. The model fit indices suggested an overall acceptable fit to the data, with a CFI of 0.983 and a TLI of 0.958, both indicating a good fit. The RMSEA of 0.080 falls within a marginally acceptable range, while the SRMR of 0.043 indicates an ideal fit.
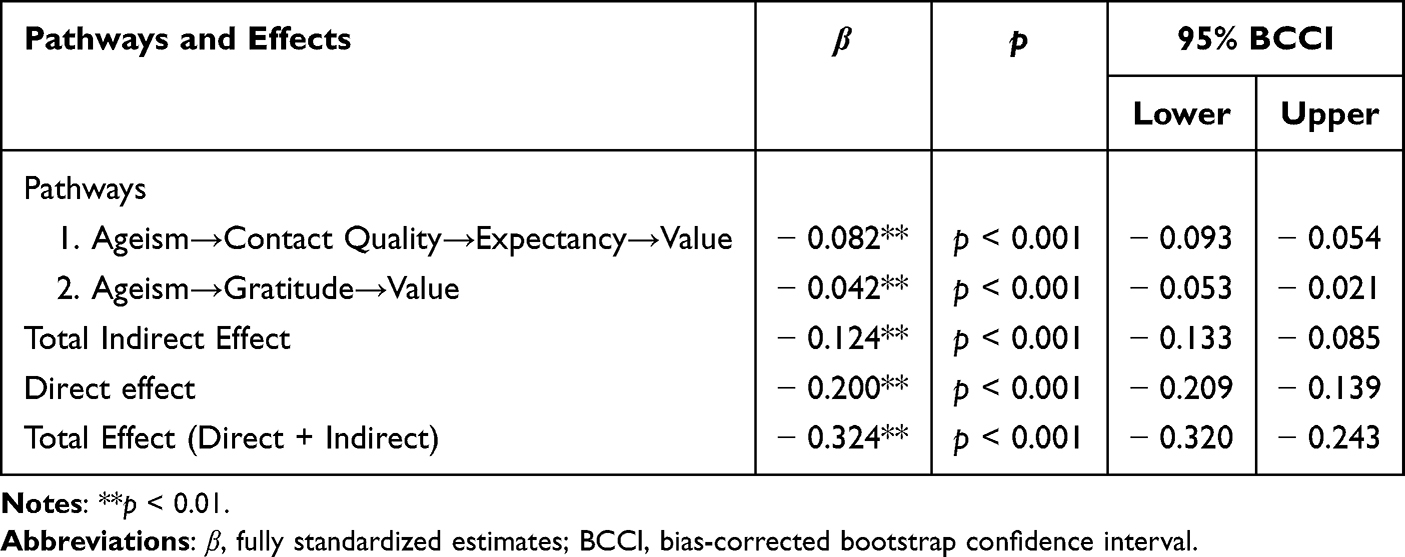 |
Table 5 SEM Mediation Analysis Results |
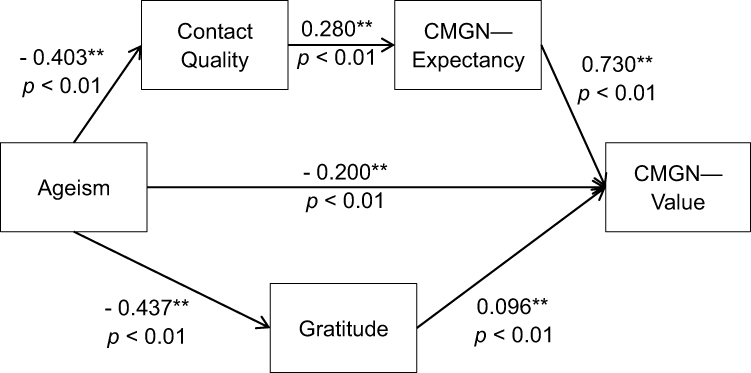 |
Figure 2 Mediation Pathways from Ageism to CMGN. Model Fit Summary: CFI = 0.983, TLI = 0.958, RMSEA = 0.080, SRMR = 0.043. Note: All values presented in the figure are fully standardized estimates (β); **p < 0.01. |
Path analysis revealed that ageism significantly impacts students’ valuation of a career in gerontological nursing through two pathways. The first pathway demonstrates that ageism leads to poorer contact quality with older adults (β = - 0.403, p < 0.001), which in turn negatively impacts students’ expectancy regarding gerontological nursing (β = 0.280, p < 0.001), ultimately reducing their valuation of this career path (β = 0.730, p < 0.001). The second pathway shows that ageism diminishes students’ level of gratitude (β = - 0.437, p < 0.001), which subsequently lowers their perceived value of a career in gerontological nursing (β = 0.096, p < 0.001).
The total indirect effect, encompassing the first pathway (β = - 0.082, p < 0.001, 95% BCCI [- 0.093, - 0.054]) and the second pathway (β = - 0.042, p < 0.001, 95% BCCI [- 0.053, - 0.021]), was significant (β = - 0.124, p < 0.001, 95% BCCI [- 0.133, - 0.085]). These results highlight the critical role of psychological and social mechanisms in mediating the impact of ageism on students’ CMGN. Additionally, even after accounting for these indirect effects, the direct effect of ageism on students’ valuation of gerontological nursing remained substantial and negative (β = - 0.200, p < 0.001, 95% BCCI [- 0.209, - 0.139]), highlighting the pervasive influence of ageism.
Discussion
Discussion for RQ1: CMGN Levels and Early Preparation
Students in this study reported moderate levels of CMGN, with room for improvement in motivation and commitment. Compared to previous studies using the same scale among Chinese nursing students, our early-year participants scored lower than those in Cheng et al’s study of final-year students post-clinical practice,13 Chai et al’s longitudinal study during clinical placements,11 and Wang et al’s sample spanning various academic stages.23 However, their scores were higher than those reported by Guo et al, who surveyed nursing undergraduates across all academic years.15
These discrepancies may be attributed to a range of factors, including regional differences, institutional contexts, cohort effects, and — most notably — students’ academic stage and level of clinical exposure. The trend of higher CMGN scores observed in studies involving final-year students provides partial support for our finding that learning and training experiences in gerontological nursing are significant positive predictors of CMGN. This alignment also corroborates broader literature emphasizing the role of structured educational and clinical experiences in shaping students’ attitudes toward gerontological care.11,14,22,35,36,69
Nevertheless, nursing educators must recognize that the effects of clinical experiences are not uniformly positive. Prior research has shown that negative encounters—such as unsupportive work environments, complex interpersonal dynamics, and emotionally demanding situations—can erode students’ initial interest in gerontological nursing.11,13,22,70 This is especially relevant for early-year students—such as those in the present study—who are at a formative stage in their professional development, with career attitudes that remain malleable and highly influenced by early clinical exposure.
It is therefore essential for educators to proactively prepare these students for working with older adults by equipping them with the necessary skills, knowledge, and confidence to navigate the challenges of gerontological care before entering practice. Equally important is the provision of timely support to help students process and adapt to these challenges as they arise during clinical placements.5,13,22,70–72 In addition, integrating interpersonal learning into pre-clinical curricula is essential for building students’ confidence—this point will be elaborated upon later in this section.
While these approaches are critical for preparing students for practice, developing a sustainable workforce equipped to meet the needs of an aging society also requires targeted interventions. Educators should design these interventions based on a nuanced understanding of the factors influencing students’ CMGN, with the goal of reinforcing enabling influences and mitigating inhibiting ones. The following subsection discusses these factors in detail.
Discussion for RQ2: Predictors of CMGN and Targeted Interventions
This study identified several significant predictors of CMGN, including self-rated health, empathy, intergenerational contact quality, learning and training experiences in gerontological nursing, caregiving experience with older adults, and ageism.
Ageism demonstrated a dimension-specific effect: it was a strong negative predictor of the Value subscale—reflecting the perceived importance and benefits of pursuing a career in gerontological nursing—but showed a non-significant regression coefficient and only a trivially small zero-order correlation with the Expectancy subscale, which captures students’ confidence in their ability to succeed in such a career. Given the negligible bivariate association with Expectancy, the absence of a regression effect is unlikely to result from shared variance with other predictors. Instead, the findings suggest that ageism more directly diminishes the perceived value of gerontological nursing, while its impact on self-efficacy beliefs may be more indirect or diffuse. By disaggregating CMGN into its Expectancy and Value components, the present study offers a dimension-specific understanding of ageism’s influence, thereby extending previous research on this relationship.10,14–17,22,73–75
Given the identified negative role of ageism, there is an urgent need for nursing educators to implement targeted anti-ageism interventions within the curriculum. Such interventions may include both stand-alone modules and integrated content within other courses, aimed at dispelling myths about aging, challenging stereotypes, and promoting accurate, evidence-based knowledge about older adults.76–79 In addition, incorporating moral sensitivity training has shown promise in fostering professional values, reducing ageism, and enhancing nursing students’ intentions to work with older adults.6
While ageism poses a barrier, empathy serves as a facilitator of CMGN, corroborating findings from previous studies.10,11,52 Empathy is associated with prosocial motivation and altruistic behavior, and it fosters a deeper understanding and appreciation of diversity.52,80 These qualities may enhance students’ empathetic responses toward individuals experiencing age-related physical or social challenges, thereby increasing their motivation to pursue a career in gerontological nursing.
Given its importance, empathy training should be an integral component of the nursing curriculum. Educators are encouraged to adopt experiential and reflective pedagogies which demonstrate their effectiveness in fostering empathy and reducing ageism among nursing students. For instance, workshops that prompt students to reflect on their interactions with older adults, examine their perceptions of aging, and identify enablers and barriers to expressing empathy toward older individuals can provide a structured environment for deepening understanding of aging and promoting compassionate care.81 Moreover, interventions such as the Aging Game—which engages students in role-playing as older adults with physical limitations—have been shown to enhance empathy, raise awareness of age-related challenges, and reduce ageism.82 Such interventions bridge theory and practice, translating classroom-based learning into real-world empathetic engagement.46,52,81,83
The quality of intergenerational contact also emerged as a strong predictor of CMGN, whereas contact frequency did not. This distinction is consistent with previous findings indicating that meaningful, high-quality interactions—rather than mere exposure—are more influential in shaping positive attitudes toward older adults and enhancing motivation for gerontological careers.6,20,52,84 These insights underscore the need for nursing educators to design pedagogical interventions—such as thoughtfully structured clinical placements and community-based programs—that facilitate authentic, empathic, and reciprocal engagement, prioritizing relational quality over the quantity of contact.11,21,85
In sum, the findings from RQ2 highlight a constellation of factors that significantly influence students’ CMGN. These insights offer important reference points for educators in designing targeted interventions that enhance positive influences while addressing barriers such as ageism. However, given the multifaceted nature of ageism, it is essential to consider not only its direct effects but also its indirect pathways.43,86 A holistic curricular approach should take these complex interplays into account to effectively support students’ career motivation. This nuanced perspective is discussed in the following subsection.
Discussion for RQ3: Holistic Approach to Enhancing CMGN by Addressing Ageism
Although prior research has established ageism as a significant barrier to nursing students’ willingness to care for older adults, relatively little attention has been paid to the mechanisms through which it exerts indirect influence. This study contributes to the literature by identifying two distinct mediation pathways: a sequential pathway involving contact quality and expectancy, and a parallel pathway with gratitude as the mediator.
In the sequential pathway, higher levels of ageism were associated with diminished intergenerational contact quality, which in turn lowered students’ expectancy of success in gerontological nursing and, ultimately, their valuation of a career in this field. While prior studies have demonstrated individual links—such as the negative association between ageism and contact quality, and the predictive role of contact quality in students’ willingness to care for older adults—this study is among the few to investigate the full sequential mediation pathway, grounded in both Allport’s contact theory and expectancy-value theory.6,13,14,20,44,50,52
To foster students’ expectancy and confidence in gerontological nursing—and simultaneously promote high-quality, meaningful intergenerational contact—curricula, particularly at the pre-clinical stage, should prioritize training in interpersonal communication and relational competencies. Recent research has found that newly graduated nurses who reported difficulties communicating with neurocognitively impaired older adults are more prone to displaying hostile forms of ageism, highlighting the need for greater communication preparedness.87 Earlier literature also underscores the value of training in interpersonal competencies—such as storytelling and narrative competence—which have been shown to enhance empathy and lead to more positive clinical experiences in gerontological settings.88–90 To develop these skills, educators can incorporate active learning strategies such as debates, case studies, role-playing, reflective writing, and reminiscing interviews focused on aging-related themes.82,85,91
The second pathway highlights the mediating role of gratitude between ageism and the perceived value of gerontological nursing. While prior research has recognized gratitude as a resource that fosters prosocial behavior and helps counteract ageism, its specific function as a mediator between ageism and career motivation remains underexplored.18,19,46 The current findings offer empirical support for conceptualizing gratitude as a promising target for educational intervention.
Notably, despite gratitude’s significant mediating role in SEM, it did not emerge as a direct predictor of either CMGN subscale in the earlier multivariate regression analysis. Given that gratitude showed small-to-moderate, yet significant, bivariate correlations with both Expectancy and Value, its lack of significance in the regression model likely reflects shared variance with other predictors, which may have attenuated its unique contribution.
These findings suggest that the role of gratitude should be considered within a broader constellation of interconnected psychological and relational mechanisms. From an educational psychology perspective, nursing educators are encouraged to incorporate gratitude-focused interventions into comprehensive curricular strategies aimed at reducing ageism and enhancing students’ CMGN. Evidence-based approaches include structured gratitude courses, gratitude journaling, and reflective assignments that encourage emotional engagement and self-awareness.92–94 Within the Chinese cultural context, interventions that emphasize filial values—alongside enhanced faculty support to fulfill students’ psychological needs for autonomy, competence, and relatedness—may further strengthen the impact of gratitude-based learning and better prepare students to combat ageism.18,95
Finally and crucially, our mediation analysis revealed that the direct negative effect of ageism on CMGN-Value remained statistically significant and substantial, even after accounting for indirect effects. This finding underscores the deep-rooted and multifaceted nature of ageism and reinforces the need for a holistic curriculum strategy. In this context, formal gerontological nursing education—comprising both theoretical instruction and practical training—plays an indispensable role. A substantial body of literature consistently affirms its positive impact on students’ CMGN as well as its protective effect against ageism.5,11,14,21,22,35,36,69,87,96,97 Educators should thoughtfully integrate those targeted interventions into, and deliver them alongside, this pedagogical foundation to enhance coherence and educational effectiveness.
Drawing on the above discussion, we propose that a robust curriculum designed to enhance CMGN should include:
- Comprehensive theoretical and clinical instruction in gerontological nursing, ensuring knowledge depth and skills readiness;
- Systematic anti-ageism education embedded across core and elective courses;
- Gratitude-promoting and empathy-building interventions using experiential and reflective pedagogies;
- Pre-clinical interpersonal communication training tailored specifically to geriatric care contexts.
Limitations
This study has several limitations. First, the use of a convenience sample from a single medical university limits the generalizability of the findings to broader populations across different regions or cultural contexts. Second, the cross-sectional design restricts the ability to draw causal inferences. Third, reliance on self-reported data may have introduced social desirability bias, as participants may have tailored their responses to align with perceived social expectations. Fourth, the survey did not include response quality screening items (eg, attention checks or logic traps), which limited the ability to detect low-quality responses. Fifth, academic track information (ie, bachelor’s vs diploma) was not collected, preventing analysis of potential differences in career motivation or related experiences across program types. This reduced the granularity of the analysis and may have introduced unmeasured heterogeneity. Finally, the structural equation model demonstrated only moderate fit, indicating room for improvement in model specification or the potential benefit of a larger and more diverse sample.
Future Research
Future research could consider employing longitudinal designs to better capture temporal changes in CMGN across nursing students’ academic trajectories, along with the evolving influence of associated factors. While longitudinal studies remain limited, existing work—such as that by Chai et al.—has largely concentrated on clinical practice periods.11 Expanding this approach to track students from their freshman year through post-clinical training would provide a more comprehensive understanding of how relationships between key predictors (eg, ageism, empathy) and CMGN evolve during critical educational transitions, such as early exposure to gerontology coursework or late-stage internships.
Additionally, collecting academic track information (ie, bachelor’s vs diploma) would allow researchers to assess whether program-level differences influence students’ motivation. Including diverse samples—such as comparisons between urban and rural regions or cross-national contexts—would further enhance the nuance and generalizability of findings. To mitigate self-report bias and improve data quality, future studies could incorporate quality screening items and adopt mixed-method approaches combining surveys with observational or third-party assessments.
Further research is also needed to evaluate how specific structural components of gerontological nursing education influence CMGN. For instance, investigations could examine the impact of targeted curricular modules and innovative pedagogies. Moreover, the effectiveness of practical training in diverse care settings—such as community-based clinics and long-term care facilities—should be systematically assessed for their role in fostering students’ commitment to gerontological nursing. By identifying the most effective educational strategies, future research can support the development of evidence-based curricula that promote sustainable interest and readiness for careers in gerontological nursing.
Conclusion
This study investigated the psychological and socio-demographic factors influencing nursing students’ career motivation toward gerontological nursing (CMGN) in the post-pandemic context. Special attention was given to how ageism exerts its influence, guided by expectancy-value theory and Allport’s contact theory.
Findings from a sequential-parallel mediation model revealed that ageism is a multifaceted barrier to CMGN—particularly to students’ perceived value of the career—operating through both direct and indirect pathways. In the sequential pathway, higher levels of ageism were associated with lower-quality intergenerational contact, which in turn diminished students’ expectancy beliefs about their potential success in gerontological nursing and ultimately reduced their perceived career value. In the parallel pathway, reduced gratitude mediated the relationship between ageism and career valuation. Together, these mechanisms illustrate how relational and emotional processes channel the negative effects of ageism on CMGN.
Additionally, empathy, intergenerational contact quality, prior caregiving experience, and exposure to gerontological nursing education emerged as consistent positive predictors of CMGN, emphasizing the importance of early, relational, and experience-based interventions.
These findings highlight key leverage points for intervention. Nursing curricula should incorporate both theoretical and practical instruction in gerontological nursing; embed anti-ageism content across courses; apply experiential and reflective pedagogies to cultivate empathy and gratitude; and provide interpersonal communication training specifically tailored to geriatric care settings.
Publication
The authors affirm that this manuscript is an original work and has not been published previously, in whole or in part, nor is it currently under consideration for publication elsewhere. No portion of the data, analysis, or findings has been published or is under review in any other journal, conference proceeding, or academic outlet. All relevant prior studies have been appropriately cited.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to extend their sincere gratitude to all the students who participated in the survey, as well as to the staff who assisted in distributing the questionnaire.
Generative AI tools, including ChatGPT-4o and DeepSeek-V3, were used under the authors’ direction to enhance the language of the manuscript. These tools were employed exclusively for language editing; all ideas, analyses, and interpretations are the original work of the authors. The use of AI tools fully complies with the Taylor & Francis policy on generative AI, and the authors take full responsibility for the integrity and content of the final manuscript.
Funding
This research was funded by the Doctoral Research Fund of Jiangxi Science and Technology Normal University, Grant Number: 2021BSQD06.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Aging. Available from: https://www.who.int/health-topics/ageing#tab=tab_1.
2. WHO. Ageing and health. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
3. Buchan J, Catton H. Recover to rebuild: investing in the nursing workforce for health system effectiveness. International Council of Nurses. https://www.icn.ch/sites/default/files/2023-07/ICN_Recover-to-Rebuild_report_EN.pdf.
4. Cheng H-L, Lam SC, Cruz JP, et al. Willingness to care for older people and associated factors in pre-registered student nurses: a multi-country survey study. Nurs Educ Today. 2022;110(1):1–7. doi:10.1016/j.nedt.2022.105279
5. Dai F, Liu Y, Ju M, Yang Y. Nursing students’ willingness to work in geriatric care: an integrative review. Nurs Open. 2021;8(5):2061–2077. doi:10.1002/nop2.726
6. Gherman M-A, Arhiri L, Holman AC. Ageism, moral sensitivity and nursing students’ intentions to work with older people – a cross-sectional study. Nurse Educ Today. 2022;113:1–44. doi:10.1016/j.nedt.2022.105372
7. Hsu P-T, Chen -J-J, Ho Y-F. The effects of narrative pedagogy on increasing nursing students’ willingness to practice older people care: a mixed-methods research. Nurse Educa Prac. 2022;62(1):1–7. doi:10.1016/j.nepr.2022.103356
8. Zubeldia-Etxeberria J, Pereda-Goikoetxea B, Elordi-Güenaga U, et al. What motivates students to pursue a career in gerontological nursing? The cultural adaptation and validation of the Spanish version of the CMGN questionnaire. Heliyon. 2024;10(7):e28477. doi:10.1016/j.heliyon.2024.e28477
9. Gallo V. Ageism in nursing education: a review of the literature. Teach Learn Nurs. 2019;14(3):208–215. doi:10.1016/j.teln.2019.04.004
10. Won J, Jang H. Factors influencing elderly care Willingness of nursing students. Inter J Adv Culture Technol. 2020;8(4):306–317. doi:10.17703/IJACT.2020.8.4.306
11. Chai X, Cheng C, Mei J, Fan X. Student nurses’ career motivation toward gerontological nursing: a longitudinal study. Nurse Educ Today. 2019;76:165–171. doi:10.1016/j.nedt.2019.01.028
12. Jang I, Kim Y, Kim Y. Nursing students’ Willingness to care for older adults. Inter J Soc Sci Stud. 2019;7(1):1–9. doi:10.11114/IJSSS.V7I1.3726
13. Cheng M, Cheng C, Tian Y, Fan X. Student nurses’ motivation to choose gerontological nursing as a career in China: a survey study. Nurse Educ Today. 2015;35(7):843–848. doi:10.1016/j.nedt.2015.03.001
14. Bergman EJ, Erickson MA, Simons JN. Attracting and training tomorrow’s gerontologists: what drives student interest in aging? Educ Gerontol. 2014;40(3):172–185. doi:10.1080/03601277.2013.802184
15. Guo Y, Yang L, Zhu L, Wan Y, Zhang S, Zhang J. Willingness and associated factors of working with older people among undergraduate nursing students in China: a cross-sectional study. BMC Nurs. 2021;20(1):113. doi:10.1186/s12912-021-00639-7
16. Che CC, Chong MC, Hairi NN. What influences student nurses’ intention to work with older people? A cross-sectional study. Inter J Nurs Stud. 2018;85:61–67. doi:10.1016/j.ijnurstu.2018.05.007
17. Fu Y, Zhang J, Cao L, et al. Nursing students’ attitudes and associated factors towards older people in Heilongjiang Province, northern China: a cross‐sectional study. Nurs Open. 2022;9(5):2454–2460. doi:10.1002/nop2.1262
18. Zhang S, Liu Y-H, Zhang H-F, Meng L-N, Liu P-X. Determinants of undergraduate nursing students’ care willingness towards the elderly in China: attitudes, gratitude and knowledge. Nurse Educ Today. 2016;43(1):28–33. doi:10.1016/j.nedt.2016.04.021
19. Calleja P, Knight-Davidson P, McVicar A, Laker C, Yu S, Roszak-Burton L. Gratitude interventions to improve wellbeing and resilience of graduate nurses transitioning to practice: a scoping review. Inter J Nurs Stud Adv. 2024;6:100188. doi:10.1016/j.ijnsa.2024.100188
20. Eshbaugh EM, Gross PE, Satrom T. Predictors of self-reported likelihood of working with older adults. Educ Gerontol. 2010;36(4):312–329. doi:10.1080/03601270903058481
21. Yan Z, Chang H-C, Montayre J, Ho M-H. How does geriatric nursing education program change the knowledge, attitude and working intention among undergraduate nursing students? A systematic literature review. Nurse Educ Today. 2022;108:105161. doi:10.1016/j.nedt.2021.105161
22. Shen J, Xiao LD. Factors affecting nursing students’ intention to work with older people in China. Nurse Educ Today. 2012;32(3):219–223. doi:10.1016/j.nedt.2011.03.016
23. Wang Y, Yang J, Wang L, et al. Nursing students’ motivation for choosing a career in geriatric nursing: a cross-sectional study. Educ Gerontol. 2024:1–10. doi:10.1080/03601277.2024.2328892.
24. Chi M-J, Shyu M-L, Wang S-Y, Chuang H-C, Chuang Y-H. Nursing students’ Willingness to care for older adults in Taiwan. J Nurs Scholar. 2016;48(2):172–178. doi:10.1111/jnu.12197
25. Mooney TB, Williams JN. The Confucian Filial Duty to Care (xiao) for Elderly Parents. In: Tālivaldis Ozoliņš J, editor. Religion and Culture in Dialogue: East and West Perspectives. Springer International Publishing; 2016:111–127.
26. Ho DYF. Filial piety scale and traditional Chinese values. In: Krägeloh CU, Alyami M, Medvedev ON, editors. International Handbook of Behavioral Health Assessment. Springer International Publishing; 2023:1–29.
27. Zhao L. China’s aging population: a review of living arrangement, intergenerational support, and wellbeing. Health Care Science. 2023;2(5):317–327. doi:10.1002/hcs2.64
28. Wang Z, Ngok K. Non-coresidential intergenerational relations from the perspective of adult children in China: typology and social welfare implications. Human Soc Sci Commun. 2024;11(1):552. doi:10.1057/s41599-024-03028-y
29. Liu X, Yu H-J, Zhang M-Z, et al. The transition of eldercare responsibility and traditional filial piety concepts and its urban-rural differences in China: an age-period-cohort analysis from 2006 to 2017. BMC Public Health. 2024;24(1):1669. doi:10.1186/s12889-024-19175-5
30. Wang J, Wang X. Urbanization, female employment, and family care choice. J Chin Sociol. 2024;11(1):14. doi:10.1186/s40711-024-00214-y
31. Zhang M, Cheng Q. Becoming a self-reliant elder: fading intergenerational reciprocity and pursuing active aging among middle-class seniors in urban China. SAGE Open. 2024;14(2):21582440241259161. doi:10.1177/21582440241259161
32. Pang R, Liu F, Li T. Professional values, ageism, attitudes and willingness towards geriatric care among nursing students in China: a multiple path analysis. BMC Nursing. 2025;24(1):162. doi:10.1186/s12912-025-02815-5
33. Zhang Y, Wang J, Zu Y, Hu Q. Attitudes of Chinese college students toward aging and living independently in the context of China’s modernization: a qualitative study. Front Psychol. 2021;12:609736. doi:10.3389/fpsyg.2021.609736
34. Han Y, Sun T. From ageism to respectful ageism: how is the China-specific phenomenon formed? J Chin Soci. 2025;12(1):9. doi:10.1186/s40711-025-00237-z
35. Hovey S, Dyck MJ, Reese C, Kim M. Nursing students’ attitudes toward persons who are aged: an integrative review. Nurse Educ Today. 2017;49(1):145–152. doi:10.1016/j.nedt.2016.11.018
36. Algoso M, Peters K, Ramjan L, East L. Exploring undergraduate nursing students’ perceptions of working in aged care settings: a review of the literature. Nurse Educ Today. 2016;36(1):275–280. doi:10.1016/j.nedt.2015.08.001
37. Wu B. Social isolation and loneliness among older adults in the context of COVID-19: a global challenge. Global Health Res Policy. 2020;5(1):27. doi:10.1186/s41256-020-00154-3
38. Webb LM, Chen CY. The COVID-19 pandemic’s impact on older adults’ mental health: contributing factors, coping strategies, and opportunities for improvement. Int J Geriatr Psychiatry. 2022;37(1). doi:10.1002/gps.5647
39. WHO. Supporting older people during the COVID-19 pandemic is everyone’s business. Available from: https://www.who.int/europe/news-room/03-04-2020-supporting-older-people-during-the-covid-19-pandemic-is-everyone-s-business.
40. Martin B, Kaminski-Ozturk N, O’Hara C, Smiley R. Examining the impact of the COVID-19 pandemic on burnout and stress among U.S. nurses. J Nurs Regulati. 2023;14(1):4–12. doi:10.1016/S2155-8256(23)00063-7
41. Fan J-Y, Zhao H-M, Liu Y-T, Kong -L-L, Mao J, Li J. Psychometric properties of a Chinese version of the Fraboni scale of ageism: evidence from medical students sample. BMC Med Educ. 2020;20(1):197. doi:10.1186/s12909-020-02111-7
42. Butler RN. Age-ism: another form of bigotry. Gerontologist. 1969;9(4):243–246. doi:10.1093/geront/9.4_Part_1.243
43. WHO. Global report on ageism. Available from: https://www.who.int/publications/i/item/9789240016866.
44. Allport GW. The Nature of Prejudice. Addison-Wesley Publishing; 1954.
45. Pettigrew TF, Tropp LR. A meta-analytic test of intergroup contact theory. J Personal Soc Psych. 2006;90(5):751–783. doi:10.1037/0022-3514.90.5.751
46. Allan LJ, Johnson JA, Emerson SD. The role of individual difference variables in ageism. Personal Indivi Differ. 2014;59(1):32–37. doi:10.1016/j.paid.2013.10.027
47. Hwang EH, Kim KH. Quality of gerontological nursing and ageism: what factors influence on nurses’ ageism in South Korea? Inter J Environ Res Public Health. 2021;18(1):4091. doi:10.3390/ijerph18084091
48. Burnes D, Sheppard C, Henderson CRJ, et al. Interventions to reduce ageism against older adults: a systematic review and meta-analysis. Ame J Public Health. 2019;109(8):e1–e9. doi:10.2105/AJPH.2019.305123
49. Cooney C, Minahan J, Siedlecki KL. Do feelings and knowledge about aging predict ageism? J Appl Gerontol. 2021;40(1):28–37. doi:10.1177/0733464819897526
50. Eccles JS, Wigfield A. In the mind of the actor: the structure of adolescents’ achievement task values and expectancy-related beliefs. Personal Soc Psycholog Bulletin. 1995;21(3):215–225. doi:10.1177/0146167295213003
51. Wigfield A, Eccles JS. Expectancy–value theory of achievement motivation. Contemp Educ Psych. 2000;25(1):68–81. doi:10.1006/ceps.1999.1015
52. Jang I, Oh D, Kim Y. Factors associated with nursing students’ willingness to care for older adults in Korea and the United States. Inter J Nurs Sci. 2019;6(1):426–431. doi:10.1016/j.ijnss.2019.09.004
53. McCullough ME, Emmons RA, Tsang J-A. The grateful disposition: a conceptual and empirical topography. J Personal Soc Psych. 2002;82(1):112–127. doi:10.1037//0022-3514.82.1.112
54. Brasher MS. Filial norms, altruism, and reciprocity: financial support to older parents in China. J Popul Ageing. 2022;15(1):259–277. doi:10.1007/s12062-020-09316-0
55. Moshagen M, Bader M. semPower: general power analysis for structural equation models. Behav Res Methods. 2024;56(4):2901–2922. doi:10.3758/s13428-023-02254-7
56. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equa Model. 1999;6(1):1–55. doi:10.1080/10705519909540118
57. MacCallum R, Browne M, Sugawara H. Power analysis and determination of sample size for covariance structure modeling. Psycholog Meth. 1996;1(2):130–149. doi:10.1037/1082-989X.1.2.130
58. Collier JE. Applied Structural Equation Modeling Using AMOS. Routledge; 2020.
59. Hair JF, Hult GTM, Ringle CM, Sarstedt M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM).
60. DeWees TA, Mazza GL, Golafshar MA, Dueck AC. Investigation into the effects of using normal distribution theory methodology for likert scale patient-reported outcome data from varying underlying distributions including floor/ceiling effects. Value in Health. 2020;23(5):625–631. doi:10.1016/j.jval.2020.01.007
61. Fraboni M, Saltstone R, Hughes S. The fraboni scale of ageism (FSA): an attempt at a more precise measure of ageism. Canad J Aging. 1990;9(1):56–66. doi:10.1017/S0714980800016093
62. Yan T, Silverstein M, Wilber KH. Does race/ethnicity affect aging anxiety in American baby boomers? Res Aging. 2011;33(4):361–378. doi:10.1177/0164027511403009
63. Wei C, Wu H-T, Kong X-N, Wang H-T. Revision of gratitude questionnaire −6 in Chinese adolescent and its validity and reliability. Chin J School Health. 2011;32(10):1201–1202. doi:10.16835/j.cnki.1000-9817.2011.10.016
64. Spreng RN, McKinnon MC, Mar RA, Levine B. The Toronto Empathy Questionnaire: scale development and initial validation of a factor-analytic solution to multiple empathy measures. J Personal Assess. 2009;91(1):62–71. doi:10.1080/00223890802484381
65. Barker G, Contreras JM, Heilman B, Singh AK, Verma RK, Nascimento M. evolving men: initial results from the international men and gender equality survey (IMAGES). 2011. Available from: https://www.equimundo.org/resources/evolving-men-initial-results-from-the-international-men-and-gender-equality-survey-images/.
66. Zeballos E, Anekwe TD. The association between nutrition information use and the healthfulness of food acquisitions. 2018. 2018. https://www.ers.usda.gov/publications/pub-details?pubid=88530.
67. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
68. Kline RB. Principles and Practice of Structural Equation Modeling (Fourth Edition). The Guilford Press; 2016.
69. Even-Zohar A, Werner S. The effect of educational interventions on willingness to work with older adults: a comparison of students of social work and health professions. J Gerontol Soc Work. 2020;63(1–2):114–132. doi:10.1080/01634372.2020.1712511
70. Brown J, Nolan M, Davies S, Nolan J, Keady J. Transforming students’ views of gerontological nursing: realising the potential of ‘enriched’ environments of learning and care: a multi-method longitudinal study. Inter J Nurs Stud. 2008;45(8):1214–1232. doi:10.1016/j.ijnurstu.2007.07.002
71. Duggan S, Mitchell EA, Moore KD. ‘With a bit of tweaking…we could be great’. An exploratory study of the perceptions of students on working with older people in a preregistration BSc (Hons) nursing course. Inter J Older People Nurs. 2013;8(3):207–215. doi:10.1111/j.1748-3743.2012.00317.x
72. Kydd A, Touhy T, Newman D, Fagerberg I, Engstrom G. Attitudes towards caring for older people in Scotland, Sweden and the United States. Nurs Older People. 2014;26(2):33–40. doi:10.7748/nop2014.02.26.2.33.e547
73. Birimoglu Okuyan C, Bilgili N, Mutlu A. Factors affecting nursing students’ intention to work as a geriatric nurse with older adults in Turkey: a cross-sectional study. Nurse Educ Today. 2020;95(1):1–6. doi:10.1016/j.nedt.2020.104563
74. Liu XL, Cheng HL, Lam SC. Predicting undergraduate nursing students’ willingness to care for older adults: a multicenter cross‐sectional study in Asia. Nurs Open. 2022;9(2):1402–1411. doi:10.1002/nop2.916
75. Boswell SS. “Old people are cranky”: helping professional trainees’ knowledge, attitudes, aging anxiety, and interest in working with older adults. Educ Gerontol. 2012;38(7):465–472. doi:10.1080/03601277.2011.559864
76. King BJ, Roberts TJ, Bowers BJ. Nursing student attitudes toward and preferences for working with older adults. Gerontol Geria Educ. 2013;34(3):272–291. doi:10.1080/02701960.2012.718012
77. Samra R, Griffiths A, Cox T, Conroy S, Knight A. Changes in medical student and doctor attitudes toward older adults after an intervention: a systematic review. J Ame Geria Soci. 2013;61(7):1188–1196. doi:10.1111/jgs.12312
78. Blais K, Mikolaj E, Jedlicka D, Strayer J, Stanek S. Innovative strategies for incorporating gerontology into BSN curricula. J Profess Nurs. 2006;22(2):98–102. doi:10.1016/j.profnurs.2006.01.006
79. Chonody JM. Addressing ageism in students: a systematic review of the pedagogical intervention literature. Educ Gerontol. 2015;41(12):859–887. doi:10.1080/03601277.2015.1059139
80. Nesje K. Nursing students’ prosocial motivation: does it predict professional commitment and involvement in the job? J Adv Nurs. 2015;71(1):115–125. doi:10.1111/jan.12456
81. Gholamzadeh S, Khastavaneh M, Khademian Z, Ghadakpour S. The effects of empathy skills training on nursing students’ empathy and attitudes toward elderly people. BMC Med Educ. 2018;18(1):198. doi:10.1186/s12909-018-1297-9
82. Henry BW, Ozier AD, Johnson A. Empathetic responses and attitudes about older adults: how experience with the aging game measures up. Educ Gerontol. 2011;37(10):924–941. doi:10.1080/03601277.2010.495540
83. Li Q, Noah A, Knight B. Empathy and ageism among college students in non-medical institutions: the mediating role of empathy. Educ Gerontol. 2023;49(2):109–120. doi:10.1080/03601277.2022.2073425
84. Schwartz LK, Simmons JP. Contact quality and attitudes toward the elderly. Educ Gerontol. 2001;27(2):127–137. doi:10.1080/03601270151075525
85. Gallagher P, Carey K. Connecting with the well-elderly through reminiscence: analysis of lived experience. Educ Gerontol. 2012;38(8):576–582. doi:10.1080/03601277.2011.595312
86. Levy SR, Lytle A, Macdonald J. The worldwide ageism crisis. J Soc Issues. 2022;78(4):743–768. doi:10.1111/josi.12568
87. Catalão MJ, Arco H, Carrajola N, Tavares J. Ageism among newly graduated nurses: the influence of sociodemographic variables and gerontogeriatric nursing education. Nurs Educ Prac. 2025;83:104285. doi:10.1016/j.nepr.2025.104285
88. Corbally M, Grant A. Narrative competence: a neglected area in undergraduate curricula. Nurse Educ Today. 2016;36:7–9. doi:10.1016/j.nedt.2015.09.004
89. Charon R. Narrative Medicine: Honoring the Stories of Illness. Oxford University Press; 2008.
90. McAllister M, Ryan C, Dodd L, Goldenberg M, Brien DL. A thematic literature review of innovative strategies to prepare nursing students for aged-care. Nurse Educ Today. 2020;87(1):1–6. doi:10.1016/j.nedt.2020.104355
91. Bhana VM. Interpersonal skills development in Generation Y student nurses: a literature review. Nurse Educ Today. 2014;34(12):1430–1434. doi:10.1016/j.nedt.2014.05.002
92. Hong J-E, Song M. The enhancing and intermediating effects of a gratitude course among nursing students. Inter J Adv Nurs Educ Res. 2020;5(1):37–42. doi:10.21742/IJANER.2020.5.1.05
93. Ko H, Kim S, Kim E. Nursing students’ experiences of gratitude journaling during the COVID-19 pandemic. Healthcare. 2021;9(11):1473. doi:10.3390/healthcare9111473
94. Fournier A, Sheehan C. Growing gratitude in undergraduate nursing students: applying findings from social and psychological domains to nursing education. Nurse Educ Today. 2015;35(12):1139–1141. doi:10.1016/j.nedt.2015.08.010
95. Jin G, Wang Y. The influence of gratitude on learning engagement among adolescents: the multiple mediating effects of teachers’ emotional support and students’ basic psychological needs. J Adolesc. 2019;77(1):21–31. doi:10.1016/j.adolescence.2019.09.006
96. Cerqueira AF, Ramos AL, Palma J. Ageism in nursing education: students’ views of ageing. Soc Sci. 2023;12(3):142. doi:10.3390/socsci12030142
97. Hsu MHK, Ling MH, Lui TL. Relationship between gerontological nursing education and attitude toward older people. Nurse Educ Today. 2019;74(1):85–90. doi:10.1016/j.nedt.2018.12.007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.