Back to Journals » Clinical Ophthalmology » Volume 20
Age-Related Differences in the Efficacy of Intense Pulsed Light Therapy for Meibomian Gland Dysfunction in Women
Authors Gotoda S ![]() , Sakai Y, Nishida T, Ichikawa K, Ichikawa K
, Sakai Y, Nishida T, Ichikawa K, Ichikawa K ![]()
Received 20 November 2025
Accepted for publication 16 January 2026
Published 21 January 2026 Volume 2026:20 583104
DOI https://doi.org/10.2147/OPTH.S583104
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Satoshi Gotoda,1 Yukihiro Sakai,1 Tomoya Nishida,1 Kei Ichikawa,1,2 Kazuo Ichikawa1
1Department of Ophthalmology, Chukyo Eye Clinic, Nagoya, Aichi, Japan; 2Department of Ophthalmology, Aoyama General Hospital, Toyokawa, Aichi, Japan
Correspondence: Satoshi Gotoda, Department of Ophthalmology, Chukyo Eye Clinic, 12-22 Sanbonmatsu-cho, Atsuta-ku, Nagoya, Aichi, 456-0032, Japan, Tel +81-52-883-1543, Email [email protected]
Purpose: Aging and hormonal factors influence meibomian gland dysfunction (MGD), which can be treated by intense pulsed light (IPL) therapy. However, the influence of age on treatment response remains unclear. This study aimed to investigate the impact of aging on the outcomes of IPL therapy among female patients with MGD.
Patients and Methods: Sixty-eight eyes of female patients who underwent four IPL treatment sessions were included. Patients were divided into two age groups: < 50 years (39.5 ± 10.2 years, n = 30) and ≥ 50 years (72.5 ± 9.49 years, n = 38). Parameters assessed before and after IPL included corneal and conjunctival staining score, fluorescein tear film break-up time (FBUT), lipid layer thickness (LLT), subjective symptoms (Standard Patient Evaluation of Eye Dryness [SPEED] score), and meibomian gland parameters (meibum quality, expressibility, and meiboscore). Statistical analyses were performed using the Mann–Whitney U and Wilcoxon signed-rank tests; p < 0.05 indicated statistical significance.
Results: At baseline, the younger group had lower LLT (p < 0.01) and poorer expressibility (p = 0.049) than did the older group, who showed worse corneal and conjunctival staining score (p = 0.04) and meiboscore (p < 0.01). After treatment, the younger group exhibited significant improvements in FBUT, LLT, meibum quality, expressibility, meiboscore, and SPEED scores, whereas the older group showed significant improvement in corneal and conjunctival staining scores, FBUT, expressibility, and SPEED scores. Between-group comparisons showed greater improvements in meibum quality and expressibility in the younger group (both p < 0.01), while improvement in corneal and conjunctival staining score was greater in the older group (p = 0.02).
Conclusion: IPL therapy improved MGD-related signs and symptoms in women of all ages. The observed age-related differences in the most responsive parameters suggest that age affects the therapeutic profile of IPL. These results may help guide age-appropriate MGD management.
Keywords: meibomian gland dysfunction, intense pulsed light, lipid layer thickness, standard patient evaluation of eye dryness score, age-related differences
Introduction
Meibomian gland dysfunction (MGD) is a leading cause of evaporative dry eye and is characterized by diffuse abnormalities in the quality and quantity of meibomian gland secretions, resulting in tear film instability, visual disturbance, and reduced quality of life.1 The underlying pathophysiology involves chronic inflammatory changes accompanied by ductal epithelial keratinization and altered meibum secretion, which have been systematically defined by the International Workshop on Meibomian Gland Dysfunction.2
Population-based studies in Japan have demonstrated that the prevalence of MGD increases with age, from approximately 5% in the 30s to 32% in the 50s, 50% in the 70s, and up to 63% in the 80s.3 Globally, a systematic review and meta-analysis estimated the overall prevalence to be approximately 35–36%.4 With the aging population and wider availability of diagnostic devices for dry eye disease, the number of patients with MGD is expected to continue rising. Current clinical practice guidelines recommend a stepwise approach, beginning with home-based care, such as warm compresses and lid hygiene, and escalating to in-office procedures as necessary.1
Intense pulsed light (IPL) therapy, initially developed for dermatologic indications such as rosacea and vascular lesions,5,6 has been adapted for MGD based on the involvement of eyelid telangiectasia and periocular inflammation. Clinical studies have reported that IPL therapy improves tear film stability, subjective symptoms, and ocular surface and meibomian gland findings in patients with MGD.7,8 In addition, reductions in tear inflammatory cytokine levels following IPL therapy have been demonstrated,9 and systematic reviews and meta-analyses have further supported its therapeutic efficacy.10–12
However, few studies have systematically investigated which clinical parameters and symptoms exhibit more pronounced changes between different age groups under a standardized IPL protocol. The underlying disease mechanisms may also differ by life stage: in younger individuals, contact lens wear and cosmetic residue may contribute to meibomian gland orifice obstruction and increased meibum viscosity,13–15 whereas in older women, age-related gland atrophy and postmenopausal hormonal changes are major etiologic factors.16,17 Based on these considerations, the present study aimed to compare pre- and post-treatment changes in young and older female patients with MGD who were treated with a standardized four-session IPL protocol and to identify the parameters that tend to show relatively greater improvement depending on age. The results are expected to be useful for designing age-appropriate strategies to optimize MGD management.
Materials and Methods
Study Design and Participants
This retrospective observational study included female patients diagnosed with MGD who completed four sessions of IPL therapy at Chukyo Eye Clinic between April 2023 and December 2024. A total of 68 eyes were analyzed. Patients were stratified into two age groups: those younger than 50 years (U group; mean age, 39.5 ± 10.2 years; n = 30) and those aged 50 years or older (O group; mean age, 72.5 ± 9.5 years; n = 38). The age threshold of 50 years was selected to represent a clinically meaningful transition phase that approximately corresponds to the menopausal phase in women, which is characterized by substantial hormonal changes that influence meibomian gland morphology and secretory function.
Exclusion criteria included pregnancy or lactation, photosensitivity, keloid predisposition, a history of epilepsy, or any condition deemed unsuitable for IPL therapy by the attending physician. This study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Chukyo Eye Clinic (approval number: 20250328092). Because this study was retrospective, we adopted an opt-out approach approved by the ethics committee of Chukyo Eye Clinic instead of obtaining written informed consent.
Diagnosis and Evaluation Parameters
The primary outcome measures were ocular surface epithelial staining, meibomian gland function (meibum quality, expressibility, and meiboscore), lipid layer thickness (LLT), and subjective symptoms.
The diagnosis of MGD was based on the Japanese MGD Clinical Practice Guidelines,1 which define MGD as the presence of ocular discomfort (such as foreign body sensation or tearing) with abnormal lid margin morphology and qualitative or quantitative abnormalities in meibomian gland secretion. All evaluations were performed before treatment and one month after the fourth IPL session by the same corneal specialist (S.G.) using slit-lamp biomicroscopy. Corneal and conjunctival staining was graded using the modified Oxford scale.18,19 Meibomian gland function was assessed by grading meibum quality (0 = clear, 1 = cloudy, 2 = cloudy with particulate matter, 3 = toothpaste-like) and expressibility (1 = easy, 2 = moderate, 3 = hard).19 Meibomian gland dropout was evaluated using the meiboscore obtained from lower-lid meibography (0 = no loss; 1 = <1/3 loss; 2 = 1/3–2/3 loss; 3 = >2/3 loss).20 LLT was measured using a non-contact interferometric method with the IDRA® ocular surface analyzer (SBM Sistemi Srl, Trino, Italy). Subjective symptoms were evaluated using the Standard Patient Evaluation of Eye Dryness (SPEED) questionnaire.21
IPL Protocol and Adjunctive Care
IPL treatment was performed using the M22 system (Lumenis Be Ltd., Yokneam, Israel) equipped with a 590-nm filter and a fluence of 12 J/cm2. The treatment sequence consisted of 13 shots per pass applied vertically to the following areas: temple → cheek → below lower eyelid → nasal area → contralateral temple (Figure 1). Two passes were administered to the skin surface, followed immediately by in-office meibomian gland expression. Each IPL session was defined as one treatment set, and four sessions were performed at approximately 4-week intervals, according to the Toyos protocol.8
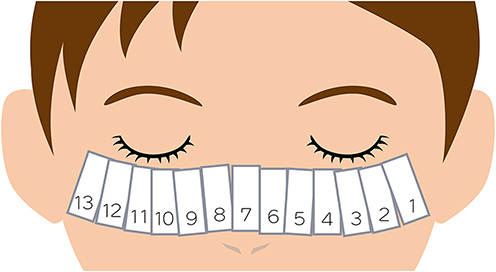 |
Figure 1 Clinical protocol for intense pulsed light therapy showing the treatment area and sequence. Abbreviation: MGD, meibomian gland dysfunction. |
All patients were receiving IPL therapy for the first time at our institution. At baseline, the patients may have been using topical treatments for meibomian gland dysfunction as part of routine clinical care. During the study period, these concomitant topical treatments were continued as clinically indicated and were not considered part of the primary intervention in this study. Therefore, they were not standardized or systematically recorded for the purpose of this analysis.
All patients were instructed to continue standardized home-based care, including warm compresses and lid hygiene, which are also recommended as first-line interventions (Step 1) in accordance with the Tear Film and Ocular Surface Society Dry Eye Workshop II (TFOS DEWS II) report and the updated TFOS DEWS III Management and Therapy report.22–24 Although patients were expected to follow these instructions, adherence to home-based care was not objectively assessed.
Given the study design, residual confounding related to baseline disease severity and concomitant treatments could not be entirely excluded.
Statistical Analysis
Normality of data distribution was assessed using the Shapiro–Wilk test, and non-parametric tests were applied accordingly. Between-group comparisons were performed using the Mann–Whitney U-test, and within-group pre- and post-treatment comparisons were performed using the Wilcoxon signed-rank test. A two-tailed p value of <0.05 indicated statistical significance. All analyses were conducted using EZR version 1.68 (Jichi Medical University, Tochigi, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). EZR is a modified version of R Commander designed to provide statistical functions frequently used in biostatistics.25
Results
Baseline Characteristics
Among the 68 eyes included in the analysis, 30 were in the U group and 38 in the O group. The O group was significantly older (p < 0.01). At baseline, the U group showed lower LLT and poorer meibum expressibility (p = 0.049), whereas the O group exhibited worse corneal and conjunctival staining score and higher meiboscore (p = 0.04 and p < 0.01, respectively). No significant between-group differences were observed in FBUT, meibum quality, or SPEED score (Table 1).
 |
Table 1 Baseline Characteristics of Female Patients with Meibomian Gland Dysfunction Before Intense Pulsed Light |
Tear Film Parameters
Corneal and conjunctival staining score decreased from 0.13 to 0.03 in the U group (p = 0.15) and from 0.74 to 0.21 in the O group (p < 0.01) (Table 2 and Figure 2). The change in corneal and conjunctival staining score (Δ Corneal and conjunctival staining score) was significantly greater in the O group (Table 3; −0.52 vs −0.10, p = 0.02). FBUT increased significantly in both groups (Table 2 and Figure 2; U group: 3.47 → 5.17 s, p < 0.01; O group: 3.68 → 5.05 s, p < 0.01), with no significant difference in the magnitude of improvement between groups (Table 3; +1.70 s vs +1.37 s, p = 0.37). LLT significantly increased in the U group (Table 2 and Figure 2; 57.2 → 64.5 nm, p = 0.04) and showed a non-significant upward trend in the O group (Table 2 and Figure 2; 68.0 → 70.5 nm, p = 0.23). The change in LLT (ΔLLT) did not differ significantly between groups (Table 3; +7.30 nm vs +2.47 nm, p = 0.28).
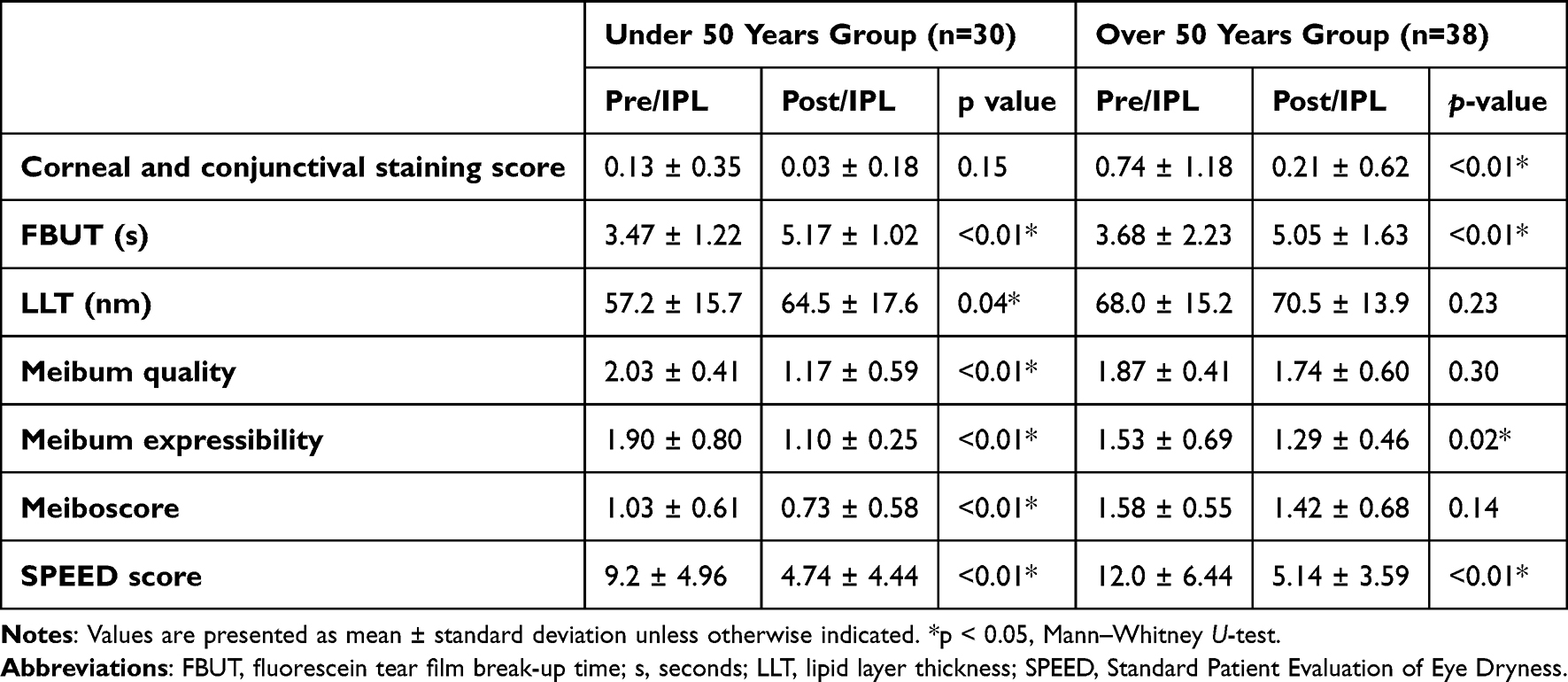 |
Table 2 Pre- and Post-Treatment Changes in Ocular Surface, Meibomian Gland, and Tear Film Parameters by Age Group After Intense Pulsed Light |
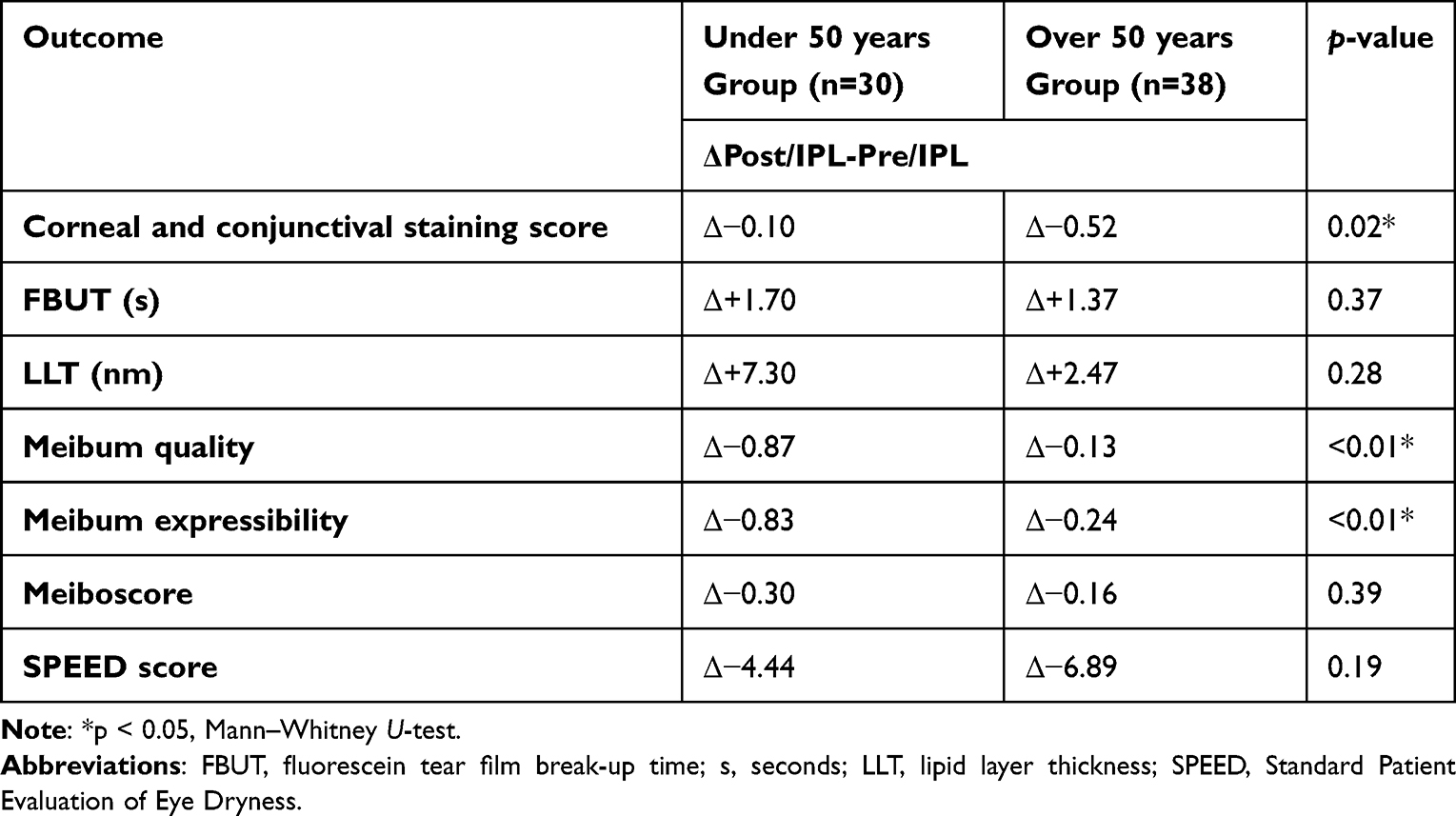 |
Table 3 Comparison of Age-Related Differences in Changes in Ocular Surface, Meibomian Gland, and Tear Film Parameters After Intense Pulsed Light |
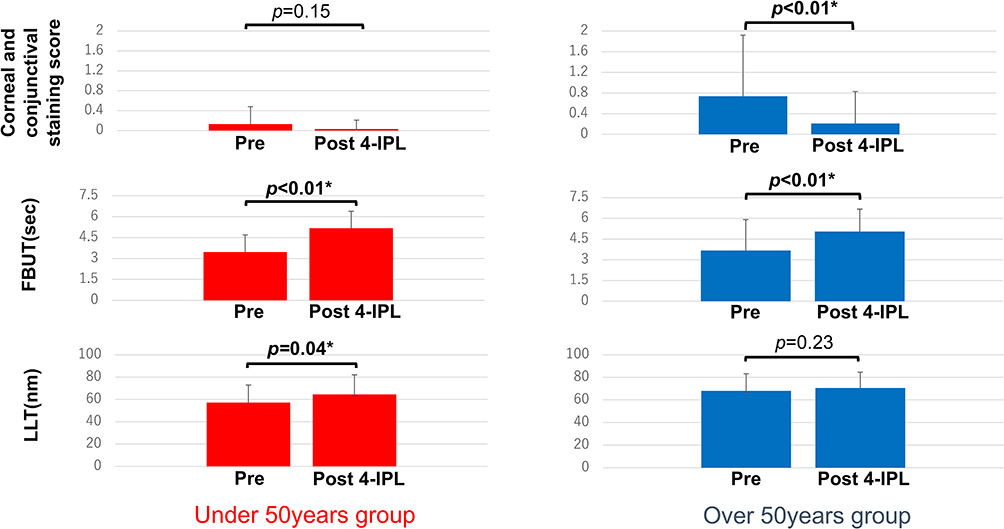 |
Figure 2 Changes in corneal and conjunctival staining score, fluorescein tear film break-up time, and lipid layer thickness. Patients are stratified into two age groups: those younger than 50 years (n = 30) and those aged 50 years or older (n = 38). Data are presented as mean ± standard deviation. Error bars represent standard deviations. Within-group comparisons have been performed using the Wilcoxon signed-rank test. *p < 0.05; Bold values indicate statistically significant changes within each group. |
Changes in Meibomian Gland Function and Morphology
Meibum quality improved significantly in the U group (Table 2 and Figure 3; 2.03 → 1.17, p < 0.01), whereas the O group showed a non-significant numerical improvement (Table 2 and Figure 3; 1.87 → 1.74, p = 0.30). Meibum expressibility improved in both groups (Table 2 and Figure 3; U group: 1.90 → 1.07, p < 0.01; O group: 1.53 → 1.29, p = 0.02).
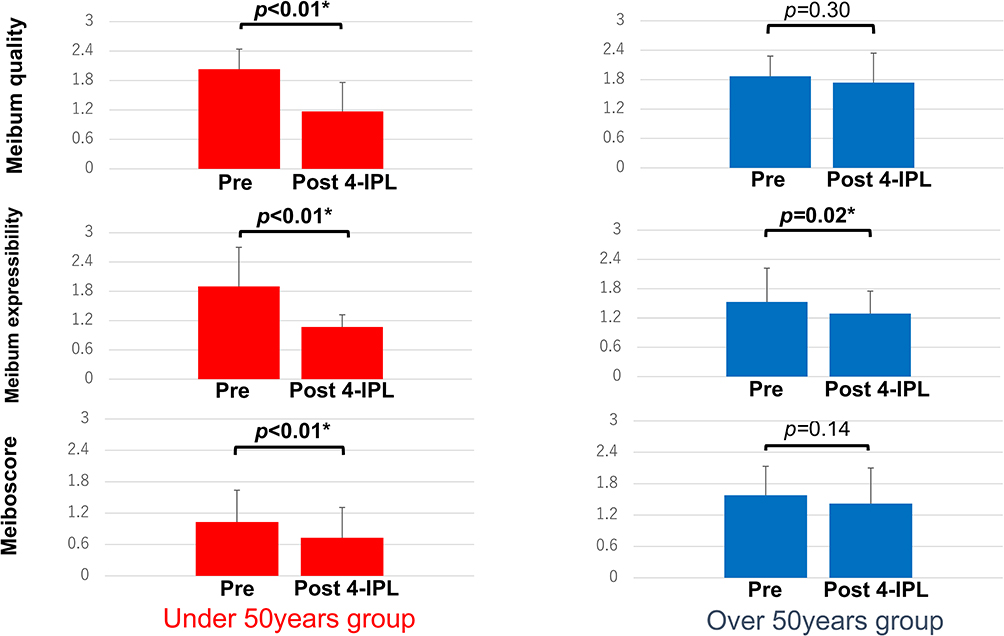 |
Figure 3 Changes in meibum quality, expressibility, and meiboscore. Patients are stratified into two age groups: those younger than 50 years (n = 30) and those aged 50 years or older (n = 38). Data are presented as mean ± standard deviation. Error bars represent standard deviations. Within-group comparisons have been performed using the Wilcoxon signed-rank test. *p < 0.05; Bold values indicate statistically significant changes within each group. |
Between-group comparison of change magnitude showed greater improvement in the U group than in the O group for both meibum quality (Δ−0.87 vs −0.13, p < 0.01) and expressibility (Δ−0.83 vs −0.24, p < 0.01). Meiboscore decreased significantly in the U group (Table 2 and Figure 3; 1.03 → 0.73, p < 0.01) and showed a non-significant decrease in the O group (Table 2 and Figure 3; 1.58 → 1.42, p = 0.14). The change in meiboscore did not differ significantly between the U and O groups (Table 3; Δ−0.30 vs −0.16, p = 0.39).
Changes in Subjective Symptoms
SPEED scores improved significantly in both groups (Table 2 and Figure 4; U group: 9.2 → 4.74; O group: 12.0 → 5.14; both p < 0.01). No significant difference was found in the change magnitude between the U and O groups (Table 3; Δ−4.44 vs −6.89, p = 0.19).
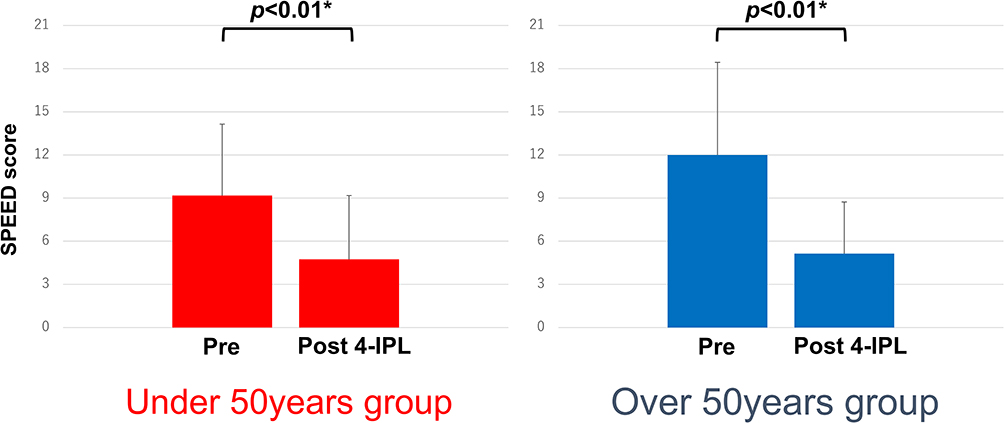 |
Figure 4 Changes in Standard Patient Evaluation of Eye Dryness score. Patients are stratified into two age groups: those younger than 50 years (n = 30) and those aged 50 years or older (n = 38). Data are presented as mean ± standard deviation. Error bars represent standard deviations. Within-group comparisons have been performed using the Wilcoxon signed-rank test. *p < 0.05; Bold values indicate statistically significant changes within each group. |
Safety
No intraoperative or postoperative complications were observed in any patients during or after the IPL treatment.
Discussion
This study applied a standardized four-session IPL protocol and examined pre- and post-treatment changes in female patients with MGD, stratified by age. The main findings were as follows: (1) FBUT significantly increased and SPEED scores decreased consistently in both age groups; (2) improvements in LLT and meibum function (quality and expressibility) were relatively greater in the U group than in the O group, although the O group also showed a significant improvement in expressibility; (3) corneal and conjunctival staining score improved more prominently in the O group than in the U group, while a decreasing trend was also observed in the U group. Furthermore, inter-individual variability was noted—some younger patients exhibited marked epithelial staining, whereas some older patients maintained favorable meiboscores. Collectively, these results indicate that while the IPL therapy led to multifaceted improvement across all age groups, the specific parameters showing the greatest relative change may differ with age.
These findings are consistent with the pathophysiologic differences associated with life stage. In younger patients, meibomian gland obstruction and increased meibum viscosity are thought to result from contact lens wear and residual cosmetic materials.13–15 This observation is consistent with the baseline characteristics in our study, including lower LLT and poorer expressibility in the U group, together with their substantial post-treatment improvement in meibum function and LLT. The IPL therapy can soften inspissated meibum and reduce peri-glandular telangiectasia and inflammation,7–12 thereby facilitating lipid outflow and enhancing the lipid layer. The resultant reinforcement of the tear film lipid layer reduces evaporation and delays tear film thinning,26,27 providing a physiologic basis for the observed FBUT prolongation in both groups.
The observed decrease in the meiboscore, particularly for younger patients, should be interpreted with caution, given the relatively short follow-up period. This change may reflect functional improvement or enhanced visualization of the meibomian glands after treatment rather than true structural gland regeneration.
In older patients, age-related atrophy of the meibomian glands and postmenopausal hormonal changes contribute to reduced lipid secretion and increased ocular surface inflammation.16,17 In the present study, the O group exhibited worse baseline meiboscore and corneal and conjunctival staining score. Although short-term structural recovery of atrophic glands is unlikely,16 the anti-vascular and anti-inflammatory effects of IPL6,9 may promote epithelial healing, accounting for the greater reduction in corneal and conjunctival staining observed in this group.
Symptom improvement was significant in the U and O groups in this study. Previous studies have demonstrated that the SPEED questionnaire provides high clinical utility and sensitivity, showing significant correlations with corneal and conjunctival staining and meibomian gland function indices.21 Although objective findings and subjective symptoms in ocular surface disease do not always align perfectly, the parallel improvements in FBUT (in the U and O groups), meibomian gland function (particularly in the U group), corneal and conjunctival staining score (particularly in the O group), and SPEED scores (in the U and O groups) observed in this study are consistent with findings from previous randomized double-masked placebo-controlled trials,28 prospective randomized studies,29 and multicenter prospective investigations.19
Regarding safety, no adverse events were observed in this study. Previous reports—including those involving direct eyelid application and combined meibomian gland expression—have described only transient sensations of heat or mild discomfort, with no serious adverse effects.9,30 Systematic reviews and meta-analyses also support the rarity of severe complications,9–11 and the procedure is generally considered safe when appropriate indications, shielding, and skin protection are followed.
This study has several limitations. It was a retrospective, single-center study, and the findings are limited to female participants; therefore, generalization to male patients should be made with caution. Concomitant in-office or at-home therapies (such as eye drops and adherence to lid hygiene) were not strictly controlled. The observation period was limited to one month after the fourth IPL session, and long-term durability of the effects remains to be verified. In particular, the persistence of changes in structural parameters such as the meiboscore and the durability of the observed age-related differences over a longer follow-up period remain unclear. Nevertheless, despite these limitations, the identification of age-related trends in relative parameter changes, the consistent multi-parameter improvements, and the absence of adverse events all strengthen the evidence supporting the efficacy and safety of the IPL therapy in women with MGD. Future studies with larger, sex-inclusive cohorts and longer follow-up periods are warranted to validate these findings and further clarify the influence of age on the therapeutic response to IPL.
Conclusions
The IPL therapy improved tear film stability and subjective symptoms in female patients with MGD across all ages. Younger patients showed greater improvement in meibomian gland function; in contrast, older patients demonstrated more pronounced reduction in corneal and conjunctival staining. Although the specific parameters with the most prominent relative changes differed by age, both the U and O groups experienced multifaceted benefits. These findings indicate that IPL is a useful and safe therapeutic option for women with MGD regardless of age.
Future studies with larger, sex-inclusive cohorts and longer follow-up periods are warranted to further elucidate age-related differences in the treatment response and determine the long-term durability of IPL therapy.
Abbreviations
MGD, meibomian gland dysfunction; IPL, intense pulsed light; FBUT, fluorescein tear film break-up time; LLT, lipid layer thickness; SPEED, Standard Patient Evaluation of Eye Dryness; TFOS DEWS II, Tear Film and Ocular Surface Society Dry Eye Workshop II.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study adhered to the tenets of the Declaration of Helsinki and was approved by the ethics committee of Chukyo Eye Clinic (approval number: 20250328092). Because this study was retrospective, an opt-out approach approved by the ethics committee was used instead of acquisition of written informed consent.
Acknowledgments
The authors would like to acknowledge Yui Morioka for her support of this study.
Author Contributions
All authors made a significant contribution to the work reported, including conception; study design; execution; acquisition, analysis, and interpretation of data; or all these areas. They also took part in drafting, revision, or critical review of the article. All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
Dr Satoshi Gotoda reports personal fees from Lumenis Be Ltd., Santen Pharmaceutical Co., Ltd., Senju Pharmaceutical Co., Ltd., Tomey Corporation, outside the submitted work. Dr Kazuo Ichikawa reports grants and/or personal fees from STAAR Surgical, Alcon, Kowa company Co. Ltd., Wakamoto Pharmaceutical Co., LTD., and Lumenis Japan Co. Ltd.; non-financial support for provision of equipment from Rxsight, outside the submitted work. The authors declare no other conflicts of interest in this work.
References
1. Amano S, Shimazaki J, Yokoi N, Hori Y, Arita R.; Committee for Meibomian Gland Dysfunction Clinical Practice Guidelines. Meibomian gland dysfunction clinical practice guidelines. Jpn J Ophthalmol. 2023;67(4):448–10. doi:10.1007/s10384-023-00995-8
2. Nichols KK, Foulks GN, Bron AJ, et al. The international workshop on meibomian gland dysfunction: executive summary. Invest Ophthalmol Vis Sci. 2011;52(4):1922–1929. doi:10.1167/iovs.10-6997a
3. Arita R, Mizoguchi T, Kawashima M, et al. Meibomian gland dysfunction and dry eye are similar but different based on a population-based study: the Hirado–Takushima study in Japan. Am J Ophthalmol. 2019;207:410–418. doi:10.1016/j.ajo.2019.02.024
4. Hassanzadeh S, Varmaghani M, Zarei-Ghanavati S, Heravian Shandiz J, Azimi Khorasani A. Global prevalence of Meibomian gland dysfunction: a systematic review and meta-analysis. Ocul Immunol Inflamm. 2021;29(1):66–75. doi:10.1080/09273948.2020.1755441
5. Schroeter CA, Haaf-von Below S, Neumann HAM. Effective treatment of rosacea using intense pulsed light systems. Dermatol Surg. 2005;31(10):1285–1289. doi:10.1111/j.1524-4725.2005.31204
6. Angermeier MC. Treatment of facial vascular lesions with intense pulsed light. J Cutan Laser Ther. 1999;1(2):95–100. doi:10.1080/14628839950516922
7. Piyacomn Y, Kasetsuwan N, Reinprayoon U, Satitpitakul V, Tesapirat L. Efficacy and safety of intense pulsed light in patients with Meibomian gland dysfunction-A randomized, double-masked, sham-controlled clinical trial. Cornea. 2020;39(3):325–332. doi:10.1097/ICO.0000000000002204
8. Toyos R, McGill W, Briscoe D. Intense pulsed light treatment for dry eye disease due to Meibomian gland dysfunction; a 3-year retrospective study. Photomed Laser Surg. 2015;33(1):41–46. doi:10.1089/pho.2014.3819
9. Liu R, Rong B, Tu P, et al. Analysis of cytokine levels in tears and clinical correlations after intense pulsed light treating Meibomian gland dysfunction. Am J Ophthalmol. 2017;183:81–90. doi:10.1016/j.ajo.2017.08.021
10. Demolin L, Es-Safi M, Soyfoo MS, Motulsky E. Intense pulsed light therapy in the treatment of dry eye diseases: a systematic review and meta-analysis. J Clin Med. 2023;12(8):3039. doi:10.3390/jcm12083039
11. Peira N, Ali EM, Modén NK, Fjellgren E, Lennmarken C, Hultcrantz M. Effectiveness and safety of intense pulsed light therapy for dry eye symptoms due to Meibomian gland dysfunction-A systematic review and meta-analysis. Acta Ophthalmol. 2025;103(4):371–379. doi:10.1111/aos.16802
12. Miao S, Yan R, Jia Y, Pan Z. Effect of intense pulsed light therapy in dry eye disease caused by Meibomian gland dysfunction: a systematic review and meta-analysis. Eye Contact Lens. 2022;48(10):424–429. doi:10.1097/ICL.0000000000000934
13. Arita R, Itoh K, Inoue K, Kuchiba A, Yamaguchi T, Amano S. Contact lens wear is associated with decrease of meibomian glands. Ophthalmology. 2009;116(3):379–384. doi:10.1016/j.ophtha.2008.10.012
14. Uçakhan Ö, Arslanturk-Eren M. The role of soft contact lens wear on Meibomian gland morphology and function. Eye Contact Lens. 2019;45(5):292–300. doi:10.1097/ICL.0000000000000572
15. Farid M, Kim CK, Spina A, Chen KG. Investigating risk factors for Meibomian gland dysfunction and loss among young medical trainees. Cornea. 2024;44(8):952–960. doi:10.1097/ICO.0000000000003768
16. Nien CJ, Massei S, Lin G, et al. Effects of age and dysfunction on human meibomian glands. Arch Ophthalmol. 2011;129(4):462–469. doi:10.1001/archophthalmol.2011.69
17. Jin X, Lin Z, Liu Y, Lin L, Zhu B. Hormone replacement therapy benefits meibomian gland dysfunction in perimenopausal women. Medicine. 2016;95(31):e4268. doi:10.1097/MD.0000000000004268
18. Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea. 2003;22(7):640–650. doi:10.1097/00003226-200310000-00008
19. Benítez-del-Castillo JM, López-Pérez MD, Cano-Ortiz A, et al. Efficacy and safety of intense pulsed light of upper and lower eyelids in Meibomian gland dysfunction: a prospective multicentric study. Eur J Ophthalmol. 2023;34(3):700–707. doi:10.1177/11206721231199121
20. Arita R, Itoh K, Inoue K, Amano S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology. 2008;115(5):911–915. doi:10.1016/j.ophtha.2007.06.031
21. Ngo W, Situ P, Keir N, Korb D, Blackie C, Simpson T. Psychometric properties and validation of the Standard Patient Evaluation of Eye Dryness questionnaire. Cornea. 2013;32(9):1204–1210. doi:10.1097/ICO.0b013e318294b0c0
22. Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15(3):575–628. doi:10.1016/j.jtos.2017.05.006
23. Ahn H, Kim BY, Kim J, et al. How long to continue eyelid hygiene to treat Meibomian gland dysfunction. J Clin Med. 2022;11(3):529. doi:10.3390/jcm11030529
24. Jones L, Craig JP, Markoulli M, et al. TFOS DEWS III: management and therapy. Am J Ophthalmol. 2025;279:289–386. doi:10.1016/j.ajo.2025.05.039
25. Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.244
26. King-Smith PE, Hinel EA, Nichols JJ. Application of a novel interferometric method to investigate the relation between lipid layer thickness and tear film thinning. Invest Ophthalmol Vis Sci. 2010;51(5):2418–2423. doi:10.1167/iovs.09-4387
27. Craig JP, Tomlinson A. Importance of the lipid layer in human tear film stability and evaporation. Optom Vis Sci. 1997;74(1):8–13. doi:10.1097/00006324-199701000-00014
28. Xue AL, Wang MTM, Ormonde SE, Craig JP. Randomised double-masked placebo-controlled trial of the cumulative treatment efficacy profile of intense pulsed light therapy for Meibomian gland dysfunction. Ocul Surf. 2020;18(2):286–297. doi:10.1016/j.jtos.2020.01.003
29. Toyos R, McGill W, Duncan S, et al. Prospective evaluation of intense pulsed light for evaporative dry eye. Photobiomodul Photomed Laser Surg. 2022;40(3):123–131.
30. Rong B, Tang Y, Tu P, et al. Intense pulsed light applied directly on eyelids combined with Meibomian gland expression to treat Meibomian gland dysfunction. Photomed Laser Surg. 2018;36(6):326–332. doi:10.1089/pho.2017.4402
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.