Back to Journals » Clinical Ophthalmology » Volume 19
Aganirsen as a Therapeutic Alternative for Modulating Corneal Neovascularization: A Real-World Case Series Study
Authors García-Delpech S ![]() , Fathi Nieto S, Hervás Ontiveros A, Udaondo P
, Fathi Nieto S, Hervás Ontiveros A, Udaondo P ![]() , Garcia-Teillard D
, Garcia-Teillard D
Received 8 June 2025
Accepted for publication 12 September 2025
Published 22 September 2025 Volume 2025:19 Pages 3497—3504
DOI https://doi.org/10.2147/OPTH.S545516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video abstract presented by García-Delpech.
Views: 139
Salvador García-Delpech,1 Sara Fathi Nieto,2 Ana Hervás Ontiveros,2,3 Patricia Udaondo,1,2 Damian Garcia-Teillard1,4
1Aiken Ophthalmological Clinic and Aiken Foundation, Valencia, Spain; 2Department of Ophthalmology, Hospital Universitario Y Politécnico La Fe, Valencia, Spain; 3Eón Oftalmología, Valencia, Spain; 4Clínica Central Ocular, Madrid, Spain
Correspondence: Salvador García-Delpech, Aiken Ophthalmological Clinic and Aiken Foundation, C/ Ciril de Amorós 31, bajo, L’Eixample, Valencia, E-46004, Spain, Tel +34 960046566, Email [email protected]
Purpose: To assess the clinical benefits of aganirsen, an antisense oligonucleotide targeting insulin receptor substrate-1 (IRS-1), for reducing corneal neovascularization (CoNV) in patients scheduled for corneal transplantation.
Patients and Methods: Retrospective cohort study of patients who were treated with 1 drop of aganirsen (0.86 mg/mL) twice daily during 1 week preoperatively and at least 3 months after surgery. Changes in neovascularization were assessed qualitatively on slit-lamp examination.
Results: The study population included 65 patients (males 61.5%), with a mean age of 60.3 years. Bilateral CoNV was observed in 1 patient only (1.5%). Main diagnoses included corneal dystrophy in 61.5% of patients, transplant rejection in 10.8%, herpes simplex keratitis and leucoma in 7.7% each, and mechanical trauma in 3.1%. A reduction of neovascularization was observed in all eyes (100%) after 3 months of treatment. Results were not influenced by demographic characteristics or diagnosis. Treatment with aganirsen made graft surgery unnecessary in 3 out of 65 patients (4.6%). Failure of corneal transplantation occurred in 5 out of 62 patients (8.1%). Diagnosis at presentation in these 5 patients were corneal dystrophy in 2, previous transplant rejection in 2, and herpetic keratouveitis in 1. Some patients presented minor conjunctival hyperemia, and 1 patient reported pruritus and discontinued the study at 2 months of treatment.
Conclusion: This real-world study of the use of aganirsen months starting 1 week before graft surgery adds evidence of the clinical benefits of this agent in modulating neovascularization. Standardizing and extending the duration of treatment with aganirsen may further optimize the outcome of corneal transplantation.
Keywords: aganirsen, corneal neovascularization, penetrating keratoplasty, real-life study, retrospective cohort
Introduction
Corneal neovascularization (CoNV), caused by a disruption of the balance between angiogenic and antiangiogenic factors that preserve corneal transparency, is characterized by the in-growth of new vessels mediated by the upregulation of angiogenic cytokines.1 These atypical vessels have increased vascular permeability leading to chronic corneal edema, lipid and protein exudation, and disarrangement of the stromal lamellae.2 The disease may occur secondary to multiple factors, such as mechanical trauma, chemical burn, infection, chronic inflammation, contact lens wearing, autoimmune disorders, limbal stem deficiency, and post-corneal surgery.3,4 CoNV is the second cause of blindness worldwide and represents a major public health concern.5–7 Also, severe CoNV (affecting three or four of the quadrants) is a significant predictor of low visual acuity and decreased corneal sensitivity.7
CoNV reduces the immune privilege of the cornea8 and is one of the main causes of failure of corneal transplantation by promoting inflammatory processes and repeated immune rejected grafts.9,10 Moreover, there is an incremental increase of risk for graft failure and rejection as more corneal quadrants are affected by neovascularization before keratoplasty.10–12 Therefore, timely treatment of CoNV is of crucial importance to prevent the impact on corneal transplantation, as well as to increase visual acuity in patients with neovascularized stromal opacities that extend into the optic axis and to control local inflammatory processes by reducing the influx of immune cells and inflammatory mediators into the injured corneal stroma.13
In clinical practice, effective treatment of corneal neovascularization is currently problematic because of the limited success of different approaches.14 Traditional treatment of CoNV involves the use of systemic immunosuppressants, such as corticosteroids and mycophenolate mofetil, but these modalities are associated with substantial risks of infectious complications and other comorbidities.15 Also, topical strategies, such as vascular endothelial factors (VEGF) inhibitors, have significant limitations especially due to the need for repeated applications and the risk of a rebound effect.16
In this context, aganirsen (GS-101), an antisense oligonucleotide targeting insulin receptor substrate-1 (IRS-1), has emerged as a promising therapeutic option for CoNV. Aganirsen inhibits IRS-1, a protein involved in corneal neovascularization pathway, potentially reducing the formation of new blood vessels and inflammation.17,18 In pathological conditions, overexpression of IRS-1 protein determines overexpression of angiogenic VEGF and IL-1β among other cytokines, which play a key role in the formation of new vessels and corneal inflammation.19,20 The dual action of aganirsen by inhibiting VEGF pathways and the expression of inflammatory mediators (such as IL-1β, IL-8, IL-12, IL-22, and TNFα) allows a sustain regulation of inflammation and neovascularization, and avoids adverse effects associated with total receptor blockade.21 Aganirsen has an Orphan Drug designation from the European Regulatory Authorities (European Medicines Agency, 2017)22 and from the Office of Orphan Products Development of the Food and Drug Administration (2016)23 for the prevention of corneal graft rejection (via the control of corneal neovascularization). Administered as topical eye drops, aganirsen has demonstrated effective penetration into the aqueous and vitreous humors, facilitating effective local action without the systemic risks associated with other treatments. In the first randomized Phase III trial, topical aganirsen significantly inhibited CoNV in patients with keratitis and reduced the need for transplantation in patients with viral keratitis and central neovascularization.24,25 These benefits, along with its favorable safety profile, position aganirsen as an innovative tool for the management of complex corneal conditions, offering not only improved clinical outcomes but also a significant reduction in healthcare costs and associated complications. However, data of the use of aganirsen in real-world studies are limited.
Aganirsen was initially marketed under compassionate use by GeneSignal, from 2009 to 2019 and was known as GS-101. In 2022, Laboratoires KÔL became the new product owner and markets it under Olisens® trademark. In the context of the commercialization of the product under compassionate use since 2023 in some European countries (Olisens® single-dose vials, Laboratoires KÔL, France), it was crucial to perform a retrospective study of Spanish patients already treated in 2009. Therefore, the objective of this retrospective cohort study was to examine the effects of topical aganirsen administered before and after corneal transplantation in a clinical series of patients attended in daily practice conditions.
Patients and Methods
Design and Participants
This was a retrospective study of the use of topical aganirsen in patients scheduled for penetrating keratoplasty attended at the Department of Ophthalmology of an acute-care teaching hospital in Valencia (Spain) between 2015 and 2017, when this drug was being used as a compassionate medication in six countries (Germany, France, Spain, Switzerland, Norway, and Colombia), with the Spanish hospital as the one with the largest number of cases. Included patients were diagnosed of different eye conditions that require corneal graft surgery who presented with neovascularization at slit-lamp examination on the course of their illness and confirmed during a minimum period of 1 week preoperatively, with corneal vessels reaching out for at least 2.5 mm from the limbus or reaching the corneal center.
The study complied with the Declaration of Helsinki. Institutional review committee approval was obtained from Hospital Universitario y Politécnico La Fe (Valencia, Spain) and all patients provided written informed consent for the compassionate use of the drug.
Treatment and Data Collection
Patients were instructed to apply 1 drop of aganirsen (0.86 mg/mL) on the affected eye twice daily, in the morning and evening, for at least 3 months including 1 week preoperatively and the remaining days during the postoperative period. All patients were carefully informed regarding the storage conditions (in the refrigerator) and the use of the product, as well as the importance of following these recommendations strictly. In cases of bilateral lesions, both eyes were treated. Other antiangiogenic treatments were not allowed during the study. Any new concomitant medication started during the study should be approved by the ophthalmologist in charge of the patient.
For the purpose of the study, patients were visited at baseline (within 1 week before surgery) and at 30-day intervals after corneal transplantation, with a final visit at 3 months after starting treatment with aganirsen. Neovascularization was assessed using standard photographs of the cornea preoperatively and over the course of follow-up by the same investigator (S.G.-D). Data collection included: demographics (age, sex); preoperative diagnosis including previous failed corneal transplant; eye affected; neovascularization; outcome of the transplant; and adverse effects (AEs). Data were collected from the patients’ medical records and were anonymized for descriptive analysis.
Endpoint
The primary endpoint of the study was to confirm the inhibitory effect of aganirsen on corneal neovascularization in patients with eye diseases requiring corneal graft surgery.
Statistical Analysis
Descriptive statistics of patients for whom complete data regarding the effect of aganirsen after 3 months of starting treatment are reported. Categorical variables are expressed as frequencies and percentages, and continuous variables as mean and standard deviation (SD).
Results
A total of 72 eligible patients were recruited during the study period, but 7 patients were excluded from the analysis because they were lost to follow-up because they were visited at another center (n = 6) and patient’s decision to cancel the surgical procedure (n = 1). Therefore, the study population included 65 patients, 40 men and 25 women, with a mean (SD) age of 60.3 (17.1) years (range 27–94 years). The main preoperative characteristics are shown in Table 1. The right eye was affected in 34 cases (52.3%) and both eyes in 1 (1.5%), so that a total of 66 eyes were treated. Corneal dystrophy was the most common diagnosis (61.5) followed by transplant rejection (10.8%), leukoma (7.7%), herpes simplex keratitis (7.7%), and mechanical trauma (3.1%). Moreover, superficial neovascularization was present in 47 (72.3%) patients and deep neovascularization in the remaining 18 (27.7%) (Table 2).
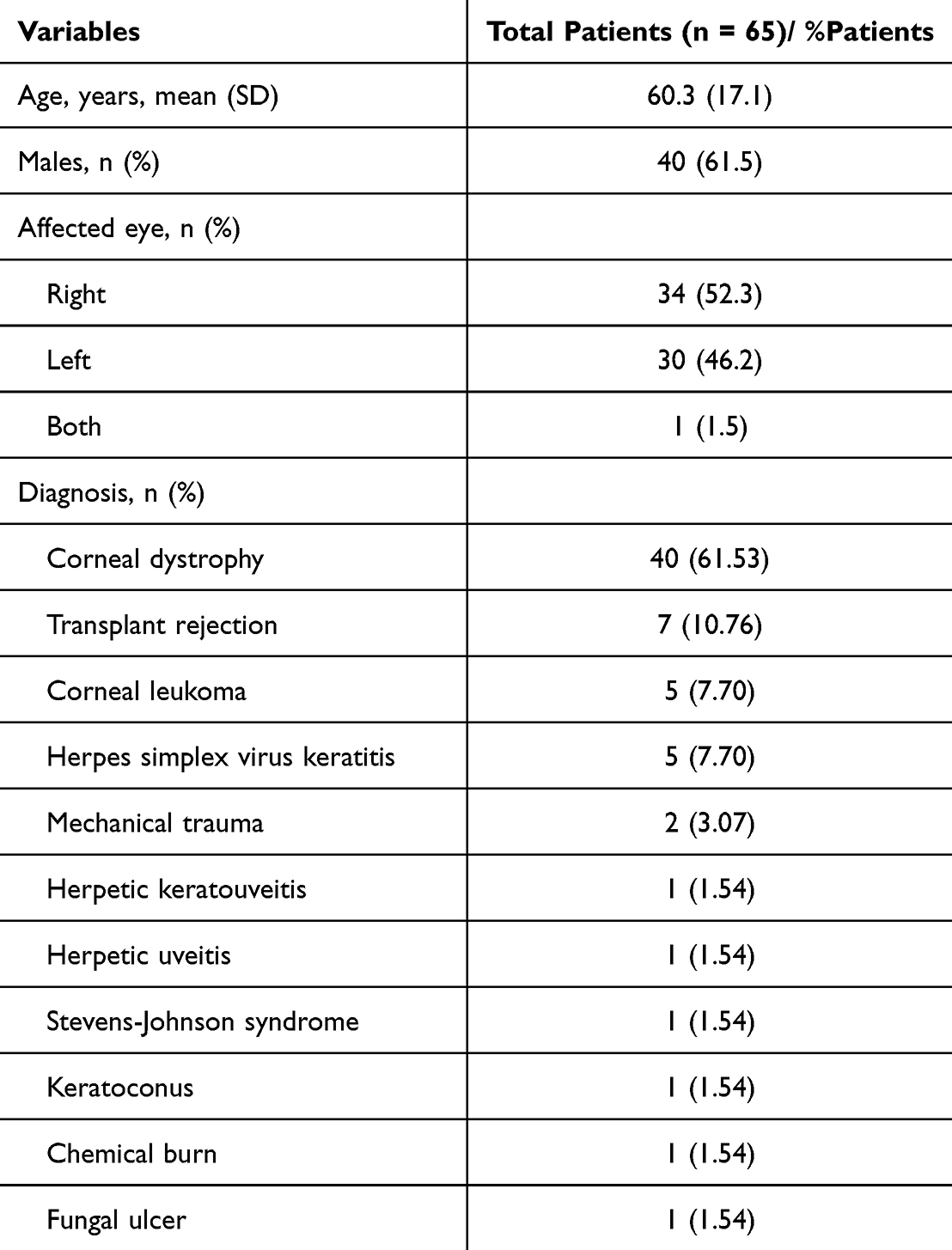 |
Table 1 Demographic Data and Preoperative Characteristics |
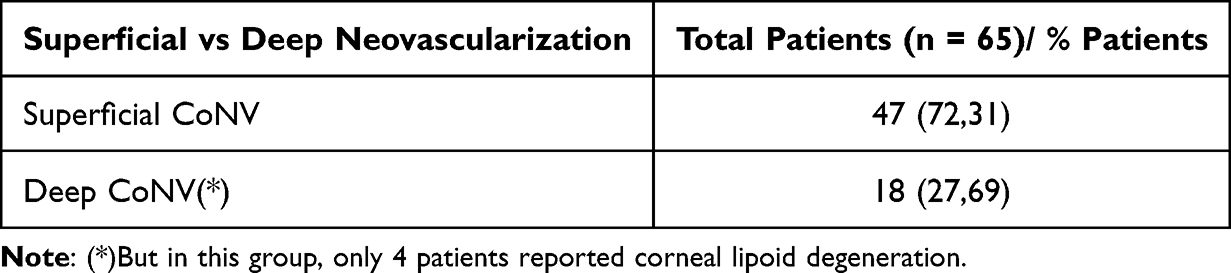 |
Table 2 Superficial Vs Deep Neovascularization |
Aganirsen remarkably improved the relative area of corneal neovascularization at a dose of 86 µg twice a day. A reduction of neovascularization was observed in all eyes (100%) after 3 months of treatment with aganirsen. The results were not influenced by the sex or age of the patients, neither by preoperative diagnosis. Treatment with aganirsen made corneal graft surgery unnecessary in 3 out of 65 patients (4.6%). Of the remaining 62 patients who underwent corneal transplantation, graft failure occurred in 5 (8.1%). Diagnosis at presentation in these 5 patients included corneal dystrophy in 2, previous transplant rejection in 2, and herpetic keratouveitis in 1. Illustrative cases of improvement of CoNV with the use of aganirsen are shown in Figures 1–4.
 |
Figure 1 Patient with corneal neovascularization and loss of visual acuity after herpetic keratitis (left). Reduction of neovascularization after 2 months of treatment with aganirsen (right). |
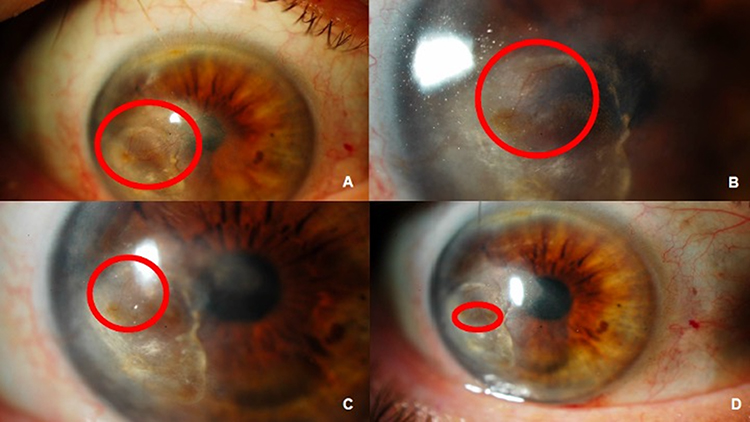 |
Figure 2 Patient with long-standing corneal neovascularization after mechanical trauma. Improvement of visual acuity and neovessels (encircled in red) over 1 year of treatment with aganirsen (A–D).(A=pre; B=1month; C=3months; D=1 year). |
 |
Figure 3 Changes of corneal neovessels (left) showing improvement with aganirsen treatment (right) in a grafted patient. |
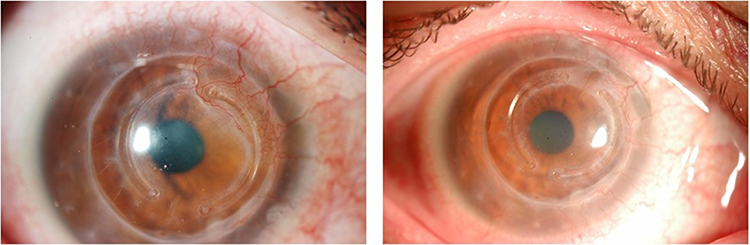 |
Figure 4 Corneal neovessels before treatment with aganirsen (left) and reduction of neovessels with disappearance of involvement of the intracorneal ring perimeter within 3 months of treatment of aganirsen (right). |
Treatment with aganirsen eye drops was safe and well tolerated. Some patients presented minor conjunctival hyperemia, which did not cause discontinuation of treatment. One patient, however, reported pruritus and was withdrawn from the study after 2 months of starting treatment with aganirsen. Serious adverse events were not found.
Discussion
This retrospective real-world study adds evidence of the efficacy of topical treatment with aganirsen eye drops for the reduction of CoNV of different etiologies after 3 months of treatment. The initial objective of the study was to improve corneal graft survival expectations in patients undergoing penetrating keratoplasty. In relation to the endpoint of the study, the present findings demonstrate the improvement in CoNV as a result of the inhibitory effect of the aganirsen on corneal angiogenesis and inflammatory pathways. Aganirsen was well tolerated, except for one patient who discontinued the study due to pruritus.
Data of this real-world study confirm the efficacy of aganirsen previously reported in experimental studies and in clinical trials. In a 10-day study of rat corneal neovascularization comparing subconjunctival injections of IRS-1 antisense oligonucleotide with phosphate buffer saline (PBS) (control), the mean area covered by new vessels was significantly larger in PBS-treated animals than in those treated with the study product (95% vs 59%, p < 0.001) and the synthesis of IRS-1 were significantly downregulated when compared with controls, opening new strategies for the potential treatment of ocular neovascular processes.21 Further studies in green monkeys with laser-induced CoNV, topical administration of 86 μg dose of aganirsen resulted in significant and near-complete inhibition of neovascularization lesions.26 In the same study, topical aganirsen inhibited retinal neovascularization in a model of oxygen-induced retinopathy in rats. Moreover, the expression of IRS-1 mRNA transcript was low in retinal biopsy samples isolated from patients with proliferative vitreoretinopathy associated with glial or retinal pigment epithelium proliferation, but was 12-fold higher (p < 0.001) in samples isolated from patients with subretinal neovascularization.26 Taken together, these results suggested a promising therapeutic profile for further testing in the clinical setting for conditions involving potent increases in IRS-1 expression, such as eye diseases associated with neovascularization. The availability of aganirsen as an inhibitor of neovascularization in this setting is clinically relevant because of the unmet need for effective therapies in these disorders.
Data of a randomized, double-blind, multicenter, Phase II clinical study showed that in 40 patients with progressive CoNV resulting from various underlying diseases being nonresponsive to conventional therapy, treated for 3 months with aganirsen at a dose of 86 µ/day produced a significant inhibition and regression of corneal neovascularization.24 In the multicenter, double-masked, randomized, placebo-controlled phase III clinical trial, differences in visual acuity scores between aganirsen and placebo were not found, but aganirsen significantly reduced the relative CoNV area after 90 days by 26.20% and this improvement persisted after 180 days. The persisting inhibitory effect of aganirsen may be explained by the anti-inflammatory activity of the drug, complementing its antiangiogenic effect. Also, in patients with viral keratitis and central neovascularization, a significant reduction in transplantation need was achieved.25
Results of the present clinical series with a reduction of neovascularization in 100% of patients and a rate of transplantation failure of only 8.1% (5 patients) adds evidence of the efficacy of this novel antisense oligonucleotide targeting IRS-1 in the management of CoNV. It should be noted that after 3 months of treatment with aganirsen, graft surgery was no longer considered necessary in 3 patients (4.6%) due to the favorable evolution of CoNV. Different strategies focused on reduction of neovascularization for improving the outcome of corneal transplantation have been explored, including intravitreal and corneal injections of anti-VEGF agents.16,27,28 However, when the effect of anti-VEGF injections disappears upon cessation of receptor blockade, a rebound phenomenon has been described.29 Other approaches including cautery of new vessels with different techniques have shown inconsistent results and might also secondarily lead to neovascularization due to an increase in inflammation and the release of proangiogenic mediators.15
Aganirsen ophthalmic solution exerts its effects through a distinct mechanism of action, primarily by modulating pathological neovascularization. It targets both the VEGF signaling pathway and IL-mediated inflammatory pathways.30 Although clinical effects may not be immediately apparent in the initial days of treatment, the formulation ultimately achieves a downregulation of the inflammatory response and angiogenic activity, leading to disease stabilization without inducing a rebound effect. The therapeutic strategy does not rely on receptor antagonism, but instead on modulating the endogenous production of these receptors. Moreover, the fact that aganirsen was developed as a topical ophthalmic formulation, and has shown absorption into both the aqueous and vitreous humors, circumvents the limitations in efficacy observed with other agents. Aganirsen eye drops may be used in association with other therapies targeting the underlying etiological factors of CoNV. Through such a combined therapeutic approach, sustained treatment over approximately 3 to 4 months can lead to clinical stabilization. Additionally, this strategy enables a significant reduction in the need for systemic immunosuppressant agents, thereby minimizing associated adverse effects and overall treatment costs.
This study was retrospective review of real-world clinical cases aimed at evaluating the effect of the drug on CoNV reduction. The outcomes were based on the within-patient change in neovascularization compared with each patient’s baseline image. As this was not a prospective clinical trial but rather a report of real-world evidence, there is no control group and no standardized quantitative assessment of neovascular reduction. Nevertheless, the presence of such a reduction is clinically relevant for the patient’s disease progression. In this respect, limitations of the study include the retrospective design, the lack of a control group and assessment of intra-observer reliability, the use of descriptive statistics, and the fact that neovascularization was assessed qualitatively rather than using objective criteria. Analysis by the etiology of CoNV or the number of quadrants affected was not performed. Also, differences in the reduction of neovascularization according to age, sex, and preoperative diagnosis were not observed, but inferential statistical analyses were not performed. However, the relatively large study population and the evaluation of clinical benefits of aganirsen in conditions of daily practice are strengths of the study.
The modulation of neovessels and inflammation, without actual receptor blockage, is the underlying mechanism of the clinically relevant effects of aganirsen. Appropriate control of neovascularization may be associated with critical advantages, including a decrease in the use of systemic immunosuppressants with prevention of their side effects and cost reduction, improvement of visual acuity depending on the central position of the neovascularization area, reduction in the incidence of transplant rejection and graft failure, and the possibility of delaying the surgical intervention or even deemed unnecessary in selected cases. It would be recommendable to standardized the use of aganirsen in all corneal transplant recipients, with the possibility of extending the treatment duration to further optimize the outcome of keratoplasty.
Conclusion
This real-world study shows that in patients with CoNV of different etiologies scheduled for corneal graft surgery, treatment with aganirsen eye drops for 3 months starting 1 week before corneal transplantation, was effective in reducing neovascularization. However, future studies with robust prospective controlled designs and quantitative endpoints are necessary to confirm these preliminary findings and to further establish the place of aganirsen in daily practice.
Data Sharing Statement
The dataset supporting the findings of this study are available from the corresponding author on request.
Acknowledgments
The authors thank Dr Marta Pulido for editing the manuscript and editorial assistance supported by KÔL Laboratories.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
S. García-Delpech: consultant for GeneSignal and member of an advisory board for Laboratoires KÔL. The remaining authors have no conflicts of interest to be disclosed for this work.
References
1. Nicholas MP, Mysore N. Corneal neovascularization. Exp Eye Res. 2021;202:108363. doi:10.1016/j.exer.2020.108363
2. Wu D, Chan KE, Lim BXH, et al. Management of corneal neovascularization: current and emerging therapeutic approaches. Indian J Ophthalmol. 2024;72(Suppl 3):S354–S371. doi:10.4103/IJO.IJO_3043_23
3. Chang JH, Gabison EE, Kato T, Azar DT. Corneal neovascularization. Curr Opin Ophthalmol. 2001;12(4):242–249. doi:10.1097/00055735-200108000-00002
4. Nomura K, Nakao M, Matsubara K. Subjective symptom of eye dryness and lifestyle factors with corneal neovascularization in contact lens wearers. Eye Contact Lens. 2004;30(2):95–98. doi:10.1097/01.icl.00000117256.77329.06
5. Skobe M, Dana R. Blocking the path of lymphatic vessels. Nat Med. 2009;15(9):993–994. doi:10.1038/nm0909-993
6. Lee P, Wang CC, Adamis AP. Ocular neovascularization: an epidemiologic review. Surv Ophthalmol. 1998;43(3):245–269. doi:10.1016/s0039-6257(98)00035-6
7. Lasagni Vitar RM, Triolo G, Fonteyne P, et al. Epidemiology of corneal neovascularization and its impact on visual acuity and sensitivity: a 14-year retrospective study. Front Med. 2021;8:733538. doi:10.3389/fmed.2021.733538
8. Niederkorn JY. Corneal transplantation and immune privilege. Int Rev Immunol. 2013;32(1):57–67. doi:10.3109/08830185.2012.737877
9. Alio JL, Montesel A, El Sayyad F, et al. Corneal graft failure: an update. Br J Ophthalmol. 2021;105(8):1049–1058. doi:10.1136/bjophthalmol-2020-316705
10. Bachmann B, Taylor RS, Cursiefen C. Corneal neovascularization as a risk factor for graft failure and rejection after keratoplasty: an evidence-based meta-analysis. Ophthalmology. 2010;117(7):1300–5.e7. doi:10.1016/j.ophtha.2010.01.039
11. Sellami D, Abid S, Bouaouaja G, et al. Epidemiology and risk factors for corneal graft rejection. Transplant Proc. 2007;39(8):2609–2611. doi:10.1016/j.transproceed.2007.08.020
12. Garcia DD, Shtein RM, Musch DC, Elner VM. Herpes simplex virus keratitis: histopathologic neovascularization and corneal allograft failure. Cornea. 2009;28(9):963–965. doi:10.1097/ICO.0b013e31819c4e55
13. Sharif Z, Sharif W. Corneal neovascularization: updates on pathophysiology, investigations & management. Rom J Ophthalmol. 2019;63(1):15–22. doi:10.22336/rjo.2019.4
14. Gupta D, Illingworth C. Treatments for corneal neovascularization: a review. Cornea. 2011;30(8):927–938. doi:10.1097/ICO.0b013e318201405a
15. Drzyzga Ł, Śpiewak D, Dorecka M, Wyględowska-Promieńska D. Available therapeutic options for corneal neovascularization: a review. Int J Mol Sci. 2024;25(10):5479. doi:10.3390/ijms25105479
16. Chang JH, Garg NK, Lunde E, Han KY, Jain S, Azar DT. Corneal neovascularization: an anti-VEGF therapy review. Surv Ophthalmol. 2012;57(5):415–429. doi:10.1016/j.survophthal.2012.01.007
17. Hos D, Regenfuss B, Bock F, Onderka J, Cursiefen C. Blockade of insulin receptor substrate-1 inhibits corneal lymphangiogenesis. Invest Ophthalmol Vis Sci. 2011;52(8):5778–5785. doi:10.1167/iovs.10-6816
18. Cursiefen C, Colin J, Dana R, et al. Consensus statement on indications for anti-angiogenic therapy in the management of corneal diseases associated with neovascularisation: outcome of an expert roundtable. Br J Ophthalmol. 2012;96(1):3–9. doi:10.1136/bjo.2011.204701
19. Rabinovsky ED, Draghia-Akli R. Insulin-like growth factor I plasmid therapy promotes in vivo angiogenesis. Mol Ther. 2004;9(1):46–55. doi:10.1016/j.ymthe.2003.10.003
20. Al-Mahmood S, Colin S, Farhat N, Thorin E, Steverlynck C, Chemtob S. Potent in vivo antiangiogenic effects of GS-101 (5’-TATCCGGAGGGCTCGCCATGCTGCT-3’), an antisense oligonucleotide preventing the expression of insulin receptor substrate-1. J Pharmacol Exp Ther. 2009;329(2):496–504. doi:10.1124/jpet.108.147496
21. Berdugo M, Andrieu-Soler C, Doat M, Courtois Y, BenEzra D, Behar-Cohen F. Downregulation of IRS-1 expression causes inhibition of corneal angiogenesis. Invest Ophthalmol Vis Sci. 2005;46(11):4072–4078. doi:10.1167/iovs.05-0105
22. Commission of the European Communities of 17-IV-2007 related to the medicinal product “Antisense Oligonucleotide (TATCCGGAGGGCTCGCCATGCTGCT)” is designated as an orphan medicinal product for the indication: prevention of corneal graft rejection. It shall be entered in the community register of orphan medicinal products under number EU/3/07/445.
23. U.S. Food & Drug Administration. U.S. Department of Health & Human Services. Orphan Drug Designation and Approval. Available from: https://www.accessdata.fda.gov/scripts/opdlisting/oopd/detailedIndex.cfm?cfgridkey=500515.
24. Cursiefen C, Bock F, Horn FK, et al. GS-101 antisense oligonucleotide eye drops inhibit corneal neovascularization: interim results of a randomized phase II trial. Ophthalmology. 2009;116(9):1630–1637. doi:10.1016/j.ophtha.2009.04.016
25. Cursiefen C, Viaud E, Bock F, et al. Aganirsen antisense oligonucleotide eye drops inhibit keratitis-induced corneal neovascularization and reduce need for transplantation: the I-CAN study. Ophthalmology. 2014;121(9):1683–1692. doi:10.1016/j.ophtha.2014.03.038
26. Cloutier F, Lawrence M, Goody R, et al. Antiangiogenic activity of aganirsen in nonhuman primate and rodent models of retinal neovascular disease after topical administration. Invest Ophthalmol Vis Sci. 2012;53(3):1195–1203. doi:10.1167/iovs.11-9064
27. Keating AM, Jacobs DS. Anti-VEGF treatment of corneal neovascularization. Ocul Surf. 2011;9(4):227–237. doi:10.1016/s1542-0124(11)70035-0
28. Lai SC, Loh EW, Chiou DI, Hong CT. Efficacy and safety of anti-vascular endothelial growth factor agents on corneal neovascularization: a meta-analysis. World J Clin Cases. 2023;11(30):7337–7349. doi:10.12998/wjcc.v11.i30.7337
29. Yasuda S, Kondo M, Kachi S, et al. Rebound of macular edema after intravitreal bevacizumab therapy in eyes with macular edema secondary to branch retinal vein occlusion. Retina. 2011;31(6):1075–1082. doi:10.1097/IAE.0b013e318206cf4b
30. Bainbridge JW, Loroch V, Viaud E, Cursiefen C. Beyond anti-VEGFs - Anti-insulin receptor substrate-1 oligonucleotides as a novel approach to ocular neovascular disorders. Eur Ophthalmic Rev. 2012;6(3):190–193. doi:10.17925/EOR.2012.06.03.190
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.