Back to Archived Journals » Research and Reports in Neonatology » Volume 12
Advancing Clinical Decision Support Systems for the Management of Neonatal Nutrition: Barriers to Implementation
Authors Falciglia GH, Sierra-Fernandez H, Freeman M, Healy D, Wicks JS ![]() , Robinson DT
, Robinson DT
Received 3 January 2022
Accepted for publication 23 May 2022
Published 20 June 2022 Volume 2022:12 Pages 11—18
DOI https://doi.org/10.2147/RRN.S355468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Schelonka
Video abstract of "Advancing CDSS for the Management of Neonatal Nutrition" [ID 355468].
Views: 168
Gustave H Falciglia,1,2 Hernan Sierra-Fernandez,3 Melissa Freeman,2 Daniel Healy,2 Jennifer S Wicks,1,2 Daniel T Robinson1,2
1Department of Pediatrics, Northwestern University Feinberg School of Medicine, Chicago, IL, USA; 2Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL, USA; 3Department of Pediatrics, Rush University Medical Center, Chicago, IL, USA
Correspondence: Gustave H Falciglia, Ann & Robert H. Lurie Children’s Hospital of Chicago, 225 E. Chicago Ave, Box #45, Chicago, IL, 60611, USA, Tel +1 312 848-3142, Email [email protected]
Purpose: Few clinical decision support systems (CDSSs) are available to help clinicians calculate nutrition intake in infants in the neonatal intensive care unit (NICU) despite improvement in the accuracy of calculations and quality of nutrition delivered. The aim of this manuscript is to qualitatively define the barriers associated with the implementation of CDSSs to calculate fluid and nutrition intake.
Methods: After defining the data necessary to calculate fluid and nutrition intake, multidisciplinary groups analyzed CDSS capabilities and barriers to implementation at two academically affiliated NICUs. They implemented CDSSs to calculate intake received in the past (retrospective) and to estimate future intake from orders (prospective). Barriers and measures to reduce them are reported.
Results: Barriers to implementation include simultaneous enteral feeding orders, the use of free text in the electronic health record (EHR), and a large variety of enteral feeding types for clinical use. These barriers made implementation of prospective CDSSs more difficult. CDSSs reported values that were normalized by both the most recent measured weight (usually obtained daily) and a dosing weight, a weight updated less frequently and used by pharmacies to facilitate prescribing.
Conclusion: Despite using an EHR from the same vendor, different solutions were implemented at each NICU. CDSSs improved access to individual infant data on fluid and nutrition intake; however, none of the CDSSs easily exported data to monitor the quality of intake for the entire NICU or specific populations (eg, infants with bronchopulmonary dysplasia). Comprehensive CDSSs that include prospective intake and monitor the quality of nutrition intake through standardized values will require continued investigation and resources.
Keywords: clinical decision support, nutrition, infant, neonatal intensive care unit
Plain Language Summary
Adequate nutrition is extremely important for infants in the neonatal intensive care unit (NICU). It is associated with improved growth and long-term developmental outcomes. Clinical decisions support systems are tools, usually found in the Electronic Health Record (EHR), which help doctors, nurses, dietitians, and pharmacists provide optimal fluid and nutrition intake for these infants. Though calculating intake does not require complicated mathematics, manual calculations are time consuming and prone to error. Yet, few NICUs have these tools despite proven benefits. At two NICUs (one affiliated with a delivery hospital and the other a children’s hospital), we implemented clinical decision support systems to calculate fluid and nutrition intake. In the process, we discovered barriers to their implementation hindering adoption.
Several aspects of the logic of nutrition orders are not always understood by the EHR, making it difficult to calculate intake. Critically ill infants may require several nutrition orders at one time. Nutrition delivery may occur through both intravenous and intestinal routes (given orally or through a feeding tube). Infants may also require donor human milk or formula to supplement a mother’s milk when her supply is low. Each nutrition order requires a specific dosage and frequency; however, this logic is frequently documented using free-text or communicated verbally between clinicians (eg, “give formula when maternal milk is unavailable”). If the EHR cannot fully understand the logic of nutrition orders, then it cannot accurately calculate intake. Improving the quality of nutrition delivery will require additional investments to address these barriers.
Introduction
Eleven percent of infants globally and ten percent of infants in the United States are born preterm.1,2 Adequate nutrition is associated with improved growth and neurodevelopmental outcomes, and less retinopathy of prematurity in these infants.3–5 Despite the importance of optimizing nutrition, nutrient deficits accumulate rapidly in infants in the neonatal intensive care unit (NICU).6,7
Although critical illness is associated with lower energy intake,8 non-clinical factors also contribute. After adjusting for illness, variation in the amount of energy and protein provided to preterm infants exists between institutions and explains differences in growth.9 One source of non-clinical variation that may contribute to inadequate nutrition delivery is the availability of clinical decision support systems (CDSSs) to facilitate the calculation of nutrition intake.10
CDSSs are tools, generally found within the electronic health record (EHR), that give clinicians pertinent, real-time data to improve patient care through improved decision-making.11 In the NICU, CDSSs have been shown to improve energy and protein prescribed in parenteral nutrition (PN) orders while reducing errors.12,13 Despite these benefits, the prevalence of CDSSs to support nutrition decision-making remains low even at children’s hospitals where more neonatal-focused CDSSs might be expected.10 Clinicians must rely on manual calculations, which are associated with error,14 or which may not be performed in a busy NICU. To optimize nutrition delivery, clinicians require a “closed-loop system” of feedback to understand both what the infant has received and will receive.15
We describe the process of implementing CDSSs to calculate fluid and nutrition intake received in the past (retrospective intake) and estimate future intake from orders (prospective intake) in two academically affiliated NICUs. Nutrition is defined as energy, macronutrients (protein, fat, and carbohydrates) and micronutrients (eg, electrolytes). The aim of this qualitative analysis is to define existing barriers to CDSSs for fluid and nutrition intake, which we believe may contribute to the low prevalence.
Methods
After defining the data necessary to calculate nutrition intake, we analyzed the baseline capabilities of each NICU’s clinical setting and implemented retrospective and prospective CDSS interventions. We report on barriers to implementation and measures to reduce these barriers.
The Ann & Robert H. Lurie Children’s Hospital of Chicago Institutional Review Board determined that this project was exempt from full review because “it did not meet the definition of human subjects research as defined in 45 CFR 46.102 as it: 1) does not involve human subjects (data through intervention or interaction with the individual or identifiable private information), and/or 2) it is not a systematic investigation designed to develop or contribute to generalizable knowledge.”
Data for Calculating Nutrition in NICUs
As nutrition for critically ill infants is provided exclusively in fluid (eg, PN, human milk, infant formula), the data necessary to calculate nutrition intake include the volume and nutritional content of the fluid. The volume of fluid intake is found within the intake flowsheet of the EHR, a table where nursing discretely documents the administered volume of feeding, PN, and intravenous fluid that an infant has received according to time and type of fluid. With a knowledge of the macronutrient concentration of a specific volume, the macronutrient and energy content of the fluid volume can be calculated. This applies to both parenteral and enteral nutrition sources (enteral energy can be calculated directly using reference concentrations for human milk or fortification amount for a formula in kcal per ounce, approximately 30 mL). Similar principles apply to micronutrients.
Values may be reported as total intake or normalized using the most recent measured weight (usually obtained daily) or a dosing weight. Dosing weights are typically updated once or twice weekly by pharmacies to facilitate medication ordering in growing infants.16 They are also used by clinicians at both NICUs to account for rapid weight gain secondary to edema.
Level III NICU
Setting
The Level III NICU has 84 beds and is situated within a tertiary care labor and delivery hospital. It provides prolonged life support, including mechanical ventilation, to acutely ill term or preterm infants.17 A multidisciplinary clinical team reviews infant clinical status, including growth and nutrition, and discusses management during the morning rounds. The clinical team consists of an attending neonatologist, a neonatal fellow, front-line providers (pediatric residents, pediatric hospitalists, or advance nurse practitioners), dietitian, pharmacist, and bedside nurse. Typically, the front-line provider enters or modifies feeding orders, while the dietitian enters PN orders within the EHR; PN orders are automatically sent to a compounding pharmacy. On average, 5–10 infants require PN each day, generally due to prematurity.
The hospital of the Level III NICU used Cerner Corporation EHR (North Kansas City, MO) for 14 years. Using Cerner EHR, the NICU had a retrospective CDSS to calculate fluid intake but not nutrition intake. Daily fluid intake in total milliliters was calculated from the intake flowsheet. The NICU did not have any prospective CDSS to estimate future intake based on orders, leaving clinicians to rely on manual calculations.
Interventions
In 2018, the hospital system of the Level III NICU transitioned from Cerner to Epic Systems EHR (Verona, WI). With the transition, the NICU evaluated barriers to CDSSs for nutrition intake and ultimately implemented retrospective and prospective CDSSs available with Epic EHR.
A retrospective CDSS was implemented to calculate fluid intake in mL/kg using the most recent measured weight and enteral energy intake in total kilocalories from feeds (Table 1). Values could be reported over a variable time frame. Prospective CDSS for nutrition intake was implemented using the Epic “Calorie and Fluid Management Report.” This optional CDSS appears alongside nutrition orders and estimates total energy, macro- and micronutrient intake from parenteral and enteral nutrition. Values were normalized by weight with the option to use the most recent measured or dosing weight. Using manual calculations, clinicians assessed the accuracy of calculations from both CDSSs.
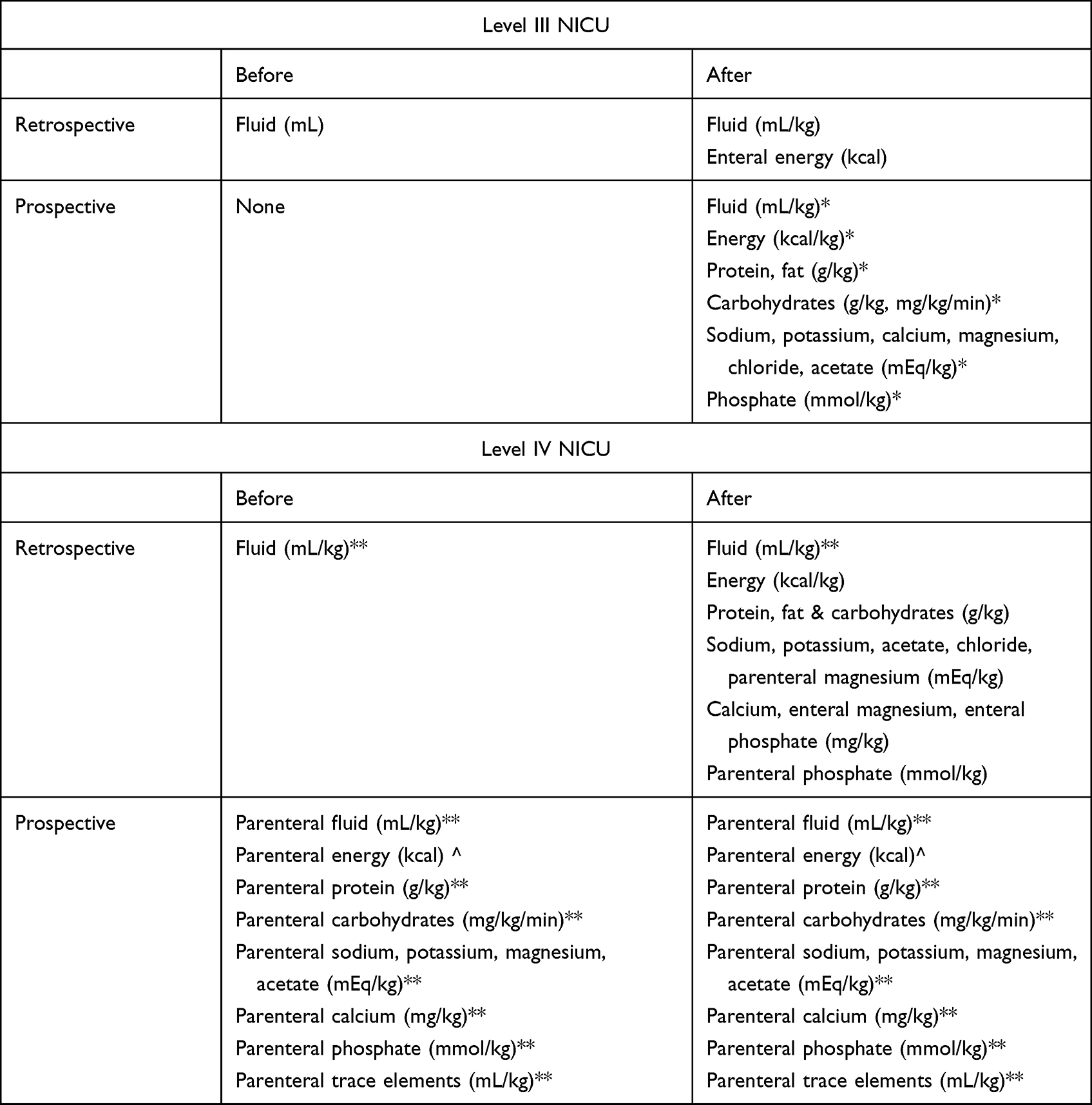 |
Table 1 Clinical Decision Support Systems to Calculate Total Fluid and Nutrition Intake |
Level IV NICU
Setting
The Level IV regional referral NICU has 64 beds and is situated within a children’s hospital. It provides subspecialty consultation or surgical care in addition to prolonged life support for infants of any gestational age.17 A multidisciplinary clinical team of similar composition as the Level III NICU also reviews infant clinical status and discusses management during the morning rounds; however, the pharmacist typically enters PN orders within the EHR, which are automatically sent to a compounding pharmacy. On average, 10–15 infants require PN each day due to prematurity or surgical pathology.
The hospital of the Level IV NICU has used Epic EHR for over 12 years and has a retrospective CDSS to calculate fluid intake in mL/kg over a variable time frame using the dosing weight. There was no retrospective CDSS to calculate nutrition intake. A prospective CDSS existed to estimate fluid, energy, macro-, and micronutrient intake from PN alongside the order.
Interventions
At the Level IV NICU, a multidisciplinary group of pharmacists, dietitians, physicians, and a project coordinator met 23 times over two years to implement retrospective and prospective CDSSs for nutrition intake. Early in the process, the group evaluated barriers to CDSS implementation and interventions. They considered CDSSs that were typed (calculations required clinicians to transcribe EHR data into the CDSS) versus automated (calculations did not require data transcription) and CDSSs that were integrated within the EHR versus standalone (operating outside the EHR).10 They preferred automated to typed CDSSs because they believed the latter were inefficient and prone to transcription error.
The multidisciplinary group implemented the Epic EHR “Nutrition Summary Accordion Report”, a CDSS that retrospectively calculated energy, macro- and micronutrient intake normalized using the most recent measured weight (Table 1). The choice of the measured weight differed from the existing retrospective CDSS for fluid using the dosing weight. Anecdotally, the dosing weight was smaller than the daily weight once the infant had regained birth weight. Therefore, there was a concern that normalizing nutrition intake with the dosing weight would overestimate intake. The retrospective fluid intake CDSS continued using the dosing weight because there was a concern that normalizing fluid intake with the measured weight would underestimate intake in an edematous infant. The group evaluated, but did not implement, the previously mentioned Epic EHR “Calorie and Fluid Management Report” to estimate nutrition intake prospectively.
Results
Level III NICU
Barriers
Several barriers were identified as obstacles to improving CDSSs at the Level III NICU. A major barrier included the use of simultaneous enteral feeding orders. Simultaneous feeding orders typically involved two isocaloric orders with the same volume and frequency linked by conditional logic (eg, “give formula if human milk is unavailable”). They gave nursing the flexibility to administer formula or donor human milk if indicated when the supply of maternal human milk was low. Occasionally, simultaneous orders varied in energy concentration (eg, unfortified human milk with 20 kcal per 30 mL and a transitional formula with 22 kcal per 30 mL) or route (eg, thickened formula fed orally and human milk without thickener fed via a gavage tube). The conditional nature of the orders (“either, or”) was typically implicit or communicated verbally from clinician to clinician rather than explicitly documented within the EHR.18 Besides introducing the opportunity for error, the EHR lacked the ability to recognize this implicit logic needed to estimate intake from orders.
Another barrier was the use of free-text entries within feeding orders, which allowed for considerable heterogeneity in how feeding details were prescribed. Free text is unstructured or narrative, and, unlike structured text, it is not organized around established clinical concepts that use discrete and consistent terminology.19 The NICU used free text in orders because it allowed for flexibility. Though many orders involved a specific volume at a specific time, clinicians also needed to account for scenarios of on-demand feeding orders (ie, per os ad libitum [POAL]), accelerating orders (eg, “increase continuous feeds by 1 mL per hour every 8 hours until at goal feeds”) or nursing advanced feeding protocols. Regardless, implementing prospective CDSSs required the categorization of free text within the EHR to discretely capture the volume and frequency of enteral feeds.20
Free-text entries also adversely impacted the generation of other aspects of retrospective CDSSs. Though nursing recorded fluid volumes discretely and numerically within the intake flowsheet of Cerner EHR, they recorded fluid descriptors with free text. The same type of fluid could be described differently due to typographical errors, non-standardized abbreviations, and inconsistent inclusion of select components. For example, we found 353 unique ways in which an intravenous fluid of 10% dextrose was documented despite containing the same concentration of carbohydrate and energy (Supplemental Figure 1). Thus, a retrospective CDSS for fluid intake had existed because discrete volumes from different types of fluids could be added together. Retrospective CDSS for nutrition intake did not exist because the nutritional content of each type of fluid was not categorized.
Barrier Resolution & CDSSs Limitations
Several changes to the intake flowsheet with the EHR transition supported retrospective CDSS. The EHR generated flowsheet rows for intravenous fluids and PN from orders rather than free text. This minimized the variability in fluid-type descriptors and allowed CDSS for fluid intake to be grouped by fluid type. CDSS to calculate enteral energy intake was supported through the addition of rows within the intake flowsheet to capture the energy concentration of enteral feeds (in kcal per 30 mL) manually and discretely. Though an improvement from baseline, several limitations remained. First, the CDSS did not normalize enteral energy intake by weight as opposed to fluid intake. Second, it did not calculate enteral macro- or micronutrient intakes. Third, the calculation required nursing to chart the energy concentration of each feed, a value already captured within the EHR by the feeding order. Fourth and finally, there was no CDSS to report any nutrition intake from non-enteral sources. Values were accurate if clinicians recorded the correct energy concentration; however, the above limitations have hindered adoption.
Several changes to the ordering process supported prospective CDSS. Rather than using free text to order enteral feeds, clinicians discretely entered the volume and frequency of enteral feeds to be administered. Thus, CDSS can estimate enteral intake from these discrete values and estimate parenteral intake from the composition of ordered PN (eg, g/kg of protein) or intravenous fluid (eg, percent dextrose). Although the prospective CDSS was comprehensive, providing data on fluid, energy, macro- and micronutrients with the option to normalize values using the measured or dosing weight, the conditional nature of simultaneous feeding orders remained unrecognized. Therefore, the CDSS frequently overestimated enteral intake by a factor of two, limiting usefulness and adoption by clinicians.
Level IV NICU
Barriers
Barriers to implementing CDSSs included the use of simultaneous feeding orders, free-text entries within enteral orders, and a large formulary of enteral feeds. Due to the complexity of diagnoses managed at the Level IV NICU, the formulary contained 108 different infant formula and human milk orders when all fortification concentrations were included (198 including available pediatric and adult formulas). This variation did not include modular additives such as medium-chain triglycerides and liquid protein. Retrospective and prospective CDSSs depended on the EHR’s ability to determine the nutritional content of each feeding type.
Barrier Resolution & CDSSs Limitations
Implementation of retrospective CDSS required changes to the EHR. Previously, the EHR had generated a single row within the intake flowsheet for PN, whereas each order of intravenous fluids was associated with a new row. Infants may be on PN for several weeks and this minimized the number of flowsheet rows in the chart. This approach hindered retrospective calculations because the volume associated with each unique PN order could not be determined. The EHR now provided a unique flowsheet row for each specific PN infusion to capture the volume from different PN orders with different nutrient concentrations.
The retrospective CDSS used details from orders to calculate nutrition intake from the volume documented within the flowsheet. The macro- and micronutrient concentrations of each order were defined, and the energy intake was calculated from the macronutrient intake. Given the number of enteral feeding orders, the CDSS extrapolated the macronutrient content for higher fortification levels (eg, the CDSS assumed that 24 kcal per 30 mL formula had 20% more protein than 20 kcal per 30 mL formula). Although this is accurate for formulas, which may be concentrated in less water to achieve a desired concentration, extrapolation may introduce a small error in human milk calculations because the addition of fortifiers displaces the original human milk volume.
The final retrospective CDSS provided a detailed summary of retrospective energy, macronutrients and selected micronutrients intake for infants and children (Figure 1) with the functionality to import updated values into a daily progress note, though one issue remained. Contributions from modular additives were not able to be included. The EHR could not recognize the ratio of the amount of additive (in g or mL) to the volume of enteral feeds because enteral feeding orders continued using free text.
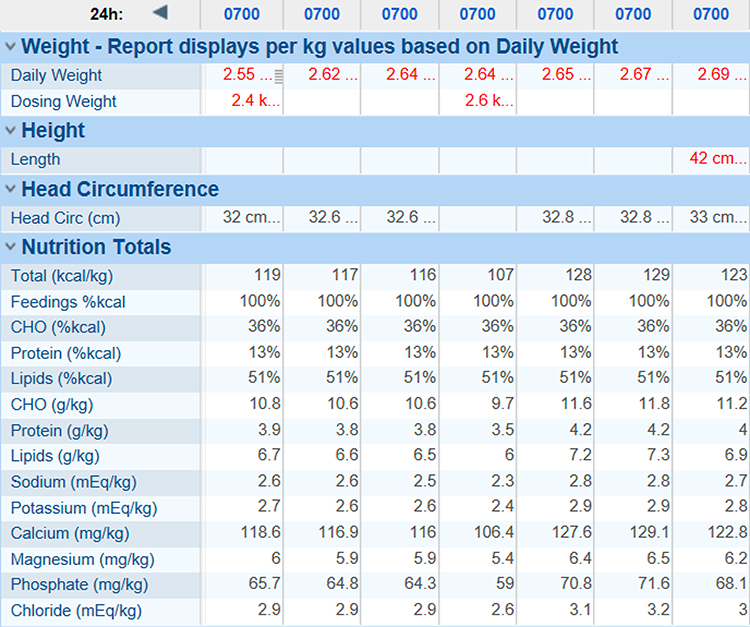 |
Figure 1 Clinical Decision Support System for Retrospective Nutrition Intake. |
After rigorous testing by the dietitians who compared their manual calculations with the automated CDSS calculations, the CDSS was available throughout all units in the hospital. The group did not implement prospective “Calorie and Fluid Management Report” because it would not understand the conditional nature of simultaneous feeding orders.
Discussion
The benefits of CDSSs to calculate nutrition and fluid intake include improved accuracy and consistent access to data required for the management of critically ill infants.14 For a 60-bed NICU, automated calculations for retrospective intake would save an estimated 2–3 hours of clinician time per day, assuming an average of 2–3 minutes per calculation (including data collection) per patient.21 More importantly, they would ensure that these calculations are completed and available in real time.
Implementing CDSSs to calculate nutrition and fluid intake can be accomplished through considerable time and multidisciplinary efforts. The solutions are specific to each hospital and may not be “copied and pasted” from another. EHRs from the same vendor are customized for the needs of each healthcare system and the selected functions and capabilities vary considerably. Barriers to implementation include simultaneous feeding orders, free-text entries, and a large variety of enteral feeding types. These findings, however, are based on observations at two NICUs and may not be generalizable. There is considerable EHR variation, and each EHR may present unique challenges to CDSS implementation.
Several issues remain unresolved. Widespread adoption and interpretation of CDSSs requires standardization of reported values. Even within the same NICU, values were normalized and reported using both the measured and dosing weights, and micronutrients such as phosphate were reported with different units for parenteral and enteral values (Table 1).10 Though the use of each weight was justified, the lack of consistency may hinder interpretation. There are few articles on when to use dosing weights and how to calculate them for infants in the NICU; however, variation in the use has been described.10
Initially, we assumed that implementing CDSSs to calculate nutrition intake for PN and intravenous fluids would be more challenging than enteral feeds. PN and intravenous fluids consist of many individual components that are each adjusted, whereas an enteral feed is ordered whole. Nevertheless, the values of each component and the logic of administration are available to the EHR facilitating calculations. The unrecognized logic of simultaneous enteral feeds and free text, and contribution from modular additives hinder the implementation of CDSSs for enteral intake. These findings may explain why prospective CDSSs for parenteral calories, and fluid are more common than enteral calories and fluid.10
Finally, existing solutions only monitor intake in individual patients. None of the CDSSs described can export calculated intake data from the EHR to monitor the quality of nutrition for all infants or specific populations in the unit (eg, infants with bronchopulmonary dysplasia). Quality improvement requires data that can be systematically aggregated and tracked.
Conclusion
Comprehensive and real-time CDSS for nutrition and fluid intake will require ongoing investment of resources by hospital systems and EHR vendors to address remaining barriers and inefficiencies. We expect that greater access to CDSS will improve nutrition order prescribing, delivery and monitoring, especially during the transition from PN to enteral feeds in high-risk infants and other critically ill populations.7,22,23
Abbreviations
NICU, neonatal intensive care unit; CDSS, clinical decisions support system; EHR, electronic health record; PN, parenteral nutrition.
Acknowledgments
The authors would like to thank Larry Klein and Patrice Swiontek, RD, LDN for their assistance in implementing clinical decision support systems.
Funding
There is no funding to report.
Disclosure
Gustave H. Falciglia has applied for a small business technology transfer grant (STTR) through the National Institute of Health with Medical Predictive Science Corporation (MPSC). The grant is pending, and he does not have a financial relationship with MPSC outside the grant. The other authors report no other potential conflicts of interest in relation to this work.
References
1. Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–2172. doi:10.1016/S0140-6736(12)60820-4
2. Harrison W, Goodman D. Epidemiologic trends in neonatal intensive care, 2007–2012. JAMA Pediatr. 2015;169(9):855–862. doi:10.1001/jamapediatrics.2015.1305
3. Martin CR, Brown YF, Ehrenkranz RA, et al. Nutritional practices and growth velocity in the first month of life in extremely premature infants. Pediatrics. 2009;124(2):649–657. doi:10.1542/peds.2008-3258
4. Stephens BE, Walden RV, Gargus RA, et al. First-week protein and energy intakes are associated with 18-month developmental outcomes in extremely low birth weight infants. Pediatrics. 2009;123(5):1337–1343. doi:10.1542/peds.2008-0211
5. Kumar RK, Singhal A, Vaidya U, Banerjee S, Anwar F, Rao S. Optimizing nutrition in preterm low birth weight infants—consensus summary. Front Nutr. 2017;4:1–9. doi:10.3389/fnut.2017.00020
6. Embleton NE, Pang N, Cooke RJ. Postnatal malnutrition and growth retardation: an inevitable consequence of current recommendations in preterm infants? Pediatrics. 2001;107(2):270–273. doi:10.1542/peds.107.2.270
7. Falciglia GH, Murthy K, Holl JL, et al. Energy and protein intake during the transition from parenteral to enteral nutrition in infants of very low birth weight. J Pediatr. 2018;202:38–43.e1. doi:10.1016/j.jpeds.2018.07.010
8. Ehrenkranz RA, Das A, Wrage LA, et al. Early nutrition mediates the influence of severity of illness on extremely LBW infants. Pediatr Res. 2011;69(6):522–529. doi:10.1203/PDR.0b013e318217f4f1
9. Olsen IE, Richardson DK, Schmid CH, Ausman LM, Dwyer JT. Intersite differences in weight growth velocity of extremely premature infants. Pediatrics. 2002;110(6):1125–1132. doi:10.1542/peds.110.6.1125
10. Falciglia GH, Murthy K, Holl JL, Palac HL, Woods DM, Robinson DT. Low prevalence of clinical decision support to calculate caloric and fluid intake for infants in the neonatal intensive care unit. J Perinatol. 2020;40(3):497–503. doi:10.1038/s41372-019-0546-z
11. Osheroff JA, Teich JM, Middleton B, Steen EB, Wright A, Detmer DE. JAMIA perspectives on informatics a roadmap for national action on clinical decision support. J Am Med Inf Assoc. 2007;14(2):141–145. doi:10.1197/jamia.M2334.Introduction
12. Skouroliakou M, Koutri K, Stathopoulou M, Vourvouhaki E, Giannopoulou I, Gounaris A. Comparison of two types of TPN prescription methods in preterm neonates. Pharm World Sci. 2009;31(2):202–208. doi:10.1007/s11096-009-9281-4
13. Lehmann CU, Conner KG, Cox JM. Preventing provider errors: online total parenteral nutrition calculator. Pediatrics. 2004;113(4):748–753. doi:10.1542/peds.113.4.748
14. Dingley J, Cromey C, Bodger O, Williams D. Evaluation of 2 novel devices for calculation of fluid requirements in pediatric burns. Ann Plast Surg. 2015;74(6):658–664. doi:10.1097/SAP.0000000000000540
15. Pande PS, Neuman RP, Cavanaugh RR. Key concepts of the six sigma system. In: The Six Sigma Way.
16. Bertoni CB, Prusakov P. Clinical decision support to improve dosing weight use in infants with neonatal abstinence syndrome. Pediatr Qual Saf. 2015;4(4). doi:10.1097/pq9.0000000000000184
17. Barfield WD, Papile L-A, Baley JE; American Academy of Pediatrics Committee on Fetus And Newborn. Levels of neonatal care. Pediatrics. 2012;130(3):587–597. doi:10.1542/peds.2012-1999
18. Wyatt JC, Liu JLY. Basic concepts in medical informatics. J Epidemiol Community Health. 2002;56(11):808–812. doi:10.1136/jech.56.11.808
19. Ford E, Oswald M, Hassan L, Bozentko K, Nenadic G, Cassell J. Should free-text data in electronic medical records be shared for research? A citizens’ jury study in the UK. J Med Ethics. 2020;46(6):367–377. doi:10.1136/medethics-2019-105472
20. Musen MA, Middleton B, Greenes RA. Clinical decision support systems. In: Shortliffe EH, Cimino JJ, editors. Biomedical Informatics.
21. Falciglia GH, Murthy K, Holl J, et al. Association between the 7-day moving average for nutrition and growth in very low birth weight infants. JPEN J Parenter Enteral Nutr. 2017:148607117722927. doi:10.1177/0148607117722927
22. Miller M, Vaidya R, Rastogi D, Bhutada A, Rastogi S. From parenteral to enteral nutrition: a nutrition-based approach for evaluating postnatal growth failure in preterm infants. JPEN J Parenter Enteral Nutr. 2014;38(4):489–497. doi:10.1177/0148607113487926
23. Brennan A-M, Fenton S, Murphy BP, Kiely ME. Transition phase nutrition recommendations. J Parenter Enter Nutr. 2017;014860711668628. doi:10.1177/0148607116686289
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.