Back to Journals » International Journal of Nanomedicine » Volume 20
Advances in the Drug Delivery Systems for Psoriasis Topical Therapy
Authors Liu Y ![]() , Chang R, Deng H, Liang F, Xu X, Luo Y
, Chang R, Deng H, Liang F, Xu X, Luo Y
Received 7 April 2025
Accepted for publication 15 August 2025
Published 11 October 2025 Volume 2025:20 Pages 12307—12329
DOI https://doi.org/10.2147/IJN.S529899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Dongwoo Khang
Yang Liu,1,* Ruizhen Chang,2,* Huan Deng,2 Feiqing Liang,2 Xi Xu,2 Yuning Luo2
1Hunan Provincial Key Laboratory of Tumor Microenvironment Responsive Drug Research, Hunan Province Cooperative Innovation Center for Molecular Target New Drug Study, School of Pharmaceutical Science, Hengyang Medical School, University of South China, Hengyang, Hunan, 421001, People’s Republic of China; 2Shenzhen Longgang Second People’s Hospital, Shenzhen, Guangdong, 518112, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xi Xu, Shenzhen Longgang Second People’s Hospital, Shenzhen, Guangdong, 518112, People’s Republic of China, Email [email protected] Yuning Luo, Shenzhen Longgang Second People’s Hospital, Shenzhen, Guangdong, 518112, People’s Republic of China, Email [email protected]
Abstract: Psoriasis (PSO) is an immune-related skin disease featured by rapid and excessive cell growth leading to thick red scaly skin plaques. The main treatment strategy for PSO involves using anti-inflammatory drugs, immunosuppressants, etc, to relieve symptoms, suppress inflammation, and retard the overgrowth and division of skin cells. However, these drugs generally have disadvantages such as poor targeting, short half-life, low bioavailability, significant toxic side effects, etc. which impose a huge physiological and pathological burden on patients. Recently, the use of delivery systems to topical deliver drugs to the damaged psoriatic skin sites has received extensive attention from researchers. These systems promote drug stability, enhance drug penetration, and improve drug efficacies. The continuous development of various multifunctional topical delivery systems provides more therapeutic ideas for the cure of PSO. Based on this, this manuscript reviews the research progress of various delivery systems (including nanoparticles, hydrogels, microneedles, micelles, dendrimers, liposomes, nanoemulsions, vesicles, etc.) for PSO topical therapy and summarizes their development status in clinical treatment. It’s expected to provide reference for the design of novel topical delivery systems and promote the development of PSO therapy methods.
Keywords: psoriasis, drug carrier, drug delivery, topical therapy
Introduction
Psoriasis (PSO) is an immune-related, inflammatory, chronic, systemic disease with 2% ~ 5% incidence rates.1–3 It is characterized by scaly erythema or plaques that may be localized or widely distributed. Many types of PSO exist, including plaque PSO (vulgaris), drip PSO, pustular PSO, and erythrodermic PSO. Patients often have several complications such as arthritis, hypertension, angiocardiopathy, diabetes and depression.4,5 The etiology of PSO is complex, and its occurrence and progression may involve T cell differentiation, inflammatory cell infiltration and proliferation of keratinocytes.6,7 Furthermore, heredity, infection, metabolic disorders, endocrine abnormalities, and other related factors (smoking, drinking, trauma, fatigue, and mental factors) can induce or even aggravate PSO.8–10 Thus, the clinical treatment of PSO is difficult and can recur easily, which seriously affects the quality of life of patients.
The ultimate goal of various treatments is to effectively control symptoms, reduce inflammation, and decrease the frequency of flare-ups. The choice of therapy is mainly related to the development of disease, PSO type, and other individual factors.11,12 If PSO is mild for age and overall health, topical medication is the most common treatment. Medications such as glucocorticosteroids, vitamin D drugs, and keratolytics can alleviate inflammatory cytokines or inhibit immune activation, thereby slowing skin cell growth and reducing symptoms. However, their long-term use may result in side effects such as skin thinning, hyperpigmentation, etc.13 Systemic therapies may be used to treat moderate to severe PSO. Immunosuppressants such as methotrexate and cyclosporine can effectively inhibit cell proliferation and rapidly control the disease; however, their serious nephrotoxicity limits their use. Moreover, many biological agents, such as TNF-α inhibitors (enasip, infliximab, and adalimumab), IL-17A inhibitors (skutecimab and ezekizumab), IL-23 inhibitors (guselchizumab), IL-12/23 inhibitors (ustekinumab), and IL-36R inhibitors (pesolizumab), have also been approved for PSO therapy at home and abroad. They can precisely target and remove inflammatory mediators related to PSO, and most rashes can subside rapidly usually within 1 month.14,15 However, their clinical application is still relatively short, and their long-term safety and efficacy need to be observed. Currently under development, small-molecule targeted drugs mainly focus on PDE4 (apremilast (APR)),16,17 JAK1-3 (tofacitinib and upapatinib),18 and TYK2 (deucravacitinib (DEU)).19 Owing to their different targets and mechanisms of action, there are large differences in the efficacy, safety, and risk of adverse reactions. Moreover, narrow-spectrum medium-wave ultraviolet, a type of physical therapy, can inhibit the overproliferation of skin cells and is more effective in treating plaque-type PSO; however, long-term irradiation increases the risk of skin cancer.20 Thus far, there is still no safe and effective method to cure PSO completely.
Among them, topical medication is the perfect mode of administration because it is non-invasive and has high patient compliance. The skin barrier function of PSO patients is impaired due to increased proliferation and decreased differentiation of keratinocytes, inflammation-related vasodilatation, and increased vascular permeability, which greatly improves the drug permeability and provides a favorable “use environment” for topical drug delivery to the affected area.21,22 However, many topical drugs generally have disadvantages such as short half-life, poor targeting, low bioavailability, significant toxic side effects, etc., make it difficult to achieve the desired therapeutic effect. To solve this problem, the construction of drug delivery systems has become a promising approach.23–26 They can be designed to deliver drugs specifically to PSO lesions, minimize side effects, and achieve controlled or extended release. In addition, they can alter drug pharmacokinetics, prolong the drug circulation time, and improve bioavailability. Researchers have utilized their specific advantages to develop novel formulations to shine in the field of PSO therapy. Therefore, based on the merits and demerits of different drugs for PSO therapy, the latest progress in delivery systems such as nanoparticles (NPs), hydrogels, microneedles (MNs), micelles, dendrimers, liposomes, nanoemulsions, and vesicles for the treatment of PSO has been reviewed (Figure 1). Their research progress in clinical trials in recent years was also summarized. We hope to provide references for the design of novel topical delivery systems for PSO therapy.
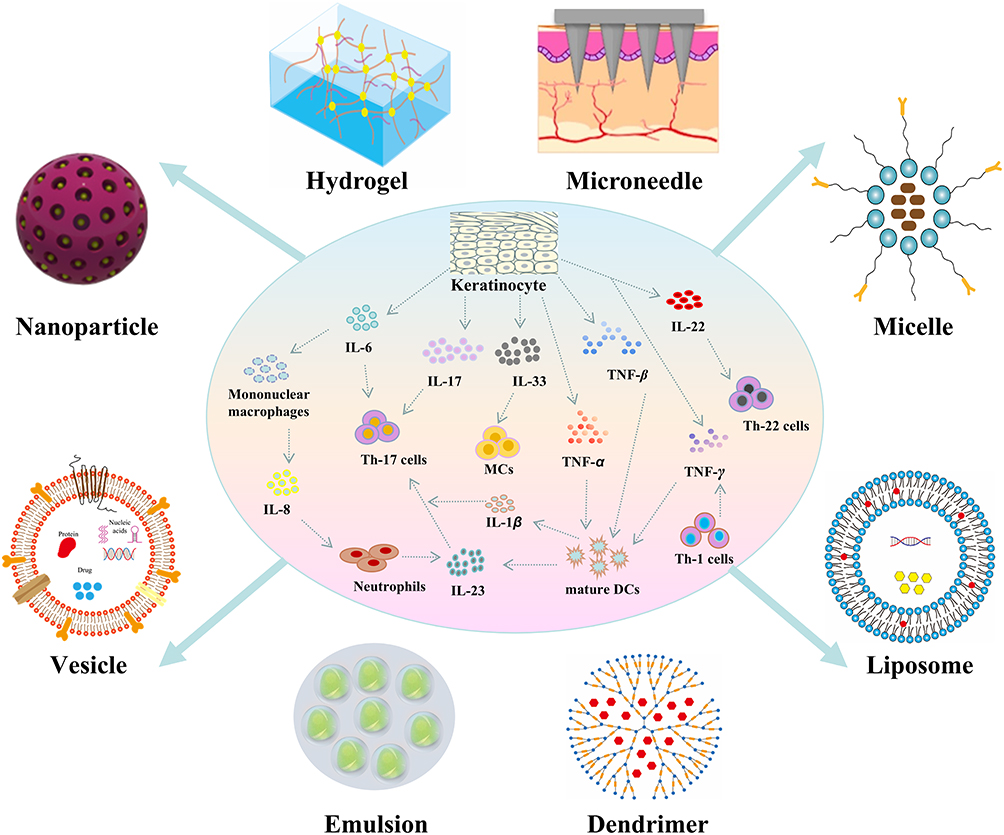 |
Figure 1 Overview of the various drug delivery systems for PSO topical therapy. |
Various Drug Delivery Systems for PSO Topical Therapy
As the research progressed, various types of drug delivery systems played a significant role in the topical treatment of PSO. They effectively enhanced the therapeutic effect of anti-PSO drugs and reduced their side effects. At present, the delivery systems of anti-PSO drugs that have attracted much attention mainly include NPs, hydrogels, MNs, micelles, dendrimers, liposomes, nanoemulsions, vesicles, etc (Figure 1).
Nanoparticles
NPs have significant advantages in drug delivery because of their unique physical properties such as large surface area and small size.27 These properties not only help achieve targeted drug delivery but also achieve controlled drug release. Especially in PSO therapy, NPs are prepared to carry anti-inflammatory ingredients, immunosuppressants, or other small-molecule therapeutic drugs, which could directly act on skin lesions and increase the trans-epidermal uptake efficiency.28,29 This delivery method could improve the route of drugs entering the skin epidermis and promote better drug absorption, thereby significantly improving the therapeutic effect. In addition, NPs can be modified to provide excellent bioadhesion, skin permeability, and specific targeting. Therefore, despite some limitations, such as complex preparation and high cost, and potential delivery inefficiency due to skin barrier status in a few patients, the overall advantages in improving treatment precision and reducing systemic exposure risks of NPs are substantial, providing a safer and more effective treatment scheme for PSO patients.
The team of Deng developed a new local drug delivery system using disease-specific bioadhesive NPs (BNPs) to load the glucocorticoid drug betamethasone dipropionate (BD), aiming to treat PSO with a single dose (Figure 2A).30 In their study, polylactic acid-hyperbranched polyglycerol (PLA-HPG) was self-assembled to synthesize the BNPs. The surface of BNPs contains aldehyde groups, which can form Schiff base links with proteins, giving the nanoparticles great bioadhesion. The modified BNPs, Tris-BNPs, were further obtained by dispersing them in Tris-HCl, which could penetrate the damaged cuticle of PSO and enter the epidermis. After penetration, Tris-HCl would be detached, which would restore the adhesion of BNPs, make it stay in the epidermis for sustained and controlled release of drugs, prolong the action time, and more importantly, do not penetrate healthy skin and reduce adverse reactions. Experiments showed that Tris-BNPs were waterproof and difficult to physically remove, and the symptoms in PSO mice were significantly improved by external administration. Because psoriatic cells highly express proteins, such as LL37, SA0019, and S100A8, which induce PSO recurrence, Xin et al constructed a kind of “antigen-scavenging” NPs (HLNP-MNs) loaded with reactive oxygen species (ROS)-responsive MTX prodrugs and TNF-α-targeted siRNAs.31 HLNP-MNs could absorb PSO-specific proteins and accumulate in the peripheral inflammatory immune cells. They then released active MTX and siRNA in this high ROS microenvironment and exerted a synergistic therapeutic effect on the regulation of immune abnormalities in PSO, providing a highly promising strategy for PSO therapy.
 |
Figure 2 Representative nanoparticle-based delivery systems for PSO topical therapy. (A) The schematic of Tris-BNPs for PSO therapy. Reprinted from Journal of Controlled Release, 349, Mai Y, Ouyang Y, Yu M, et al, Topical formulation based on disease-specific nanoparticles for single-dose cure of psoriasis, 354–366, Copyright 2022, with permission from Elsevier.30 Copyright 2022, Elsevier. (B) The schematic of HA@CS-GA NPs for PSO treatment mediated by CD44 receptor. Reprinted from Environmental Research, 238, Sheikh A, Hazari SA, Molugulu N, et al, Hyaluronic acid engineered gallic acid embedded chitosan nanoparticle as an effective delivery system for treatment of psoriasis, 117086, Copyright 2023, with permission from Elsevier.32 Copyright 2023, Elsevier. (C) The schematic of MTX@HMN-Ce6-HA NPs for PSO treatment. Reprinted from Chemical Engineering Journal, 490, Fan Z, Zhao G, Gan Y, et al. Synergistic chemo-photodynamic therapy based on hollow mesoporous organosilica nanoparticles for reducing psoriasis-like inflammation, 151613, Copyright 2024, with permission from Elsevier.33 |
NPs can also be surface modified for specific targeted delivery. Since the hyaluronic acid (HA) receptor CD44 is overexpressed in the skin of patients with PSO, several research teams have modified NPs with HA for active targeting.34,35 The obtained HA-mediated transdermal delivery systems should exhibit enhanced permeability and targeted drug inhibition. Lee and coworkers designed HA-based NPs (HA-NPs) through self-assembly of hydrophobic lithocholic acid-modified HA.36 Subcutaneous injection of HA-NPs protected psoriatic mice from PSO-like dermatitis induced by imiquimod (IMQ), and the Psoriasis Area Severity Index (PASI) was remarkably reduced. Importantly, HA-NPs effectively treated PSO-like dermatitis by suppressing the natural immune response and repairing the barrier function of the skin; the therapeutic effect was dose-dependent, with no obvious signs of toxicity. Additionally, Chen and coworkers designed chitosan (CS)/HA nanoparticles (CHALT) loaded with alantolactone and explored their potential therapeutic effects on PSO.37 It has been confirmed that CHALT could effectively inhibit cell proliferation by inducing apoptosis mediated by ROS and restraining the activation of Signal Transducer and Activator of Transcription 3 (STAT3) signaling and inflammatory reaction caused by IL-6 in human immortalized keratinocytes (HaCaT cell line). In the PSO model induced by IMQ, local treatment of PSO lesions with CHALT effectively reduced the overactivation of STAT3 and immune cell recruitment, thus improving PSO symptoms. Moreover, Sheikh et al32 constructed a type of HA-based NPs (HA@CS-GA NPs) through the modification of gallic acid (GA)-loaded CS NPs with HA to enhance the anti-inflammatory efficacy of PSO therapy (Figure 2B). The NPs could target diseased keratinocytes via HA-CD44 receptor interactions, and the antiproliferative activity of the NPs on HaCaT cells was greatly enhanced compared to that of free GA, which was attributed to their pH-responsive release properties and enhanced cellular uptake efficiency. In an in vivo PSO model, this system significantly inhibited epidermal thickening and downregulated the proportion of Ki67-positive cells, while suppressing the expression of pro-inflammatory factors through the NF-κB pathway. This mechanism of targeted delivery and multipathway regulation provides an innovative strategy for the treatment of PSO, and its biocompatibility and CD44-targeting properties make it a promising candidate for clinical translation.
In addition to polymer-based NPs, NPs formed from metal or nonmetal atoms can also deliver anti-PSO drugs. Fan et al designed HA, MTX, and Ce6 loaded hollow mesoporous silica NPs (MTX@HMN-Ce6-HA).33 These NPs could produce ROS in light, which disrupts internal disulfide bonds to release MTX and HA and enhance permeability. They further decreased HaCaT cell viability, induced apoptosis, and reduced inflammation by modulating the STAT3-NF-κB p65 pathway. The combination of MTX chemotherapy and Ce6 phototherapy had a synergistic therapeutic effect on PSO (Figure 2C). Han et al38 developed a self-therapeutic gold nanoparticle with a 3 nm gold core and an octadecyl-modified polyethylene glycol (PEG) shell. In the IMQ-induced PSO mice, these NPs were able to penetrate the stratum corneum and enter the keratinocytes preferentially. After 4 days of treatment, the mice showed reduced skin inflammation, less scaling and hardening, and smoother skin, which were superior to those treated with vitamin D analogs. In addition, NPs downregulated genes related to the interleukin-17 signaling pathway, with no significant side effects. Moreover, Zhang et al39 prepared a type of platinum-doped carbon dots with positive charges for PSO therapy. In the IMQ-induced PSO mouse model, they could clear free extracellular DNA, reduce skin inflammation, suppress overactivation of the cGAS-STING pathway, and recover from internal skin environment homeostasis, thereby showing favorable therapeutic effects. These studies suggested that these NPs integrated with multiple therapeutic modalities such as chemotherapy, phototherapy, and immunomodulation, offer a collaborative PSO therapeutic strategy, show casing their significant potential for clinical application.
Hydrogels
Hydrogels, which are smart polymer materials with three-dimensional crosslinked network structures, can be efficiently loaded with biologically active molecules (siRNA, antibody fragments, etc.) and hydrophilic/hydrophobic drugs through physical/chemical interactions to construct a multidrug co-delivery system. This integrated design overcomes the limitations of single therapeutics and realizes the synergistic effects of gene silencing, immunomodulation, and targeted drug release.40–44 In addition, its dynamic network structure provides dual advantages, such as reversible crosslinking to form an adhesive protective film for prolonged skin permeability of the drug, and solubilization properties in response to microenvironmental changes (pH/enzyme concentration) for controlled release. This sustained delivery mode has attracted considerable attraction in the therapeutic field because it is suitable for PSO with chronic recurrence and significantly reduces the dosing frequency.45,46
The key to breaking the bottleneck of PSO treatment is the development of a preparation with high permeability and viscosity that can increase the degree of drug retention on the skin surface. Yao et al47 invented the first water-responsive hydrogel (WRG) from glyceryl dioleate (GDO) and phosphatidyl choline (PC), which has the unique characteristics of a water-induced sol-gel transition. When there was no water, it was in the solution state, and when water was added, it immediately became a hydrogel. A potent anti-PSO drug curcumin (Cur) with immunomodulatory, anti-inflammatory, and antibacterial properties was successfully loaded into WRG and realized sustained drug release (Figure 3A). The WRG preparation (CUR-WRG) not only prolonged the residence time in the skin but also promoted drug penetration. It inhibited the hyperproliferation of psoriatic skin by reducing the expression of Ki67 and CK10 in the PSO model. Lai et al48 constructed a novel hydrogel system (TYK2i-BO-gel) in which skin permeability was enhanced by the introduction of borneol (BO) to effectively deliver the tyrosine kinase 2 inhibitor (TYK2i) into the deeper skin layers at the site of inflammation (Figure 3B). This delivery system was found to significantly suppress the Th17 immune response by inhibiting antimicrobial peptide (AMPs) expression and modulating the STAT3 pathway, with efficacy comparable to that of glucocorticoids, and with a lower relapse rate. Its clinically approved drug combinations and robust, scalable manufacturing process offer potential for monotherapy or adjunctive therapy conversion, particularly for patients with drug-resistant lesions and high relapse rates. Additionally, Fan et al designed a kind of cationic hydrogels from hyperbranched dendritic-linear-dendritic-linear copolymers (HBDLDs).49 The hydrogel not only showed good antibacterial activity, but also induced the expression of RNase 7 and PSO-associated substances, which enhanced host-mediated bacterial clearance. This material significantly reduced the mitochondrial ROS level, IL-1β and reactive nitrogen in HaCaT cells, which synergistically reduced the inflammatory response through multiple pathways.
 |
Figure 3 Representative hydrogel-based delivery systems for PSO topical therapy. (A) The schematic of a novel CUR-WRG gel for topical delivery of curcumin for PSO therapy. Reproduced with permission from Yao Q, Zhai YY, He Z, et al. Water-responsive gel extends drug retention and facilitates skin penetration for curcumin topical delivery against psoriasis. Asian J Pharm Sci. 2023;18(2):100782. Creative Commons.47 (B) Schematic representation of a novel TYK2i-BO-gel preparation for topical delivery of TYK2i. Reproduced with permission from Lai Y, Wu X, Jiang Z, et al. Topical treatment of tyrosine kinase 2 inhibitor through borneol-embedded hydrogel: evaluation for preventive, therapeutic, and Recurrent management of psoriasis. Bioact Mater. 2024;41:83–95. Creative Commons.48 (C) Schematic representation of CS-HANGs co-delivering MTX and ALA for combined chemotherapy and photodynamic therapy of PSO. Reprinted from Carbohydrate Polymers, 277, Wang Y, Fu S, Lu Y, et al. Chitosan/hyaluronan nanogels co-delivering methotrexate and 5-aminolevulinic acid: a combined chemo-photodynamic therapy for psoriasis, 118819, Copyright 2022, with permission from Elsevier.50 |
Recently, researchers developed a novel MTX delivery system from thermosensitive hydrogel in combination with gold nanorods (GNRs).51 Its sol-gel transition enhanced its permeability and increased the retention time of MTX on the skin. And the photothermal conversion capability of GNRs could induce apoptosis of keratinocyte cells and promote MTX release under NIR irradiation. In the PSO mice model, the system demonstrated efficacy comparable to commercially available ointments without skin wrinkling, providing a more precise and efficient solution for PSO treatment. Moreover, nanogels, which combine the advantages of both NPs and hydrogels, have also attracted significant attention for PSO therapy. Therefore, Wang et al designed a type of nanogels by combining the cellular uptake-enhancing ability of CS and the internalization effect of HA to achieve the targeted delivery of MTX and 5-aminoleavulinic acid (ALA) in PSO therapy (Figure 3C).50 The gels promoted the penetration of MTX and ALA into the epidermis. Under light exposure, they can produce ROS and undergo synergistic antiproliferation and apoptosis in lipopolysaccharide (LPS)--stimulated HaCaT cells with MTX. They also showed a significant anti-PSO effect in IMQ-induced mice.
Microneedles
Microneedles (MNs) are a type of composite delivery system composed of hundreds of small needle tips with a length of 25 ~ 1000 μm in the form of an array.52,53 The active ingredient can be loaded into the MN array and the concentration gradient inside and outside is the driving force for release. This enables it to cross the stratum corneum in a targeted manner without having to pass through the stratum corneum to participate in microcirculation and exert pharmacological responses. MN-based drug delivery is convenient, self-administered, and the rate of transdermal absorption is stable As we all know, the skin lesions of PSO patients are relatively thick, which is critical to deliver drugs, while MN therapy can penetrate the stratum corneum, circumventing the step of penetration required for topical drugs, and achieve the purpose of sustained, precise and long-term relief of symptoms. Furthermore, MN may have imaging, diagnostic, and therapeutic capabilities that can help assess the severity of PSO and guide treatment. Recently, MNs have demonstrated good potential for transdermal drug delivery in dermatologic therapy. Research has been focused on improving their component, structure, and function for smart drug delivery.54,55
Li et al56 constructed an MN for BD delivery by introducing BD-loaded zinc-doped mesoporous silica nanoparticles (Zn-MSNs) into a methacrylated gelatin hydrogel. MN had a high efficiency of transdermal delivery and could realize the sustained release of BD and Zn2+, which could promote macrophage polarization toward the M2 phenotype, inhibit pro-inflammatory factor expression, and enhance the anti-inflammatory effect compared with BD cream in PSO therapy. On the other hand, oxidative stress is closely associated with ROS overproduction.57,58 Elevated ROS levels in the skin constitute both therapeutic targets and endogenous triggers. Based on this, Bi et al constructed an ROS-responsive MN patch with simultaneous delivery of the antiproliferative drug MTX and the ROS-scavenging drug epigallocatechin catechin (EGCG) through crosslinking between EGCG and phenylboronic acid-modified HA for combination therapy with PSO.59 It was found that the MN had a stepwise drug release property combining ROS-responsive EGCG release and rapid MTX release, and the released drugs could effectively inhibit NF-κB inflammatory pathway by scavenging ROS. In addition, compared with soluble non-crosslinked MN, MN resided in the skin for an extended period, which is conducive to the long-term management of PSO.
The targeted and precise delivery properties of MNs make them uniquely suited for the treatment of PSO. Zhou and coworkers designed a CD44-targeted ROS-responsive delivery system in which an MTX precursor (MTX-TK-HA) was assembled with poly(lactic acid)-methoxy PEG (PLA-mPEG) and loaded onto an HA-based soluble MN (Figure 4A).60 This system actively targeted hyperproliferative keratinocytes via CD44 receptors and penetrated the epidermis to a depth of 210 μm. Upon ROS stimulation, MTX prodrug releases active MTX, which blocks the NF-κB pathway, inhibits epidermal cell proliferation, and alleviates inflammation. MN enables precise transdermal delivery while maintaining the biocompatibility of the nanocomponents, providing an innovative strategy for PSO treatment. While Dan et al61 also designed an HA-based MN patch containing IL-17 and MXene using micromolding technology. MN has excellent mechanical strength and biocompatibility, which minimize the immune response. Under irradiation, MN rapidly melts and leads to IL-17 release, owing to the photothermal conversion ability of MXene. It effectively reduced PSO-like inflammation in an IMQ animal model, inhibited lesion deterioration, reduced the systemic dose, and provided excellent therapeutic efficacy for the treatment of PSO. In addition, to enhance the targeting capability, a selected macrophage membrane with the ability to target multiple inflammatory factors in PSO was combined with etomoxir and MN.62 It was shown that this system performed better in attenuating PSO symptoms and inhibiting relapse than CPT.
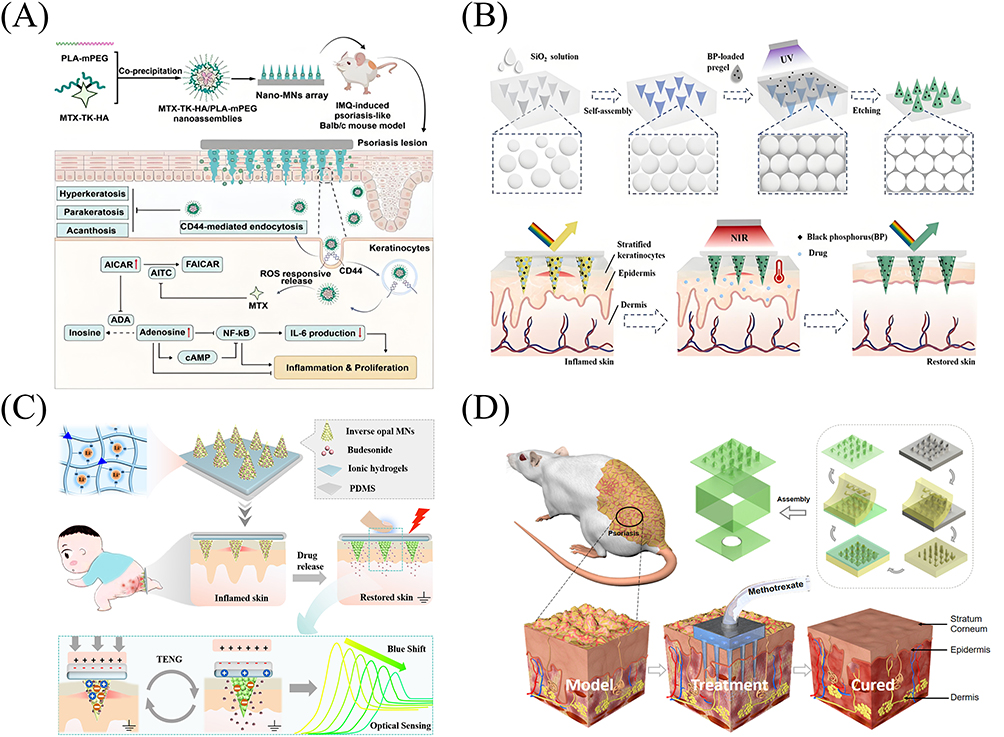 |
Figure 4 Representative microneedle-based delivery systems for PSO topical therapy. (A) The schematic of MTX-TK-HA/PLA-mPEG nanocomposition for painless transdermal delivery in PSO treatment. Reproduced with permission from Zhou Y, Yang L, Lyu Y. Topical delivery of ROS-responsive methotrexate prodrug nanoassemblies by a dissolvable microneedle patch for psoriasis therapy. Int J Nanomed. 2023;18:899–915. Creative Commons.60 (B) Schematic of the synthesis of BP-loaded hydrogel MN for PSO therapy and drug delivery monitoring. Reprinted from Nano Today, 54, Lu M, Zhang X, Cai L, et al. Black phosphorus hydrogel inverse opal microneedle patches for psoriasis treatment, 102072, Copyright 2024, with permission from Elsevier.63 (C) Schematic diagram of a multifunctional color-structured triboelectric MN patch for PSO treatment. Reprinted from Matter, 6/5, Wang Y, Zhang X, Chen G, Lu M, Zhao Y. Multifunctional structural color triboelectric microneedle patches for psoriasis treatment, 1555–1568, Copyright 2023, with permission from Elsevier.64 (D) Preparation of a three-dimensional structured HMN for PSO treatment. Adapted with permission from Detamornrat U, McAlister E, Hutton ARJ, Larrañeta E, Donnelly RF. The role of 3d printing technology in microengineering of microneedles. Small. 2022;18(18):2106392. Creative Commons.65 |
Moreover, the imaging capabilities of MNs can be used for monitoring and diagnostics, as well as for studying drug pharmacokinetics. Lu et al63 constructed a hydrogel MN consisting of a black phosphorus (BP)-loaded N-isopropylacrylamide (NIPAM)/poly(ethylene glycol) diacrylate (PEGDA) inverse opal scaffold and drug-loaded gelatin/agarose fillers in the scaffold pores for the PSO treatment (Figure 4B). Because of the photothermal conversion ability of BP, the thermoresponsive contraction property of NIPAM, and the thermoresponsive gelatin, the resulting MNs possessed good hydrophobic drug-carrying capacity and photothermally controllable release. In addition, owing to the optical properties of the inverse opal structure, the MN exhibited bright structural colors and produced a characteristic wavelength shift that enabled real-time drug monitoring. Wang et al prepared a colorful triboelectric MN patch-targeted delivery system based on an ionic hydrogel with inverse opal structures (PAM-PEGDA-LiCl) (Figure 4C).64 The system encapsulates budesonide at the tip of the MN and utilizes the charge produced by friction to achieve electrostatic repulsion to drive drug release. Experiments showed that in IMQ-induced PSO model mice, this MN patch promoted angiogenesis through mechanical friction, while the dynamic charge change regulated the drug release rate, effectively alleviating the rising trend of the skin lesion area and the PASI score. The inverse opal structure of the MN patch gave the patch structural color properties (reflective peak wavelength of 580 nm), which allowed real-time drug release monitoring through color changes, providing visual feedback for PSO treatment.
The emergence of 3D printing technology has significantly boosted the use of MNs in the biomedical field.66 Its versatility, design flexibility, ease of customization, and high complexity not only enhance the drug delivery effect of MNs but also provide more possibilities for new applications of MNs beyond drug delivery.67–69 For the first time, researchers successfully prepared hollow MNs (HMNs) with different morphologies, heights, and inner and outer diameters using high-precision 3D printing technology (microArch S240) (Figure 4D).65 In addition, the substrate material can be adjusted to be flexible or rigid, as needed, and its thickness can be flexibly adjusted. In a mouse model of PSO, similar efficacy was achieved by hollow MN administration using only 1/10 of the oral dose, showing better anti-PSO effects than oral drugs. Another group utilized continuous liquid interface production printing to fabricate MN array patches (MAP-MNs) of different shapes loaded with BD formulations for PSO treatment.70 It was found that obelisk-shaped MAP-MNs had better durability than other shaped MAP-MNs did. When combined with an oleogel-based BD formulation, the amount of BD that penetrated the skin significantly increased with increasing MN length, and the anti-PSO effect was more pronounced.
Micelles
A micelle contains a lipophilic nucleus for encapsulating drugs and a hydrophilic shell, which can interact with cells and proteins to influence pharmacokinetics and distribution, thus controlling delivery inside the body.71,72 The special external structure and small size of micelles make them less likely to interact with plasma and tissues, and allow them to remain for long periods without being recognized by proteins and phagocytes, thus protecting the drug from the external environment. In addition, micelles can improve drug targeting and reduce side effects associated with systemic absorption. Based on these characteristics, micelles have significant advantages in the treatment of PSO.73 Studies have confirmed that micelles can effectively deliver PSO medications, such as APR, DEU, and calcipotriol (CPT), to enhance their skin penetration and target therapeutic effects.
APR can inhibit phosphodiesterase 4, and is an effective drug against PSO. Nevertheless, weak oral bioavailability, coupled with side effects, has severely limited its utility in clinical setting.74,75 Therefore, Sontakke and coworkers designed a hybrid micellar gel (HMMG) for topical APR delivery (Figure 5A).76 The micelles prepared by this system had an mean dimension of 83.59 ± 4.46 nm, an encapsulation rate of 94.78 ± 3.98%, a drug loading capacity of 11.37 ± 3.14%, a 38-fold increase in deep skin retention compared with the traditional formulation, and an efficacy superior to that of betamethasone valerate at 0.1% with no irritation, which provided a new strategy for anti-PSO drug delivery.
 |
Figure 5 Representative micelle/dendrimer-based delivery systems for PSO topical therapy. (A) Hybrid micelles of a fatty acid-surfactant concatenate (HMMG) for topical delivery of APR for PSO therapy (** = p < 0.01). Reprinted from International Journal of Pharmaceutics, 655, Sontakke A, Dighe S, Sharma R, Yadav V, Jain S. Harnessing the potential of fatty acid-surfactant-based micellar gel for enhanced topical delivery of apremilast in psoriasis treatment, 124026, Copyright 2024, with permission from Elsevier.76 (B) Schematic of the Car@Deu@PEPS supermolecular micelles with ROS scavenging capability for PSO therapy. Reproduced with permission from Yao L, Tian F, Meng Q, et al. Reactive oxygen species-responsive supramolecular deucravacitinib self-assembly polymer micelles alleviate psoriatic skin inflammation by reducing mitochondrial oxidative stress. Front Immunol. 2024;15:1407782. Creative Commons.77 (C) Schematic of the dendritic polymer (13cRA-D) for controlled transdermal delivery of isotretinoin for the treatment of PSO. Reproduced from Zhao T, Zhou M, Wu R, et al. Dendrimer-conjugated isotretinoin for controlled transdermal drug delivery. J Nanobiotechnology. 2023;21(1):285. http://creativecommons.org/licenses/by/4.0/.78 Copyright 2023, Springer Nature. (D) A bifunctional polymer with efficient delivery of cell membrane proteins and Cas9 RNP for PSO treatment. Reproduced with permission from Tan E, Wan T, Pan Q, et al. Dual-responsive nanocarriers for efficient cytosolic protein delivery and CRISPR-Cas9 gene therapy of inflammatory skin disorders. Sci Adv. 2024;10(16):eadl4336. http://creativecommons.org/licenses/by/4.0/.79 |
Moreover, DEU is a potent oral TYK2 inhibitor for PSO therapy.80,81 However, it is difficult for a single therapy to fully address the complexities of PSO, including ROS overload and persistent inflammation. To address the limitations of DEU therapy, Yao et al constructed a supramolecular micelle (Car@Deu@PEPS) to encapsulate DEU using PEG block-polypropylene sulphide (PEG-b-PPS) block copolymers, which exhibited anti-inflammatory effects by repairing mitochondrial DNA function in a TNF-α/IL-17A-induced HaCaT cell model, prolonged dermal retention time, and inhibition of NLRP3 inflammatory vesicle-mediated cellular charring in the IMQ-induced PSO model, with a higher safety profile and patient compliance than oral formulations (Figure 5B).77 These innovative delivery systems offer safer and more efficient solutions for PSO treatment.
In addition, Hua et al designed an ROS-responsive nanomicelles transdermal delivery system from CPT-loaded methoxypolyethylene glycol-thioether-thiol (mPEG-SS).82 This system significantly promoted CPT transdermal penetration by enhancing drug stability and targeting. The presence of the thioether bonds enabled the nanomicelles to dissociate in the presence of high level of GSH, thereby accelerating the release of CPT. Small animal imaging system monitoring verified that the endogenous ROS specifically triggered CPT release from these micelles, which exhibited excellent inhibition of inflammation in the IMQ-induced PSO model, verifying their potential application in PSO treatment.
Dendrimers
Dendrimers are hyperbranched polymers with unique structures and controllable physical and chemical properties.83–86 These molecules have a stable single-molecule structure and well-defined number of surface functional groups that can be modified to target ligands, and their internal cavities can encapsulate hydrophobic small-molecule drugs. Dendritic macromolecules can easily penetrate cell membranes, thereby increasing drug uptake efficiency. In addition, owing to their controllable structure and modification ability, dendrimers can regulate drug release, protect them from damage, achieve slow release and targeted delivery, and play an essential role in transdermal delivery systems. Dendrimers such as dithranol, isotretinoin, and nucleic acids have been shown to be effective in delivering PSO therapeutics.
The teratogenic side effects of isotretinoin make it a nonfirst-line treatment for PSO. Reducing its side effects and enhancing its permeability are urgent issues to be addressed. Therefore, Zhao et al78 developed a novel self-assembled dendrimer conjugate system (13cRA-D) by connecting isotretinoin to a PEG-based tetra-branched dendrimer with an ester bond, specifically for the transdermal delivery of isotretinoin, to enhance its efficacy in local dermatological treatments, especially for PSO (Figure 5C). This study found that the release characteristics of 13cRA-D were significantly pH-sensitive, with fast release in the low-pH environments of inflamed tissues. This controlled-release action helped reduce non-teratogenic side effects and promoted effective penetration into the skin. Additionally, compared to free isotretinoin, 13cRA-D showed excellent therapeutic effects in the PSO model. Notably, the skin irritation caused by 13cRA-D was minimal, indicating that the system not only improved therapeutic efficacy, but also improved patient safety and comfort. Meanwhile, the group of Tripathi utilized the microsponge gel made of Generation-4 (G4) poly(amido) amine (PAMAM) dendrimers for dithranol delivery.87 It was stable and nonirritating for dermal application. Pharmacokinetic studies demonstrated that it prolonged the dermal penetration time of dithranol, with effects comparable to those of commercially available formulations, showing good potential for the treatment of PSO.
Protein drugs are valued for their high efficacy, selectivity, and low side effects; however, their inability to penetrate cell membranes limits their effective action on intracellular targets. Tan et al developed a novel dual-responsive dendrimer library (GBLA) by grafting different amounts of lipoic acid (LA) and phenylboronate (GB) ligands onto G5 polyamidoamine dendrimers. These dendrimers effectively delivered proteins, enzymes, monoclonal antibodies, and Cas9 RNP to the cytoplasm (Figure 5D).79 GB can coordinate with lysine or histidine residues on proteins via boronate nitrogen to stabilize the polymer/protein complex, successfully delivering Cas9 ribonucleoprotein to the NLRP3 inflammasome and improving inflammation. LA, with its amphiphilicity, can produce disulfide bonds with free thiols on the surface of cells, promoting endocytosis and releasing protein drugs. GBLA-22, the most efficient Cas9 RNP delivery carrier, significantly downregulated the expression of PSO-related inflammatory cytokines and improved PSO symptoms in mice via the genome editing of NLRP3. This study provides new strategies for cytoplasmic protein delivery, demonstrating the potential of dendrimers to significantly enhance cytoplasmic protein delivery efficiency, while retaining drug activity in PSO therapy.
Liposomes
Liposomes with lipid-based nanobilayer structures are widely recognized as drug carriers because of their excellent biodegradability, biocompatibility, and immunogenicity.88,89 Liposomes can potentiate solubility, modulate dissemination, and provide flexible surface modifications to facilitate targeted slow release of drugs. They are typically used for pharmaceutical encapsulation, rendering them suitable for drug delivery via multiple pathways. Liposomal therapy for PSO is a form of dermal drug delivery that increases the local concentration and duration of action of drugs in the skin.90 Therefore, the scientific and rational design and precise and efficient fabrication of liposomes are undoubtedly of great significance for enhancing the therapeutic effect of PSO and improving the quality of life of patients.
Liposomes played an important role in the delivery of Cur, which significantly improved the therapeutic efficacy and bioavailability of Cur in PSO treatment. For instance, Yu and coworkers prepared a peptide-modified liposome (CRC-TD-Lip) loaded with Cur to enhance its anti-PSO effect.91 CRC-TD-Lip was characterized by uniform preparation, high stability, and a high encapsulation rate of Cur. The peptide modification altered the structure of the stratum corneum, so that CRC-TD-Lip could rapidly penetrate the skin barrier and efficiently deliver Cur to the affected area. The results shown that this system significantly improved intracellular uptake and increased transdermal ability. In the IMQ-induced PSO model, the CRC-TD-Lip exhibited enhanced anti-PSO effects. To further improve the permeability of Cur, Lu et al92 successfully prepared a Cur-based ionic liquid liposome (Cur-Bet-IL-Lip) (Figure 6A). This system integrates the properties of Cur, ionic liquids, and liposomes and has good stability and biocompatibility. It effectively penetrated the skin stratum corneum and delivered Cur to dermis and epidermis within 24 h, with a cumulative penetration rate of 49% and a significantly higher uptake capacity in HaCaT cells. The liposomes also significantly reduced the expression of inflammatory factors and increased the expression of collagen-I, implying that the system significantly enhanced the permeability and solubility of difficult-to-solubilize drugs, which opens up new possibilities for the clinical application of Cur.
 |
Figure 6 Representative liposome/nanoemulsion-based delivery systems for PSO topical therapy. (A) Schematic of the Cur-based Cur-Bet-IL-Lip ionic liquid liposomes for PSO therapy. Reproduced with permission from Lu B, Zhang J, Zhang J. Enhancing transdermal delivery of curcumin-based ionic liquid liposomes for application in psoriasis. ACS Appl Bio Mater. 2023;6(12):5864–5873.92 Copyright © 2023 American Chemical Society. (B) Schematic of the liposomes integrated HA-based MNs for PSO therapy. Adapted with permission from Qu F, Sun Y, Bi D, et al. Regulating size and charge of liposomes in microneedles to enhance intracellular drug delivery efficiency in skin for psoriasis therapy. Adv Healthc Mater. 2023;12(31):2302314. © 2023 Wiley-VCH GmbH.93 (C) Schematic of the nanoemulsion-based gel for improving the skin permeability of fluticasone propionate. Reprinted from Journal of Drug Delivery Science and Technology, 84, Jain S, Pattewad V, Bhargavi N, et al. Exploring the therapeutic potential of functional excipient-based nanoemulgel of fluticasone propionate for the management of psoriasis, 104435, Copyright 2023, with permission from Elsevier.94 (D) Schematic of the novel foam nanoemulsion for PSO treatment. Reproduced with permission from Ma X, Bian Q, Xu Y, et al. Foamed microemulsion nanodroplets loaded with chlorin e6 for epidermal-targeted treatment against psoriasis. Nano Res. 2024;17(11):9920–9931. https://link.springer.com/article/10.1007/s12274-024-6916-7. Copyright 2024, Springer Nature.95 |
In addition, Qu et al investigated the effects of the charge and size of liposomes on the efficiency of pharmaceutical delivery to skin cells (Figure 6B).93 They prepared liposomes with different particle sizes and charges, and integrated them into HA-based MNs. The results showed that liposomes of appropriate size (250 nm) and stronger positive charge significantly improved the duration of stay of dexamethasone (dex) in the skin, thus increasing treatment efficacy. It was hypothesized that the treatment mechanism of liposomes in PSO may be related to their ability to improve skin barrier function, reduce the release of inflammatory mediators, and modulate the immune system. Liposomes contributed to more effective control of PSO symptoms by enhancing the local concentration of dex in the skin. However, the long-standing safety and optimal dosing strategy of liposomes for PSO therapy still needs to be further investigated. Recently, Zhang et al96 constructed a type of HA-modified propylene glycol-based liposomes (HA-ES) for topical administration of Cur. In this system, surface HA formed a gel network, which reduced Cur leakage and improved its stability. Compared with normal alcohol plasmid (ES) and Cur/propylene glycol solution (PGS), HA-ES significantly enhanced the transdermal penetration of Cur by 1.6 and 1.4 times, and increased the transdermal volume and skin retention after 8 h by 3.1 and 3.3 times, respectively. After treatment with Cur-loaded HA-ES in the PSO model, the most pronounced relief of inflammatory symptoms was observed, with a significant reduction in skin inflammatory factors. This study demonstrated that HA-modified propylene glycol-based hybrid liposomes with high deformability and targeting properties could deliver drugs to inflamed skin tissues with high CD44 expression and boost the curative effect at the lesion site.
Nanoemulsions
Nanoemulsions are stable and transparent dispersion systems consisting of a water phase and an insoluble oil phase with droplet sizes between 5 and 200 nm stabilized by surfactants.97,98 In PSO therapy, nanoemulsions offer significant advantages over conventional emulsions, avoiding stability problems, such as flaking, delamination, deposition, and coarsening, while significantly improving drug permeability and loading capacity to enhance therapeutic efficacy.99 Through formulation design and ingredient screening, nanoemulsions provide a safer and more effective delivery system for anti-PSO drugs, such as tacrolimus, methotrexate, and glucocorticoid analogs, to enhance skin penetration and therapeutic efficacy.
Rai et al100 crafted a new nanoemulsion loaded with azelaic acid and tacrolimus (ATNEG) from vitamin E oil and soy lecithin to boost the local drug bioavailability and effectiveness against PSO. This was achieved by optimizing the droplet size, ensuring its uniform distribution, and controlling its viscosity, all of which enhanced the topical drug availability and efficacy. Its pH is close to the natural pH of the skin and it exhibits desirable topical application properties. Moreover, the emulsion exhibited a controlled drug release pattern with long-term penetration of over 24 h. This characteristic is expected to ensure the continuous availability of drugs for skin absorption. In contrast to commercially available tacrolimus ointment, this emulsion enabled longer-lasting and higher levels of skin drug accumulation. Jain and coworkers designed a nanoemulsion gel to improve the skin permeability of fluticasone propionate (Figure 6C).94 The nanoemulsion gel, which consisted of fluticasone propionate, negentropic gel, and Aloe vera gel, showed synergistic effects in achieving long-term PSO relief. These results also indicate that it enhanced skin permeability. It was found to increase the retention of fluticasone propionate in deep skin to nearly four times the previous level. In vivo tests showed a better anti-PSO effect of the nanoemulsion gel than that of a commercially available formulation. In addition, Rashid et al101 successfully developed an MTX and olive oil-based nanoemulsion (MTX NEG) for the PSO treatment. Through continuous optimization, the nanoemulsion exhibited better dimensions and polydispersity index, and its embedding efficiency reached 76.57 ± 2.48%. After 24 h, the MTX penetration could reach 70.78 ± 5.8 μg/cm². In a rat PSO model, the PASI reduction effect of MTX NEG was comparable or even superior to that of MTX tablets, reaching a 91% reduction. Olive oil-based MTX-NEG may be a therapeutic approach for PSO and reduce the remission of PSO-like symptoms.
Recently, Ma et al95 prepared a foamed nanoemulsion containing photosensitizer Ce6 (Ce6 FM) (Figure 6D). When applied to the skin, Ce6 could penetrate the cuticle and remain in the epithelial layer, enabling targeted delivery to the abnormally proliferating keratinocytes in the epidermis. Laser irradiation efficiently generated intracellular ROS, induced apoptosis in HaCaT cells, and promoted the expression of cyclooxygenase-2 (COX2), thus regulating the over-immune state of the skin while inhibiting the proliferation of keratinocytes. In healthy mice, no skin irritation features, such as redness and swelling, were observed, indicating that this was a safe and effective method for PSO therapy.
Vesicles
Vesicles are nonionic surfactant-based drug delivery systems that confine hydrophilic drugs to the core region and hydrophobic portion of the surface bilayered structure, allowing controlled and targeted drug delivery.102,103 Vesicles of different origins (eg, nanovesicles, outer membrane vesicles, and exosomes) play vital roles in intercellular communication, inflammation regulation, and immunomodulation. In particular, many studies have verified that extracellular vesicles (EVs) extracted from mesenchymal stem cells (MSCs) have therapeutic potential for PSO, owing to their potent immunomodulatory and anti-inflammatory effects.104,105
Zhang et al106 extracted a kind of Evs (IFNγ-sEVs) from human umbilical cord MSCs through the induction of IFN-γ (Figure 7A). Their experiments demonstrated that IFNγ-sEVs inhibited the growth of keratin-forming cells and alleviated the symptoms of PSO lesions. The researchers further loaded ASO-210, an antisense nucleotide drug of miR-210, into IFNγ-sEVs via electroporation to improve drug stability and delivery efficiency, and reduce toxic side effects. In vivo experiments showed that they could effectively alleviate PSO symptoms and synergistically treat PSO through immunomodulation and the targeted delivery of ASO-210. In addition, researchers have developed a method for bulk extraction of outer membrane vesicles (Pg OMVs) from Parabacteroides goldsteinii (Figure 7B).107 The investigation revealed that when Pg OMVs were orally administered, they crossed the intestinal barrier and reached the inflamed skin of PSO-like mice, thereby reducing epidermal hyperplasia, inhibiting inflammatory cell infiltration, and effectively alleviating inflammation. Furthermore, when Pg OMVs was loaded in the thermosensitive PF-127 hydrogel and subcutaneously injected, they exerted an immunomodulation effect. This enabled the continuous release of Pg OMVs, powerfully suppressed skin inflammation, and ameliorated the PSO. Another study used keratinocyte-derived EVs loaded with JPH203 inhibitor for PSO treatment.108 Under ultraviolet radiation, the EVs could produce more IL-1 receptor antagonist and inhibit inflammation, while JPH203 could suppress mTOR-signaling pathway. This dual modification strategy significantly reduced IL-17 release and epidermal hyperplasia in PSO model.
 |
Figure 7 Representative vesicle-based delivery systems for PSO topical therapy. (A) Schematic of ASO-210@IFNγ-sEVs for PSO therapy. Reproduced with permission from Zhang W, Lin J, Shi p, et al. Small extracellular vesicles derived from MSCs have immunomodulatory effects to enhance delivery of aso-210 for psoriasis treatment. Front Cell Dev Biol. 2022;10:842813. Creative Commons.106 (B) Schematic of Pg OMVs in PSO therapy. Reprinted from Journal of Controlled Release, 377, Su D, Li M, Xie Y, et al. Gut commensal bacteria Parabacteroides goldsteinii-derived outer membrane vesicles suppress skin inflammation in psoriasis, 127–145, Copyright 2025, with permission from Elsevier.107 (C) Schematic diagram of the multifunctional fusion vesicle FV@CX5461 and its therapeutic effect on autoimmune skin diseases. Reproduced with permission from Huang R, Jia B, Su D, et al. Plant exosomes fused with engineered mesenchymal stem cell-derived nanovesicles for synergistic therapy of autoimmune skin disorders. J Extracell Vesicles. 2023;12(10):e12361. Creative Commons. https://creativecommons.org/licenses/by-nc-nd/4.0/.109 |
Recently, Huang et al109 developed a multipurpose vesicle (FV@CX5461) to deliver the immunosuppressive drug CX5461 by fusing exosome-like nanovesicles (GEVs) from grapefruit and genetically engineered gingival mesenchymal stem cell (GMSC)-derived EVs (CCR6-NV) (Figure 7C). The vesicles reserved the anti-inflammatory and antioxidant properties of GEVs and the targeting ability of CCR6-NV, and exhibited potent immune-modulating functions from CX5461. In PSO models, it remarkably attenuated the symptoms, mainly by remodeling immune microenvironment and inhibiting inflammatory immune cell targeting to repair the tissue lesions. In another study, a macrophage membrane coated bilirubin-based “nanobrake” was designed to achieve ROS scavenging, reduction of inflammation, and immune remodeling.110 This system precisely interfered with the immune microenvironment of the dermis, which shown a good therapeutic effect in PSO.
Clinical Research Progress of Drug Delivery Systems for PSO Topical Therapy
With advances in technology, various delivery carriers of anti-PSO drugs have exhibited great potential in the laboratory, and some have entered clinical trials, showing their potential for PSO therapy. Many of these results were encouraging. Table 1 summarizes the latest clinical trials of anti-PSO delivery systems.
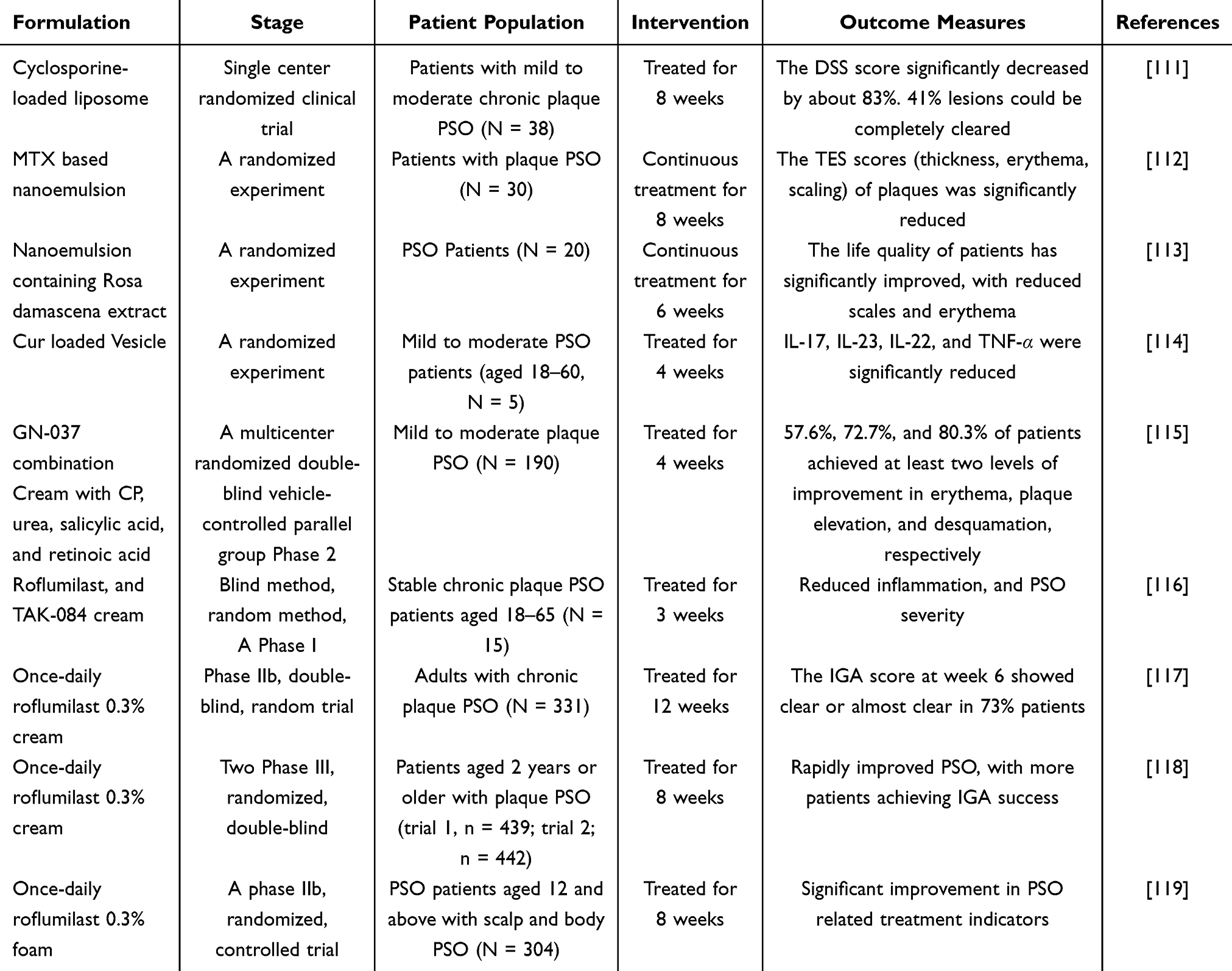 |
Table 1 Clinical Trial Progress of Drug Delivery Systems for PSO Therapy |
Kumar and coworkers evaluated the safety and curative effects of liposomal nanocarriers of cyclosporine for the treatment of limited chronic plaque PSO.111 Thirty-eight mild-to-moderate patients were enrolled in the trial, which demonstrated that 95% of the patients cured with 2% cyclosporine liposomes responded favorably. After 8 weeks of treatment, the dermatological sum score (DSS) of the lesion site significantly decreased by approximately 83%, and 41% of lesions were completely cleared, whereas none of those cured with placebo or traditional cream were completely cleared. In addition, no systemic accumulation of cyclosporine was observed.
Ramez et al further explored an MTX based nanoemulsion consisting of 40% jojoba oil, 45% tween-80 and strychnine-85 (3: 1 ratio), and 15% water for PSO treatment.112 In an 8-week clinical trial of 30 patients with plaque PSO, the TES scores (thickness, erythema, scaling) of psoriatic plaques were significantly reduced, indicating that MTX nanoemulsion is safe and promising for clinical use in PSO. Moreover, some researchers have developed nanoemulsions containing lyophilized forms of natural Rosa damascena extracts with antioxidant and anti-inflammatory effects.113 It was successfully formulated with the assistance of isopropyl myristate, Transcutol HP and Cremophor RH40. After six weeks of application in 20 patients with PSO, the patients’ quality of life improved significantly with less scaly erythema and less hardening, providing strong evidence for the therapy of related diseases with nanoemulsions of natural active ingredients.
In addition, Kolahdooz et al prepared vesicles containing Cur to enhance drug delivery and anti-inflammatory capabilities using the film hydration method.114 After adding them to HA and marine collagen-based gels, a formulation was formed. In a four-week topical treatment study of five patients with moderate to mild PSO, redness and epidermal peeling were significantly reduced compared with placebo. As a topical treatment, vesicles are expected to enhance the therapeutic effect and promote the healing of psoriatic skin injuries.
A multicenter, double-blind, randomized, controlled Phase II study was performed to assess the effectiveness of the combination cream GN-037 and clobetasol 17-propionate (CP) in treating mild-to-moderate plaque-type PSO.115 A total of 190 patients were divided into GN-037, CP, and control cream groups and received four-week treatment. The results showed that the GN-037 group was superior to the control group in terms of treatment success rate, improvement of erythema, plaque elevation, and desquamation and had good safety, which confirmed its efficacy and safety. To assess the therapeutic efficacy of the PDE4 inhibitors TAK-084 and roflumilast, 15 patients participated in a blinded randomized study that compared six topical creams.116 After 3 weeks of treatment, the skin infiltration thickness in each treatment group significantly improved. Among these, roflumilast and TAK-084 exhibited the best effects. Adverse events were mostly mild or moderate, indicating the potential to replace corticosteroid hormone therapy. In addition, in a phase IIb trial, 331 adults with chronic plaque PSO were assigned in a 1: 1: 1 ratio to a 0.15% roflumilast foam group, a 0.3% roflumilast foam group, and a control group for 12 weeks of treatment.117 The investigator’s global assessment (IGA) score at week 6 showed that the healing rate of 0.3% roflumilast foam group was 73%, which was much higher than 44% of the roflumilast 0.15% group and 29% of the control group. Further clinical studies have demonstrated a good therapeutic potential.118,119
Discussion
Owing to their unique physicochemical properties, various drug delivery systems exhibit significant advantages in terms of improved drug stability, controlled release, biocompatibility, and targeting. These properties have brought about the increasing therapeutic potential of PSO, as they can effectively increase the drug concentration in the lesion skin area, while reducing the impact on normal skin and lowering side effects. However, every type of delivery system has its pros and cons. Table 2 summarizes the advantages and disadvantages of different delivery systems for the topical treatment of PSO.
 |
Table 2 The Comparison of Different Drug Delivery Systems for PSO Therapy |
NPs are expected to be utilized in the therapy of diverse types of PSO. Given their ability to deliver drugs directly to the affected region through passive or active targeting, they can enhance the efficacy and reduce side effects. However, these methods have several disadvantages and challenges.120,121 Owing to cuticula thickening in patients with PSO, it is challenging for NPs to penetrate the skin and deliver drugs. In addition, the pathogenesis of PSO is complex, and topical application of a single drug may make it difficult to cover multiple inflammatory cycles, thus limiting their therapeutic efficacy. In the future, multifunctional composite NPs loaded with multiple drugs should be designed via surface engineering to improve skin permeability and enhance the drug delivery efficiency. Alternatively, biomarkers and multiomics technologies can be used to develop personalized treatments.122
By virtue of their three-dimensional network structure, hydrogels can accurately encapsulate drugs and release them slowly to maintain the effective drug concentration in PSO lesions for a long time, and they can also be targeted to lesions with the help of surface modification to improve therapeutic efficacy. However, the preparation process is complicated and requires strict control of the monomer concentration, crosslinking agent ratio, and reaction conditions, which are costly and unfavorable for large-scale production and clinical application. In addition, the safeties of their in vivo metabolic pathway and degradation products are still unclear, which poses potential risks. In the future, the development of smart-responsive hydrogels which utilize the microenvironment of the lesion to trigger drug release,123,124 and the construction of multifunctional composite systems especially from natural materials,125–127 will promote their wide application in the treatment of PSO.
The advantage of MN technology is its minimally invasive nature, which reduces patient pain and the risk of infection, and enhances patient compliance. When treating PSO, MNs can effectively penetrate the cuticula and deliver drugs directly to the lesion to enhance their therapeutic effects. The versatility of MNs opens up new possibilities for disease diagnosis and treatment.128 However, MN technology has limitations in carrying drugs and not all drugs are suitable Second, the biocompatibility of the primary and excipients, as well as the transdermal mechanism, is complex and requires multidisciplinary cooperation for research. There is an insufficient understanding of the mechanism of PSO recurrence, and more studies are needed to facilitate translational research on MNs. In the future, MN technology is expected to lead to breakthroughs in material innovation, structural optimization, and functional expansion, resulting in better treatment outcomes and quality of life for patients.
Micelles are self-assembled nanocarriers with a high drug-carrying capacity, which can wrap insoluble drugs through hydrophobicity, enhance water solubility and in vivo drug delivery efficiency, and passively target skin lesions by virtue of their small particle size. Nevertheless, micelles are easily removed by the reticuloendothelial system because of their small particle size and short circulation time. They have potential toxicity owing to their accumulation and interference with cellular functions during long-term use, which limits their wide application. In the future, strategies such as surface conjugation with targeting ligands and the development of intelligent micelles that respond to the microenvironment of psoriatic lesions can be employed to prolong their circulation time and enable active targeting.82 Furthermore, the development of biocompatible, biodegradable materials for constructing micelles and a thorough exploration of their metabolic pathways can drive their clinical translation and development in PSO treatment.
Dendrimers have specific surface groups that can be altered with targeted ligands, such as peptides, to achieve precise drug delivery. However, their physical and chemical stabilities have potential constraints. Second, the synthesis of dendrimers is complex and costly, limiting their large-scale application. In addition, the aggregation phenomenon and potential toxicity of dendrimers are issues that need to be addressed. Future developments are focused on improving the stability and biocompatibility of dendrimers, as well as opening up new synthesis methods to reduce costs.129 In the meanwhile, combining multiple treatment strategies and developing responsive dendrimers is also a major trend.130
Liposomes have become a popular choice in nanotechnology for drug delivery because of their remarkable versatility in transporting both water- and fat-soluble drugs.88 Their appeal lies in their excellent biocompatibility and minimal risk of toxicity or immune reaction. In PSO treatment, liposomes help to deliver drugs to the skin more precisely, potentially boosting their effectiveness and minimizing adverse reactions. However, their stability is limited by the fragility of phospholipid membranes and sensitivity to peroxidation, which can lead to physical degradation. Therefore, the long-term safety of liposomes and the optimal dosing strategies require further investigation. The cost and technical challenges of the preparation and delivery process are also issues that need to be addressed. Future studies should focus on developing innovative liposomal therapies and delivery mechanisms tailored to diverse patient requirements.131,132
Nanoemulsions show promise for PSO therapy because of their improved skin absorption and drug solubility, which are ideal for addressing skin folds and creases. Although generally safe, nanoemulsions may trigger skin irritation or cytotoxic reactions and drug penetration into the thickened epidermis is difficult, resulting in low bioavailability. Prolonged use of corticosteroid-containing nanoemulsions may also cause adverse effects such as hormone dependence and skin atrophy. Advancements in nanoemulsion preparation can significantly enhance transdermal delivery of anti-inflammatory medications. By refining these formulations, the likelihood of hormone dependency and skin thinning can be minimized, paving the way for safer and more potent treatments with reduced systemic risk.133
Vesicles exhibit high biocompatibility, minimal immunogenicity, and effective drug delivery for PSO therapy.134 However, the yield and quality of vesicles are influenced by organoids, and natural vesicles have suboptimal efficacy and lack target specificity. However, their mode of operation remains unclear, restricting their widespread application. Future directions include engineering vesicles to improve their targeting and efficacy and developing vesicle-mediated multifunctional combination therapies to enhance therapeutic efficacy.135
As an autoimmune-related disease, there is currently no method that can completely cure PSO. Therefore, the construction of drug delivery systems based on various types of drug carriers has increasingly attracted attention. By utilizing drug delivery systems, not only has the therapeutic effect of existing drugs been enhanced, and the toxic side effects have been reduced, but it is also expected to enable the combined delivery of multiple types of drugs. By leveraging the characteristics of PSO and fully utilizing the advantages of various types of drug carriers, selectively delivering drugs locally will provide more strategies for the treatment of PSO and offer more options for the development of clinical drugs.
Conclusion
In summary, the key targets for effective therapy of PSO by topical delivery systems include improving skin permeability and drug accumulation, while reducing systemic absorption. Rational delivery systems integrated with specific drug ingredients can potentially achieve this target. This review explores various topical delivery systems such as NPs, hydrogels, MNs, micelles, dendrimers, liposomes, nanoemulsions, vesicles, etc., in PSO therapy. Through material innovation and dosage form optimization, they have demonstrated significant advantages in breaking through skin barrier, achieving targeted localization, prolonging residence time, and reducing systemic exposure, thus providing a theoretical basis and technological paradigm for future development of PSO therapy strategies.
However, current topical delivery systems still face multiple challenges, such as the long-term bioaccumulation of drug carriers that may trigger immunogenicity, and the difficulty of precisely matching their degradation rate with drug release kinetics. Process complexities such as crosslinking regulation of hydrogels and size homogenization of vesicles lead to high production cost and limiting scale-up. The limitations of passive targeting relying on the high permeability of the inflammation site still put normal tissues at drug exposure risk, while the permeability barrier of the stratum corneum to macromolecular drugs has not yet been fully breached. In addition, PSO involves multiple pathological mechanisms, and it is difficult to realize the whole chain of regulation with the existing single-target intervention system.
In the future, we can construct delivery systems with responsiveness, such as pH/ROS sensitivity, to realize drug cascade release triggered by inflammatory microenvironment. At the same time, the development of plant-derived exosomes and immune cell membrane based fusion delivery systems, through the membrane surface receptors to mediate active targeting, while integrating immunotherapy and other treatment strategies, to promote the standardization of clinical translation, have a significant development potential. It’s worthy notice that combining artificial intelligence (AI)-assisted material design to optimize the production process and exploring the combination of drug carriers with various treatment methods is expected to promote the development of drug delivery systems. With the in-depth analysis of the action mechanism of delivery system and technology iteration, it is expected to develop more efficient and safer therapeutic solutions, and provide PSO patients with innovative therapies with both precision and tolerability. It is believed that, through the efforts of researchers, multitudinous multifunctional drug delivery systems will emerge in the treatment of PSO, and it is ultimately expected to achieve a clinical cure for PSO.
Abbreviations
Psoriasis, PSO; apremilast, APR; deucravacitinib, DEU; Nanoparticles, NPs; Microneedles, MNs; bioadhesive NPs, BNPs; betamethasone dipropionate, BD; polylactic acid-hyperbranched polyglycerol, PLA-HPG; reactive oxygen species, ROS; hyaluronic acid, HA; Imiquimod, IMQ; Psoriasis Area Severity Index, PASI; chitosan, CS; Signal Transducer and Activator of Transcription 3, STAT3; human immortalized keratinocytes, HaCaT cell line; gallic acid, GA; polyethylene glycol, PEG; water-responsive hydrogel, WRG; glyceryl dioleate, GDO; phosphatidyl choline, PC; Curcumin, Cur; borneol, BO; tyrosine kinase 2 inhibitor, TYK2i; 5-aminoleavulinic acid, ALA; epigallocatechin catechin, EGCG; calcipotriol, CPT; phenylboronate, GB; lipoic acid, LA; dexamethasone, dex; cyclooxygenase-2, COX2; extracellular vesicles, EVs; mesenchymal stem cells, MSCs; dermatological sum score, DSS; investigator’s global assessment, IGA.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
2. Sewerin P, Brinks R, Schneider M, Haase I, Vordenbäumen S. Prevalence and incidence of psoriasis and psoriatic arthritis. Ann Rheum Dis. 2019;78(2):286–287. doi:10.1136/annrheumdis-2018-214065
3. Guo J, Zhang H, Lin W, Lu L, Su J, Chen X. Signaling pathways and targeted therapies for psoriasis. Signal Transduct Target Ther. 2023;8(1):437. doi:10.1038/s41392-023-01655-6
4. Maronese CA, Valenti M, Moltrasio C, et al. paradoxical psoriasis: an updated review of clinical features, pathogenesis, and treatment options. J Invest Dermatol. 2024;144(11):2364–2376. doi:10.1016/j.jid.2024.05.015
5. Veale DJ, Fearon U. The pathogenesis of psoriatic arthritis. Lancet. 2018;391(10136):2273–2284. doi:10.1016/S0140-6736(18)30830-4
6. Nussbaum L, Chen YL, Ogg GS. Role of regulatory T cells in psoriasis pathogenesis and treatment. Br J Dermatol. 2021;184(1):14–24. doi:10.1111/bjd.19380
7. Sieminska I, Pieniawska M, Grzywa TM. The immunology of psoriasis-current concepts in pathogenesis. Clin Rev Allergy Immunol. 2024;66(2):164–191. doi:10.1007/s12016-024-08991-7
8. Bravo A, Kavanaugh A. Bedside to bench: defining the immunopathogenesis of psoriatic arthritis. Nat Rev Rheumatol. 2019;15(11):645–656. doi:10.1038/s41584-019-0285-8
9. Olejnik-Wojciechowska J, Boboryko D, Bratborska AW, et al. The role of epigenetic factors in the pathogenesis of psoriasis. Int J Mol Sci. 2024;25(7):3831. doi:10.3390/ijms25073831
10. Wu JJ, Kavanaugh A, Lebwohl MG, Gniadecki R, Merola JF. Psoriasis and metabolic syndrome: implications for the management and treatment of psoriasis. J Eur Acad Dermatol Venereol. 2022;36(6):797–806. doi:10.1111/jdv.18044
11. Yu J, Zhao Q, Wang X, et al. Pathogenesis, multi-omics research, and clinical treatment of psoriasis. J Autoimmun. 2022;133:102916. doi:10.1016/j.jaut.2022.102916
12. Lee H, Kim M. Challenges and future trends in the treatment of psoriasis. Int J Mol Sci. 2023;24(17):13313. doi:10.3390/ijms241713313
13. Brozyna AA, Slominski RM, Nedoszytko B, Zmijewski MA, Slominski AT. Vitamin D signaling in psoriasis: pathogenesis and therapy. Int J Mol Sci. 2022;23(15):8575. doi:10.3390/ijms23158575
14. Hjort G, Schwarz CW, Skov L, Loft N. Clinical characteristics associated with response to biologics in the treatment of psoriasis: a meta-analysis. JAMA Dermatol. 2024;160(8):830–837. doi:10.1001/jamadermatol.2024.1677
15. ZPBL L. Predictors of response to treatment with biologics in people with moderate-to-severe psoriasis. Br J Dermatol. 2024;190(5):e55.
16. Lee EB, Amin M, Wu JJ. Drug survival of apremilast in patients treated for psoriasis in a real-world setting. J Am Acad Dermatol. 2018;79(4):760–761. doi:10.1016/j.jaad.2018.03.028
17. Ridha Z, Ouchene L, Netchiporouk E, Gooderham MJ. Topical PDE-4 inhibitors are emerging for psoriasis treatment. J Cutan Med Surg. 2021;25(1):109–110. doi:10.1177/1203475420960429
18. Mease P, Coates LC, Helliwell PS, et al. Efficacy and safety of filgotinib, a selective Janus kinase 1 inhibitor, in patients with active psoriatic arthritis (EQUATOR): results from a randomised, placebo-controlled, phase 2 trial. Lancet. 2018;392(10162):2367–2377. doi:10.1016/S0140-6736(18)32483-8
19. Morand E, Merola JF, Tanaka Y, Gladman D, Fleischmann R. TYK2: an emerging therapeutic target in rheumatic disease. Nat Rev Rheumatol. 2024;20(4):232–240. doi:10.1038/s41584-024-01093-w
20. Kurz B, Berneburg M, Bäumler W, Karrer S. Phototherapy: theory and practice. J Dtsch Dermatol Ges. 2023;21(8):882–897.
21. Ramic L, Sator P. Topical treatment of psoriasis vulgaris. J Dtsch Dermatol Ges. 2023;21(6):631–642.
22. Ahmad MZ, Mohammed AA, Algahtani MS, Mishra A, Ahmad J. nanoscale topical pharmacotherapy in management of psoriasis: contemporary research and scope. J Funct Biomater. 2022;14(1):19. doi:10.3390/jfb14010019
23. Gungor S, Rezigue M. nanocarriers mediated topical drug delivery for psoriasis treatment. Curr Drug Metab. 2017;18(5):454–468. doi:10.2174/1389200218666170222145240
24. Pradhan M, Alexander A, Singh MR, et al. Understanding the prospective of nano-formulations towards the treatment of psoriasis. Biomed Pharmacother. 2018;107:447–463. doi:10.1016/j.biopha.2018.07.156
25. Jyothi SL, Krishna KL, Ameena Shirin VK, Sankar R, Pramod K, Gangadharappa HV. Drug delivery systems for the treatment of psoriasis: current status and prospects. J Drug Deliv Sci Technol. 2021;62:102364. doi:10.1016/j.jddst.2021.102364
26. Singh S, Sharma N, Behl T, et al. promising strategies of colloidal drug delivery-based approaches in psoriasis management. Pharmaceutics. 2021;13(11):1978. doi:10.3390/pharmaceutics13111978
27. Mitchell MJ, Billingsley MM, Haley RM, Wechsler ME, Peppas NA, Langer R. Engineering precision nanoparticles for drug delivery. Nat Rev Drug Discov. 2021;20(2):101–124. doi:10.1038/s41573-020-0090-8
28. Bodnár K, Fehér P, Ujhelyi Z, Bácskay I, Józsa L. Recent approaches for the topical treatment of psoriasis using nanoparticles. Pharmaceutics. 2024;16(4):449. doi:10.3390/pharmaceutics16040449
29. Gomes GS, Frank LA, Contri RV, Longhi MS, Pohlmann AR, Guterres SS. Nanotechnology-based alternatives for the topical delivery of immunosuppressive agents in psoriasis. Int J Pharm. 2023;631:122535. doi:10.1016/j.ijpharm.2022.122535
30. Mai Y, Ouyang Y, Yu M, et al. Topical formulation based on disease-specific nanoparticles for single-dose cure of psoriasis. J Control Release. 2022;349:354–366. doi:10.1016/j.jconrel.2022.07.006
31. Xin X, Zhou Y, Lyu Y, et al. Disease-specific Corona mediated co-delivery of MTX and siRNA-TNFα by a polypeptide nanoplatform with antigen-scavenging functions in psoriasis. J Control Release. 2023;364:326–342. doi:10.1016/j.jconrel.2023.10.035
32. Sheikh A, Hazari SA, Molugulu N, et al. Hyaluronic acid engineered gallic acid embedded chitosan nanoparticle as an effective delivery system for treatment of psoriasis. Environ Res. 2023;238(Pt 1):117086. doi:10.1016/j.envres.2023.117086
33. Fan Z, Zhao G, Gan Y, et al. Synergistic chemo-photodynamic therapy based on hollow mesoporous organosilica nanoparticles for reducing psoriasis-like inflammation. Chem Eng J. 2024;490:151613. doi:10.1016/j.cej.2024.151613
34. Li L, Liu C, Fu J, et al. CD44 targeted indirubin nanocrystal-loaded hyaluronic acid hydrogel for the treatment of psoriasis. Int J Biol Macromol. 2023;243:125239. doi:10.1016/j.ijbiomac.2023.125239
35. Lugović Mihić L, Novak Bilić G, Vučić M, Japundžić I, Bukvić I. CD44 expression in human skin: high expression in irritant and allergic contact dermatitis and moderate expression in psoriasis lesions in comparison with healthy controls. Contact Dermatitis. 2020;82(5):297–306. doi:10.1111/cod.13463
36. Lee WH, Rho JG, Yang Y, et al. hyaluronic acid nanoparticles as a topical agent for treating psoriasis. ACS Nano. 2022;16(12):20057–20074. doi:10.1021/acsnano.2c07843
37. Chen R, Zhai Y, Sun L, et al. Alantolactone-loaded chitosan/hyaluronic acid nanoparticles suppress psoriasis by deactivating STAT3 pathway and restricting immune cell recruitment. Asian J Pharm Sci. 2022;17(2):268–283. doi:10.1016/j.ajps.2022.02.003
38. Han R, LWC H, Bai Q, et al. Alkyl-terminated gold nanoparticles as a self-therapeutic treatment for psoriasis. Nano Lett. 2021;21(20):8723–8733. doi:10.1021/acs.nanolett.1c02899
39. Zhang Z, Zhou D, Li Z, et al. A nanoinhibitor targeting CGAS‐sting pathway to reverse the homeostatic imbalance of inflammation in psoriasis. Angew. Chem. Int. Ed. 2024;63(2):e202316007. doi:10.1002/anie.202316007
40. Luo Y, Tan J, Zhou Y, et al. From crosslinking strategies to biomedical applications of hyaluronic acid-based hydrogels: a review. Int J Biol Macromol. 2023;231:123308. doi:10.1016/j.ijbiomac.2023.123308
41. Tan J, Luo Y, Guo Y, et al. Development of alginate-based hydrogels: crosslinking strategies and biomedical applications. Int J Biol Macromol. 2023;239:124275. doi:10.1016/j.ijbiomac.2023.124275
42. Liao X, Feng X, Xiao Z, et al. Multifunctional phenylboric acid modified carboxymethyl chitosan based hydrogel crosslinked by tannic acid. Int J Biol Macromol. 2025;304(Pt 2):140958. doi:10.1016/j.ijbiomac.2025.140958
43. Damiri F, Fatimi A, Liu Y, et al. Recent advances in 3D bioprinted polysaccharide hydrogels for biomedical applications: a comprehensive review. Carbohydr Polym. 2025;348(Pt B):122845. doi:10.1016/j.carbpol.2024.122845
44. Tang Y, Huang J, Damiri F, et al. The preparation of silk fibroin-based hydrogels and their applications in cartilage repair. Int J Biol Macromol. 2025;310(Pt 4):143610. doi:10.1016/j.ijbiomac.2025.143610
45. Vasowala T, Gharat S, Mhase M, Momin M. Advances in hydrogels based cutaneous drug delivery system for management of psoriasis. Eur Polym J. 2024;202:112630. doi:10.1016/j.eurpolymj.2023.112630
46. Dutt P, Singhvi G, Tomar Y, Sain S, Rana V. Unveiling hydrogel’s prominence: a breakthrough in topical formulations for psoriasis treatment. Int J Polym Mater Polym Biomat. 2024;73(17):1525–1549. doi:10.1080/00914037.2023.2299801
47. Yao Q, Zhai YY, He Z, et al. Water-responsive gel extends drug retention and facilitates skin penetration for curcumin topical delivery against psoriasis. Asian J Pharm Sci. 2023;18(2):100782. doi:10.1016/j.ajps.2023.100782
48. Lai Y, Wu X, Jiang Z, et al. Topical treatment of tyrosine kinase 2 inhibitor through borneol-embedded hydrogel: evaluation for preventive, therapeutic, and Recurrent management of psoriasis. Bioact Mater. 2024;41:83–95. doi:10.1016/j.bioactmat.2024.07.013
49. Fan Y, Mohanty S, Zhang Y, et al. Dendritic hydrogels induce immune modulation in human keratinocytes and effectively eradicate bacterial pathogens. J Am Chem Soc. 2021;143(41):17180–17190. doi:10.1021/jacs.1c07492
50. Wang Y, Fu S, Lu Y, et al. Chitosan/hyaluronan nanogels co-delivering methotrexate and 5-aminolevulinic acid: a combined chemo-photodynamic therapy for psoriasis. Carbohydr Polym. 2022;277:118819. doi:10.1016/j.carbpol.2021.118819
51. Chen H, Xu J, Jiang Y, et al. Controlled delivery of MTX from thermosensitive hydrogels using au nanorods for enhanced therapeutics of psoriasis via improving stratum corneum penetration. Small. 2025;21(9):e2410566. doi:10.1002/smll.202410566
52. Lee K, MJ G, Tebon P, et al. Non-transdermal microneedles for advanced drug delivery. Adv Drug Deliv Rev. 2020;165-166:41–59. doi:10.1016/j.addr.2019.11.010
53. Ma G, Wu C. Microneedle, bio-microneedle and bio-inspired microneedle: a review. J Control Release. 2017;251:11–23. doi:10.1016/j.jconrel.2017.02.011
54. Gowda B, Ahmed MG, Hani U, Kesharwani P, Wahab S, Paul K. Microneedles as a momentous platform for psoriasis therapy and diagnosis: a state-of-the-art review. Int J Pharm. 2023;632:122591. doi:10.1016/j.ijpharm.2023.122591
55. Qu F, Geng R, Liu Y, Zhu J. Advanced nanocarrier- and microneedle-based transdermal drug delivery strategies for skin diseases treatment. Theranostics. 2022;12(7):3372–3406. doi:10.7150/thno.69999
56. Li J, Yuan Z, Shi S, et al. Microneedle patches incorporating zinc-doped mesoporous silica nanoparticles loaded with betamethasone dipropionate for psoriasis treatment. J Nanobiotechnology. 2024;22(1):706. doi:10.1186/s12951-024-02986-4
57. Hu J, Bian Q, Ma X, Xu Y, Gao J. A double-edged sword: ROS related therapies in the treatment of psoriasis. Asian J Pharm Sci. 2022;17(6):798–816. doi:10.1016/j.ajps.2022.10.005
58. Wronski A, Wojcik P. Impact of ROS-dependent lipid metabolism on psoriasis pathophysiology. Int J Mol Sci. 2022;23(20):12137. doi:10.3390/ijms232012137
59. Bi D, Qu F, Xiao W, et al. Reactive oxygen species-responsive gel-based microneedle patches for prolonged and intelligent psoriasis management. ACS Nano. 2023;17(5):4346–4357. doi:10.1021/acsnano.2c08979
60. Zhou Y, Yang L, Lyu Y. Topical delivery of ROS-responsive methotrexate prodrug nanoassemblies by a dissolvable microneedle patch for psoriasis therapy. Int J Nanomed. 2023;18:899–915. doi:10.2147/IJN.S394957
61. Wu D, Shou X, Yu Y, et al. Biologics-loaded photothermally dissolvable hyaluronic acid microneedle patch for PSO treatment. Adv Funct Mater. 2022;32(47):2205847. doi:10.1002/adfm.202205847
62. Huang L, Luo Y, Kuai L, et al. An approach for psoriasis of microneedle patch simultaneously targeting multiple inflammatory cytokines and relapse related T cells. Biomaterials. 2025;318:123120. doi:10.1016/j.biomaterials.2025.123120
63. Lu M, Zhang X, Cai L, et al. Black phosphorus hydrogel inverse opal microneedle patches for psoriasis treatment. Nano Today. 2024;54:102072. doi:10.1016/j.nantod.2023.102072
64. Wang Y, Zhang X, Chen G, Lu M, Zhao Y. Multifunctional structural color triboelectric microneedle patches for psoriasis treatment. Matter. 2023;6(5):1555–1568. doi:10.1016/j.matt.2023.03.005
65. Detamornrat U, McAlister E, Hutton ARJ, Larrañeta E, Donnelly RF. The role of 3d printing technology in microengineering of microneedles. Small. 2022;18(18):2106392. doi:10.1002/smll.202106392
66. Desai S, Parupelli SK, Desai S. A review of 3D-printing of microneedles. Pharmaceutics. 2022;14(12):2693. doi:10.3390/pharmaceutics14122693
67. Liu H, Nail A, Meng D, et al. Recent progress in the 3D printing of microneedle patches for biomedical applications. Int J Pharm. 2025;668:124995. doi:10.1016/j.ijpharm.2024.124995
68. Govender M, Indermun S, Choonara YE. 3D bioprinted microneedles: merging drug delivery and scaffold science for tissue-specific applications. Expert Opin Drug Deliv. 2024;21(11):1559–1572. doi:10.1080/17425247.2024.2351928
69. Razzaghi M, Alexander NJ, Akbari M. Advancements in materials for 3D-printed microneedle arrays: enhancing performance and biocompatibility. Micromachines. 2024;15(12):1433. doi:10.3390/mi15121433
70. Punnel LC, Palmtag M, Lunter DJ, Perry JL. Development of 3D printed microneedles of varied needle geometries and lengths, designed to improve the dermal delivery of topically applied psoriasis treatments. Eur J Pharm Biopharm. 2024;204:114523. doi:10.1016/j.ejpb.2024.114523
71. Kamal YT, Aldawsari HM, Badr-Eldin SM, Nair AB, YT K. Progress in polymeric micelles for drug delivery applications. Pharmaceutics. 2022;14(8):1636. doi:10.3390/pharmaceutics14081636
72. DH A, A JDR, Avka B. Polymeric micelles for the delivery of poorly soluble drugs: from nanoformulation to clinical approval. Adv Drug Deliv Rev. 2020;156(S1):80–118. doi:10.1016/j.addr.2020.09.009
73. Makhmalzade BS, Chavoshy F. Polymeric micelles as cutaneous drug delivery system in normal skin and dermatological disorders. J Adv Pharm Technol Res. 2018;9(1):2–8. doi:10.4103/japtr.JAPTR_314_17
74. Jiang Y, Chen Y, Yu Q, Shi Y. Biologic and small-molecule therapies for moderate-to-severe psoriasis: focus on psoriasis comorbidities. Biodrugs. 2023;37(1):35–55. doi:10.1007/s40259-022-00569-z
75. Keating GM. Apremilast: a review in psoriasis and psoriatic arthritis. Drugs. 2017;77(4):459–472. doi:10.1007/s40265-017-0709-1
76. Sontakke A, Dighe S, Sharma R, Yadav V, Jain S. Harnessing the potential of fatty acid-surfactant-based micellar gel for enhanced topical delivery of apremilast in psoriasis treatment. Int J Pharm. 2024;655:124026. doi:10.1016/j.ijpharm.2024.124026
77. Yao L, Tian F, Meng Q, et al. Reactive oxygen species-responsive supramolecular deucravacitinib self-assembly polymer micelles alleviate psoriatic skin inflammation by reducing mitochondrial oxidative stress. Front Immunol. 2024;15:1407782. doi:10.3389/fimmu.2024.1407782
78. Zhao T, Zhou M, Wu R, et al. Dendrimer-conjugated isotretinoin for controlled transdermal drug delivery. J Nanobiotechnology. 2023;21(1):285. doi:10.1186/s12951-023-02052-5
79. Tan E, Wan T, Pan Q, et al. Dual-responsive nanocarriers for efficient cytosolic protein delivery and CRISPR-Cas9 gene therapy of inflammatory skin disorders. Sci Adv. 2024;10(16):eadl4336. doi:10.1126/sciadv.adl4336
80. Roskoski R. Deucravacitinib is an allosteric TYK2 protein kinase inhibitor FDA-approved for the treatment of psoriasis. Pharmacol Res. 2023;189:106642. doi:10.1016/j.phrs.2022.106642
81. Truong TM, Pathak GN, Singal A, Taranto V, Rao BK. Deucravacitinib: the First FDA-Approved Oral TYK2 inhibitor for moderate to severe plaque psoriasis. Ann Pharmacother. 2024;58(4):416–427. doi:10.1177/10600280231153863
82. Hua Y, Chang T, Jiang K, et al. ROS-sensitive calcipotriol nano-micelles prepared by methoxypolyethylene glycol (mPEG) – modified polymer for the treatment of psoriasis. Drug Deliv. 2022;29(1):1903–1913. doi:10.1080/10717544.2022.2086944
83. Chauhan AS. Dendrimers for Drug Delivery. Molecules. 2018;23(4):938. doi:10.3390/molecules23040938
84. Huang D, Wu D. Biodegradable dendrimers for drug delivery. Mater Sci Eng C. 2018;90:713–727. doi:10.1016/j.msec.2018.03.002
85. Guo Y, He X, Williams GR, et al. Tumor microenvironment-responsive hyperbranched polymers for controlled drug delivery. J Pharm Anal. 2024;14(12):101003. doi:10.1016/j.jpha.2024.101003
86. Chis AA, Dobrea C, Morgovan C, et al. Applications and limitations of dendrimers in biomedicine. Molecules. 2020;25(17):3982. doi:10.3390/molecules25173982
87. Tripathi PK, Gorain B, Choudhury H, Srivastava A, Kesharwani P. Dendrimer entrapped microsponge gel of dithranol for effective topical treatment. Heliyon. 2019;5(3):e1343. doi:10.1016/j.heliyon.2019.e01343
88. Large DE, Abdelmessih RG, Fink EA, Auguste DT. Liposome composition in drug delivery design, synthesis, characterization, and clinical application. Adv Drug Deliv Rev. 2021;176:113851. doi:10.1016/j.addr.2021.113851
89. Liu P, Chen G, Zhang J. A review of liposomes as a drug delivery system: current status of approved products, regulatory environments, and future perspectives. Molecules. 2022;27(4):1372. doi:10.3390/molecules27041372
90. Mohd Nordin UU, Ahmad N, Salim N, Mohd yusof NS. Lipid-based nanoparticles for psoriasis treatment: a review on conventional treatments, recent works, and future prospects. RSC Adv. 2021;11(46):29080–29101. doi:10.1039/D1RA06087B
91. Yu F, Zhang Y, Yang C, Li F, Qiu B, Ding W. Enhanced transdermal efficiency of curcumin-loaded peptide-modified liposomes for highly effective antipsoriatic therapy. J Mat Chem B. 2021;9(24):4846–4856. doi:10.1039/D1TB00557J
92. Lu B, Zhang J, Zhang J. Enhancing transdermal delivery of curcumin-based ionic liquid liposomes for application in psoriasis. ACS Appl Bio Mater. 2023;6(12):5864–5873. doi:10.1021/acsabm.3c01026
93. Qu F, Sun Y, Bi D, et al. Regulating size and charge of liposomes in microneedles to enhance intracellular drug delivery efficiency in skin for psoriasis therapy. Adv Healthc Mater. 2023;12(31):2302314. doi:10.1002/adhm.202302314
94. Jain S, Pattewad V, Bhargavi N, et al. Exploring the therapeutic potential of functional excipient-based nanoemulgel of fluticasone propionate for the management of psoriasis. J Drug Deliv Sci Technol. 2023;84:104435. doi:10.1016/j.jddst.2023.104435
95. Ma X, Bian Q, Xu Y, et al. Foamed microemulsion nanodroplets loaded with chlorin e6 for epidermal-targeted treatment against psoriasis. Nano Res. 2024;17(11):9920–9931. doi:10.1007/s12274-024-6916-7
96. Zhang Y, Xia Q, Li Y, et al. CD44 assists the topical anti-psoriatic efficacy of curcumin-loaded hyaluronan-modified ethosomes: a new strategy for clustering drug in inflammatory skin. Theranostics. 2019;9(1):48–64. doi:10.7150/thno.29715
97. Rai VK, Mishra N, Yadav KS, Yadav NP. Nanoemulsion as pharmaceutical carrier for dermal and transdermal drug delivery: formulation development, stability issues, basic considerations and applications. J Control Release. 2018;270:203–225. doi:10.1016/j.jconrel.2017.11.049
98. Pandey P, Gulati N, Makhija M, Purohit D, Dureja H. Nanoemulsion: a novel drug delivery approach for enhancement of bioavailability. Recent Pat Nanotechnol. 2020;14(4):276–293. doi:10.2174/1872210514666200604145755
99. Dinshaw IJ, Ahmad N, Salim N, Leo BF. Nanoemulsions: a review on the conceptualization of treatment for psoriasis using a ‘green’ surfactant with low-energy emulsification method. Pharmaceutics. 2021;13(7):1024. doi:10.3390/pharmaceutics13071024
100. Rai V, Roy A, Sharma A, et al. Development and pharmaceutical evaluation of azelaic acid and vitamin e oil-based nanoemulgel of tacrolimus for topical application in plaque psoriasis. J Pharm Innov. 2023;18(4):1616–1625. doi:10.1007/s12247-023-09740-7
101. Rashid SA, Bashir S, Naseem F, Farid A, Rather IA, Hakeem KR. Olive oil based methotrexate loaded topical nanoemulsion gel for the treatment of imiquimod induced psoriasis-like skin inflammation in an animal model. Biology-Basel. 2021;10(11):1121. doi:10.3390/biology10111121
102. Sharma S, Masud MK, Kaneti YV, Rewatkar P, Salomon C. extracellular vesicle nanoarchitectonics for novel drug delivery applications. Small. 2021;17(42):e2102220. doi:10.1002/smll.202102220
103. Yadav K, Singh D, MR S. Nanovesicles delivery approach for targeting steroid mediated mechanism of antipsoriatic therapeutics. J Drug Deliv Sci Technol. 2021;65:102688. doi:10.1016/j.jddst.2021.102688
104. Iuliano M, Grimaldi L, Rosa P, et al. Extracellular vescicles in psoriasis: from pathogenesis to possible roles in therapy. Front Immunol. 2024;15:1360618. doi:10.3389/fimmu.2024.1360618
105. Yu H, Feng H, Zeng H, et al. Exosomes: the emerging mechanisms and potential clinical applications in dermatology. Int J Biol Sci. 2024;20(5):1778–1795. doi:10.7150/ijbs.92897
106. Zhang W, Lin J, Shi p, et al. Small extracellular vesicles derived from MSCs have immunomodulatory effects to enhance delivery of aso-210 for psoriasis treatment. Front Cell Dev Biol. 2022;10:842813. doi:10.3389/fcell.2022.842813
107. Su D, Li M, Xie Y, et al. Gut commensal bacteria Parabacteroides goldsteinii-derived outer membrane vesicles suppress skin inflammation in psoriasis. J Control Release. 2025;377:127–145. doi:10.1016/j.jconrel.2024.11.014
108. Jiang X, Jiang Z, Huang S, et al. Ultraviolet B radiation-induced JPH203-loaded keratinocyte extracellular vesicles exert etiological interventions for psoriasis therapy. J Control Release. 2023;362:468–478. doi:10.1016/j.jconrel.2023.08.059
109. Huang R, Jia B, Su D, et al. Plant exosomes fused with engineered mesenchymal stem cell-derived nanovesicles for synergistic therapy of autoimmune skin disorders. J Extracell Vesicles. 2023;12(10):e12361. doi:10.1002/jev2.12361
110. Chen R, Duan B, Li S, et al. A triple-targeting “nano-brake” remodeling the impaired immune microenvironment in skin lesions for psoriasis treatment. Mater Today Bio. 2025;32:101875. doi:10.1016/j.mtbio.2025.101875
111. Kumar R, Dogra S, Amarji B, et al. Efficacy of novel topical liposomal formulation of cyclosporine in mild to moderate stable plaque psoriasis: a randomized clinical trial. JAMA Dermatol. 2016;152(7):807–815. doi:10.1001/jamadermatol.2016.0859
112. Ramez SA, MM S, Fadel M, et al. Novel methotrexate soft nanocarrier/fractional erbium YAG laser combination for clinical treatment of plaque psoriasis. Artif. Cells Nanomed. Biotechnol. 2018;46(sup1):996–1002. doi:10.1080/21691401.2018.1440236
113. Gavra DI, Endres L, Pető Á, et al. In vitro and human pilot studies of different topical formulations containing rosa species for the treatment of psoriasis. Molecules. 2022;27(17):5499. doi:10.3390/molecules27175499
114. Kolahdooz H, Khori V, Erfani-Moghadam V, Livani F, Mohammadi S, Memarian A. Niosomal curcumin suppresses IL17/IL23 immunopathogenic axis in skin lesions of psoriatic patients: a pilot randomized controlled trial. Life-Basel. 2023;13(5):1076. doi:10.3390/life13051076
115. Engin B, Güler ÖM, Karstarlı Bakay ÖS, et al. A multicenter randomized double-blind vehicle-controlled parallel group phase 2 study evaluating the efficacy and safety of gn-037 cream in patients with mild-to-moderate plaque psoriasis. Dermatol Ther. 2024;14(12):3337–3350. doi:10.1007/s13555-024-01301-1
116. Snape SD, Wigger-Alberti W, Goehring UM. A Phase I randomized trial to assess the effect on skin infiltrate thickness and tolerability of topical phosphodiesterase inhibitors in the treatment of psoriasis vulgaris using a modified psoriasis plaque test. Br J Dermatol. 2016;175(3):479–486. doi:10.1111/bjd.14634
117. Lebwohl MG, Papp KA, Stein GL, et al. Trial of Roflumilast Cream for Chronic Plaque Psoriasis. New England Journal of Medicine. 2020;383(3):229–239. doi:10.1056/NEJMoa2000073
118. Lebwohl MG, Kircik LH, Moore AY, et al. Effect of roflumilast cream vs vehicle cream on chronic plaque psoriasis. JAMA. 2022;328(11):1073. doi:10.1001/jama.2022.15632
119. Kircik LH, Alonso-Llamazares J, Bhatia N, et al. Once-daily roflumilast foam 0.3% for scalp and body psoriasis: a randomized, double-blind, vehicle-controlled phase IIb study. Br J Dermatol. 2023;189(4):392–399. doi:10.1093/bjd/ljad182
120. Madawi EA, Al JA, Rawas-Qalaji M, et al. Polymeric nanoparticles as tunable nanocarriers for targeted delivery of drugs to skin tissues for treatment of topical skin diseases. Pharmaceutics. 2023;15(2):657. doi:10.3390/pharmaceutics15020657
121. Almuqbil RM, Aldhubiab B. bioadhesive nanoparticles in topical drug delivery: advances, applications, and potential for skin disorder treatments. Pharmaceutics. 2025;17(2):229. doi:10.3390/pharmaceutics17020229
122. Aydin B, Arga KY, Karadag AS. Omics-driven biomarkers of psoriasis: recent insights, current challenges, and future prospects. Clin Cosmet Invest Dermatol. 2020;13:611–625. doi:10.2147/CCID.S227896
123. Jindal S, Awasthi R, Goyal K, Kulkarni GT. Hydrogels for localized drug delivery: a special emphasis on dermatologic applications. Dermatol Ther. 2022;35(11):e15830. doi:10.1111/dth.15830
124. Chen Y, Chen N, Feng X. The role of internal and external stimuli in the rational design of skin-specific drug delivery systems. Int J Pharm. 2021;592:120081. doi:10.1016/j.ijpharm.2020.120081
125. Feng X, Luo Y, Li F, Jian X, Liu Y. Development of natural-drugs-based low-molecular-weight supramolecular gels. Gels. 2021;7(3):105. doi:10.3390/gels7030105
126. Song Z, Sun J, Williams GR, et al. Glucan-based biomaterials and their applications in the biomedical field. Int J Biol Macromol. 2025;318(Pt 1):144940. doi:10.1016/j.ijbiomac.2025.144940
127. Jian X, Feng X, Luo Y, et al. Development, preparation, and biomedical applications of DNA-based hydrogels. Front Bioeng Biotechnol. 2021;9:661409. doi:10.3389/fbioe.2021.661409
128. Balde A, Kim SK, Nazeer RA. A review on microneedle patch as a delivery system for proteins/peptides and their applications in transdermal inflammation suppression. Int J Biol Macromol. 2025;307(Pt 2):141963. doi:10.1016/j.ijbiomac.2025.141963
129. Caminade AM, Turrin CO, Poupot R. Curing inflammatory diseases using phosphorous dendrimers. Wiley Interdiscip Rev -Nanomed Nanobiotechnol. 2022;14(4):e1783. doi:10.1002/wnan.1783
130. Yu H, Liu Y, Zheng F, Chen W, Wei K. Erianin-loaded photo-responsive dendrimer mesoporous silica nanoparticles: exploration of a psoriasis treatment method. Molecules. 2022;27(19):6328. doi:10.3390/molecules27196328
131. Bahadur S, Sharma M. Liposome based drug delivery for the management of psoriasis - a comprehensive review. Curr Pharm Biotechnol. 2023;24(11):1383–1396. doi:10.2174/1389201024666221213144228
132. Kapoor DU, Garg R, Maheshwari R, Gaur M, Sharma D, Prajapati BG. Advancing psoriasis drug delivery through topical liposomes. Z Naturforsch C J Biosci. 2025;80(3–4):41–60. doi:10.1515/znc-2024-0118
133. Lal DK, Kumar B, Saeedan AS, Ansari MN. An overview of nanoemulgels for bioavailability enhancement in inflammatory conditions via topical delivery. Pharmaceutics. 2023;15(4):1187. doi:10.3390/pharmaceutics15041187
134. Tang B, Bi Y, Zheng X, et al. The role of extracellular vesicles in the development and treatment of psoriasis: narrative review. Pharmaceutics. 2024;16(12):1586. doi:10.3390/pharmaceutics16121586
135. Born LJ, Khachemoune A. Extracellular vesicles: a comprehensive review of their roles as biomarkers and potential therapeutics in psoriasis and psoriatic arthritis. Clin Exp Dermatol. 2023;48(4):310–318. doi:10.1093/ced/llac108
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.