Back to Journals » Risk Management and Healthcare Policy » Volume 15
Advanced Practice Nurses’ Experiences on Patient Safety Culture in Hospital-Based Home Healthcare: A Qualitative Descriptive Study
Authors Lee S, Lee JY ![]() , Kim H
, Kim H ![]() , Lee K
, Lee K ![]() , Lee T
, Lee T ![]()
Received 7 September 2022
Accepted for publication 26 November 2022
Published 5 December 2022 Volume 2022:15 Pages 2297—2309
DOI https://doi.org/10.2147/RMHP.S388902
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Soohee Lee,1 Ji Yeon Lee,2 Hyejin Kim,3 Kayoung Lee,1 Taewha Lee4
1College of Nursing, Gachon University, Incheon, South Korea; 2College of Nursing, Yonsei University, Seoul, South Korea; 3Red Cross College of Nursing, Chung-Ang University, Seoul, South Korea; 4Mo-Im Kim Nursing Research Institute, Yonsei University College of Nursing, Seoul, South Korea
Correspondence: Kayoung Lee, Gachon University College of Nursing, 191 Hambakmoero, Yeonsu-Gu, Incheon, 21936, South Korea, Tel +82-32-820-4227, Email [email protected] Taewha Lee, Yonsei University, 50-1 Yonsei-ro, Seodaemun-gu, Seoul, 03722, South Korea, Tel +82-2-2227-8303, Email [email protected]
Purpose: Despite the increasing interest in patient safety, most research have been conducted in hospital settings, thereby demonstrating an overall lack of research regarding patient safety culture in home healthcare. South Korea has three types of home healthcare services based on hospitals, public health centers, and long-term care insurance. Home healthcare nurses in hospitals require a master’s degree and advanced nursing skills. They play important roles in ensuring patients’ safe transition into home health care. This study aimed to explore the experience of patient safety culture among South Korean advanced practice nurses in hospital-based home healthcare.
Methods: This qualitative descriptive study was conducted through purposive sampling, whereby twenty advanced practice nurses involved in home healthcare were recruited from twelve hospitals located in three different cities throughout South Korea. Face-to-face semi-structured interviews were conducted, and the collected data were analyzed through inductive and deductive content analyses.
Results: Three main categories were finally confirmed: (a) teamwork climate, (b) safety climate, and (c) working condition. The sub-categories of the teamwork climate included the collaboration between patients, caregivers, and nurses, collaboration within medical institutions, and collaboration among the individuals involved in community partnerships. The sub-categories of the safety climate included nurses’ commitment to patient safety, the associated institutions’ commitment to patient safety, and the government’s commitment to patient safety. The sub-categories of the working condition included the frontline working environments and the associated institutions’ support aimed at ensuring effective working environments.
Conclusion: Cultivating patient safety culture is crucial for ensuring the safe transition of patients from acute care hospitals to home healthcare. This study revealed significant aspects of patient safety culture in hospital-based home healthcare, allowing for the continuum of care among the associated patients. Such aspects include communicating with caregivers, building community partnerships, understanding unexpected home environments, and enhancing the safety of nurses.
Keywords: patient safety, home care services, hospital-based, qualitative research
Introduction
In the report titled “To Err Is Human”, the Institute of Medicine (IOM) presented various medical errors and suggested enhancing patient safety culture in health care organizations as the first step towards improving the quality of care among patients.1 Patient safety culture refers to the extent to which medical organizations support and promote patient safety by incorporating various values, beliefs, and norms that must be adopted by healthcare providers throughout such organizations.2 Numerous studies on patient safety culture have been conducted in acute care hospital settings,3 whereas patient safety culture in home healthcare settings has received relatively less attention.4,5
Regardless of the small number of studies on patient safety culture in home healthcare contexts, ensuring patient safety culture in home healthcare environments is crucial for enhancing the quality of care.6 Regarding patients discharged from acute care hospitals as a result of sub-acute symptoms, nurses involved in home healthcare play a significant role in ensuring the safe transition of such patients into home healthcare. Therefore, it is necessary for nurses providing home healthcare to be aware of the importance of patient safety.
There has also been a growing interest in patient safety in South Korea.7 The Korean government enacted the Patient Safety Act in 2015, and as a result, many hospitals currently focus their efforts on promoting and improving the quality of care by cultivating patient safety culture. However, few studies associated with home healthcare settings have been conducted.8 Currently, in South Korea, there are 180 home healthcare facilities,9 and they can be categorized into hospital-based home healthcare services, home visiting healthcare services based on public health centers, and home visiting nursing services based on long-term care insurance.10,11 Each category involves different staff mixes, home healthcare activities, and various types of patients with differently-severe medical conditions.10 Among these categories, this study focused on hospital-based home healthcare services requiring significantly complex nursing skills and higher education-based qualifications for ensuring the transition of patients from acute care hospitals to home healthcare environments.
Although hospital and home healthcare approaches differ depending on individual medical organizational contexts, most studies on patient safety culture, as it pertains to home healthcare, adopt varying definitions, assessments, and implementations of the patient safety culture approach developed in various hospital settings without sufficient supporting evidence.4,5 Therefore, this study explores the experiences of patient safety culture among home healthcare nurses providing hospital-based home healthcare in South Korea.
Methods
Study Design and Aim
This study used a qualitative descriptive design to describe advanced nurses’ perceptions of patient safety culture and safety management activities in hospital-based home healthcare in South Korea. When conducting health care studies, a qualitative descriptive design is beneficial in that the collected interview data can be used to capture detailed descriptions of the participants’ experiences in a straightforward and focused manner, thereby providing data that enables an enhanced understanding of the different phenomena involved.12
Participants and Settings
Purposive sampling was used to select the participants involved in this study. The participants were recruited from 12 hospitals located in three different cities throughout South Korea. Based on the full list of hostpial-based home healthcare center/units provided by Health Insurance Review and Assessment Service of Korea, two researchers contacted the unit managers through email and telephone, and recruited the participants according to the selection criteria. The inclusion criteria were as follows: (a) certified advanced practice nurses (APNs) specializing in home healthcare and (b) certified APNs affiliated with primary, general, or tertiary hospitals, as categorized by the Korean Health Insurance Review and Assessment Service. The exclusion criteria involved home-visiting nurses (a) affiliated with public health centers or (b) those providing home visiting nursing services covered by long-term care insurance policies.
Data Collection
As shown in Table 1, the data used in this study were collected from January 2019 to September 2019 through individual, face-to-face, and semi-structured interviews. These interviews were conducted in calm environments, such as the participants’ affiliated hospitals. When conducting the interviews in each hospital, a place with a calm environment was requested to ensure minimal distractions and maintain confidentiality. The interviews lasted for approximately 30–50 min. The researcher recorded field notes and collected information regarding the participants’ demographic backgrounds (age, gender, duration of clinical experiences, position, working times, and education) at the end of the interviews. The participants involved in this study received a $50 gift card after the interviews. During data collection, the data were preliminary analyzed when it began to repeat.
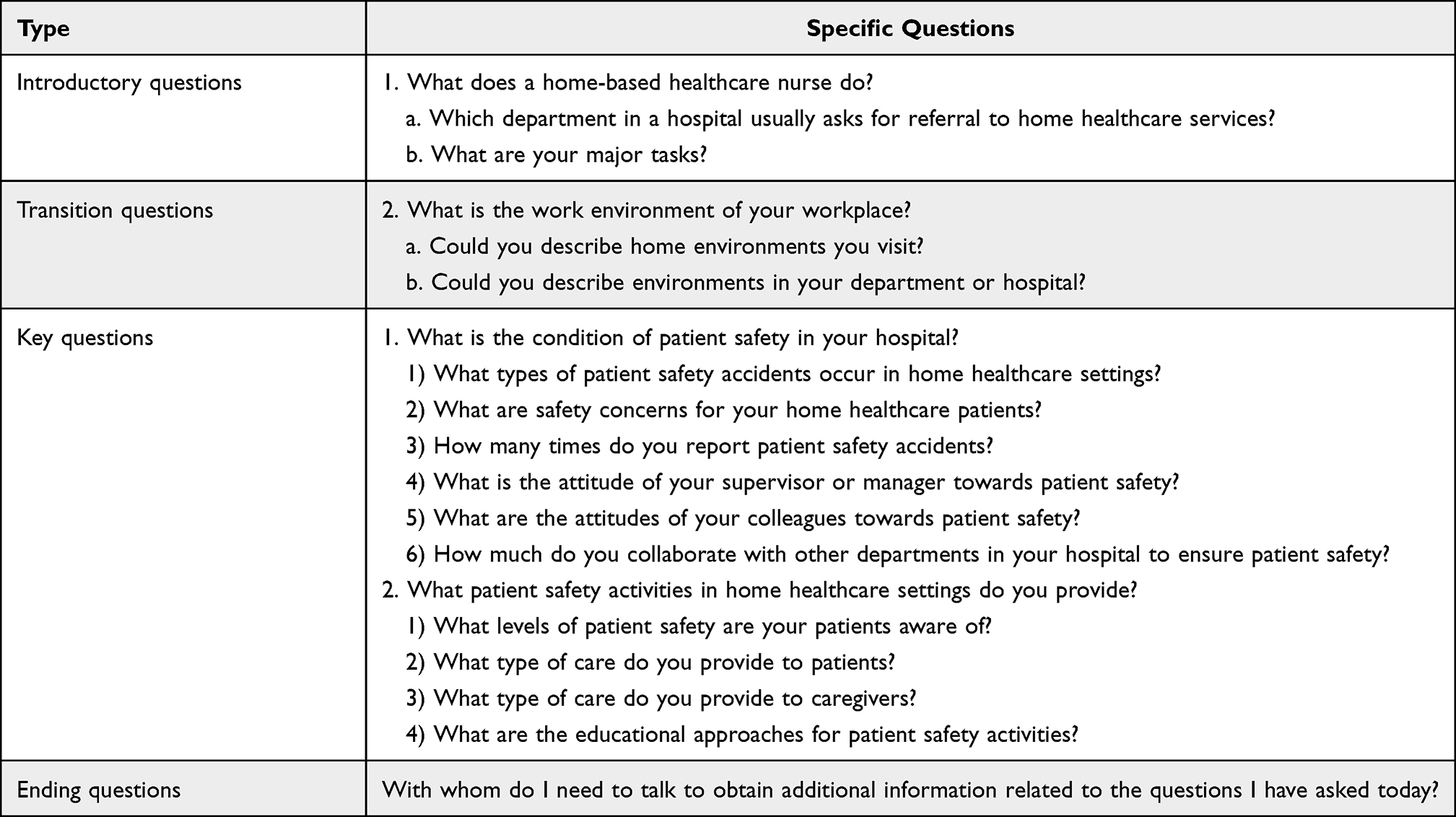 |
Table 1 Interview Guide Questions |
When preliminary analyses revealed a point at which no new information could be obtained, data saturation was considered to have been achieved. Code saturation was achieved upon interviewing 20 participants. Repeat interviews were not conducted in this study.
Data Analysis
To ensure the study’s credibility, all the interviews conducted were recorded in audio format, after which the recordings were transcribed verbatim. The transcripts and field notes were used for data analysis. This study used inductive and deductive content analyses to analyze the collected data.13,14 Regarding deductive content analysis, six predetermined categories of patient safety culture were developed based on the Safety Attitudes Questionnaire,15 which is a reliable and valid tool for evaluating healthcare providers’ attitudes towards issues relevant to patient safety, ie, safety climate or safety culture. The original tool comprises six predetermined categories: (a) teamwork climate, (b) safety climate, (c) job satisfaction, (d) stress recognition, (e) perception of management, and (f) working condition. A primary codebook was created using the content analysis approach.14 Two team members read the same transcripts separately, after which they generated codes. The generated codes were then aggregated into sub-categories, and thereby resulting in a categorization frame involving six predetermined categories. Then, three main categories (teamwork climate, safety climate, and working condition) and their sub-categories were refined through inductive content analysis. Active discussions were held to achieve consensus among all the researchers conducting this study. This iterative process ensured the consistency and comprehensive understanding of the data collected through the interviews. Data analysis proceeded until no further categories could be derived from the data. This study used NVivo software (release 1.4.1) for data management and analysis.
COREQ Guideline
This study was conducted and reported in accordance with the guidelines provided in the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist16(Supplementary Table 1).
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Yonsei University (approval number: Y-2020-0095). Informed consent was obtained from all participants. The participants’ informed consent included publication of anonymized responses and the rights to withdraw from participation at any time during the study. All the information regarding this study, including the researchers’ contact information, was duly provided. Anonymity was guaranteed throughout the research process associated with this study. The well-being of the participants involved in this study was monitored throughout the interviews.
Trustworthiness
This study relied on the aspects of credibility, transferability, dependability, and confirmability to establish trustworthiness and ensure that the findings of this study reflected the participants’ perspectives.17 Credibility was ensured through prolonged engagement and persistent observations. The participants involved in this study were encouraged to support their statements using detailed examples. The interviewers also asked follow-up questions. Additionally, the members of the research team constantly read and re-read the data, and they re-labeled the associated codes until the final core categories were revealed. Throughout this study, transferability was ensured by providing a rich description of the associated categories, including the participants’ attitudes, experiences, and contextual aspects. Dependability was established through the detailed description of the processes used for the collection and analyses of the data. Confirmability was achieved through the formulation of a composite research team and through discussions regarding the potential biases that may affect the interpretation of this study’s findings. In this study, the achievement of the confirmability aspect involved engaging two APNs (nurse practitioners) and three registered nurses (non-APNs), with community nursing, home healthcare nursing, or nursing management being their primary research interests.
Results
In this study, semi-structured interviews involving 20 home healthcare APNs were conducted. The characteristics of the participants are listed and described in Table 2. Most of the APNs involved in this study had a master’s degree or higher (n = 16, 80%), and they are currently working in large-sized (tertiary) hospitals (n = 15, 75%).
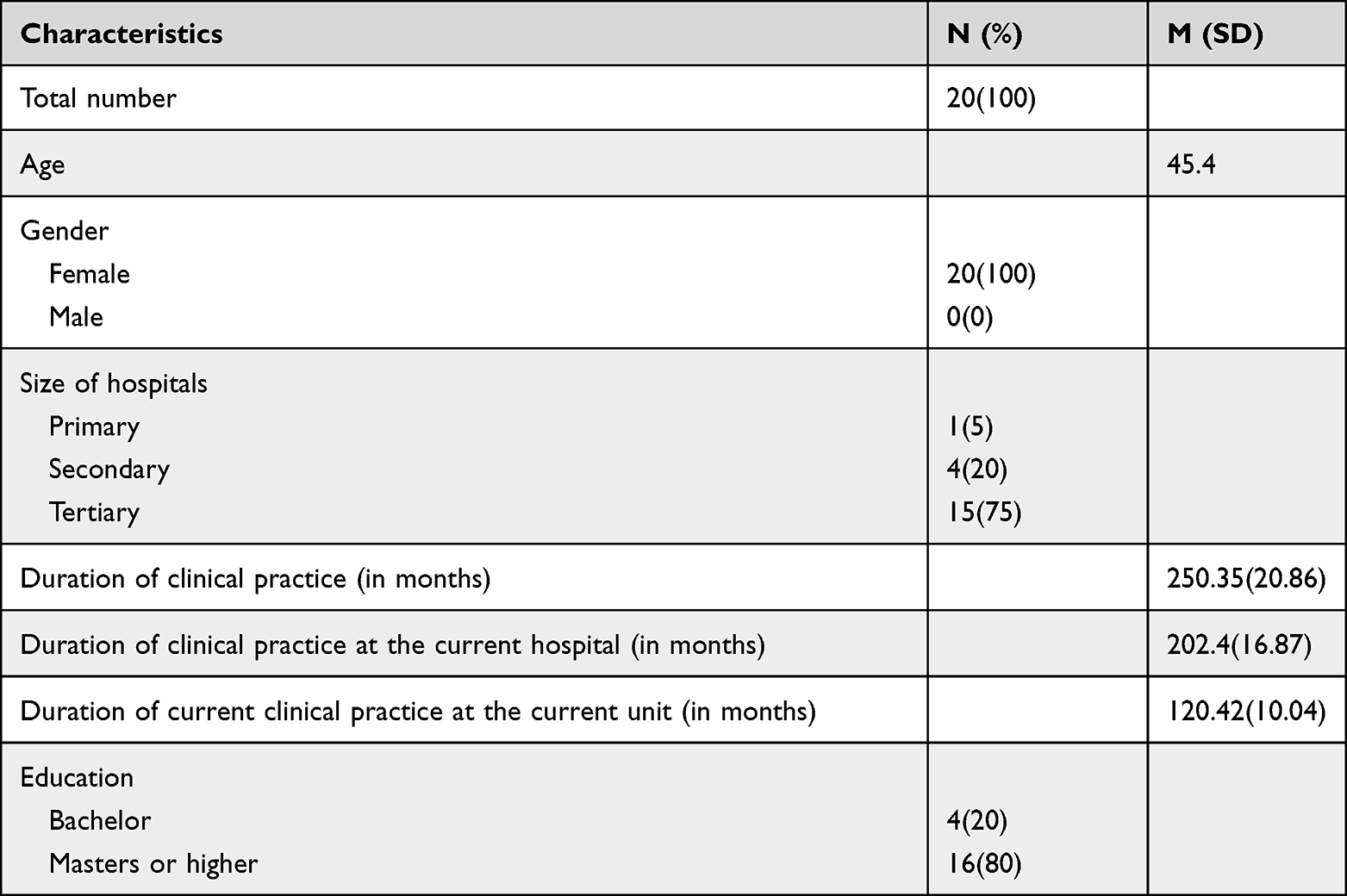 |
Table 2 Characteristics of Participants (n=20) |
After the inductive and deductive content analyses, three main categories and eight sub-categories associated with nurses’ experiences on patient safety culture in home healthcare contexts were finally confirmed (Table 3). Such categories included (a) teamwork climate, (b) safety climate, and (c) working condition. Among the categorization frame involving six categories, job satisfaction, stress recognition, and the perception of management were finally deleted owing to insufficient codes, and some codes were aggregated into the three main categories. The main categories, sub-categories, and condensed meaning units are listed in Table 4.
 |
Table 3 Categorization Matrix for Deductive Content Analysis |
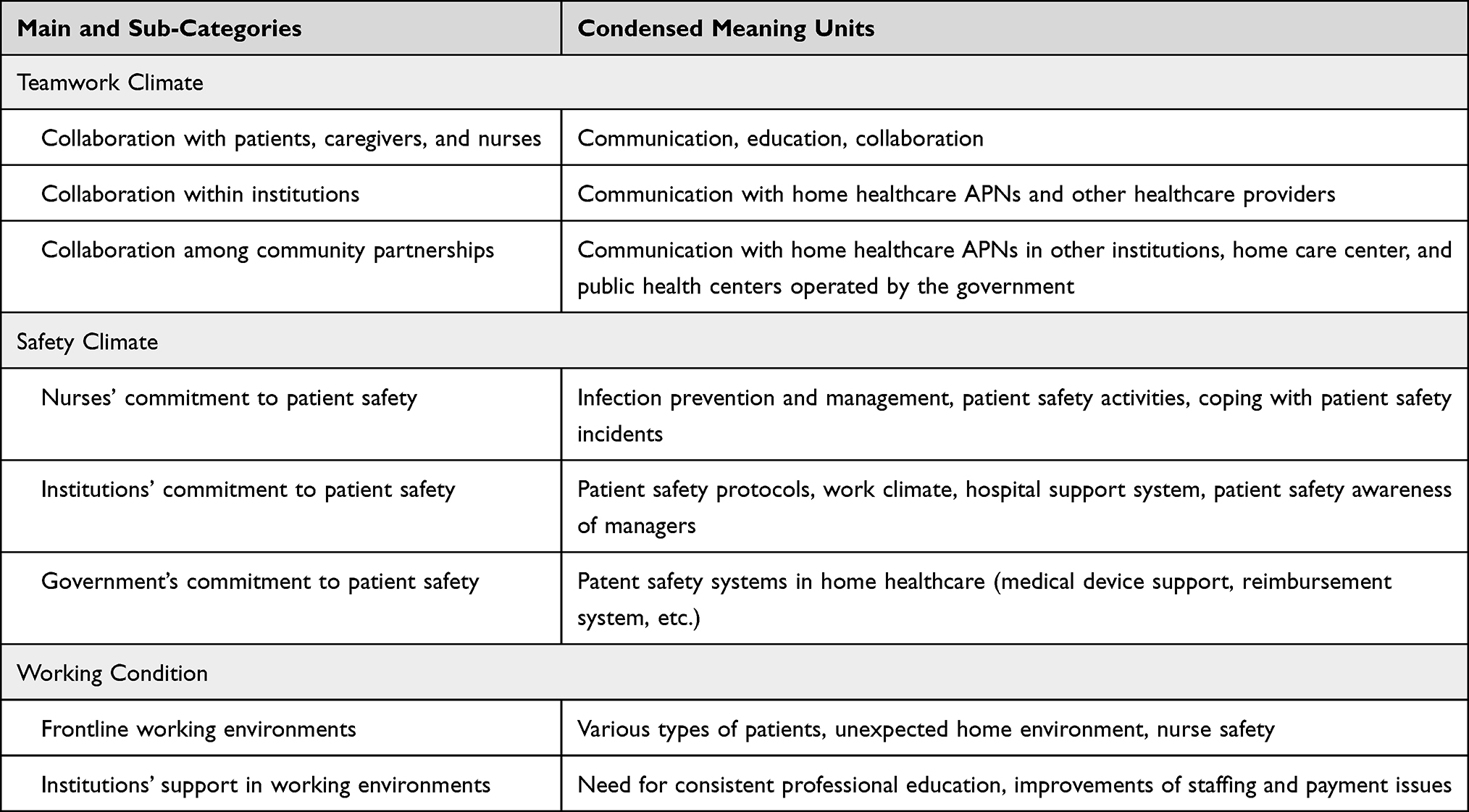 |
Table 4 Main and Sub-Categories, Code Frequencies, Condensed Meaning Units |
Teamwork Climate
Collaboration with Patients, Caregivers, and Nurses
Collaboration with patients, caregivers, and nurses is crucial for promoting a patient safety culture. In home care environments, providing care to patients for 24 hours is more challenging than providing the same in hospital settings. This is because, in hospital settings, healthcare providers can respond to medical emergencies immediately. Collaboration is a multiple-way process that involves patient education provided by nurses as well as the active engagement of patients and caregivers during nursing care processes. A home healthcare nurse states that during routine advanced nursing procedures, such as a tracheostomy tube change for an unconscious patient, two-way collaborations, such as verbal encouragement from the nurses and the patient’s reaction, are significantly helpful in ensuring highly safe environments for the effective provision of home healthcare.
Unconscious patients can still hear. When I talk to unconscious patients requiring a tracheostomy change and say, “I am your nurse, and I am here”, I may get no response from such patients, but there surely is something. When I say, “Can you do a good job today like the last time?” they move their neck like this. (P01)
At home, patients have various caregivers, such as family, personal care assistants, or unlicensed assistive personnel. Among various caregivers, their relationships and roles are complex and dynamic. Therefore, in home healthcare settings, it is imperative to actively communicate patients’ conditions and the associated home healthcare procedures among home healthcare APNs, their patients, and the various types of caregivers, including family members.
If any symptoms appear, as nurses, we investigate such symptoms immediately and treat them using medications as well as other approaches. Therefore, I believe that these approaches, as well as the drugs administered, can be considered aspects of collaboration and education. (P02)
Collaboration Within Institutions
To ensure patient safety culture, home healthcare APNs frequently share their care experiences through instant messaging tools to communicate with their colleagues. These shared experiences help such medical professionals to identify specific aspects they may have missed nursing care when providing home healthcare. Additionally, in such contexts and when necessary, home healthcare APNs provide significant help to their colleagues. Moreover, there is a care plan that involves meeting with other health care providers every day, week, or month. Such professional interactions promote the implementation of best practices among nursing professionals as they provide care to patients requiring home healthcare.
After completing home healthcare visits, we share what the patients were like and what we explained among ourselves. Therefore, after patients tell me what they were told previously, I double-check with my colleagues, after which I call the patients later to provide further explanations and give further instructions. (P09)
In the context of hospital-based home healthcare, home healthcare APNs often work with other healthcare providers in the hospital. Medical institutions usually have technical support systems, thereby ensuring that home healthcare APNs can easily communicate with other healthcare providers in the institutions. Such technical support systems enhance the continuum of care among patients requiring home healthcare.
If we call the emergency department of a medical institution and inform them in advance that one of our patients is going to their emergency department for a specific problem, even if it is not a priority, if we notify them in advance, they can reduce the amount of time spent asking why the patient came to the emergency room (ER), thereby ensuring the continuum of care among such patients. (P02)
Collaboration Among Community Partnerships
Various types of community partnerships ensure the provision of home healthcare. They include public health care centers funded by the government or home care centers funded through long-term care insurance policies. Although they belong to different medical institutions, nurses providing home healthcare in different communities have a communication network that allows them to share information.
In a way, compared to nursing professionals working at the same hospital, those who play similar roles in similar areas have a more special connection, and they take part in meaningful discussions, whether they are hospital workers or visiting nurses at public health centers. (P20)
Sometimes, patients that are assigned home healthcare APNs are admitted to long-term care facilities. In such cases, communication processes between the associated care workers and the assigned APNs can be complex and ineffective. Although home healthcare APNs record and communicate their visits with a patient’s family, care workers in long-term care facilities often ask APNs specializing in home healthcare to inform them directly. When such home healthcare APNs perceive that care workers have inadequate levels of education on patient safety, the training of care workers becomes another issue. In such contexts, the healthcare delivery process in accordance with physicians’ orders also becomes significantly complex. For example, if a blood sample is required, the physicians in the institutions to which the APNs specializing in home healthcare belong must send a referral to the physicians in the associated long-term care facilities.
We can visit immediately, but only if the visiting doctor shares the blood tests required with the patient’s primary care provider at a specific hospital, after which the primary care provider orders the required blood tests. (P02)
Safety Climate
Nurses’ Commitment to Patient Safety
Home healthcare APNs play a critical role in ensuring patient safety because individual home environments are unique and different, and as a result, such different environments may affect patient safety. For example, uncontrolled or untrained pets, home dust, or slippery floors can increase the risks of getting infections or injuries among patients. Moreover, many home healthcare patients are seniors who may have cognitive impairments that prevent them from understanding education, eg, discharge education. In such cases, home healthcare APNs may need to provide patient education using teach-back methods. Therefore, the roles of APNs vary from environmental inspection to education provision.
Among cancer patients, we identify the number of pets as well as the number of stuffed animals they have in the house. For respiratory disease patients, we tell them to put away all the stuffed animals because of dust. (P01)
There are some restrictions associated with managing patient safety in home healthcare settings. Because the visiting hours for home healthcare provision are significantly limited, most issues associated with patient safety occur during non-visiting hours. Additionally, in the context of home healthcare, there is no 24-hour monitoring for patients. Moreover, home healthcare APNs have decreased control over the associated situations and less responsibility for issues related to patient safety that occur during non-visiting hours. Regarding special equipment, such as home ventilators, the companies that invent such equipment are responsible for managing patients and responding to their emergencies.
Regarding accidents that occur in patients’ homes when I am not around, I have to say that I do not feel as responsible as I do when it comes to accidents that occur within hospital environments. (P04)
Institutions’ Commitment to Patient Safety
Most hospitals have a manual for patient safety, and they regularly provide education on enhancing patient safety among APNs specializing in home healthcare. Additionally, most hospitals support the provision of medical equipment and supplies in such contexts. Although most hospitals provide a specific manual, such as that involving the management of the vehicles used for home visits, most of the manuals are designed for hospitalized patients, thereby requiring new manuals tailored for home healthcare contexts. For instance, home healthcare APNs demonstrate that the manual for contact precautions is unreliable, and as a result, they concern themselves with managing patients’ symptoms for vancomycin-resistant enterococci (VRE) following their release from quarantine, without a culture.
In hospitals, the contact management for VRE and methicillin-resistant staphylococcus aureus (MRSA) is on a different level. Apart from infection management, every aspect is under watch in all hospitals. Regardless of whether it is MRSA or VRE, we perceive it similarly. However, the quarantine for such is lifted following a certain period after a patient is discharged from the hospital, and we are supposed to follow the general protocols applied to any other patient. I am not really sure whether this is the correct approach. (P09)
When APNs specializing in home healthcare APNs perceive problems with a patient care, they use their hospital’s report system. Some present the issues to the nurse in charge or the manager, whereas others solve the issues by engaging in discussions with physicians before reporting. If the manager and the team are supportive, home healthcare APNs are willing to share the patient’s safety concerns. If not, it is difficult to speak up. Regarding patient safety incidents, APNs specializing in home healthcare report the cases that occur on their watch.
First, we are in an environment where we are supposed to speak up. Therefore, I do not feel like hiding anything. In terms of the solution, we do not ask, “Why did you focus on that?” Rather, we ask, “How did you deal with it after?” and “What do you want the hospital to help you with next?” (P04)
Government’s Commitment to Patient Safety
Policies significantly influence the quality of patient safety culture. In South Korea, long-term care insurance systems assist patients requiring home healthcare nursing by covering rental fees for a medically necessary adjustable bed, mattress, and chair, among other requirements. However, currently, the reimbursement system for nursing services is not well established. For example, in South Korea, the healthcare insurance system does not pay for home healthcare nursing services for patients not undergoing physician-recommended treatments. Owing to this problem, the care provided to patients could be intermittent and discontinuous.
In the meantime, owing to the current reimbursement system, we are not allowed to visit just to check on the patient’s condition or to provide education without treatment recommendations from a physician. (P16)
The number of patients to whom home healthcare APNs provide care daily varies. When home healthcare APNs visit an additional number of patients, or when the distance to a patient is far, such APNs might provide poor quality of care. Moreover, the government is yet to provide a manual for providing care to patients with contact precautions in different communities, and this attribute may result in increased safety risks among patients.
We set the number as high as possible. Yesterday, I inserted the L-tube. The entire process lasted for only 10 minutes from entering the house, washing my hands, checking the vitals, inserting the tube, and confirming that everything was all right. Afterward, the process was complete, and I could leave without doing anything else. However, it took 40 minutes to sit and talk with the caregivers about the past month and the events that occurred, among other things. Therefore, in such situations, I may get out of the house 50 minutes later. However, then, that was possible because I only had to visit three patients that morning, and thus, I had some time to spare, but let us assume that I had to go to Anyang to visit six or seven patients. In such a case, I would not be able to spend that much time in one place. (P07)
Working Condition
Frontline Working Environments
Unlike in hospital settings, frontline working environments in home healthcare settings vary. Because physicians engaged in various medical specialties, such as internal medicine, cardiovascular medicine, oncology, general surgery, neurosurgery, obstetrics and gynecology, pediatric medicine, and ophthalmology, must provide consultation for home healthcare services, the types of patients vary significantly, and such patients require different nursing approaches and activities. Moreover, home healthcare APNs are used to visiting patients requiring continuous care after discharge from the hospital, and there are special requests for patients suffering from terminal illnesses and those suffering from contagious diseases. When providing care to such patients, home healthcare APNs can experience emotional exhaustion and other difficulties that can have a negative impact on patient safety.
Because we have a cancer center, over 50% of patients requiring home-based healthcare are cancer patients. However, it is well-known that cancer patients require a lot of care throughout the treatment process. Such care involves the management of the central venous catheter, hydration, and administering auxiliary treatment medications in between treatment regimens. All these services can be provided in the outpatient clinic. However, the outpatient clinic is so crowded that even chemotherapy is not convenient. Therefore, everyone in our visiting area asks us to carry out these tasks. (P10)
The residential environments of patients requiring home healthcare are also diverse. Most home nursing care is provided in the patients’ homes. The housing conditions of patients vary. Some patients live in large houses with excellent indoor environments, whereas others live in single rooms with substandard conditions. As home healthcare expands, patients that are discharged early become clients of home healthcare nursing, and they sometimes request to meet in their working places, which do not often provide suitable areas or supplies. Additionally, home healthcare APNs re visit not only the patients’ homes but also the facilities to which they go for treatment or are admitted, such as long-term care facilities or postpartum care centers. Such facilities do not always welcome home healthcare APNs, and in some cases, such facilities even deny visits from these medical professionals.
I even go to patients’ workplaces. Sometimes. It is significantly inconvenient. In many cases, there is no separate designated space, such as an infirmary, in the patients’ workplaces. The reason why we go to patients’ workplaces is that some patients are discharged from the hospital early on the condition that they will receive home healthcare. (P05)
Home healthcare APNs often face unexpected and unprecedented situations posing risks to their health and well-being. Because home healthcare APNs work alone in the field, they often feel stressed owing to the uncertainties associated with conducting home visits. Such medical professionals face various safety risks, including aggressive patients or caregivers, sexual harassment, hostile pets, exposure to infections, car accidents, and bad weather. Home healthcare APNs often ask patients’ families to stay around during visits. However, many patients do not have families or caregivers. Additionally, in some cases, patients’ family members threaten the APNs providing home healthcare services.
We should think about the safety of patients, the safety of caregivers, and the safety of visiting nurses. However, currently, there are a lot of caregivers with a predisposition to psychological problems. Usually, in almost 90% of the cases in South Korea, home healthcare is provided by one visiting person. Therefore, it is about time we considered the safety of the nurses and that of other individuals providing home healthcare services. (P18)
Institutions’ Support in Working Environments
Hospitals provide mandatory or non-mandatory education programs on patient safety. As such programs are targeted at all healthcare providers in hospitals, the contents are not specified for home healthcare APNs. To complement such educational strategies, home healthcare APNs should participate in the seminars hosted by the Academic Society of Home Health Care Nursing or APN units specializing in home healthcare should occasionally develop self-training programs.
They do not seem to care about the safety of discharged patients in their homes. Safety management is primarily dedicated to the prevention of accidents inside hospitals. (P16)
Despite support from medical institutions, the working conditions of home healthcare APNs remain substandard. Many APN units specializing in home healthcare prefer a team-based nursing approach to primary nursing because the number of home healthcare APNs is insufficient, ie, 3–5. In team-based contexts, these medical professionals share their patients’ information and take turns when conducting home visits. If the number of patients requiring home visits is too large, or if the distance to the target patients is too far, the quality of care can be affected. Some home healthcare APNs are not under full-time employment contracts, and as a result, they receive low payments. Moreover, requests for administrative support, such as the provision of devices that enable the secure storage of medication, addressing issues related to vehicles for transportation, and assistants for helping in the provision of home nursing care during home visits, remain persistent.
When a nurse visits a patient, to invest enough time and effort, if there is an hour or two to spare for a small number of patients, the quality of nursing care will improve significantly. However, the university hospital systems in this country are not like that, and therefore, the same challenges will be experienced in private hospitals. (P07)
Discussion
This study explored the experiences of patient safety culture among APNs specializing in the provision of home healthcare. In this study, patient safety culture was finally classified into three categories: teamwork climate, safety climate, and working condition. The findings of this study are similar to those of other studies, as they pertain to the understanding of various perspectives on patient safety culture.18 Colla et al reviewed nine instruments for evaluating patient safety culture, and they came up with five prevalent dimensions for ensuring patient safety: climate leadership, policies and procedures, staffing, communication, and reporting.18 Consistent with the results presented in previous studies, the results of this study demonstrated that teamwork climate is significantly related to communication, safety climate includes policies, procedures, and reporting, and working conditions are significantly related to staffing procedures.18
The findings of this study showed that home healthcare APNs perceived teamwork climate as a crucial aspect for achieving effective patient safety culture. This finding reflects those of previous studies.19,20 Using the Brazilian version of the self-assessment questionnaire (SAQ), Lousada et al evaluated patient safety culture in home healthcare settings in Brazil, and they established that teamwork achieved high scores in home healthcare services.19 Using the Norwegian version of the AHRQ Hospital Survey on Patient Safety Culture (NHSOPSC), Ree and Wiig also reported that teamwork positively affected the provision of home healthcare services in Norway.20 Specifically, home healthcare APNs collaborate with their colleagues in various medical institutions as well as with patients and caregivers. Additionally, they build community partnerships. This broadened objective of communication can account for the characteristics of APN teams, such as small team size, daily patient assignment systems, multiple caregivers, and fluctuated home environments. The role of caregivers is specifically important in home healthcare because it enables the prevention of accidents among patients as most accidents among such home healthcare patients occur during the hours in which home healthcare APNs do not conduct home visits. The importance of effective communication with patients, caregivers, and nurses is also demonstrated in other studies.21,22 Lang et al explored safety issues in Canadian home healthcare settings, and they established that the relationships and communication among patients and their families and caregivers and their providers are inextricably linked.21 Yoon and Wu identified the relationship between family and teamwork as the perception of patient safety in Korean nursing homes.22 Therefore, home healthcare APNs must be aware of the importance of collaboration between a wide range of aspects to enhance patient safety in home healthcare settings.
The next section of our findings involves the aspect of safety climate categorized into different levels, ie, nurses, institutions, and governments, as they pertain to commitments associated with ensuring patient safety. Because the surrounding environments in home healthcare settings vary and are unpredictable compared to those of other healthcare settings,23 home healthcare APNs must pay more attention to ensure patient safety. Although medical institutions and the government are currently engaged in extensive efforts aimed at addressing the issues related to patient safety, most support is focused on inpatient settings.24,25 For example, institutions used to provide the same standard patient safety manuals for hospitalized patients and home healthcare patients. Another example is that institutions provide APNs with a manual for contact precautions at different levels. The home care setting could be regarded as an isolated space. However, evidence showing that infection prevention and control approaches employed in home healthcare settings are safe is not enough. A study that described patient safety in home healthcare nursing pointed out incorrect or outdated routines and guidelines in home healthcare settings.4 Therefore, medical institutions and governments must be aware of patient safety in home healthcare settings in different ways. Another interesting finding is that there is a controversial discussion on reporting issues associated with patient safety. It is unclear to what extent home healthcare APNs have to provide reports, eg, in cases that occur during non-visiting hours. This finding could be the reason why the responses of participants in-home healthcare units have a low reporting rate of near-missed events and potentially harmful events.20,26
This study divides working condition in home healthcare settings into frontline working environments and institutional support. Home healthcare APNs encounter complex frontline working environments. They meet various patients in different disease groups, which could burden home healthcare APNs because these medical professionals must prepare care in different contexts.9,23,27 Patients’ residential environments also vary. Poor home environments can not only impede patient care but also threaten the safety of home healthcare APNs.23 The safety of home healthcare APNs is a crucial issue. Home healthcare APNs are placed under unexpected situations, such as threats from patients or caregivers, traffic accidents, bad weather, and exposure to infections.28,29 Despite these threats related to the working environment, institutional support and formal policies aimed at enhancing nurses’ safety are limited. For example, there are few standard practice guidelines for dealing with such threats. Although the Health Insurance Review and Assessment Service of Korea allows for a limited number of visits (seven visits a day on a monthly average) for home healthcare APNs in nursing homes,30 the institutions used to have a low nurse staffing level that could physically and emotionally burden home healthcare APNs. These findings are similar to those of other studies. Lousada et al established that work condition had the lowest scores among six dimensions of patient safety culture in home healthcare settings.19 Ree and Wiig also reported low scores on staffing, training, and skills in home healthcare settings.20 As this study pointed out previously, Johannessen et al mentioned several challenges in the quality and safety of work conducted in home healthcare settings. Managers have to improve efficiency, which could sometimes result in a low quality of care, and these researchers also reported difficulties with nursing coverage.26
The strength of this study is that it contributes to further insights into the experience of patient safety culture among home healthcare APNs. Despite abundant studies on patient safety,3,6 there are few studies on patient safety in home healthcare settings. There are some consensus-related aspects of patient safety in hospitals and home healthcare settings. However, patient safety culture in hospital settings might not adequately capture the complex nature of home healthcare services. This study has several limitations. The first limitation involves the lack of generality throughout the population. The study involved home healthcare APNs working at hospitals that may have improved systems and supports for home healthcare APNs. There could be some differences in the structures or contexts between hospital-based home healthcare services and purely home healthcare services provided by public health centers and through coverage by long-term care insurance policies. Moreover, this study recruited participants from three major cities in Korea. This means that we may have missed some local barriers affecting the perspectives of patient safety among home healthcare APNs in small towns. Second, this study used a qualitative descriptive approach. Further research using in-depth qualitative or quantitative approaches is required to achieve conclusive results.
This study can be implemented in the planning for the implementation of best practices for ensuring patient safety among home healthcare APNs. To enhance patient safety, education programs targeted at caregivers could be developed. Medical institutions and governments must understand the different aspects of patient safety in home healthcare settings. They can consider the several important points presented in this study to provide highly positive safety cultures among home healthcare APNs. For example, medical institutions can provide escorts to APNs during home visits to ensure their safety, and governments can implement policies aimed at protecting nurses from threats and increasing nurse staffing levels. Regarding the patient safety guidelines, we must approach this subject carefully. Although the standard guidelines do not reflect some aspects related to home healthcare, determining to what extent the guidelines are tailored for home healthcare settings is not easy. As Johannessen et al mentioned, new national plans and guidelines can result in increased workloads, thereby impeding the continuity of care.26 Therefore, further research on this matter is required.
Conclusion
To ensure the safe transition from acute care hospitals to home healthcare among patients, cultivating patient safety culture in home healthcare settings is imperative. This study shows some distinctive aspects of patient safety culture, as it pertains to hospital-based home healthcare services. First, teamwork is essential in the provision of home healthcare. Home healthcare APNs must communicate and collaborate with not only patients and caregivers but also colleagues as well as medical professionals involved in community partnerships. Second, regarding the safety climate, the roles of home healthcare nurses are crucial. Therefore, the education of nurses and home healthcare providers might be essential to enhance patient safety. In addition, medical institutions might need to develop tailored protocols or guidelines, and governments might need to increase their efforts in understanding different aspects of patient safety culture in home healthcare settings. Moreover, in home healthcare settings, the working conditions are significantly complex. Further research must be conducted to determine the best way to establish tailored guidelines without impeding care continuity. Finally, the support provided by medical institutions for both patient safety and nurse safety is crucial. These findings will provide further insights into understanding and promoting patient safety culture in hospital-based home healthcare settings.
Ethical Considerations
This study was approved by the Yonsei University Institutional Review Board (Y-2018-0095). All the participants received oral and written information. Participation in this study was voluntary, and anonymity was guaranteed throughout the research process. The participants involved in this study provided informed written consent for their participation in the study. The participants were informed of their right to withdraw from participation at any time during the study. The information involved in this study, including the researchers’ contact information, was provided. The safety and well-being of the participants were monitored throughout the interviews.
Funding
This study was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (2018R1A6A3A01012296); the Korea government (MSIT) (2021R1C1C2011587); and the Gachon University research fund of 2020 (GCU-202008420002).
Disclosure
The authors report no conflicts of interest in this study.
References
1. Institute of Medicine. (US) committee on quality of health care in America. In: Kohn LT, Corrigan JM, Donaldson MS, editors. To Err is Human: Building a Safer Health System. Washington (DC): National Academies Press; 2000.
2. Sorra J, Gray L, Streagle S, et al. AHRQ Hospital survey on patient safety culture: user’s guide. (prepared by westat, under Contract No. HHSA290201300003C). AHRQ Publication No. 18-0036-EF (Replaces 04-0041, 15 (16)-0049-EF). Rockville, MD: Agency for Healthcare Research and Quality; 2018. Available from: https://www.ahrq.gov/sops/qualitypatient-safety/patientsafetyculture/hospital/index.html.
3. Hwang JY, Kim JK. A literature review of patient safety in Korea: focused on domestic studies. J Korean Soc Dent Hyg. 2018;18(1):1–8. doi:10.13065/jksdh.2018.18.01.1
4. Lee SE, Scott LD, Dahinten VS, Vincent C, Lopez KD, Park CG. Safety culture, patient safety, and quality of care outcomes: a literature review. West J Nurs Res. 2019;41(2):279–304. doi:10.1177/0193945917747416
5. Berland A, Holm AL, Gundersen D, Bentsen SB. Patient safety culture in home care: experiences of home-care nurses. J Nurs Manag. 2012;20(6):794–801. doi:10.1111/j.1365-2834.2012.01461.x
6. Gartshore E, Waring J, Timmons S. Patient safety culture in care homes for older people: a scoping review. BMC Health Serv Res. 2017;17(1):752. doi:10.1186/s12913-017-2713-2
7. Byun J, Kim H. A study on the research trends in visiting nursing in South Korea. J Converg Inf Technol. 2019;9(11):71–80. doi:10.22156/CS4SMB.2019.9.11.071
8. Yount N, Zebrak KA, Famolaro T, Sorra J, Birch R. Linking patient safety culture to quality ratings in the nursing home setting. J Appl Gerontol. 2022;41(1):73–81. doi:10.1177/0733464820969283
9. Korean homehealthcare nurses association. Seoul: Status of Home Nursing Institution; 2022. Available from: http://www.hcna.or.kr/sub2/2_7.php.
10. Song CR. Role of hospital-based home health nursing in community care. J Korean Acad Soc Home Health Care Nurs. 2022;29(1):5–17.
11. Kim KS, Kang SJ, Kim BJ, et al. Theory and Practice of Community Health Nursing.
12. Kim H, Sefcik JS, Bradway C. Characteristics of qualitative descriptive studies: a systematic review. Res Nurs Health. 2017;40(1):23–42. doi:10.1002/nur.21768
13. Azungah T. Qualitative research: deductive and inductive approaches to data analysis. Qual Res J. 2018;18(4):383–400. doi:10.1108/QRJ-D-18-00035
14. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
15. Sexton JB, Helmreich RL, Neilands TB, et al. The safety attitudes questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. 2006;6:44. doi:10.1186/1472-6963-6-44
16. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
17. Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park: SAGE; 1985.
18. Colla JB, Bracken AC, Kinney LM, Weeks WB. Measuring patient safety climate: a review of surveys. Qual Saf Health Care. 2005;14(5):364–366. doi:10.1136/qshc.2005.014217
19. Lousada LM, da Silva Dutra FC, da Silva BV, et al. Patient safety culture in primary and home care services. BMC Fam Pract. 2020;21(1):188. doi:10.1186/s12875-020-01263-1
20. Ree E, Wiig S. Employees’ perceptions of patient safety culture in Norwegian nursing homes and home care services. BMC Health Serv Res. 2019;19(1):607. doi:10.1186/s12913-019-4456-8
21. Lang A, Edwards N, Fleiszer A. Safety in home care: a broadened perspective of patient safety. Int J Qual Health Care. 2008;20(2):130–135. doi:10.1093/intqhc/mzm068
22. Yoon SH, Wu X. Content analysis of patient safety culture in nursing homes. J Korean Acad Nurs Adm. 2013;19(1):118–127. doi:10.11111/jkana.2013.19.1.118
23. Ellenbecker CH, Samia L, Cushman MJ, Alster K. Chapter 13. Patient safety and quality in home health care. In: Hughes RG, editor. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville (MD); 2008. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2631/.
24. Seo JH, Song ES, Choi SE, Woo KS. Patient safety in Korea: current status and policy issues. Seoul, Korea: Korea Institute for Health and Social Affairs; 2016. Available from: http://repository.kihasa.re.kr/handle/201002/20928.
25. Lee S-I. Current status and future challenges of patient safety improvement in Korea. Yakhak Hoeji. 2020;64(3):179–184. doi:10.17480/psk.2020.64.3.179
26. Johannessen T, Ree E, Aase I, Bal R, Wiig S. Exploring challenges in quality and safety work in nursing homes and home care – a case study as basis for theory development. BMC Health Serv Res. 2020;20(1):277. doi:10.1186/s12913-020-05149-x
27. Park E. Current state and the future tasks of home visit nursing care in South Korea. J Agr Community Health. 2019;44(1):28–38.
28. Bien E, Davis K, Gillespie G. Home healthcare workers’ occupational exposures. Home Healthc Now. 2020;38(5):247–253. doi:10.1097/NHH.0000000000000891
29. Hittle B, Agbonifo N, Suarez R, Davis KG, Ballard T. Complexity of occupational exposures for home health-care workers: nurses vs. home health aides. J Nurs Manag. 2016;24(8):1071–1079. doi:10.1111/jonm.12408
30. Health Insurance Review & Assessment Service of Korea. Reimbursement criteria and procedures of medical claims. Seoul; 2021. Available from: https://www.hira.or.kr/ebooksc/ebook_662/ebook_662_202110260434596540.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025