Back to Journals » Drug Design, Development and Therapy » Volume 19
Advanced Natural Therapeutics and Delivery Strategies for Diabetic Foot Ulcers: A Mini Review
Received 2 August 2025
Accepted for publication 14 November 2025
Published 25 November 2025 Volume 2025:19 Pages 10449—10472
DOI https://doi.org/10.2147/DDDT.S557827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Qi Liu,1 Xinxin Yu2
1Department of Peripheral Vascular II, First Affiliated Hospital of Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, 150040, People’s Republic of China; 2Department of Peripheral Vascular, Heilongjiang Academy of Traditional Chinese Medicine, Harbin, Heilongjiang, 150036, People’s Republic of China
Correspondence: Xinxin Yu, Department of Peripheral Vascular, Heilongjiang Academy of Traditional Chinese Medicine, Harbin, Heilongjiang, 150036, People’s Republic of China, Email [email protected]
Abstract: Diabetic foot ulcers (DFUs) are a severe complication of diabetes mellitus with complex pathophysiology. Conventional therapies often lead to poor healing and high recurrence. This mini-review highlights the promise of advanced natural therapeutics and delivery strategies for DFU management. We focus on bioactive natural compounds, such as ginsenosides, astragalus polysaccharides, and resveratrol, that target critical processes like hyperglycemia, vascular impairment, and oxidative stress by modulating key signaling pathways. To improve bioavailability, innovative delivery systems including nanotechnology and nitric oxide-releasing platforms have been developed, enabling sustained release and enhanced healing. Clinical evidence shows promising results, such as shortened healing time and improved ulcer closure rates, supports the translational potential of standardized natural formulations. Moving forward, priorities should focus on standardizing natural formulations, optimizing delivery, and conducting rigorous clinical trials. With continued innovation, natural therapeutics hold significant potential to improve wound healing, reduce amputations, and enhance the quality of life for DFU patients.
Keywords: diabetic foot ulcers, natural therapeutics, bioactive compounds, wound healing, nanotechnology
Introduction
Diabetic foot ulcers (DFUs) represent a critical complication of diabetes mellitus and pose a significant global healthcare challenge. Globally, over 550 million people live with diabetes, including 37 million in the United States.1 Approximately 18.6 million new DFU cases occur annually, affecting about 34% of the diabetic population. DFUs are chronic, non-healing wounds that predominantly occur on the feet, driven by a multifactorial etiology including hyperglycemia-induced peripheral neuropathy, tissue ischemia and impaired angiogenesis due to peripheral arterial disease, and dysregulated chronic inflammation with compromised immune defense.2 The impact of DFUs is profound, resulting in substantial disability-adjusted life years (DALYs) lost and healthcare costs amounting to billions of dollars annually.3 DFU management accounts for a significant portion of diabetes-related expenditures, driven by high hospitalization rates and prolonged treatments. Moreover, DFUs are a leading cause of lower limb amputations, with approximately 20% of diabetic patients with foot ulcers requiring amputation, either partial or complete.4,5 In the United States alone, over 150,000 non-traumatic lower limb amputations are performed annually, contributing to a global total of 1.6 million amputations, of which 33% involve complete limb loss.6,7 These factors collectively underscore the urgent need for innovative therapeutic strategies to alleviate the socioeconomic impact of DFUs on both patients’ quality of life and healthcare systems.
Standard management of DFUs has traditionally relied on practices such as debridement, infection control, and offloading pressure from the affected area.8 However, these conventional therapies often prove insufficient, as many patients experience slow or incomplete wound healing, which significantly compromises their recovery.9 The high recurrence rate of DFUs, which can be as high as 60%, further highlights the limitations of current standard-of-care, which frequently fails to address the underlying pathological mechanisms such as persistent inflammation, microvascular dysfunction, and cellular senescence. This therapeutic failure poses ongoing risks to patients’ health and quality of life.10 This persistent clinical challenge underscores the urgent need for innovative therapeutic approaches that can effectively target the multifaceted pathophysiological mechanisms of DFUs, particularly those related to impaired tissue regeneration and chronic inflammation.11
Given these unmet needs, there is growing interest in exploring alternative and adjunctive therapies. Recent advancements in natural therapeutics have opened new avenues for DFUs management by combining bioactive compounds with cutting-edge delivery technologies.12,13 Phytochemicals, a diverse group of naturally occurring compounds found in plants such as fruits, vegetables, grains, and other plant foods, have emerged as promising therapeutic agents due to their multi-targeted actions.14 Preclinical, clinical, and epidemiological studies suggest that phytochemicals may be effective in treating various diseases owing to their anti-inflammatory, antioxidant, and pro-angiogenic activities.15 However, challenges such as poor bioavailability, chemical instability, and limited tissue penetration have historically constrained their clinical application. To overcome these barriers, nanotechnology-driven strategies have been employed to enhance their therapeutic potential. For instance, nano-encapsulation of active ingredients enables sustained release, targeted delivery to wound sites, and improved cellular uptake.16,17 These innovations not only optimize pharmacokinetics but also amplify key healing processes such as collagen synthesis, macrophage polarization, and angiogenesis.
Therefore, this mini-review aims to synthesize current mechanistic evidence and translational opportunities for advanced natural therapeutics in DFUs care. The potential of these agents is explored, focusing on their ability to target critical pathological processes, including hyperglycemia, peripheral neuropathy, vascular insufficiency, persistent inflammation, wound infection, and oxidative stress. Furthermore, supplementary strategies, such as nanocarriers and nitric oxide (NO)-releasing gels, are discussed for their role in enhancing therapeutic efficacy. While clinical trials demonstrate promising translational progress, challenges related to standardization and scalability remain. By integrating mechanistic insights with therapeutic advancements, this review highlights the transformative potential of natural compounds in redefining DFU management.
Pathophysiology of Diabetic Foot Ulcers
Hyperglycemia-Induced Neuropathy
Diabetic peripheral neuropathy (DPN) is a critical factor in the pathogenesis and progression of diabetic foot complications and is strongly associated with lower limb ulcers, amputations, and disability.18 One of its core clinical consequences is severe impairment of sensory nerve function, coupled with autonomic neuropathy leading to dysfunction in sweat gland secretion.19 Neuropathy-induced sensory deficits, particularly in pain perception, significantly elevate the risk of trauma in diabetic patients. Alarmingly, this sensory impairment often leads to delayed detection of skin injuries and ulcers, which may remain unnoticed by both patients and healthcare providers for weeks or even months, resulting in inadequate and untimely intervention.20
Persistent hyperglycemia, typically defined as blood glucose levels exceeding 180 mg/dL, drives nerve damage through a complex interplay of mechanisms. Firstly, it induces metabolic dysregulation, characterized by the accumulation of fructose and sorbitol and a decline in myo-inositol levels.21 This metabolic imbalance triggers osmotic disturbances, including sodium and water retention, as well as reduced Na+, K+-ATPase activity, which directly injures neurons. Secondly, glucose overload exacerbates mitochondrial dysfunction, leading to the generation of excessive reactive oxygen species (ROS) that damage Schwann cell DNA and impair the axonal transport of neurotrophic factors.22 In an oversaturated system, acetyl-CoA converts to acylcarnitine, inducing stress in Schwann cells and dorsal root ganglion (DRG) neurons while further exacerbating mitochondrial dysfunction, ultimately resulting in axonal degeneration.23 Thirdly, hyperglycemia degrades type IV collagen within the basement membrane of nerve-nourishing blood vessels and disrupts the distribution of aquaporins on astrocyte end-feet, compromising the glio-vascular interface and exacerbating nerve ischemia.24 Collectively, these processes impair axonal conduction, signal transmission, and neurotrophic support, culminating in centripetal degeneration and distal axonal length-dependent loss.
Ischemic-Vascular Pathology
Diabetes induces widespread ischemic vascular pathology by damaging both macro- and microvascular systems, posing a severe threat to peripheral nerves and wound healing. Chronic hyperglycemia is the central driver of these vascular complications.25 At the macrovascular level, it accelerates atherosclerosis through mechanisms involving hyperglycemia, insulin resistance, excess free fatty acids, and advanced glycation end products (AGEs).26 These factors collectively suppress endothelial nitric oxide synthase (eNOS) activity, increase ROS production, and activate pro-inflammatory transcription factors such as NF-κB and aquaporin 1.27 This inflammatory cascade promotes leukocyte adhesion, migration, and lipid uptake by macrophages, leading to foam cell formation and atherosclerotic plaque development. Atherosclerosis, affecting large arteries, is a primary cause of cardiovascular disease, stroke, and peripheral arterial disease (PAD). PAD, in turn, impairs distal limb perfusion, contributing to approximately 50% of DFUs, while delaying wound healing and increasing infection risks.28
At the microvascular level, diabetes triggers characteristic microangiopathy, involving small arteries and capillaries, which underpins nephropathy, retinopathy, and DPN. Endothelial injury initiates microvascular dysfunction, causing hemodynamic abnormalities, impaired oxygen delivery, and fluid filtration imbalance.29 Damage to the vasa nervorum, the microvessels supplying nerves, is particularly critical, reducing blood flow to neural tissues.30 This manifests as impaired intraneural hemodynamics, loss of autoregulation, and structural abnormalities such as basement membrane thickening, endothelial cell swelling, and reduced tight junction proteins. These changes lead to vessel narrowing, increased resistance, and chronic ischemia, contributing to DPN pathogenesis.31
Thus, diabetic vascular pathology creates a vicious cycle of macrovascular occlusion and microvascular dysfunction, exacerbated by vasoconstriction and hypercoagulability. This not only elevates ulcer risk but also impedes wound healing by depriving tissues of oxygen and nutrients, ultimately leading to non-healing ulcers and catastrophic outcomes like amputations.32
Inflammation-Infection Vicious Cycle
In diabetic patients, skin barrier disruption facilitates bacterial invasion, initiating a complex interplay between infection and a maladaptive host inflammatory response that is central to the pathophysiology of DFUs.33 Unhealed ulcers provide an ideal environment for polymicrobial infections. Gram-positive bacteria (eg, Staphylococcus aureus, Streptococcus species) often dominate superficial wounds, while Gram-negative bacteria colonize deeper abscesses. Mixed infections, involving bacteria (eg, coagulase-negative staphylococci, enterococci, anaerobes) and fungi (eg, Candida albicans, Candida parapsilosis), complicate treatment, impair healing, and increase the risk of chronic wounds and scarring.34
Chronic inflammation is a central barrier to DFU healing.35 Even before skin breakdown, endogenous damage in diabetic feet is linked to abnormal inflammatory cytokine levels. Persistent inflammation disrupts the epidermal microenvironment, impairs cellular repair, exacerbates hyperglycemia, and increases insulin resistance.36 Hyperglycemia itself compromises immune function, reducing monocyte counts, disrupting T-cell subsets, and impairing phagocytic activity in neutrophils and macrophages, while promoting excessive inflammatory cytokine release.37 During wound healing, macrophage polarization from pro-inflammatory M1 to anti-inflammatory M2 phenotypes is critical for resolving inflammation.38 However, in DFUs, macrophage dysfunction and impaired polarization perpetuate a pro-inflammatory state, delaying repair.
Immune cell dysfunction exacerbates the inflammation-infection cycle. Diabetic wounds exhibit impaired neutrophil chemotaxis, phagocytosis, degranulation, and ROS production, further compromised by hyperglycemia-induced upregulation of protein arginine deiminase 4 and inhibition of neutrophil extracellular trap formation. This weakens antimicrobial defense and promotes tissue damage through excessive cytokine and protease release.39,40 This dysfunction is compounded by a protease imbalance caused by activated macrophages and neutrophils, which secrete proteases such as MMPs that degrade extracellular matrix proteins, including collagen, elastin, and fibronectin. The resulting fragments recruit inflammatory cells, sustain inflammation, and activate additional MMPs, creating a destructive feedback loop.41 Additionally, diabetic wounds suffer from immune dysregulation, characterized by disrupted collaboration between immune cells, such as macrophages, neutrophils, and lymphocytes, and repair cells, including keratinocytes, fibroblasts, and endothelial cells, which collectively undermines the healing process.42,43
Thus, DFUs are trapped in a self-perpetuating inflammation-infection cycle: hyperglycemia and initial injury trigger chronic inflammation and immune suppression, increasing infection susceptibility. Persistent infections, in turn, activate dysfunctional immune cells that release destructive mediators, further impeding healing and maintaining a non-healing wound environment. Breaking this cycle is therefore a primary therapeutic objective in DFU management. Figure 1.
 |
Figure 1 Pathophysiology of Diabetic Foot Ulcers. |
Current Treatment Strategies for Diabetic Foot Ulcers
The treatment strategies for DFUs require a comprehensive approach that directly addresses the complex pathophysiology, outlined in Pathophysiology of Diabetic Foot Ulcers, including hyperglycemia-induced neuropathy, ischemic-vascular pathology, and the inflammation-infection vicious cycle.
Management of Hyperglycemia-Induced Neuropathy
Strict glycemic control is the cornerstone of DPN management, with pancreatic transplantation showing significant efficacy in normalizing blood glucose and improving motor and sensory neuropathy.44 For pharmacological treatment, pregabalin, tapentadol, and duloxetine are FDA-approved for alleviating DPN-related pain.45 Additionally, antioxidants such as alpha-lipoic acid (ALA) have shown potential in delaying or reversing peripheral nerve damage.46 Stem cell therapy and low-dose IL-6 biotherapy are also under exploration, offering new directions for DPN treatment by promoting angiogenesis and neuroprotection.47,48
Intervention for Ischemic-Vascular Pathology
Ischemic vascular pathology is a major barrier to DFU healing. Revascularization techniques, such as bypass surgery and endovascular angioplasty, are primary methods for restoring blood flow.49,50 While atherectomy can remove atherosclerotic plaques, its efficacy has not been proven superior to angioplasty.51 Postoperative multidisciplinary care, including the management of hypertension and hypercholesterolemia, is crucial for successful outcomes. Hyperbaric oxygen therapy (HBOT) enhances tissue oxygenation by increasing plasma oxygen levels, significantly boosting physically dissolved oxygen.52 According to Fick’s law, elevated oxygen partial pressure enhances the driving force and diffusion distance of oxygen, accelerating ulcer healing. Furthermore, HBOT activates the hypoxia-inducible factor (HIF-1α) signaling pathway, promoting the expression of vascular endothelial growth factor (VEGF) and improving local blood supply, thereby providing the oxygen and nutrients necessary for tissue repair.53,54
Control of the Inflammation-Infection Vicious Cycle
Given the critical role of the inflammation-infection cycle described in the previous section, its control is paramount in DFU management. Infection control is a critical component. The choice of empirical antibiotic therapy should be selected based on the likely pathogens and the severity of the infection.55 Mild infections may be treated with dicloxacillin or cephalexin, moderate infections with vancomycin combined with ampicillin/sulbactam, and severe infections with broad-spectrum antibiotics such as piperacillin/tazobactam or carbapenems. HBOT enhances the antibacterial effects of antibiotics by promoting bacterial aerobic metabolism and increasing drug uptake.56 Additionally, HBOT induces the production of oxygen free radicals, directly damaging bacterial membrane proteins and DNA structures, inhibiting the generation of inflammatory factors, and promoting the resolution of inflammation at the infection site.57
Debridement is a crucial component of infection management, as it removes bacterial biofilms and necrotic tissue from the wound, creating favorable conditions for healing.58 Wound debridement and cleansing are typically performed using isotonic saline solution and are essential adjuncts to antibiotic therapy. Wound dressings, such as hydrogels,59 alginate dressings,60 hydrocolloids,61 foam adhesives,62 and hydrofibers,63 protect the wound from infection and environmental exposure while maintaining optimal moisture levels to promote new tissue formation and autolytic debridement.
Advanced Natural Therapeutics for Diabetic Foot Ulcers
Key Bioactive Compounds and Mechanisms
Advanced natural therapeutics address the core pathophysiological mechanisms of DFUs through multifaceted approaches. Of particular relevance is their potential to disrupt the persistent inflammation-infection cycle that profoundly impedes healing.
Immunomodulatory and Anti-Inflammatory Mechanisms
Inflammation and infection control are addressed through the modulation of innate immune responses, directly targeting pathways involved in the vicious cycle. Bletilla striata polysaccharide (BSP) inhibits NLRP3 inflammasome activation, targeting a key driver of chronic inflammation in DFUs.64 Puerarin suppresses NF-κB and MAPK signaling pathways and promotes macrophage polarization towards the reparative M2 phenotype.65 Astragalus polysaccharide shifts macrophage polarization via β-catenin/NF-κB and Nrf2/HO-1 pathways, significantly reducing pro-inflammatory cytokines such as TNF-α, IL-6, and IL-12.66,67 Resveratrol exhibits broad anti-inflammatory effects, inhibits the AGE-RAGE pathway and promotes healing via PI3K/Akt signaling.68,69
In summary, the immunomodulatory actions of these natural compounds are pivotal for breaking the inflammation-infection cycle in DFUs. By targeting key inflammatory signaling hubs and promoting a pro-resolving macrophage phenotype, they help resolve chronic inflammation, reduce tissue damage, and create a microenvironment conducive to healing. This represents a fundamental shift from merely suppressing infection to actively reprogramming the dysfunctional immune response.
Glucose-Lowering and Neuropathy-Targeting Mechanisms
Beyond inflammation control, these therapeutics also target other key pathological axes, primarily hyperglycemia reduction and neuropathy improvement. Gomisin A enhances insulin sensitivity and accelerates wound healing by suppressing the neuroinflammatory TLR4/p38 MAPK/IL6 pathway.70 Similarly, the ethanolic extract of Euphorbia hirta demonstrates dual efficacy by reducing hyperglycemia and oxidative stress markers such as malondialdehyde and NO while promoting wound closure.71
Collectively, targeting hyperglycemia and associated neuropathic pathways addresses the root cause of DFU development. By improving glycemic control and directly protecting nerves from glucotoxic insults, these compounds can prevent initial ulceration and improve sensory function, thereby reducing the risk of unnoticed trauma, a critical factor in DFU pathogenesis.
Pro-Angiogenic Mechanisms
For alleviation of vascular lesions and impaired angiogenesis, several compounds exhibit potent activity. Ginsenoside Rg1, which promotes endothelial cell function and neovascularization, acts through PI3K/Akt/eNOS signaling and modulates microRNAs including miR-489-3p/Sirt1 and miR-23a/IRF-1.72–74 Ramulus Mori alkaloids (SZ-A) protect endothelial cells from oxidative damage and stimulate angiogenesis via the NRF2/HO-1/eNOS axis.75 β-sitosterol activates MAPK/mTOR/VEGF pathways, enhancing microvascular perfusion,76 while Astragalus aqueous extract upregulates HIF-1α and VEGF expression, directly counteracting tissue ischemia.77
The core significance of these pro-angiogenic agents lies in their ability to reverse tissue ischemia, a major barrier to healing in DFUs. By activating critical pathways that drive the formation of new blood vessels and enhancing endothelial cell survival, they improve the delivery of oxygen and nutrients to the wound bed, which is essential for supporting the cellular activities required for tissue repair.
Antioxidant Mechanisms
Moreover, oxidative stress mitigation represents another critical therapeutic axis. Resveratrol alleviates hyperglycemia-induced ferroptosis in endothelial cells by regulating Nrf2 activity and key markers such as GPX4, SLC7A11, and ACSL4.78 Dracorhodin activates the Nrf2 pathway while inhibiting ferroptosis, reducing ROS and promoting repair.79 Narirutin reprograms cellular metabolism via the AMPK/Mfn2 pathway, reducing oxidative damage and inflammation.80
The antioxidant mechanisms, particularly those involving the Nrf2 pathway, are crucial for mitigating oxidative damage that perpetuates cellular dysfunction and death in the diabetic wound environment.
Nanotechnology and Hydrogel-Based Delivery Systems
To overcome bioavailability limitations, nanotechnology-driven delivery systems have been developed to enhance therapeutic potential. Gallium-modified gelatin nanoparticles loaded with quercetin, which promote sustained release and TGF-β/Smad-mediated M2 macrophage polarization, accelerate repair while inhibiting scar formation.81 Curcumin nanoparticle hydrogel (Cur-NP/HG), which outperforms conventional formulations, enhances re-epithelialization and collagen deposition while reducing inflammation.82 Chitosan nanogel encapsulating Teucrium polium nanoparticles (TP-NP/CS-NG), which improves stability and bioavailability, effectively alleviates oxidative stress and promotes angiogenesis.83
A cutting-edge metal-polyphenol nanocomposite hybrid hydrogel has been developed for DFU microenvironment reprogramming.84 Composed of EGCG/Fe3+ nanoparticles loaded with salvianolic acid B and glucose oxidase within a polysaccharide hydrogel, it exhibits potent antibacterial activity, promotes M2 macrophage polarization, angiogenesis, and ROS scavenging, significantly accelerating wound healing. NO-releasing gels represent a sophisticated strategy that combines natural compounds with gaseous signaling molecules. Asiaticoside-NO gel, which enhances healing via Wnt/β-catenin signaling, increases VEGF, iNOS, eNOS, and CD34 expression while exerting antimicrobial effects.85 Asiaticoside-NO hydrogel (ACNO), which modulates critical metabolic pathways such as methyl histidine metabolism and the malate-aspartate shuttle, attenuates SRC/STAT3 activation to promote repair.86 Centella asiatica total glycosides-NO gel (CATGNOG), which provides a stable and non-toxic delivery platform, demonstrates significant clinical potential.87
Multicomponent Hydrogels synergize bioactive properties. The BSP/Berberine hydrogel, which achieves 94.9% ± 1.81% wound closure in diabetic mice by day 14, combines antibacterial, anti-inflammatory, and antioxidant actions.88
Preclinical and Clinical Evidence
Robust clinical evidence supports ON101, a standardized blend of Plectranthus amboinicus PA-F4 and Centella asiatica S1. A multicenter, randomized controlled trial demonstrated a significantly higher complete healing rate with ON101 cream (60.7%) versus absorbent dressing (35.1%) over 16 weeks, with an odds ratio of 2.84 and a 95% confidence interval of 1.66–4.84.89 Post-hoc analysis confirmed efficacy in high-risk patients, including those with Wagner grade 2 ulcers, size ≥5 cm2, duration ≥3 months, HbA1c ≥9%, and BMI ≥25.90 Teucrium polium ointment, which significantly enhances healing of non-infected DFUs, has also been validated in a randomized clinical trial.91 Table 1.
 |
Table 1 Advanced Natural Therapeutics for Diabetic Foot Ulcers |
Challenges and Future Perspectives
Comparative Analysis and Therapeutic Modalities
A critical evaluation of the different natural product classes and delivery systems reveals distinct advantage and niches for each, which is crucial for guiding future research and clinical application. Flavonoids and polyphenols, including quercetin, puerarin, resveratrol, and curcumin, are particularly notable for their potent antioxidant and anti-inflammatory activities, primarily mediated through the Nrf2 and NF-κB pathways. In contrast, polysaccharides such as Astragalus polysaccharide and BSP exhibit superior immunomodulatory effects, excellent water solubility, and biocompatibility, making them ideal for hydrogel-based dressings. Saponins, exemplified by Ginsenoside Rg1, demonstrate remarkable pro-angiogenic efficacy via pathways like PI3K/Akt/eNOS.
Regarding delivery platforms, nanocarriers, such as nanoparticles and nanogels, excel in protecting labile compounds, enabling targeted and sustained release to specific wound cells, and enhancing penetration into wound beds. Hydrogel systems provide a moist wound-healing environment, are ideally suited for topical application, and can be designed to respond to wound microenvironment cues. The emerging trend of embedding nanocarriers within hydrogels represents a promising synergy, combining the protective and targeted delivery advantages of nanotechnology with the practical application and sustained reservoir benefits of hydrogels. Table 2.
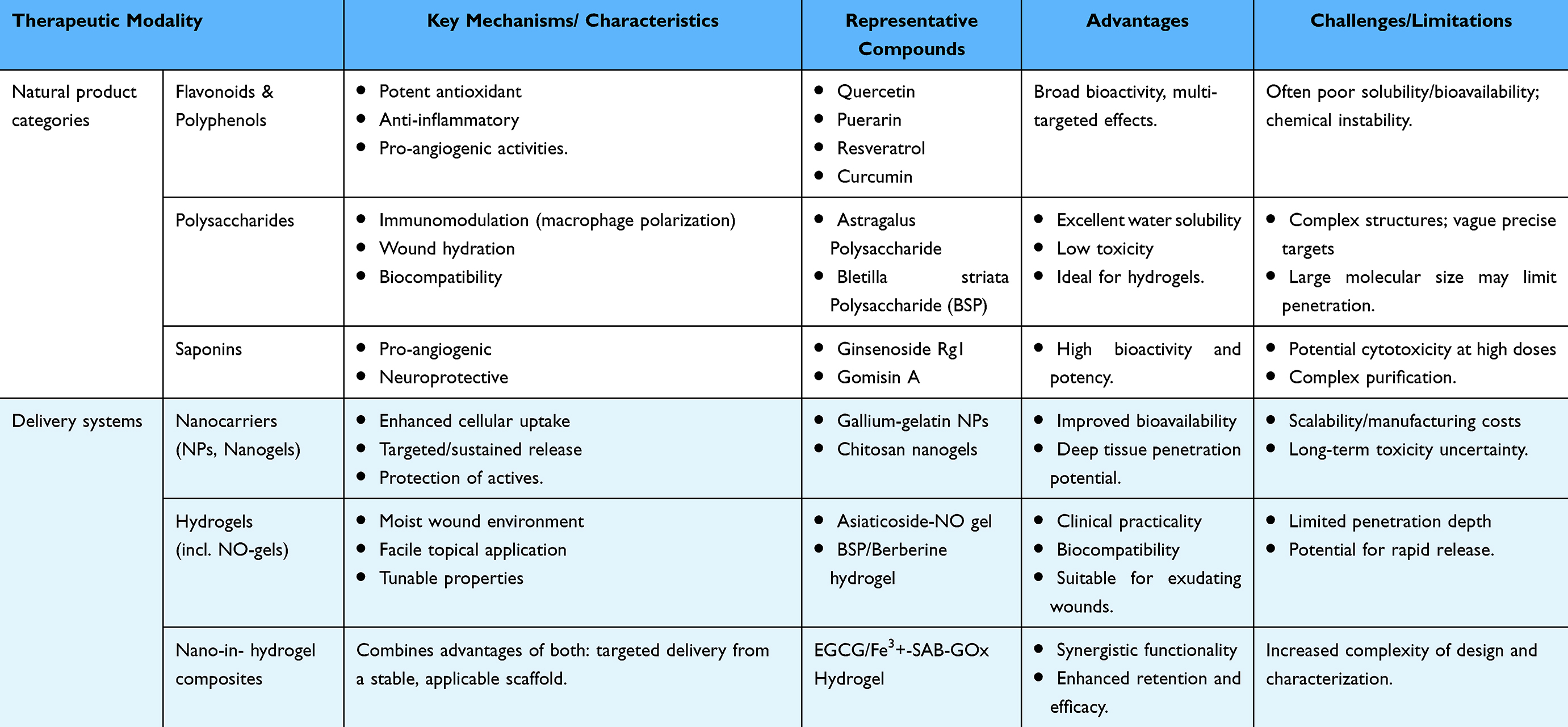 |
Table 2 Comparison of Major Natural Product Categories and Delivery Systems for Diabetic Foot Ulcer Management |
Translational Challenges and Standardization Hurdles
Despite promising preclinical and early clinical results, significant translational challenges hinder the widespread adoption of natural therapeutics for DFUs. Standardization and quality control remain critical obstacles due to variability in plant sourcing, extraction methodologies, and active compound content.157,158 Rigorous phytochemical standardization using advanced analytical techniques such as HPLC and LC-MS, along with the establishment of pharmacopeial standards, is essential to ensure batch-to-batch consistency and meet regulatory requirements.
Challenges in bioavailability and delivery optimization persist. While advanced systems such as nanoparticles and NO-gels show promise, achieving effective drug concentrations in deep, ischemic ulcer beds requires further engineering. It is also important to note that the current body of literature, including this review, leans towards reporting positive preclinical outcomes. A more balanced perspective for the field requires increased publication and discussion of negative, inconclusive, or contradictory findings to fully assess therapeutic potential and avoid publication bias. Key priorities include improving the physicochemical properties and reproducibility of nanomaterials for clinical applications, as well as addressing uncertainties regarding their biodistribution, degradation, and long-term biological effects.16 Additionally, more in vivo studies in large animal models are needed, as current research predominantly relies on rodent models that imperfectly replicate human DFU pathophysiology. Developing simpler, more controllable, and reproducible delivery systems is essential to facilitate translation. Furthermore, more specific and convenient administration methods should be explored to enhance efficacy and clinical practicality.
Clinical trial design complexity arises from DFU heterogeneity.159 Future trials must implement rigorous stratification based on ulcer characteristics and patient factors to identify responsive subgroups, as demonstrated by ON101’s efficacy in high-risk patients. Safety and long-term outcomes require meticulous assessment, including comprehensive toxicology profiles, potential drug-herb interactions, and monitoring for long-term complications.
Future Research Priorities
Future research priorities should focus on several critical areas to advance the field of natural therapeutics for DFUs. First, the development of advanced delivery systems is essential, particularly next-generation platforms that incorporate antimicrobials or debriding enzymes alongside natural active compounds to achieve synergistic therapeutic effects. Second, combination therapy optimization should be systematically evaluated, integrating natural therapeutics with standard care and advanced modalities to maximize treatment outcomes. Third, biomarker-driven personalization is crucial, as identifying predictive biomarkers will enable the matching of patients with the most effective natural therapeutics based on their unique profiles. Fourth, research should prioritize treatment-refractory ulcers, focusing on efficacy studies in patients with hard-to-heal DFUs who do not respond to conventional therapies. Fifth, the integration of “omics” technologies, such as transcriptomics, proteomics, and metabolomics, will help elucidate comprehensive mechanisms of action and uncover synergistic phytochemical combinations. Finally, generating real-world evidence through the establishment of registries is vital to monitor the long-term effectiveness, safety, and cost-effectiveness of these therapies in diverse clinical settings. Addressing these priorities will significantly enhance the translation of natural therapeutics into clinical practice and improve outcomes for patients with DFUs. Table 3.
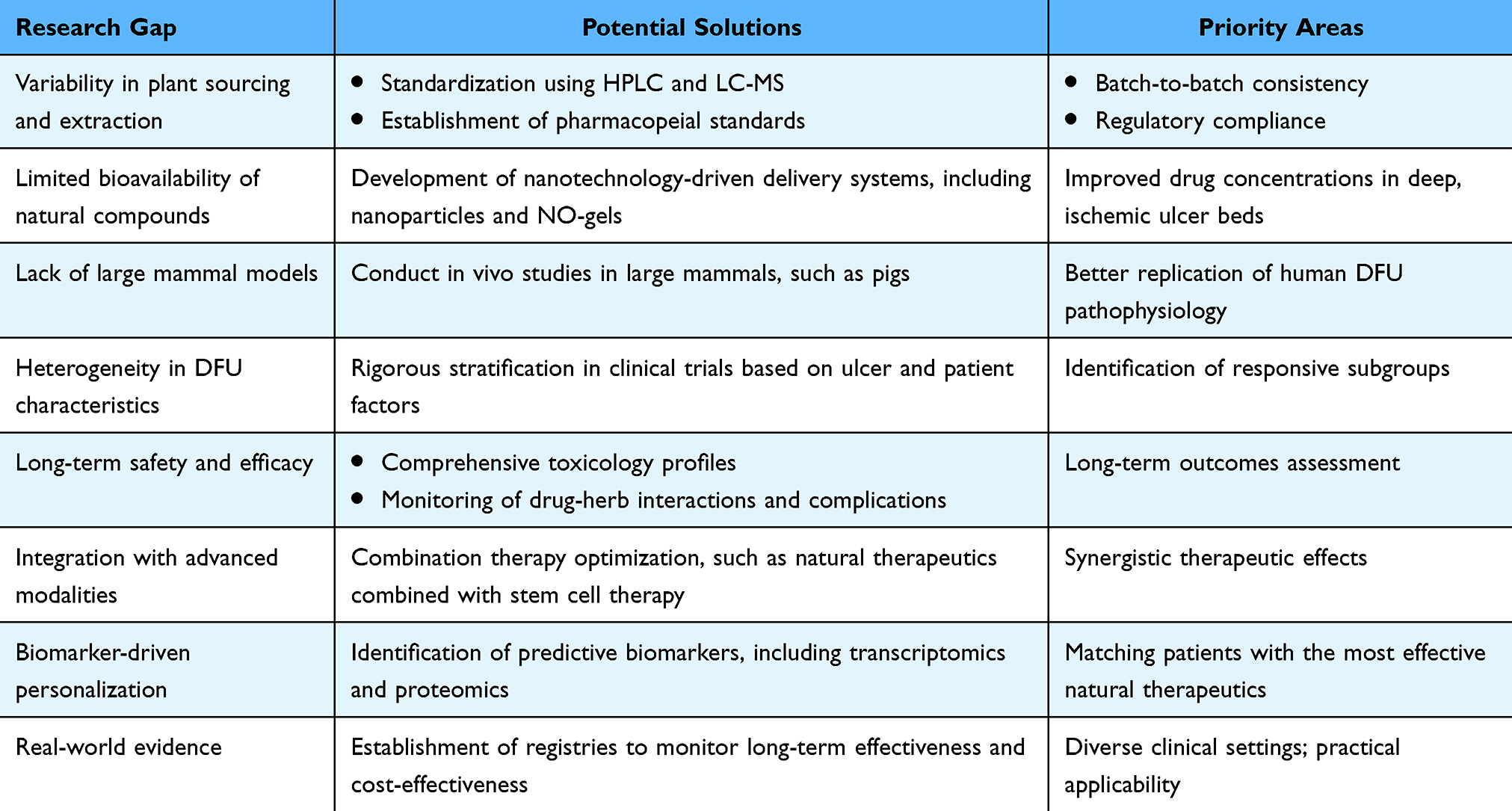 |
Table 3 Research Gaps, Potential Solutions, and Priority Areas for Future Investigation |
Conclusion
In contrast to conventional approaches that primarily address symptoms or advanced standard-of-care therapies targeting single pathways, advanced natural therapeutics present a promising multi-targeted strategy for the complex pathophysiology of DFUs. This review synthesizes evidence on bioactive compounds that modulate key healing processes, with advanced delivery systems overcoming bioavailability limitations. Preclinical and early clinical trials with standardized formulations show considerable promise. However, the current clinical evidence remains limited, primarily consisting of a few promising but small-scale studies. This underscores the critical need for larger, well-designed randomized controlled trials to robustly establish efficacy, optimal dosing, and long-term safety.
Translating this potential into practice, however, faces challenges in phytochemical standardization, delivery optimization, and the design of robust clinical trials for heterogeneity of DFU populations. Bridging there evidence gaps is essential to seize the translational opportunities, which include developing synergistic combinations and biomarker-driven personalization.
Looking ahead, the successful integration of these therapies has the potential to significantly influence future clinical guidelines, promoting personalized wound care strategies. Broader adoption could yield substantial public health benefits, including reduced healthcare costs, improved patient outcomes, and a lower burden of diabetes-related complications. Realizing this impact necessitates continued research and collaborative innovation.
Acknowledgments
Figure was created in https://BioRender.com.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
There is no conflict of interests.
References
1. Armstrong DG, Tan T-W, Boulton AJM, Bus SA. Diabetic foot ulcers: a review. JAMA. 2023;330(1):62–75. doi:10.1001/jama.2023.10578
2. Lim JZ, Ng NS, Thomas C. Prevention and treatment of diabetic foot ulcers. J R Soc Med. 2017;110(3):104–109. doi:10.1177/0141076816688346
3. Collaborators GD. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2023;402(10397):203–234. doi:10.1016/s0140-6736(23)01301-6
4. Bus SA, Sacco ICN, Monteiro-Soares M, et al. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes Metab Res Rev. 2024;40(3):e3651. doi:10.1002/dmrr.3651
5. Jeon BJ, Choi HJ, Kang JS, Tak MS, Park ES. Comparison of five systems of classification of diabetic foot ulcers and predictive factors for amputation. Int Wound J. 2017;14(3):537–545. doi:10.1111/iwj.12642
6. Taylor CG Jr, Krimholtz M, Belgrave KC, Hambleton I, George CN, Rayman G. The extensive inpatient burden of diabetes and diabetes-related foot disease in Barbados. Clin Med. 2014;14(4):367–370. doi:10.7861/clinmedicine.14-4-367
7. Xu J, Haider A, Sheikh A, González-Fernández M. Epidemiology and impact of limb loss in the united states and globally. Phys Med Rehab Clin. 2024;35(4):679–690. doi:10.1016/j.pmr.2024.05.003
8. Frykberg RG. Topical wound oxygen therapy in the treatment of chronic diabetic foot ulcers. Medicina. 2021;57(9):917. doi:10.3390/medicina57090917
9. Tentolouris A, Eleftheriadou I, Samakidou G, Tentolouris N. Developments in the management of diabetic foot ulcers (Review). World Acad Sci J. 2025;7(3):46. doi:10.3892/wasj.2025.334
10. Guo Q, Ying G, Jing O, et al. Influencing factors for the recurrence of diabetic foot ulcers: a meta-analysis. Int Wound J. 2023;20(5):1762–1775. doi:10.1111/iwj.14017
11. Bardill JR, Laughter MR, Stager M, Liechty KW, Krebs MD, Zgheib C. Topical gel-based biomaterials for the treatment of diabetic foot ulcers. Acta Biomater. 2022;138:73–91. doi:10.1016/j.actbio.2021.10.045
12. Song J, Liu A, Liu B, et al. Natural biologics accelerate healing of diabetic foot ulcers by regulating oxidative stress. Front Biosci. 2022;27(10):285. doi:10.31083/j.fbl2710285
13. Rao SS, Venkatesan J, Prabhu A, Rekha PD. Natural polymeric biomaterials in growth factor delivery for treating diabetic foot ulcers. J Drug Delivery Sci Technol. 2020;55:101385. doi:10.1016/j.jddst.2019.101385
14. Kumar A, N P, Kumar M, et al. Major phytochemicals: recent advances in health benefits and extraction method. Molecules. 2023;28(2). doi:10.3390/molecules28020887
15. Hossain MS, Wazed MA, Asha S, Amin MR, Shimul IM. Dietary phytochemicals in health and disease: mechanisms, clinical evidence, and applications-A comprehensive review. Food Sci Nutr. 2025;13(3):e70101. doi:10.1002/fsn3.70101
16. Huang F, Lu X, Yang Y, et al. Microenvironment-based diabetic foot ulcer nanomedicine. Adv Sci. 2023;10(2):e2203308. doi:10.1002/advs.202203308
17. Jia S, Wu S, Yi M, et al. New strategies for the treatment of diabetic foot ulcers using nanoenzymes: frontline advances in anti-infection, immune regulation, and microenvironment improvement. Int J Nanomed. 2025;20:8783–8810. doi:10.2147/ijn.S531396
18. Wang X, Yuan CX, Xu B, Yu Z. Diabetic foot ulcers: classification, risk factors and management. World J Diabetes. 2022;13(12):1049–1065. doi:10.4239/wjd.v13.i12.1049
19. Pop-Busui R. Autonomic diabetic neuropathies: a brief overview. Diab Res Clin Pract. 2023;206. doi:10.1016/j.diabres.2023.110762.
20. Davis FM, Kimball A, Boniakowski A, Gallagher K. Dysfunctional wound healing in diabetic foot ulcers: new crossroads. Curr Diab Rep. 2018;18(1):2. doi:10.1007/s11892-018-0970-z
21. Zglejc-Waszak K, Mukherjee K, Korytko A, et al. Novel insights into the nervous system affected by prolonged hyperglycemia. J Mol Med. 2023;101(8):1015–1028. doi:10.1007/s00109-023-02347-y
22. Liu YP, Shao SJ, Guo HD. Schwann cells apoptosis is induced by high glucose in diabetic peripheral neuropathy. Life Sci. 2020;248:117459. doi:10.1016/j.lfs.2020.117459
23. Viader A, Sasaki Y, Kim S, et al. Aberrant Schwann cell lipid metabolism linked to mitochondrial deficits leads to axon degeneration and neuropathy. Neuron. 2013;77(5):886–898. doi:10.1016/j.neuron.2013.01.012
24. Stultz CM, Edelman ER. A structural model that explains the effects of hyperglycemia on collagenolysis. Biophys J. 2003;85(4):2198–2204. doi:10.1016/s0006-3495(03)74645-1
25. Yang DR, Wang MY, Zhang CL, Wang Y. Endothelial dysfunction in vascular complications of diabetes: a comprehensive review of mechanisms and implications. Front Endocrinol. 2024;15:1359255. doi:10.3389/fendo.2024.1359255
26. Li Y, Liu Y, Liu S, et al. Diabetic vascular diseases: molecular mechanisms and therapeutic strategies. Signal Transduction Targeted Ther. 2023;8(1):152. doi:10.1038/s41392-023-01400-z
27. Chawla A, Chawla R, Jaggi S. Microvasular and macrovascular complications in diabetes mellitus: distinct or continuum? Indian J Endocrinol Metab. 2016;20(4):546–551. doi:10.4103/2230-8210.183480
28. Forsythe RO, Brownrigg J, Hinchliffe RJ. Peripheral arterial disease and revascularization of the diabetic foot. Diabetes Obes Metab. 2015;17(5):435–444. doi:10.1111/dom.12422
29. Li Q, Wen Y, Wang L, et al. Hyperglycemia-induced accumulation of advanced glycosylation end products in fibroblast-like synoviocytes promotes knee osteoarthritis. Exp Mol Med. 2021;53(11):1735–1747. doi:10.1038/s12276-021-00697-6
30. Gao Y, Weng C, Wang X. Changes in nerve microcirculation following peripheral nerve compression. Neural Regen Res. 2013;8(11):1041–1047. doi:10.3969/j.issn.1673-5374.2013.11.010
31. Zhu J, Hu Z, Luo Y, et al. Diabetic peripheral neuropathy: pathogenetic mechanisms and treatment. Front Endocrinol. 2023;14:1265372. doi:10.3389/fendo.2023.1265372
32. Li WW, Carter MJ, Mashiach E, Guthrie SD. Vascular assessment of wound healing: a clinical review. Int Wound J. 2017;14(3):460–469. doi:10.1111/iwj.12622
33. Lou J, Xiang Z, Zhu X, et al. Skin microbiota and diabetic foot ulcers. Front Microbiol. 2025;16:1575081. doi:10.3389/fmicb.2025.1575081
34. Bruni E, Scaglione GL, Tampone D, et al. The healing process of diabetic ulcers correlates with changes in the cutaneous microbiota. Sci Rep. 2024;14(1):27628. doi:10.1038/s41598-024-77987-2
35. Yang S, Hu L, Han R, Yang Y. Neuropeptides, inflammation, biofilms, and diabetic foot ulcers. Exp Clin Endocrinol Diabetes. 2022;130(7):439–446. doi:10.1055/a-1493-0458
36. Chai W, Wang Y, Zheng H, et al. The profile of microbiological pathogens in diabetic foot ulcers. Front Med. 2021;8:656467. doi:10.3389/fmed.2021.656467
37. Lee H, Kim MJ, Lee IK, Hong CW, Jeon JH. Impact of hyperglycemia on immune cell function: a comprehensive review. Diabetol Int. 2024;15(4):745–760. doi:10.1007/s13340-024-00741-6
38. Zhu M, Ou J, Chen Y, et al. Programming of macrophage polarization in different stages for accelerating wound healing. Chem Eng J. 2024;491:152131. doi:10.1016/j.cej.2024.152131
39. Raghavan JV, Jhunjhunwala S. Role of innate immune cells in chronic diabetic wounds. J Indian Inst Sci. 2023;103(1):249–271. doi:10.1007/s41745-022-00355-4
40. Wong SL, Demers M, Martinod K, et al. Diabetes primes neutrophils to undergo NETosis, which impairs wound healing. Nature Med. 2015;21(7):815–819. doi:10.1038/nm.3887
41. Dawi J, Tumanyan K, Tomas K, et al. Diabetic foot ulcers: pathophysiology, immune dysregulation, and emerging therapeutic strategies. Biomedicines. 2025;13(5). doi:10.3390/biomedicines13051076
42. Lin S, Wang Q, Huang X, et al. Wounds under diabetic milieu: the role of immune cellar components and signaling pathways. Biomed Pharmacother. 2023;157:114052. doi:10.1016/j.biopha.2022.114052
43. Song J, Hu L, Liu B, et al. The emerging role of immune cells and targeted therapeutic strategies in diabetic wounds healing. J Inflamm Res. 2022;15:4119–4138. doi:10.2147/jir.S371939
44. Fridell JA, Stratta RJ, Gruessner AC. Pancreas transplantation: current challenges, considerations, and controversies. J Clin Endocrinol Metab. 2023;108(3):614–623. doi:10.1210/clinem/dgac644
45. Azmi S, ElHadd KT, Nelson A, et al. Pregabalin in the management of painful diabetic neuropathy: a narrative review. Diabetes Ther. 2019;10(1):35–56. doi:10.1007/s13300-018-0550-x
46. Perez-Favila A, Martinez-Fierro ML, Rodriguez-Lazalde JG, et al. Current therapeutic strategies in diabetic foot ulcers. Medicina. 2019;55(11). doi:10.3390/medicina55110714
47. Lopes L, Setia O, Aurshina A, et al. Stem cell therapy for diabetic foot ulcers: a review of preclinical and clinical research. Stem Cell Res Ther. 2018;9(1):188. doi:10.1186/s13287-018-0938-6
48. Kartika RW, Alwi I, Suyatna FD, et al. The role of VEGF, PDGF and IL-6 on diabetic foot ulcer after platelet rich Fibrin + hyaluronic therapy. Heliyon. 2021;7(9):e07934. doi:10.1016/j.heliyon.2021.e07934
49. Scatena A, Apicella M, Mantuano M, et al. Bypass surgery versus endovascular revascularization for occlusive infrainguinal peripheral artery disease: a meta-analysis of randomized controlled trials for the development of the Italian Guidelines for the treatment of diabetic foot syndrome. Acta Diabetol. 2024;61(1):19–28. doi:10.1007/s00592-023-02185-x
50. Wong YT. Endovascular treatment of diabetic foot ischemic ulcer - Technical review. J Interv Med. 2020;3(1):17–26. doi:10.1016/j.jimed.2020.01.002
51. Uccioli L, Meloni M, Izzo V, Giurato L, Merolla S, Gandini R. Critical limb ischemia: current challenges and future prospects. Vasc Health Risk Manag. 2018;14:63–74. doi:10.2147/vhrm.S125065
52. Zhang Z, Zhang W, Xu Y, Liu D. Efficacy of hyperbaric oxygen therapy for diabetic foot ulcers: an updated systematic review and meta-analysis. Asian J Surg. 2022;45(1):68–78. doi:10.1016/j.asjsur.2021.07.047
53. Sunkari VG, Lind F, Botusan IR, et al. Hyperbaric oxygen therapy activates hypoxia-inducible factor 1 (HIF-1), which contributes to improved wound healing in diabetic mice. Wound Repair Regen. 2015;23(1):98–103. doi:10.1111/wrr.12253
54. Semadi NI. The role of VEGF and TNF-alpha on epithelialization of diabetic foot ulcers after hyperbaric oxygen therapy. Open Access Maced J Med Sci. 2019;7(19):3177–3183. doi:10.3889/oamjms.2019.297
55. Schmidt BM, Kaye KS, Armstrong DG, Pop-Busui R. Empirical antibiotic therapy in diabetic foot ulcer infection increases hospitalization. Open Forum Infect Dis. 2023;10(10):ofad495. doi:10.1093/ofid/ofad495
56. Cimşit M, Uzun G, Yildiz S. Hyperbaric oxygen therapy as an anti-infective agent. Expert Rev Anti Infect Ther. 2009;7(8):1015–1026. doi:10.1586/eri.09.76
57. Mackay K, Thompson R, Parker M, et al. The role of hyperbaric oxygen therapy in the treatment of diabetic foot ulcers - A literature review. J Diabet Complicat. 2025;39(3):108973. doi:10.1016/j.jdiacomp.2025.108973
58. Dayya D, O’Neill OJ, Huedo-Medina TB, Habib N, Moore J, Iyer K. Debridement of diabetic foot ulcers. Adv Wound Care. 2022;11(12):666–686. doi:10.1089/wound.2021.0016
59. Zhao S, Hu X, Zhao Y, et al. Hydrogel-based therapies for diabetic foot ulcers: recent developments and clinical implications. Burns Trauma. 2025;13:tkae084. doi:10.1093/burnst/tkae084
60. Dumville JC, O’Meara S, Deshpande S, Speak K. Alginate dressings for healing diabetic foot ulcers. Cochrane Database Syst Rev. 2013;2013(6):Cd009110. doi:10.1002/14651858.CD009110.pub3
61. Dumville JC, Deshpande S, O’Meara S, Speak K. Hydrocolloid dressings for healing diabetic foot ulcers. Cochrane Database Syst Rev. 2012;(2):Cd009099. doi:10.1002/14651858.CD009099.pub2
62. Wang YC, Lee HC, Chen CL, et al. The effects of silver-releasing foam dressings on diabetic foot ulcer healing. J Clin Med. 2021;10(7). doi:10.3390/jcm10071495
63. Richetta AG, Cantisani C, Li VW, et al. Hydrofiber dressing and wound repair: review of the literature and new patents. Recent Pat Inflamm Allergy Drug Discov. 2011;5(2):150–154. doi:10.2174/187221311795399264
64. Zhao Y, Wang Q, Yan S, et al. Bletilla striata polysaccharide promotes diabetic wound healing through inhibition of the NLRP3 inflammasome. Front Pharmacol. 2021;12:659215. doi:10.3389/fphar.2021.659215
65. Li S, Yang P, Ding X, Zhang H, Ding Y, Tan Q. Puerarin improves diabetic wound healing via regulation of macrophage M2 polarization phenotype. Burns Trauma. 2022;10:tkac046. doi:10.1093/burnst/tkac046
66. Zhen Z, Wei S, Yunfei W, et al. Astragalus polysaccharide improves diabetic ulcers by promoting M2-polarization of macrophages to reduce excessive inflammation via the β-catenin/ NF-κB axis at the late phase of wound-healing. Heliyon. 2024;10(4):e24644. doi:10.1016/j.heliyon.2024.e24644
67. Sha W, Zhao B, Wei H, et al. Astragalus polysaccharide ameliorates vascular endothelial dysfunction by stimulating macrophage M2 polarization via potentiating Nrf2/HO-1 signaling pathway. Phytomedicine. 2023;112:154667. doi:10.1016/j.phymed.2023.154667
68. Ding Y, Yang P, Li S, Zhang H, Ding X, Tan Q. Resveratrol accelerates wound healing by inducing M2 macrophage polarisation in diabetic mice. Pharm Biol. 2022;60(1):2328–2337. doi:10.1080/13880209.2022.2149821
69. Youjun D, Huang Y, Lai Y, et al. Mechanisms of resveratrol against diabetic wound by network pharmacology and experimental validation. Ann Med. 2023;55(2):2280811. doi:10.1080/07853890.2023.2280811
70. Zhang Z, Yang W, Chen J, Chen X, Gu Y. Efficacy and mechanism of Schisandra chinensis active component Gomisin A on diabetic skin wound healing: network pharmacology and in vivo experimental validation. J Ethnopharmacol. 2025;337(Pt 1):118828. doi:10.1016/j.jep.2024.118828
71. Tuhin RH, Begum MM, Rahman MS, et al. Wound healing effect of Euphorbia hirta linn. (Euphorbiaceae) in alloxan induced diabetic rats. BMC Complement Altern Med. 2017;17(1):423. doi:10.1186/s12906-017-1930-x
72. Huang L, Cai HA, Zhang MS, Liao RY, Huang X, Hu FD. Ginsenoside Rg1 promoted the wound healing in diabetic foot ulcers via miR-489-3p/Sirt1 axis. J Pharmacol Sci. 2021;147(3):271–283. doi:10.1016/j.jphs.2021.07.008
73. Cai HA, Huang L, Zheng LJ, et al. Ginsenoside (Rg-1) promoted the wound closure of diabetic foot ulcer through iNOS elevation via miR-23a/IRF-1 axis. Life Sci. 2019;233:116525. doi:10.1016/j.lfs.2019.05.081
74. Xiao M, Qiu Y, Jiang C, Zhang C, Yao J. Upregulation of miR-155-5p impaired ginsenoside Rg1-mediated wound healing in diabetic foot ulcers by targeting E2F2/CDCA7L signaling: rg1 improves DFU wound healing via inhibiting miR-155-5p. Mol Biol Rep. 2025;52(1):523. doi:10.1007/s11033-025-10600-5
75. Xiao F, Rui S, Zhang X, et al. Accelerating diabetic wound healing with Ramulus Mori (Sangzhi) alkaloids via NRF2/HO-1/eNOS pathway. Phytomedicine. 2024;134:155990. doi:10.1016/j.phymed.2024.155990
76. Liu Y, Li Z, Li W, et al. Discovery of β-sitosterol’s effects on molecular changes in rat diabetic wounds and its impact on angiogenesis and macrophages. Int Immunopharmacol. 2024;126:111283. doi:10.1016/j.intimp.2023.111283
77. Jia X, Yang J, Guo Q, et al. Hypoxia-inducible factor-1α/vascular endothelial growth factor signaling pathway-based ulcer-healing mechanism of Astragalus Aqueous extract in diabetic foot rats. Cell Mol Biol. 2024;70(7):79–84. doi:10.14715/cmb/2024.70.7.11
78. Xiao K, Wang S, Li G, Chen W, Chen B, Li X. Resveratrol promotes diabetic wound healing by inhibiting ferroptosis in vascular endothelial cells. Burns. 2024;50(9):107198. doi:10.1016/j.burns.2024.07.002
79. Tang G, Wang Y, Deng P, et al. Mechanism of dracorhodin in accelerating diabetic foot ulcer healing via the Nrf2 pathway, a network pharmacology, molecular docking and experimental validation. Sci Rep. 2025;15(1):12492. doi:10.1038/s41598-025-97831-5
80. Liu L, Wang H, Zhou J, et al. Narirutin treatment accelerates the process of diabetic wound repair by regulating phenotype switching of macrophages through affecting metabolic reprogramming. Front Pharmacol. 2025;16:1614967. doi:10.3389/fphar.2025.1614967
81. Yang N, Shi N, Yao Z, Liu H, Guo W. Gallium-modified gelatin nanoparticles loaded with quercetin promote skin wound healing via the regulation of bacterial proliferation and macrophage polarization. Front Bioeng Biotechnol. 2023;11:1124944. doi:10.3389/fbioe.2023.1124944
82. Kamar SS, Abdel-Kader DH, Rashed LA. Beneficial effect of Curcumin nanoparticles-hydrogel on excisional skin wound healing in type-I diabetic rat: histological and immunohistochemical studies. Ann Anat. 2019;222:94–102. doi:10.1016/j.aanat.2018.11.005
83. Algandaby MM, Esmat A, Nasrullah MZ, et al. LC-MS based metabolic profiling and wound healing activity of a chitosan nanoparticle-loaded formula of Teucrium polium in diabetic rats. Biomed Pharmacother. 2023;168:115626. doi:10.1016/j.biopha.2023.115626
84. Gong H, Yang L, Li Y, et al. Metal-polyphenol nanocomposite hybrid hydrogel: a multifunctional platform for treating diabetic foot ulcers through metabolic microenvironment reprogramming. Biomaterials. 2025;322:123414. doi:10.1016/j.biomaterials.2025.123414
85. Nie X, Zhang H, Shi X, et al. Asiaticoside nitric oxide gel accelerates diabetic cutaneous ulcers healing by activating Wnt/β-catenin signaling pathway. Int Immunopharmacol. 2020;79:106109. doi:10.1016/j.intimp.2019.106109
86. Mu X, Chen J, Zhu H, et al. Asiaticoside-nitric oxide synergistically accelerate diabetic wound healing by regulating key metabolites and SRC/STAT3 signaling. Burns Trauma. 2025;13:tkaf009. doi:10.1093/burnst/tkaf009
87. Liu YQ, Zhang D, Deng J, Liu Y, Li W, Nie X. Preparation and safety evaluation of centella asiatica total glycosides nitric oxide gel and its therapeutic effect on diabetic cutaneous ulcers. Evid Based Complement Alternat Med. 2022;2022:1419146. doi:10.1155/2022/1419146
88. Chen X, Hu Z, Zhao K, et al. Microenvironment-responsive, multimodulated herbal polysaccharide hydrogel for diabetic foot ulcer healing. Sci Rep. 2024;14(1):22135. doi:10.1038/s41598-024-72972-1
89. Huang YY, Lin CW, Cheng NC, et al. Effect of a novel macrophage-regulating drug on wound healing in patients with diabetic foot ulcers: a randomized clinical trial. JAMA Network Open. 2021;4(9):e2122607. doi:10.1001/jamanetworkopen.2021.22607
90. Chang SC, Lin CW, Chen JC, et al. Effects of ON101 for hard-to-heal diabetic foot ulcers in a randomized Phase III trial: a Post Hoc analysis. Adv Wound Care. 2024. doi:10.1089/wound.2023.0167
91. Fallah Huseini H, Yaghoobi M, Fallahi F, et al. Topical administration of teucrium polium on diabetic foot ulcers accelerates healing: a placebo-controlled randomized clinical study. Int J Low Extrem Wounds. 2024;23(2):238–246. doi:10.1177/15347346211048371
92. Wang H, Pei S, Fang S, et al. Irisin restores high glucose-induced cell injury in vascular endothelial cells by activating Notch pathway via Notch receptor 1. Biosci Biotechnol Biochem. 2021;85(10):2093–2102. doi:10.1093/bbb/zbab137
93. Taowen P, Shuyuan F, Xiaoli S, et al. Study on the action mechanism of the peptide compounds of Wuguchong on diabetic ulcers, based on UHPLC-Q-TOF-MS, network pharmacology and experimental validation. J Ethnopharmacol. 2022;288:114974. doi:10.1016/j.jep.2022.114974
94. Ding X, Li S, Huang H, et al. Bioactive triterpenoid compounds of Poria cocos (Schw.) Wolf in the treatment of diabetic ulcers via regulating the PI3K-AKT signaling pathway. J Ethnopharmacol. 2024;325:117812. doi:10.1016/j.jep.2024.117812
95. Tian M, Wu J, Du Q, et al. Revealing the mechanisms of shikonin against diabetic wounds: a combined network pharmacology and in vitro investigation. J Diabetes Res. 2025;2025:4656485. doi:10.1155/jdr/4656485
96. Bardaa S, Makni K, Boudaouara O, et al. Development and evaluation of the wound healing effect of a novel topical cream formula based on Ginkgo biloba extract on wounds in diabetic rats. Biomed Res Int. 2021;2021:6474706. doi:10.1155/2021/6474706
97. Akter S, Ahmad SU, Bhuiyan MA, et al. Network pharmacology, molecular docking and experimental validation on potential application of diabetic wound healing of Cinnamomum zeylanicum through matrix metalloproteinases-8 and 9 (MMP-8 And MMP-9). Drug Des Devel Ther. 2025;19:1753–1782. doi:10.2147/dddt.S489113
98. Daemi A, Lotfi M, Farahpour MR, Oryan A, Ghayour SJ, Sonboli A. Topical application of Cinnamomum hydroethanolic extract improves wound healing by enhancing re-epithelialization and keratin biosynthesis in streptozotocin-induced diabetic mice. Pharm Biol. 2019;57(1):799–806. doi:10.1080/13880209.2019.1687525
99. Mao X, Li Z, Li B, Wang H. Baicalin regulates mRNA expression of VEGF-c, Ang-1/Tie2, TGF-β and Smad2/3 to inhibit wound healing in streptozotocin-induced diabetic foot ulcer rats. J Biochem Mol Toxicol. 2021;35(11):e22893. doi:10.1002/jbt.22893
100. Li W, Kandhare AD, Mukherjee AA, Bodhankar SL. Hesperidin, a plant flavonoid accelerated the cutaneous wound healing in streptozotocin-induced diabetic rats: role of TGF-ß/Smads and Ang-1/Tie-2 signaling pathways. Excli J. 2018;17:399–419. doi:10.17179/excli2018-1036
101. Zhang EY, Gao B, Shi HL, et al. 20(S)-Protopanaxadiol enhances angiogenesis via HIF-1α-mediated VEGF secretion by activating p70S6 kinase and benefits wound healing in genetically diabetic mice. Exp Mol Med. 2017;49(10):e387. doi:10.1038/emm.2017.151
102. Guo J, Hu Z, Yan F, et al. Angelica dahurica promoted angiogenesis and accelerated wound healing in db/db mice via the HIF-1α/PDGF-β signaling pathway. Free Radic Biol Med. 2020;160:447–457. doi:10.1016/j.freeradbiomed.2020.08.015
103. Zhang XN, Ma ZJ, Wang Y, et al. Angelica Dahurica ethanolic extract improves impaired wound healing by activating angiogenesis in diabetes. PLoS One. 2017;12(5):e0177862. doi:10.1371/journal.pone.0177862
104. Song M, Chen L, Zhang L, et al. Cryptotanshinone enhances wound healing in type 2 diabetes with modulatory effects on inflammation, angiogenesis and extracellular matrix remodelling. Pharm Biol. 2020;58(1):845–853. doi:10.1080/13880209.2020.1803369
105. Song J, Zeng J, Zheng S, et al. Sanguisorba officinalis L. promotes diabetic wound healing in rats through inflammation response mediated by macrophage. Phytother Res. 2023;37(9):4265–4281. doi:10.1002/ptr.7906
106. Kun L, Yunpeng D, Shuyuan F. Mechanism of DT-13 regulating macrophages in diabetic wound healing. Cell Signal. 2024;124:111446. doi:10.1016/j.cellsig.2024.111446
107. Chen C, Lin Z, Liu W, et al. Emodin accelerates diabetic wound healing by promoting anti-inflammatory macrophage polarization. Eur J Pharmacol. 2022;936:175329. doi:10.1016/j.ejphar.2022.175329
108. Huang Y, Wang B, Ma Z, et al. Sulforaphane promotes diabetic wound healing by regulating macrophage efferocytosis and polarization. Int Immunopharmacol. 2025;150:114243. doi:10.1016/j.intimp.2025.114243
109. Li K, Wu L, Jiang J. Apigenin accelerates wound healing in diabetic mice by promoting macrophage M2-type polarization via increasing miR-21 expression. Mol Cell Biochem. 2024;479(11):3119–3127. doi:10.1007/s11010-023-04885-y
110. Zhang Z, Chen T, Liu W, Xiong J, Jiang L, Liu M. Paeonol accelerates skin wound healing by regulating macrophage polarization and inflammation in diabetic rats. Kor J Physiol Pharmacol. 2023;27(5):437–448. doi:10.4196/kjpp.2023.27.5.437
111. Li K, Zhang Y, Diao Y, Fan S. Paeonol regulates the DDIT4-mTOR signaling pathway in macrophages to promote diabetic wound healing. Int Immunopharmacol. 2025;151:114347. doi:10.1016/j.intimp.2025.114347
112. Lei L, Wan G, Geng X, et al. The total iridoid glycoside extract of Lamiophlomis rotata Kudo induces M2 macrophage polarization to accelerate wound healing by RAS/ p38 MAPK/NF-κB pathway. J Ethnopharmacol. 2023;307:116193. doi:10.1016/j.jep.2023.116193
113. Geng X, Wang Y, Li H, et al. Total iridoid glycoside extract of Lamiophlomis rotata (Benth) Kudo accelerates diabetic wound healing by the NRF2/COX2 axis. Chin Med. 2024;19(1):53. doi:10.1186/s13020-024-00921-1
114. Chen J, Ma H, Meng Y, et al. Analysis of the mechanism underlying diabetic wound healing acceleration by Calycosin-7-glycoside using network pharmacology and molecular docking. Phytomedicine. 2023;114:154773. doi:10.1016/j.phymed.2023.154773
115. Liu Y, Zhao J, Mu X, et al. Asiaticoside-nitric oxide promoting diabetic wound healing through the miRNA-21-5p/TGF-β1/SMAD7/TIMP3 signaling pathway. J Ethnopharmacol. 2024;319(Pt 2):117266. doi:10.1016/j.jep.2023.117266
116. Ye P, Wu X, Gu R, et al. ACNO hydrogel enhances diabetic wound healing by modulating the Bcl-2/Bax/Caspase-3/PARP pathway. Int Immunopharmacol. 2025;147:113997. doi:10.1016/j.intimp.2024.113997
117. Fu J, Huang J, Lin M, Xie T, You T. Quercetin promotes diabetic wound healing via switching macrophages from M1 to M2 polarization. J Surg Res. 2020;246:213–223. doi:10.1016/j.jss.2019.09.011
118. Zhang Z, Wang L, Li X, Miao Y, Li D. Integrating network pharmacology, molecular docking and experimental validation to explore the pharmacological mechanisms of quercetin against diabetic wound. Int J Med Sci. 2024;21(14):2837–2850. doi:10.7150/ijms.100468
119. Kant V, Jangir BL, Sharma M, Kumar V, Joshi VG. Topical application of quercetin improves wound repair and regeneration in diabetic rats. Immunopharmacol Immunotoxicol. 2021;43(5):536–553. doi:10.1080/08923973.2021.1950758
120. Fallah Huseini H, Abdolghaffari AH, Ahwazi M, Jasemi E, Yaghoobi M, Ziaee M. Topical application of teucrium polium can improve wound healing in diabetic rats. Int J Low Extrem Wounds. 2020;19(2):132–138. doi:10.1177/1534734619868629
121. Gharaboghaz MNZ, Farahpour MR, Saghaie S. Topical co-administration of Teucrium polium hydroethanolic extract and Aloe vera gel triggered wound healing by accelerating cell proliferation in diabetic mouse model. Biomed Pharmacother. 2020;127:110189. doi:10.1016/j.biopha.2020.110189
122. Dehghani S, Dalirfardouei R, Jafari Najaf Abadi MH, Ebrahimi Nik M, Jaafari MR, Mahdipour E. Topical application of curcumin regulates the angiogenesis in diabetic-impaired cutaneous wound. Cell Biochem Funct. 2020;38(5):558–566. doi:10.1002/cbf.3500
123. Dardmah F, Farahpour MR. Quercus infectoria gall extract aids wound healing in a streptozocin-induced diabetic mouse model. J Wound Care. 2021;30(8):618–625. doi:10.12968/jowc.2021.30.8.618
124. Farahpour MR, Pirkhezr E, Ashrafian A, Sonboli A. Accelerated healing by topical administration of Salvia officinalis essential oil on Pseudomonas aeruginosa and Staphylococcus aureus infected wound model. Biomed Pharmacother. 2020;128:110120. doi:10.1016/j.biopha.2020.110120
125. Güzel S, Özay Y, Kumaş M, et al. Wound healing properties, antimicrobial and antioxidant activities of Salvia kronenburgii Rech. f. and Salvia euphratica Montbret, Aucher & Rech. f. var. euphratica on excision and incision wound models in diabetic rats. Biomed Pharmacother. 2019;111:1260–1276. doi:10.1016/j.biopha.2019.01.038
126. Manzuoerh R, Farahpour MR, Oryan A, Sonboli A. Effectiveness of topical administration of Anethum graveolens essential oil on MRSA-infected wounds. Biomed Pharmacother. 2019;109:1650–1658. doi:10.1016/j.biopha.2018.10.117
127. Li H, Chen C, Chen X, et al. Identification of active ingredients from Lamiophlomis rotata that increase wound repair in mouse skin. Br J Pharmacol. 2025;182(12):2754–2771. doi:10.1111/bph.17452
128. Bai X, He T, Liu J, et al. Loureirin B inhibits fibroblast proliferation and extracellular matrix deposition in hypertrophic scar via TGF-β/Smad pathway. Exp Dermatol. 2015;24(5):355–360. doi:10.1111/exd.12665
129. Wahedi HM, Jeong M, Chae JK, Do SG, Yoon H, Kim SY. Aloesin from Aloe vera accelerates skin wound healing by modulating MAPK/Rho and Smad signaling pathways in vitro and in vivo. Phytomedicine. 2017;28:19–26. doi:10.1016/j.phymed.2017.02.005
130. Xu C, Hu L, Zeng J, et al. Gynura divaricata (L.) DC. promotes diabetic wound healing by activating Nrf2 signaling in diabetic rats. J Ethnopharmacol. 2024;323:117638. doi:10.1016/j.jep.2023.117638
131. Sun X, Wang X, Zhao Z, Chen J, Li C, Zhao G. Paeoniflorin accelerates foot wound healing in diabetic rats though activating the Nrf2 pathway. Acta Histochem. 2020;122(8):151649. doi:10.1016/j.acthis.2020.151649
132. Deng P, Liang H, Wang S, et al. Combined metabolomics and network pharmacology to elucidate the mechanisms of Dracorhodin Perchlorate in treating diabetic foot ulcer rats. Front Pharmacol. 2022;13:1038656. doi:10.3389/fphar.2022.1038656
133. Sun Y, Gao C, Liu H, Liu X, Yue T. Exploring the mechanism by which aqueous Gynura divaricata inhibits diabetic foot based on network pharmacology, molecular docking and experimental verification. Mol Med. 2023;29(1):11. doi:10.1186/s10020-023-00605-w
134. Zhang E, Gao B, Yang L, Wu X, Wang Z. Notoginsenoside Ft1 promotes fibroblast proliferation via PI3K/Akt/mTOR signaling pathway and benefits wound healing in genetically diabetic mice. J Pharmacol Exp Ther. 2016;356(2):324–332. doi:10.1124/jpet.115.229369
135. Liu YS, Lai MC, Tzeng YC, Liu IM. Polyphenolic hispolon derived from medicinal mushrooms of the inonotus and phellinus genera promotes wound healing in hyperglycemia-induced impairments. Nutrients. 2025;17(2). doi:10.3390/nu17020266
136. Sanaei N, Mohammadi R, Raisi A, Zarei L. Extract of Berula angustifolia (L.) Mertens enhances wound healing in streptozotocin-induced diabetic rats. Wounds. 2018;30(8):242–248.
137. Khodaie SA, Emadi F, Naseri M, et al. The effect of Myrtus communis Aqueous extract-containing gel on wound healing in streptozotocin-induced diabetic rats. Curr Drug Discov Technol. 2021;18(4):542–547. doi:10.2174/1570163817666200712163956
138. Duarte MS, Fuhro VM, de Souza Nogueira J, Romana-Souza B. Polyphenol hydroxytyrosol present olive oil improves skin wound healing of diabetic mice. Wound Repair Regen. 2024;32(6):904–915. doi:10.1111/wrr.13217
139. Nasiry D, Khalatbary AR, Ghaemi A, Ebrahimzadeh MA, Hosseinzadeh MH. Topical administration of Juglans regia L. leaf extract accelerates diabetic wound healing. BMC Complement Med Ther. 2022;22(1):255. doi:10.1186/s12906-022-03735-6
140. Atia A, Atmani-Kilani D, Atmani D, et al. Wound healing potential of a formula based on Populus nigra L. flower buds extract with anti-inflammatory activity. J Ethnopharmacol. 2024;331:118319. doi:10.1016/j.jep.2024.118319
141. Soheilifar MH, Dastan D, Masoudi-Khoram N, et al. In vitro and in vivo evaluation of the diabetic wound healing properties of Saffron (Crocus Sativus L.) petals. Sci Rep. 2024;14(1):19373. doi:10.1038/s41598-024-70010-8
142. Daemi A, Farahpour MR, Oryan A, Karimzadeh S, Tajer E. Topical administration of hydroethanolic extract of Lawsonia inermis (henna) accelerates excisional wound healing process by reducing tissue inflammation and amplifying glucose uptake. Kaohsiung J Med Sci. 2019;35(1):24–32. doi:10.1002/kjm2.12005
143. Kshetrimayum V, Chanu KD, Biona T, et al. Paris polyphylla Sm. characterized extract infused ointment accelerates diabetic wound healing in in-vivo model. J Ethnopharmacol. 2024;331:118296. doi:10.1016/j.jep.2024.118296
144. Manzoureh R, Farahpour MR. Topical administration of hydroethanolic extract of Trifolium pratense (red clover) accelerates wound healing by apoptosis and re-epithelialization. Biotech Histochem. 2021;96(4):276–286. doi:10.1080/10520295.2020.1797875
145. Özay Y, Güzel S, Yumrutaş Ö, et al. Wound healing effect of kaempferol in diabetic and nondiabetic rats. J Surg Res. 2019;233:284–296. doi:10.1016/j.jss.2018.08.009
146. Omarizadeh K, Farahpour MR, Alipour M. Topical administration of an ointment prepared from satureja Sahendica essential oil accelerated infected full-thickness wound healing by modulating inflammatory response in a mouse model. Wounds. 2021;33(12):321–328.
147. Al-Qaisi T, Al-Rawadeih S, Alsarayreh A, et al. The effects of Anchusa azurea methanolic extract on burn wound healing: histological, antioxidant, and anti-inflammatory evaluation. Burns. 2024;50(7):1812–1822. doi:10.1016/j.burns.2024.05.001
148. Can NM, Thao DTP. Wound healing activity of Crassocephalum crepidioides (Benth.) S. Moore. Leaf hydroethanolic extract. Oxid Med Cell Longev. 2020;2020:2483187. doi:10.1155/2020/2483187
149. Figueiredo FF, Cechinel Filho V, Damazo AS, et al. Sorocea guilleminiana Gaudich.: wound healing activity, action mechanisms, and chemical characterization of the leaf infusion. J Ethnopharmacol. 2020;248:112307. doi:10.1016/j.jep.2019.112307
150. Hashemnia M, Nikousefat Z, Mohammadalipour A, Zangeneh MM, Zangeneh A. Wound healing activity of Pimpinella anisum methanolic extract in streptozotocin-induced diabetic rats. J Wound Care. 2019;28(Sup10):S26–s36. doi:10.12968/jowc.2019.28.Sup10.S26
151. Ozay Y, Ozkorkmaz EG, Kumas-Kulualp M, et al. Wound healing activity of Salvia huberi ethanolic extract in streptozocin-induced diabetic rats. J Wound Care. 2023;32(Sup3a):i–xiii. doi:10.12968/jowc.2023.32.Sup3a.i
152. Chandran R, Abrahamse H, Parimelazhagan T, Durai G. Syzygium mundagam bark methanol extract restores skin to normal in diabetic wounded rats. Biomed Pharmacother. 2017;94:781–786. doi:10.1016/j.biopha.2017.07.114
153. Naji S, Zarei L, Pourjabali M, Mohammadi R. The extract of Lycium depressum stocks enhances wound healing in streptozotocin-induced diabetic rats. Int J Low Extrem Wounds. 2017;16(2):85–93. doi:10.1177/1534734617700538
154. Dos Santos Gramma LS, Marques FM, Vittorazzi C, et al. Struthanthus vulgaris ointment prevents an over expression of inflammatory response and accelerates the cutaneous wound healing. J Ethnopharmacol. 2016;190:319–327. doi:10.1016/j.jep.2016.06.050
155. Upadhyay NK, Keshri GK, Gupta A. Hippophae rhamnoides L. leaf extract augments dermal wound healing in streptozocin-induced diabetic rats. J Wound Care. 2025;34(2):146–153. doi:10.12968/jowc.2021.0309
156. Yan Y, Liu X, Zhuang Y, et al. Pien Tze Huang accelerated wound healing by inhibition of abnormal fibroblast apoptosis in Streptozotocin induced diabetic mice. J Ethnopharmacol. 2020;261:113203. doi:10.1016/j.jep.2020.113203
157. Muyumba NW, Mutombo SC, Sheridan H, Nachtergael A, Duez P. Quality control of herbal drugs and preparations: the methods of analysis, their relevance and applications. Talanta Open. 2021;4:100070. doi:10.1016/j.talo.2021.100070
158. Wang H, Chen Y, Wang L, Liu Q, Yang S, Wang C. Advancing herbal medicine: enhancing product quality and safety through robust quality control practices. Front Pharmacol. 2023;14:1265178. doi:10.3389/fphar.2023.1265178
159. Spicer AB, Cavalcanti AB, Zampieri FG. Subgroup analyses and heterogeneity of treatment effects in randomized trials: a primer for the clinician. Curr Opin Crit Care. 2024;30(5):427–438. doi:10.1097/mcc.0000000000001186
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Research Progress on Nanoformulations Based on Active Components from Traditional Chinese Medicine for MASLD
Gou ZX, Li NW, Yao JY, Wang YL
International Journal of Nanomedicine 2026, 21:597554
Published Date: 30 April 2026