Back to Journals » Clinical Ophthalmology » Volume 19
Advanced Age Does Not Predispose to Intraoperative Complications Among High-Risk Cataract Surgeries
Authors Nemet A ![]() , Anaki L, Shitrit IB, Wasser LM, Plopsky G, Beluga S, Tuuminen R
, Anaki L, Shitrit IB, Wasser LM, Plopsky G, Beluga S, Tuuminen R ![]()
Received 15 July 2025
Accepted for publication 23 September 2025
Published 6 October 2025 Volume 2025:19 Pages 3713—3718
DOI https://doi.org/10.2147/OPTH.S553936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Achia Nemet,1,2 Liron Anaki,2 Itamar Ben Shitrit,2 Lauren M Wasser,1,2 Gilad Plopsky,1,2 Sagiv Beluga,3,4 Raimo Tuuminen5– 7
1Department of Ophthalmology, Assuta Ashdod University Medical Center, Ashdod, Israel; 2Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer Sheva, Israel; 3Department of Ophthalmology, Kaplan Medical Center, Rehovot, Israel; 4Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel; 5Helsinki Retina Research Group, Faculty of Medicine, University of Helsinki, Helsinki, Finland; 6Department of Ophthalmology, Kymenlaakso Central Hospital, Kotka, Finland; 7Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel
Correspondence: Raimo Tuuminen, Chief Physician, Kymenlaakso Central Hospital, Department of Ophthalmology, Kotkantie 41, FI-48210, Kotka, Finland, Tel +358 50 411 3870, Email [email protected]
Background: To examine whether advanced age predisposes to intraoperative complications among cataract surgery cohort preoperatively stratified as high-risk.
Methods: A retrospective analysis of 100 consecutive patients, 75 of which aged under 80 vs 25 of which aged 80 or above were analyzed for operation time, complication rates, postoperative best-corrected visual acuity (BCVA), and intraocular pressure. Secondary outcomes analysis focused on multivariable models on age and surgical outcomes adjusted for preoperative complication risk factors such as nuclear sclerosis severity, pseudoexfoliation, and intraoperative floppy iris syndrome (IFIS) and ocular comorbidities such as age-related macular degeneration and glaucoma.
Results: Baseline variables for sex distribution, concomitant ocular and systemic comorbidities, nuclear sclerosis grade, pseudoexfoliation, BCVA, and IOP were comparable between the groups. None of the patients underwent anterior or posterior vitrectomy. No differences were observed in the rate of intraoperative floppy iris (IFIS) syndrome (17% vs 16%, P=1.000) and the use of surgical adjuncts such as iris hooks (1.3% vs 4.0%, P=0.439) between patients aged under 80 years and those 80 years or above. Postoperative BCVA at 1 week (0.33± 0.35 LogMAR units vs 0.33± 0.29 LogMAR units, P=0.962) did not differ between those aged under 80 years and 80 years or above. For patient age at surgery, correlation analysis revealed no associations with operation time (B: − 0.09; 95% CI: − 0.44 to 0.27; P=0.628), surgical challenge rate (B: 1.12; 95% CI: 1.00 to 1.27; P=0.073), or postoperative BCVA at 1 week (B: 0.004; 95% CI: − 0.012 to 0.005; P=0.379). In multivariable analysis, patient age at surgery remained non-significant for operation time when adjusted for pseudoexfoliation and IFIS (B: − 0.07, 95% CI: − 0.43, 0.30; P=0.629). After adjustment for wet AMD and glaucoma, advancing age showed a trend towards worse 1-week postoperative BCVA, with each additional year corresponding to a 0.01 decline in LogMAR units (B: − 0.01; 95% CI: − 0.02, 0.00; P=0.051).
Conclusion: Advanced age should not be treated as an inherent risk factor or contraindication for cataract surgery in high-risk patients.
Keywords: advanced age, cataract surgery, intraoperative complications, intraoperative floppy iris syndrome, pseudoexfoliation, surgical outcomes
Introduction
Cataract surgery is most commonly performed and successful ophthalmic procedures worldwide;1 primarily aimed at restoring vision impaired by the opacification of the eye’s natural lens. With advancements in surgical techniques and intraocular lens (IOL) technology,2 the procedure has witnessed remarkable improvements in safety and efficacy.3 However, patient-specific factors, notably age, are assumed to influence postoperative outcomes.4
With increasing life expectancy, the demand for cataract surgery in older patients—those aged 80 years and older—continues to grow steadily, with nearly all individuals in their 90s exhibiting clinically significant cataracts.5 Despite improvements in surgical techniques and technologies, the question of whether advanced age itself constitutes an independent risk factor for adverse surgical outcomes remains under debate. Recent studies have demonstrated that elderly patients undergoing cataract surgery may face an increased risk of specific complications. These complications include posterior capsule rupture (PCR), elevated intraocular pressure, and corneal edema, likely due to age-related changes such as zonular weakness and thinner posterior capsules.4,6 Other studies have suggested that poorer postoperative outcomes observed in elderly populations may be more strongly attributed to coexisting ocular and systemic comorbidities rather than chronological age alone.7,8
Here, we aimed to evaluate whether advanced age predisposes to complications in high-risk cataract surgery patients.
Methods
Study Design
We performed a retrospective review of the records of patients who underwent cataract surgery between January 1, 2023, and December 31, 2023, at Assuta Ashdod Medical Center, Ashdod, Israel. The Institutional Review Board (IRB)/ethics committee of the 0015–23-AAA approved the study. Patient consent to review their medical records was waived due to the retrospective non-interventional nature of the study. Confidentiality of patient data was maintained. Study protocol adhered to the tenets of the Declaration of Helsinki.
Study Participants
Cataract surgery cohort preoperatively stratified as high-risk. A hundred consecutive patients, 75 of which were aged under 80 vs 25 of which were aged 80 or above. The major risk factors in both groups were risk for IFIS and pseudoexfoliation syndrome.
Preoperative Assessment
All patients were evaluated at the preoperative cataract surgery clinic of the Ophthalmology Department at Assuta Ashdod Medical Center. Cataract grading was performed using a standardized classification protocol, ensuring consistency across all examining ophthalmologists.9,10 In addition, autorefractive keratometry was performed using a NIDEK autorefractor (NIDEK Co., Ltd. Japan), and ocular biometry was conducted with a TOMEY device (TOMEY Corporation, Japan).
Postoperative Objective Outcome Measures
Best-corrected visual acuity (BCVA) was measured at 4 m under photopic conditions (167 candelas [cd]/m2). Visual acuity was measured using decimal fractions and converted into LogMAR for statistical analysis.
Statistical Analysis
An initial descriptive analysis was performed to characterize the sample population and compare baseline characteristics between age groups (<80 vs ≥80 years). Categorical variables were analyzed using the χ²-test or Fisher’s exact test (when sample size in any of the group ≤ 5). Continuous variables were assessed for normality using the Shapiro–Wilk test and visual inspection of histograms. Normally distributed continuous variables were compared using Student’s t-test, while non-normally distributed continuous variables were analyzed with the Mann–Whitney U-test. To assess the association between age and surgical outcomes, we conducted both univariable and multivariable analyses. Age was analyzed both as a continuous and categorical variable (<80 vs ≥80 years).
Primary outcomes analysis included operation time, complication rates, postoperative BCVA, and IOP. Secondary outcomes analysis focused on preoperative complication risk factors such as nuclear sclerosis severity, pseudoexfoliation, and intraoperative floppy iris syndrome (IFIS). Multivariable models were adjusted for relevant confounding variables, including preoperative complication risk factors and concomitant ocular comorbidities (age-related macular degeneration, glaucoma). For the binary variables (risk factors, complications) logistic regression models were constructed, whereas for the continuous variables linear regression models were utilized. All statistical analyses were performed using R (version 4.4.3). P-value <0.05 was considered statistically significant for all analyses.
Results
The study cohort included 100 consecutive high-risk patients, of which 75 were aged under 80 and 25 were aged 80 or above (Table 1). Baseline variables for sex distribution, concomitant ocular and systemic comorbidities, nuclear sclerosis grade, pseudoexfoliation, BCVA, and IOP were comparable between the groups (Table 1).
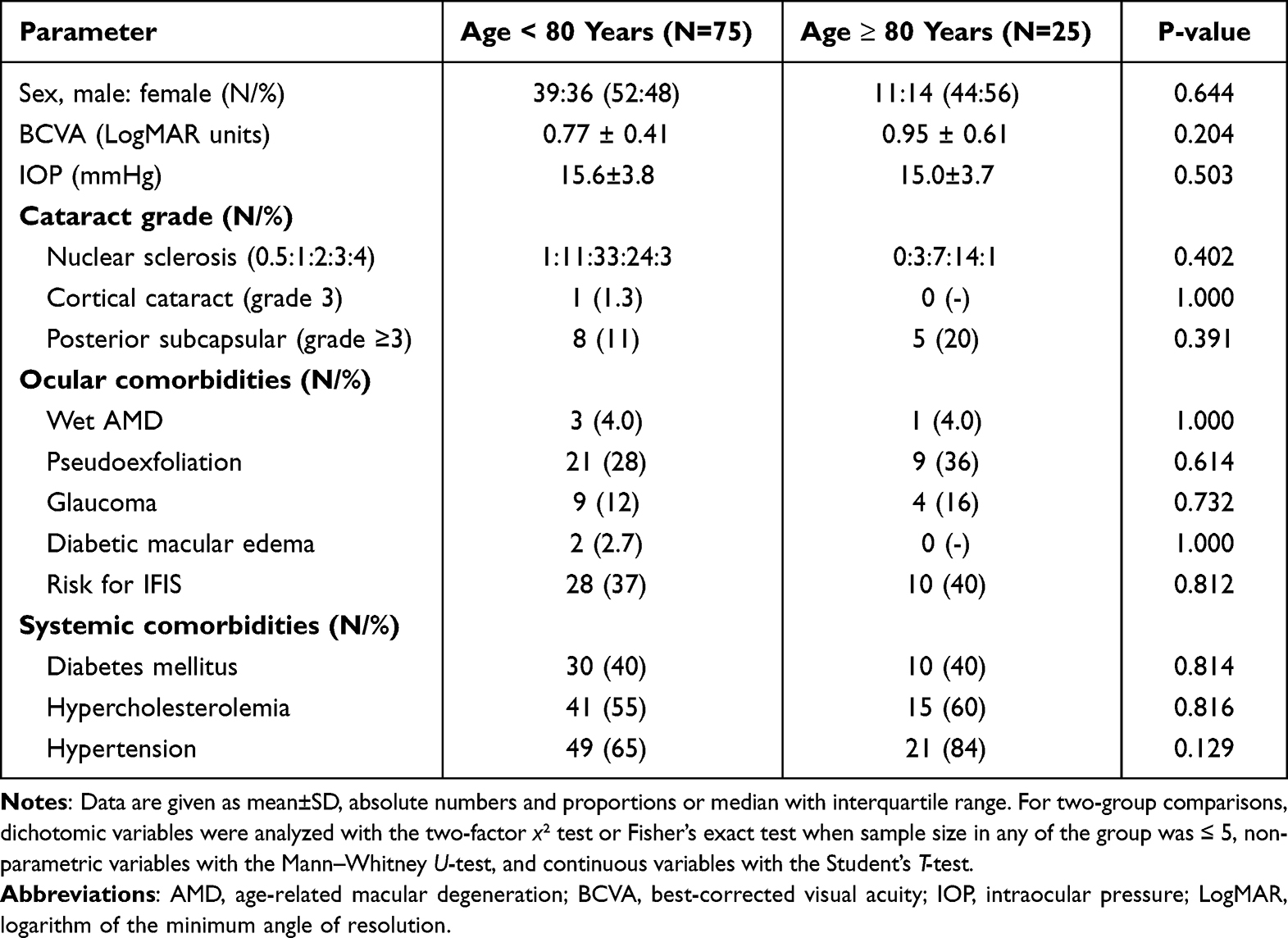 |
Table 1 Preoperative Variables |
No differences were observed in the rate of intraoperative floppy iris (IFIS) syndrome (13 out of 75 [17%] vs 4 out of 25 [16%], P=1.000) and the use of surgical adjuncts such as iris hooks (1 out of 75 [1.3%] vs 1 out of 25 [4.0%], P=0.439) between patients aged under 80 years and those 80 years or above (Table 2). Respectively, operation time between the groups was comparable (33±15 min vs 33±13 min, P=0.947, Table 2). Postoperative BCVA at 1 week (0.33±0.35 LogMAR units vs 0.33±0.29 LogMAR units, P=0.962, Table 2) did not differ between those aged under 80 years and 80 years or above, whereas postoperative IOP at 1 week was slightly higher among those aged under 80 years (14.8±3.1 mmHg) when compared to those aged 80 years or above (13.5±2.7 mmHg, P=0.049, Table 2).
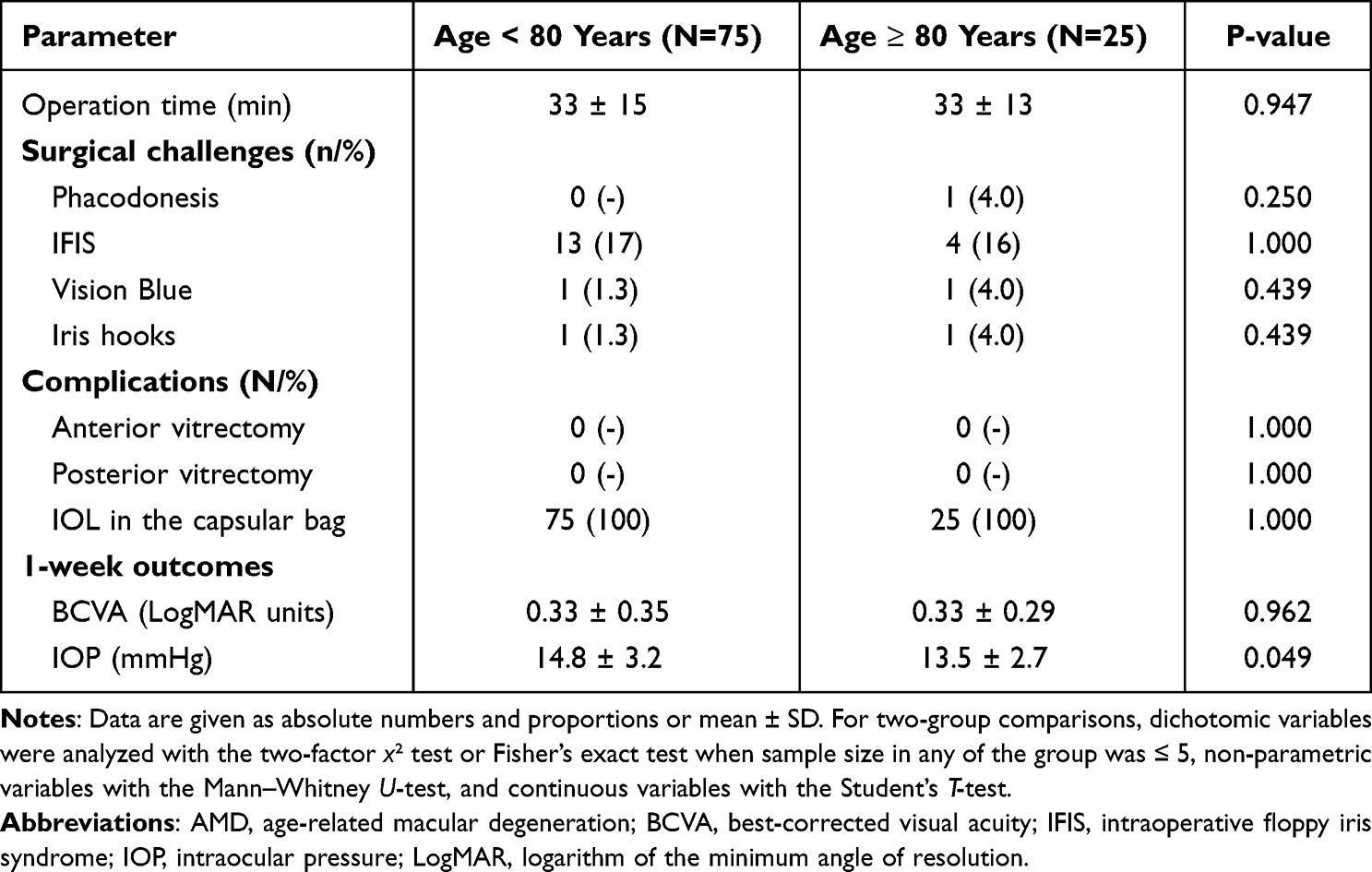 |
Table 2 Intraoperative Complications |
For patient age at surgery, correlation analysis revealed no associations with operation time (B: −0.09; 95% CI: −0.44 to 0.27; P=0.628, Table 3), surgical challenge rate (B: 1.12; 95% CI: 1.00 to 1.27; P=0.073, Table 3), postoperative BCVA at 1 week (B: 0.004; 95% CI: −0.012 to 0.005; P=0.379, Table 3), or IOP at 1 week (B: −0.04; 95% CI: −0.11 to 0.04; P=0.309, Table 3). In parallel, when comparing the patients aged under 80 years and those 80 years or above, neither operation time (B: −0.55; 95% CI: −7.29 to 6.20; P=0.873, Table 3), nor surgical challenge rate (B: 1.54; 95% CI: 0.20 to 8.46; P=0.629, Table 3), postoperative BCVA at 1 week (B: −0.01; 95% CI: −0.17 to 0.15; P=0.945, Table 3), or IOP at 1 week (B: −1.36; 95% CI: −2.81 to 0.09; P=0.066, Table 3) were different.
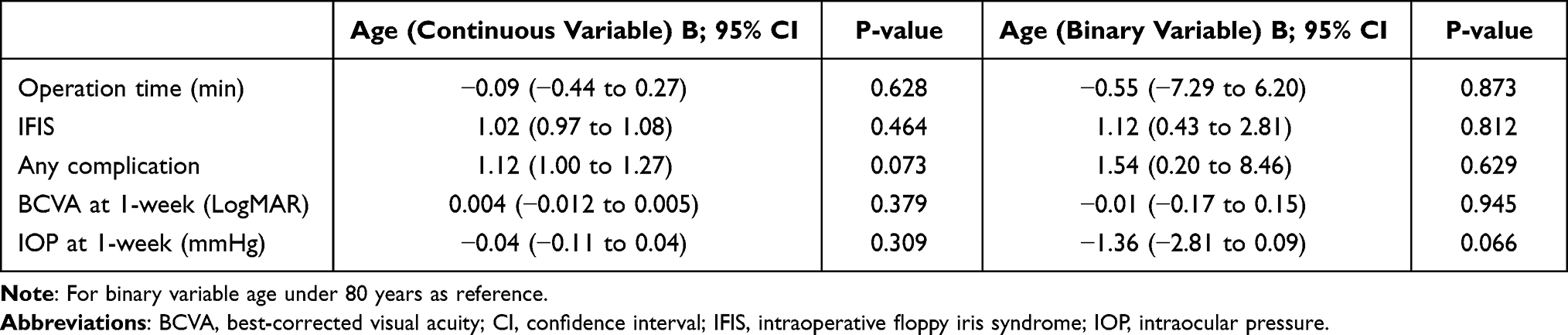 |
Table 3 The Effect of Patient Age at Surgery on Surgical Outcomes |
In multivariable analysis, patient age at surgery remained non-significant for operation time when adjusted for pseudoexfoliation and IFIS (B: −0.07, 95% CI: −0.43, 0.30; P=0.629). After adjustment for wet AMD and glaucoma, advancing age showed a trend towards worse 1-week postoperative BCVA, with each additional year corresponding to a 0.01 decline in LogMAR units (B: −0.01; 95% CI: −0.02, 0.00; P=0.051).
Discussion
This study aimed to evaluate whether advanced age (≥80 years) is associated with increased intraoperative risk or impaired outcomes after cataract surgery. A trend toward increased prevalence of certain risk factors (eg, high nuclear sclerosis grade, pseudoexfoliation, and age-related macular degeneration) was observed in older patients, but these differences did not reach statistical significance. The analysis revealed no statistically significant differences in operation time, intraoperative complication rates, or short-term visual and intraocular pressure outcomes between the groups aged under 80 years and those at least 80 years. Similarly, multivariable regression analyses did not demonstrate any significant associations between age — whether treated as a continuous or categorical variable — and key surgical outcomes.
Our findings are consistent with the growing body of literature that challenges the notion of advanced age as a contraindication or inherent risk factor for cataract surgery. For instance, Lai et al demonstrated that individuals aged 90 and older achieved significant visual improvement post-surgery, with 79.7% showing enhanced visual acuity, despite a high prevalence of systemic and ocular comorbidities.11 Similarly, Mönestam et al found that 90% of elderly patients (aged 90 and above) gained improvement in BCVA, and Ben-Eli et al found that even patients above 95 years achieved VA improvement.12,13 In contrast, Nussinovitch et al and Rosen et al found poorer outcomes in VA for cataract patients over 90 years of age.4,14 In the elderly, better postoperative visual acuity was associated with improved functional outcomes, including reduced falls and enhanced quality-of-life.15,16
The trend for a higher prevalence of advanced nuclear sclerosis, pseudoexfoliation syndrome, and age-related macular degeneration aligns with prior observations that ocular comorbidities accumulate with age. However, the presence of these conditions does not necessarily translate into increased surgical risk or inferior visual outcomes when managed appropriately. For instance, Mutoh et al demonstrated that even in the presence of such comorbidities, elderly patients undergoing cataract surgery did not experience worse intraoperative outcomes or long-term visual rehabilitation compared to younger individuals.5 Other studies, however, demonstrated that older age correlated with higher surgical challenges and complications such as IFIS and endophthalmitis.4,17
Ong et al reported that while pseudoexfoliation syndrome was associated with a higher risk of certain intraoperative challenges, postoperative visual acuity gains were ultimately comparable to those of patients without pseudoexfoliation.18 These findings reinforce the notion that it is not chronological age per se, but rather the careful preoperative assessment and intraoperative management of age-associated ocular pathology, that determines surgical success. Furthermore, specific preoperative risk factors — not chronological age — should guide surgical risk stratification. For example, Kantan et al demonstrated that pseudoexfoliation syndrome was associated with an increased risk of nuclear cataract and subsequent cataract surgery, independent of age.19 While age may correlate with the prevalence of such risk factors, its independent predictive value appears limited.
Taken together, this study supports a more individualized approach to surgical planning for elderly patients. Rather than using age as a sole criterion for risk, surgeons should rely on a combination of clinical indicators, including lens density, ocular comorbidities, and systemic health. The implication is that with modern surgical techniques and proper perioperative management, cataract surgery can be safely and effectively performed in patients aged above 80 years, without significantly increased risk of complications or having poor visual outcomes. Several limitations of this study should be acknowledged. First, the sample size was relatively small, particularly in the 80 years and above age group, which limits the statistical power to detect small to moderate differences. Second, the retrospective nature of the analysis introduces the possibility of selection bias, as patient inclusion may have been influenced by clinical or demographic factors not fully captured in the dataset. Third, only short-term postoperative outcomes were analyzed, which may not fully reflect long-term visual recovery. In most cases, visual acuity stabilizes after the initial 1–2 weeks. While those having good BCVA at 1-week are very likely to maintain good visual acuity it is not a perfect predictor for cases with subpar visual acuity due to several temporary confounding factors that tend to resolve over the first month, such as corneal edema, inflammation, ocular surface dry eye symptoms. Additionally, the study did not adjust for all potential confounding variables such as surgeon experience or intraoperative complexity scores, which may influence outcomes independently of age. Furthermore, endothelial cell density (ECD) may affect visual outcomes, especially in the short-term. We could not incorporate ECD as a residual confounder in the multivariable analysis. Given the single-center nature of this study, generalizability to broader or more diverse populations may be limited. The findings are most applicable to settings with similar healthcare infrastructure, patient demographics, and surgical protocols. Nevertheless, the results align with studies conducted in comparable clinical environments, supporting their relevance in refining perioperative risk assessment strategies for elderly individuals undergoing cataract surgery.
Conclusion
Cataract surgery in patients aged 80 years and above was not associated with increased intraoperative complications or worse short-term visual outcomes compared to younger patients. Age alone should not be considered a limiting factor; instead, surgical decisions should be based on individual risk profiles. With appropriate care, elderly patients can achieve meaningful surgical results.
Disclosure
The authors have neither proprietary nor commercial interests in any medications or materials discussed in this study. Dr. Tuuminen is a scientific adviser (advisory board, consultant, honoraria) to Alcon Laboratories, Inc., Allergan, Inc., Bayer AG, F. Hoffmann–La Roche, Ltd. and Novartis AG, has received payment for expert testimony (Bayer AG) and has received clinical trial support (study medicines) from Bayer AG and Laboratoires Théa.
References
1. Lin I-H, Lee CY, Chen JT, et al. Predisposing factors for severe complications after cataract surgery: a nationwide population-based study. J Clin Med. 2021;10(15):3336. doi:10.3390/jcm10153336
2. Hecht I, Kanclerz P, Tuuminen R. Secondary outcomes of lens and cataract surgery: more than just “best-corrected visual acuity”. Prog Retin Eye Res. 2023;95:101150. doi:10.1016/j.preteyeres.2022.101150
3. Aaronson A, Viljanen A, Kanclerz P, Grzybowski A, Tuuminen R. Cataract complications study: an analysis of adverse effects among 14,520 eyes in relation to surgical experience. Ann Transl Med. 2020;8(22):1541. doi:10.21037/atm-20-845
4. Nussinovitch H, Tsumi E, Tuuminen R, et al. Cataract surgery in very old patients: a case-control study. J Clin Med. 2021;10(20):4658. doi:10.3390/jcm10204658
5. Mutoh T, Isome S, Matsumoto Y, Chikuda M. Cataract surgery in patients older than 90 years of age. Can J Ophthalmol. 2012;47(2):140–144. doi:10.1016/j.jcjo.2012.01.009
6. Keles A, Sen E, Altas FB, Elgin U. Risk factors for posterior capsule rupture in mature cataract surgery: a study of 1302 cases. Indian J Ophthalmol. 2022;71(1):113–118. doi:10.4103/ijo.IJO_1633_22
7. Robbie SJ, Muhtaseb M, Qureshi K, Bunce C, Xing W, Ionides A. Intraoperative complications of cataract surgery in the very old. Br J Ophthalmol. 2006;90(12):1516–1518. doi:10.1136/bjo.2006.098764
8. Michalska-Małecka K, Nowak M, Gosciniewicz P, et al. Results of cataract surgery in the very elderly population. Clin Interventions Aging;2013. 1041. doi:10.2147/CIA.S44834
9. Chylack LT Jr, Wolfe JK, Singer DM, et al. The lens opacities classification system iii. the longitudinal study of cataract study group. Arch Ophthalmol. 1993;111(6):831–836. doi:10.1001/archopht.1993.01090060119035
10. Mandelblum J, Fischer N, Achiron A, et al. A Simple Pre-Operative Nuclear Classification Score (SPONCS) for grading cataract hardness in clinical studies. J Clin Med. 2020;9(11):3503. doi:10.3390/jcm9113503
11. Lai FHP, Lok JYC, Chow PPC, Young AL. Clinical outcomes of cataract surgery in very elderly adults. J Am Geriatr Soc. 2013;62(1):165–170. doi:10.1111/jgs.12590
12. Mönestam E, Wachmeister L. Impact of cataract surgery on the visual ability of the very old. Am J Ophthalmol. 2004;137(1):145–155. doi:10.1016/S0002-9394(03)00900-0
13. Ben-Eli H, Cnaany Y, Halpert M, Chowers I, Goldstein A. Investigating the impact of age and sex on cataract surgery complications and outcomes. Sci Rep. 2025;15(1). doi:10.1038/s41598-024-84382-4
14. Rosen E, Rubowitz A, Assia EI. Visual outcome following cataract extraction in patients aged 90 years and older. Eye. 2008;23(5):1120–1124. doi:10.1038/eye.2008.203
15. Harwood RH. Falls and health status in elderly women following first eye cataract surgery: a randomised controlled trial. Br J Ophthalmol. 2005;89(1):53–59. doi:10.1136/bjo.2004.049478
16. Gutiérrez-Robledo LM, Villasís-Keever MA, Avila-Avila A, Medina-Campos RH, Castrejón-Pérez RC, García-Peña C. Effect of cataract surgery on frequency of falls among older persons: a systematic review and meta-analysis. J Ophthalmol. 2021;2021:1–7. doi:10.1155/2021/2169571
17. Norregaard JC, Thoning H, Bernth-Petersen P, Andersen TF, Javitt JC, Anderson GF. Risk of endophthalmitis after cataract extraction: results from the international cataract surgery outcomes study. Br J Ophthalmol. 1997;81(2):102–106. doi:10.1136/bjo.81.2.102
18. Ong AY, Shalchi Z. Outcomes of cataract surgery in pseudoexfoliation syndrome in England: 10-year retrospective cohort study. J Cataract Refract Surg. 2021;47(2):165–171. doi:10.1097/j.jcrs.0000000000000397
19. Kanthan GL, Mitchell P, Burlutsky G, Rochtchina E, Wang JJ. Pseudoexfoliation syndrome and the long-term incidence of cataract and cataract surgery: the blue mountains eye study. Am J Ophthalmol. 2013;155(1):83–88.e1. doi:10.1016/j.ajo.2012.07.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.