Back to Journals » Risk Management and Healthcare Policy » Volume 13
Adopting the Triple Aim Framework in the Saudi Healthcare System: A Delphi Study
Authors Al Jasser B, Almoajel A ![]()
Received 23 February 2020
Accepted for publication 12 September 2020
Published 19 October 2020 Volume 2020:13 Pages 2189—2197
DOI https://doi.org/10.2147/RMHP.S251008
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Bandar Al Jasser,1 Alia Almoajel2
1Department of Health Administration, College of Business Administration, Master’s Degree Program in Health and Hospital Administration, King Saud University, Riyadh, Saudi Arabia; 2Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
Correspondence: Alia Almoajel
Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
Tel/ Fax +966 11 8050219
Email [email protected]
Purpose: Helping healthcare systems to optimize performance using particular metrics through objective monitoring will positively impact an organization’s progress toward strategic goals and objectives. The Institute of Healthcare Improvement introduced the Triple Aim framework for guiding new or transforming health systems, concurrently improving population health and patients’ care experience, and reducing per capita cost. Consensus to determine applicable and appropriate measures to monitor this transformation within the scope of the three objectives is required. Thus, the study aimed to adopt the Triple Aim measures and reach a consensus among experts in healthcare systems on the applicability of the measures in the health system of Saudi Arabia.
Methods: A two-round Delphi study was conducted with 17 invited experts who were knowledgeable and experienced in healthcare systems and administration, quality improvement, and strategic planning. These rounds were based on the measures of the three objectives, where they were introduced as statements and grouped under each respective aim. The experts were instructed to score each measure using a 5-point Likert scale and were invited to formulate new measures related to the same aim. Statements reaching a consensus level of 80% were considered applicable measures for the Saudi health system.
Results: A total of 17 measures were circulated among experts; out of which, 16 measures reached a consensus. The 16 measures represent the three main domains of the Triple Aim model, ie, population health, experience of care, and cost per capita. The measure that failed to reach a consensus was the predictive model scores because it requires medical knowledge, where the majority of the experts were non-physicians.
Conclusion: A Delphi study was used to reach consensus among experts on the Triple Aim measures as a first step to building a solid foundation for the population management required to implement these initiatives in the future.
Keywords: Delphi technique, consensus, Triple Aim framework, health system, indicators
Introduction
Helping healthcare systems to optimize performance will exert a positive impact on an organization’s progress toward its strategic goals and objectives using specific metrics to monitor performance objectively. Locally, the Saudi government had set the 2020 transformation plan, which included optimizing the performance of the Saudi health system to achieve its 2030 vision. If the organization readiness for change is high, has the required resources and situational factors are aligned, leaders of these organizations will initiate the change, make tremendous efforts, show the strength of will, and involve in more cooperative role that may lead to efficient and effective future implementation of the Saudi health-care transformational plan with fewer restrictions and less obstacles, specially by engaging the experts as early as possible to a consensus process, ie, Delphi methodology as in this study to build up the transformation plan.1
Currently, decision makers related to the Saudi health system are struggling to ensure improved overall health system quality and patient experience. Therefore, they are required to maintain quality by measuring system performance to improve and sustain quality in healthcare and to ensure patient satisfaction and safety.
In 2008, the Institute of Healthcare Improvement (IHI) developed the Triple Aim model and described it as jointly “improving the individual experience of care, improving the health of populations, and reducing the per capita costs of care for populations”.2 It requires cooperation among healthcare organizations, public health departments, social service entities, school systems, and employers. A governance body or an “integrator” is required to coordinate available resources and support the pursuit of the Triple Aim. The governance body will identify initiatives and projects to support such a pursuit and create a set of high-level measures to monitor progress. These measures should operationally define each dimension of the Triple Aim. When the outcome measures are defined, this will motivate the governors to enhance the learning system to sustain the concurrent improvements of the Triple Aim. This aspect is important for the Saudi new vision in the promotion of effective communication and cooperation across government entities and improvement of healthcare services.
According to Dr. Donald Berwick, president and chief executive officer of the IHI, three preconditions are required, namely, the enrollment of an identified population, a commitment to universality among its members, and the existence of an organization (the “integrator”) that bears the responsibility for the three aims for a particular population. Enrollment of the identified population is carried out by making a meaningful differentiation between the total population and sub-population. The total population is defined as a group of people living within a geopolitical area, whereas a sub-population is defined as groups of people classified according to means or factors, such as income, race/ethnicity, or belonging to a certain heath system. Therefore, specifying the population is necessary especially with the different sub-populations in Saudi Arabia. The second precondition is the commitment to universality, which refers to the policy constraint that maintains balance among the three aims. This precondition is not preset because it is derived from multiple processes of decision making, politics, and contracts with the population involved. For example, if an administrative directorate decided against spending a certain amount of money per year on healthcare, then this decision will lead to constraints on one or two of the three aims. The third precondition, establishing a single entity (ie, the integrator) will link healthcare organizations including public health and social service centers given that their missions overlap across the spectrum of delivery.2
The integrator must possess five components, namely, partnership with individuals and families, redesign of primary care, population health management, financial management, and macro-system integration.2 Partnership with individuals and families occur when all parties are consistently informed about the determinants of their health status and the benefits and limitations of healthcare practices and procedures. A good example is changing an individual’s culture of “the more the better” through transparency, education, effective communication, and shared decision making with patients and families. The second component of the integrator is the redesign of primary care by taking the responsibility for building the required infrastructure and resources to activate shared long-term relationships between the primary care team and patients. In this manner, the shared care plan, available subspecialties, involvement of community resources, and innovative methods of communication, such as personalized health records of patients, will be enhanced. The third component is accountability to efficiently deploy resources by applying segmentation to the served population according to health status, level of support required from families, and socioeconomic status. This component aims to manage population health by increasing preventive efforts toward causes of mortality, such as smoking, violence, and obesity, at the national level and encourage participation in policy making and formulation of programs to prevent the said behaviors. The fourth component is financial management through defining, measuring, and making transparent the per capita cost of care for the defined population. Reducing per capita cost includes intensive efforts to eliminate wastes in all forms, such as non-added value services, rework, errors, and unscientific care. The last component is system integration at the macro-level. In this component, the integrator is required to pursue a contract with an entity that will establish individual health that are evidence-based and highly reliable by providing access to the latest medical knowledge, standardized definitions of quality and cost, and evidence and measurement collected and distributed by a trusted body.
Additionally, organizations and communities should adhere to the following major principles when implementing the Triple Aim. First, the appropriate foundation for population management should be created by identifying the relevant population as described in the abovementioned preconditions. Second, managing services at the population scale, in which the execution of redesigned services and portfolio of projects begins after establishing population management. Third, a learning system should be established to drive and sustain work over time after intentional continuous testing and learning, which will be supplemented with rich feedback loops to enable the leadership to compare performance with the goals and measures for the selected population.3
Success stories were reported of the Triple Aim model and its application in Germany, Canada, Singapore, and the United Kingdom. Such studies showed improvement in population health, experience of care, and reduced per capita cost.4–7 The use of the Triple Aim framework also showed an improvement in health outcomes in many common cases.8
The Saudi Ministry of Health is using the Value-based Healthcare (VBHC) approach to improve the delivery of its healthcare services. However, research illustrated that the Triple Aim framework led to better outcomes. Three main differences are noted between the VBHC and Triple Aim approaches. First, VBHC is a disease-specific chain approach, whereas the Triple Aim is population-based. In other words, people with more complicated health status will rely on fragmented entities to manage their cases under the Triple Aim, which includes treatment plans, financing procedures, and separate locations. Second, VBHC is an example of a linear improvement approach derived from the automotive industry, whereas the Triple Aim approach is based on the circular causality between interventions and outcomes derived from complex adaptive system theory. Instead of single-disease management, which represents the linear improvement approach in this context, the circular (networking) approach, which is similar to best practices worldwide, proved that including primary and secondary care providers into a long-term disease contract to form a unified network will improve the desired results in terms of quality improvement and cost savings. Third, the VBHC concept assumes that a competitive model exists based on outcomes, whereas the Triple Aim is based on a collaborative model for the exchange of products, services, and knowledge. On other hand, the VBHC concept is possible for simple health conditions because of the range of services and manageability of financial risk. However, in terms of vulnerable patients and complicated cases, this will definitely lead to increased fragmentation of care and waste.9
Several studies have used the Delphi technique to gain consensus toward a set of statements. The first round of data collection in the classic Delphi technique includes the creation of qualitative data, which are then used to develop statements for the rounds of questionnaire. A modified Delphi technique, which concludes the qualitative round, can be used in situations where statements are obtained from the literature or previous research, as in the case of the study, which derived its statements from the IHI.10,11
The Delphi study can be conducted on an existing framework to obtain expert consensus on the applicability of the framework in the geographic locations where the initiatives will take place.12
The study aims to primarily adopt the Triple Aim measures by reaching a consensus among experts in healthcare systems on the applicability of such measures in the Saudi health system.
Materials and Methods
The study applied literature study and the Delphi methodology to confirm the applicability of the Triple Aim model in a systematic manner. Evidence- and expert-based knowledge was combined to achieve a clear adoption of the Triple Aim model for the transformation of the Saudi health system.12
A literature review was carried out to determine the applicability of the Triple Aim framework worldwide, the advantages that will exert a positive impact on the Saudi health system, and the aspects that differentiate the framework from other initiatives that have been established in Saudi Arabia. Moreover, the review aims to identify the set of measures that can be shared with experts to obtain consensus.
The IHI selected a set of indicators by measuring new and transforming health systems.11,13 Such indicators were grouped into the following main domains: population health, experience of care, and cost per capita. The researchers’ concern was the applicability of these measures to the context of the Saudi health system. Therefore, the measures were listed in a questionnaire using a 5-point Likert scale (1 = Strongly Agree; 2 = Agree; 3 = Neither Agree nor Disagree; 4 = Disagree, and 5 = Strongly Disagree) to obtain expert agreement.10 For analysis, the 5-point Likert scale was divided into a 3-point scale with 1–2 representing total disagreement, 3 denoting neutral, and 4–5 standing for total agreement, as suggested by other studies.14,15 The reason for this designation is that several responses graded all statements as 4 because the experts agreed that a measure was important with the consideration that “it (a measure) can always get better.” However, others graded a statement 5 when they considered a statement important but “it is either important or not.”
Ethical Considerations
Ethics approval for conducting this study was received from King Abdullah Bin Abdulaziz University Hospital (KAAUH) with IRB log number 20–0230 and IRB registration number with King Abdulaziz City for Science and Technology (KACST) H-01-R-059 in Saudi Arabia. The study was carried out in accordance with the principles of the Declaration of Helsinki.
The researcher send written informed consent through email with the expert’s professional title and full name stating the aim and purpose of this study. They had the opportunity to ask questions and obtain explanations. After giving their written consent in a replying email apporoved and signed by the experts for participation in the study, then the respondents were provided with a questionnaire containing the set of triple aim set of measures.
Study Instruments
According to the nature of the data, approach used, and time availability, the researchers found that two rounds of the Delphi study is the most appropriate instrument to be used within this context. Although the model had never been applied in the Middle East and Arabian Gulf countries, the researchers followed the methodology to obtain the experts’ consensus on the above-mentioned measures and used Google Forms to construct the questionnaires (Appendices 1 and 2).
The questionnaire basically included the set of measures that IHI developed for the Triple Aim framework. “Used with permission. © 2012 Institute for Healthcare Improvement.”
The expert will score each measure using the Likert scale to reflect the extent of agreement to its applicability to the Saudi health system.10
Study Methods
The Delphi study was carried out to improve, complete, and restrict the list of indicators for the transformation of the Saudi health system using a set of measures from the Triple Aim model. The Delphi study is a method that uses expert judgments and compares such judgments through several rounds with the aggregate judgments of other experts until a consensus criterion is reached.10–12,16
The reasons for selecting the Delphi method are as follows. The Delphi technique is generally viewed as cost-effective and has the ability to generate large amounts of data. It is a flexible approach, which enables the data collection from participants who may be geographically separated. Although this type of research tends to be time-consuming, it can be completed in a relatively short time span.13,17
The participants were selected using “purposive or criterion sampling” instead of random sampling,18 because the participants are selected for a purpose, ie, to apply their knowledge or expertise to a certain proposal within the area under investigation. The Delphi technique for data collection does not restrict the sample size; however, eight is acceptable as the minimum number of participants.18,19 The criteria were set as at least 10 or more years of experience and rich knowledge and experience in healthcare systems and administration, quality improvement, and strategic planning.
The experts were holding leadership positions from different types of organizations around the Kingdom. The majority were from eight hospitals, namely, King Abdullah bin Abdulaziz University Hospital, Dr. Faqih Hospital, King Fahad Medical City, Royal Clinics, King Faisal Specialized Hospital in Tabuk, King Fahad Medical City in Taif, Armed Forces Hospital in Dhahran, and Zulfi General Hospital.
Regulators and policy makers were involved as the experts from the Ministry of Health’s Strategic Planning and Management of Information Transformation and Patient Experience. Moreover, an expert from the National Accrediting Body of the Central Board for Accrediting Health Institutions (CBAHI) was employed. Lastly, academic experts were invited to participate from Saudi Universities (ie, King Saud University and Al Marefah University). Table 1 presents the characteristics of the experts.
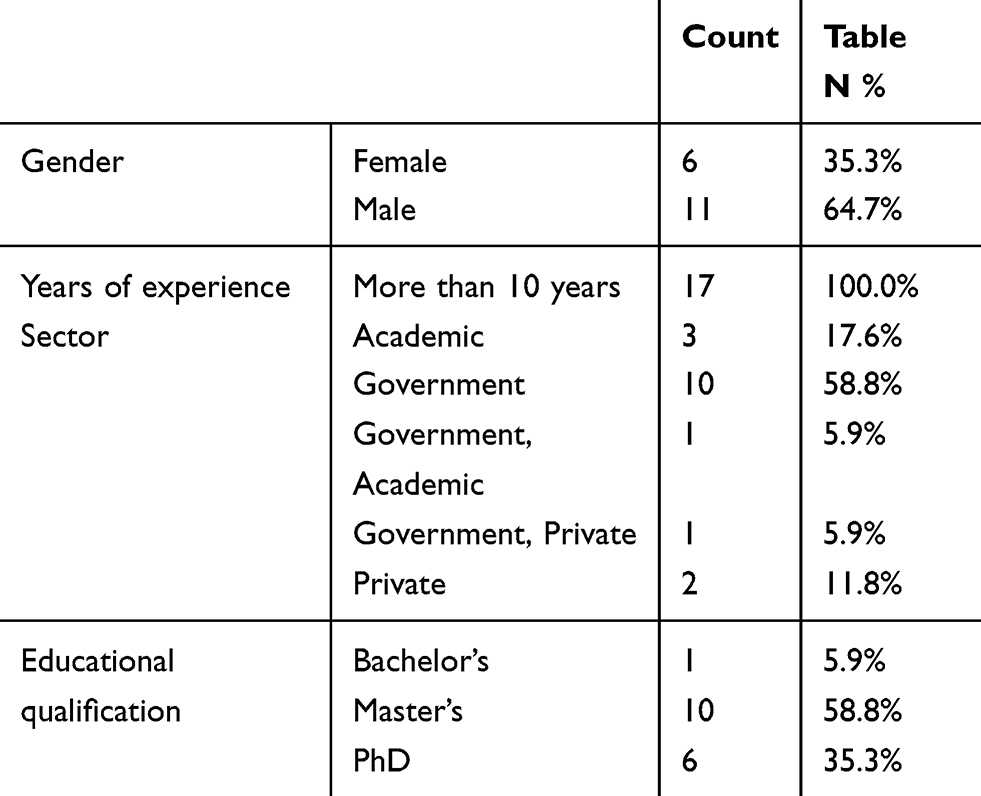 |
Table 1 Experts Characteristics Round |
One of the basic principles of the Delphi method is to employ as many rounds as required to achieve a consensus or until the law of diminishing returns occurs, in which adding more measures will negatively impact the effectiveness of the measurement framework.12,16
The Delphi method requires at least two rounds to allow for feedback and opportunity to receive earlier responses. However, the number of rounds can be disputed. Although no strict guidelines are applied on the correct number of rounds, the number can depend on available time. In this regard, a two-round Delphi study was used to solicit expert opinions about the measures of the Triple Aim model given the short time frame.
The experts were informed about the study and estimated time of commitment via personal contact (phone call or face-to-face).16 During the contact with experts, they were furnished with a guide of the model (ie, purpose, procedures, benefits, timeline, and time involvement for participation) and an online questionnaire with instructions by email or social network applications.
Each round lasted from one to two weeks, starting from the day that the questionnaire was sent to the day feedback was received.
Respondents
First Round
The participants, who agreed to participate over phone call or email, were recruited. Each participant held at least 10 years of experience in the healthcare system and a leadership position in strategic planning or policy making. In the first round, a total of 17 participants actually responded from the list for the first round containing 25 Saudi experts (response rate = 68%). The experts were instructed to score each measure using the using a 5-point Likert scale (Strongly Agree, Agree, Neither Agree nor Disagree, Disagree, and Strongly Disagree) and were invited to add new measures related to the same aim. Round 1 started on May 25, 2019 and the last responses were collected on June 8, 2019.
Second Round
After analyzing the responses from Round 1, minor modifications were made to 13 statements to improve clarity based on the participants’ comments (n = 13). The measures that reached experts’ consensus scored 80% and above in Round 1 and the modified statements, in which the experts failed to reach a consensus, were reintroduced in Round 2 with clearer definitions and examples on June 16, 2019. The previous responses for Round 1 were sent with the Round 2 questionnaire to allow them to consider their previous answers and provide responses for Round 2 to ensure better clarity and understanding. All experts provided responses for Round 2 with a response rate of 100%. The last responses were received on June 30, 2019.
Scale of Measurement
The following measurements were used to quantify the variables in the study. Nominal — basically classifies variables in terms of their names, and categories cannot be ranked. Ordinal — contains non-numeric categories than can be ranked, such as “Strongly Agree” and “Agree,” which take a value of “3,” “Neither agree nor disagree,” which takes a value of “2”, and “Disagree” and “Strongly disagree,” which take a value of “1,” as shown in Table 2.
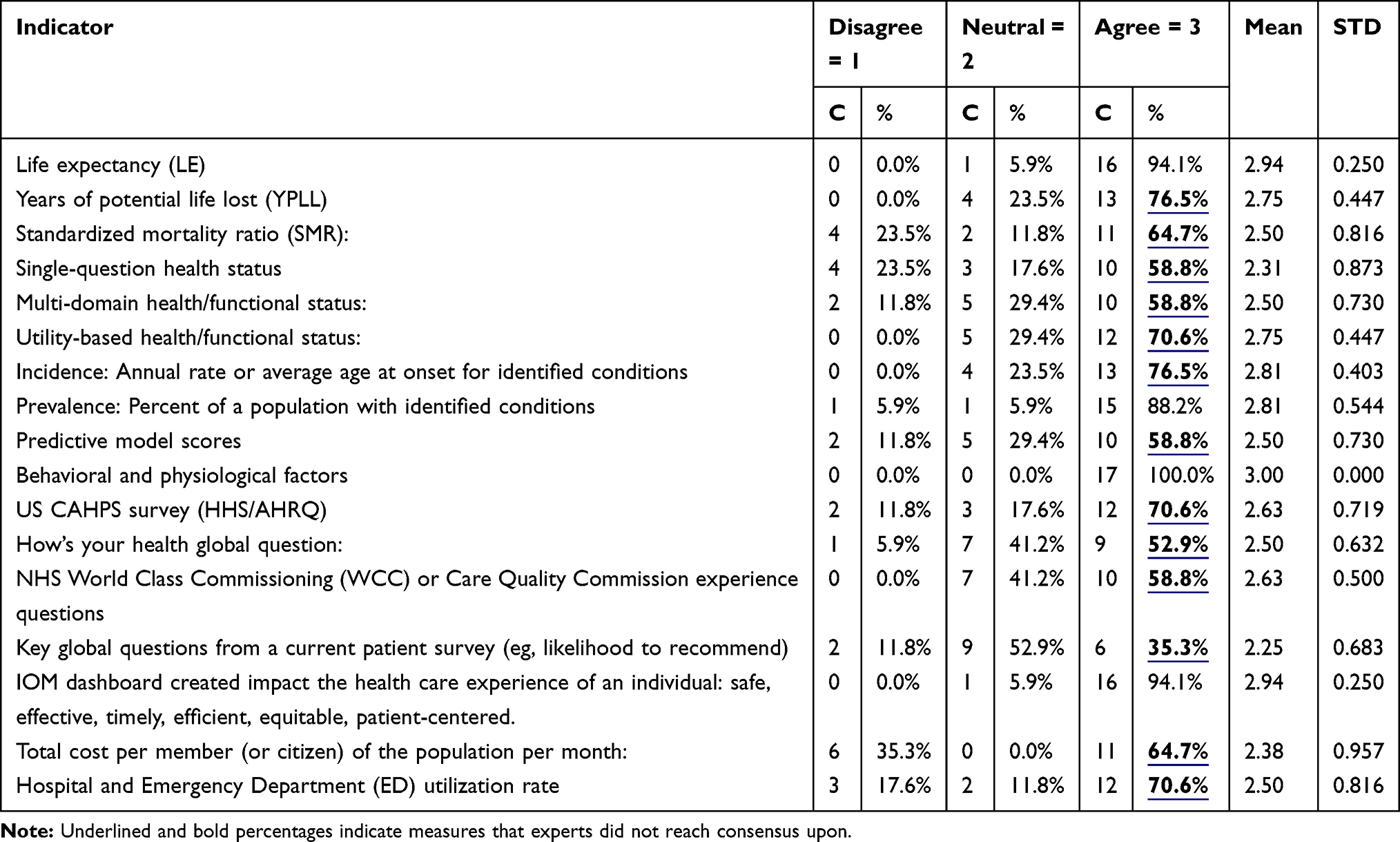 |
Table 2 Round One Measures Which Did Not Reach Experts Consensus |
Results
Data Analysis
Data analysis of the Delphi survey involved statistical methods and content analysis. IBM SPSS Version 25 was used for all quantitative analysis. Descriptive statistics were used to describe each item, including mean, and standard deviation; the reliability of the Delphi method was tested by expert opinion consensus and calculating the Cronbach’s alpha.
First Round
In the first round, the reliability test was carried with Cronbach’s alpha = 0.72. The survey comprises all indicators listed in the Triple Aim guide (n = 17) (sourced from www.IHI.org with permission of the Institute for Healthcare Improvement, ©2020).
The experts agreed on 4 out of 17 measures and reached a consensus. Additionally, two experts added 14 measures that should be considered to achieve the desired outcomes of the respective domain.
This misunderstanding was resolved in Round 2 because all measures that the experts suggested in Round 1 have been included in the questionnaire but were unclear to the experts. For example, one of the experts suggested to monitor the timely triage process in the emergency department. However, this measure has been listed under the six dimensions provided by the Institute of Medicine (IOM), specifically the time dimension. Minor issues were observed in terms of the clarity of the measures in Round 1. Therefore, a consensus level of 80% in the first round was considered very low. The major issue with clarity (all listed measures of the Triple Aim framework including the set of measures), is that the experts only needed to review the material in depth to identify the included measures. Therefore, the researchers provide examples and appropriate definitions of such measures.
Analysis on the measures was carried out by calculating the mean and standard deviation of each measure to quantify a central tendency (mean) and dispersion level (standard deviation; SD), as shown in Table 2.
Second Round
The researchers rephrased the statements that did not reach a consensus level of 80%, which the experts suggested were unclear, with properly referenced definitions and accompanied by real-life examples. In Round 2, 16 out of 17 measures reached a consensus level of 80% with mean scores ranging between 2.82 and 3.00 and standard deviation scores ranging between 0.000 and 0.529. The only measure that did not reach the consensus level was the predicative model measures with mean = 2.56 and SD = 0.493. The reason was that this measure is a purely medical measure and, despite a clear definition, it was difficult to be understood by experts who are not physicians (Table 3).
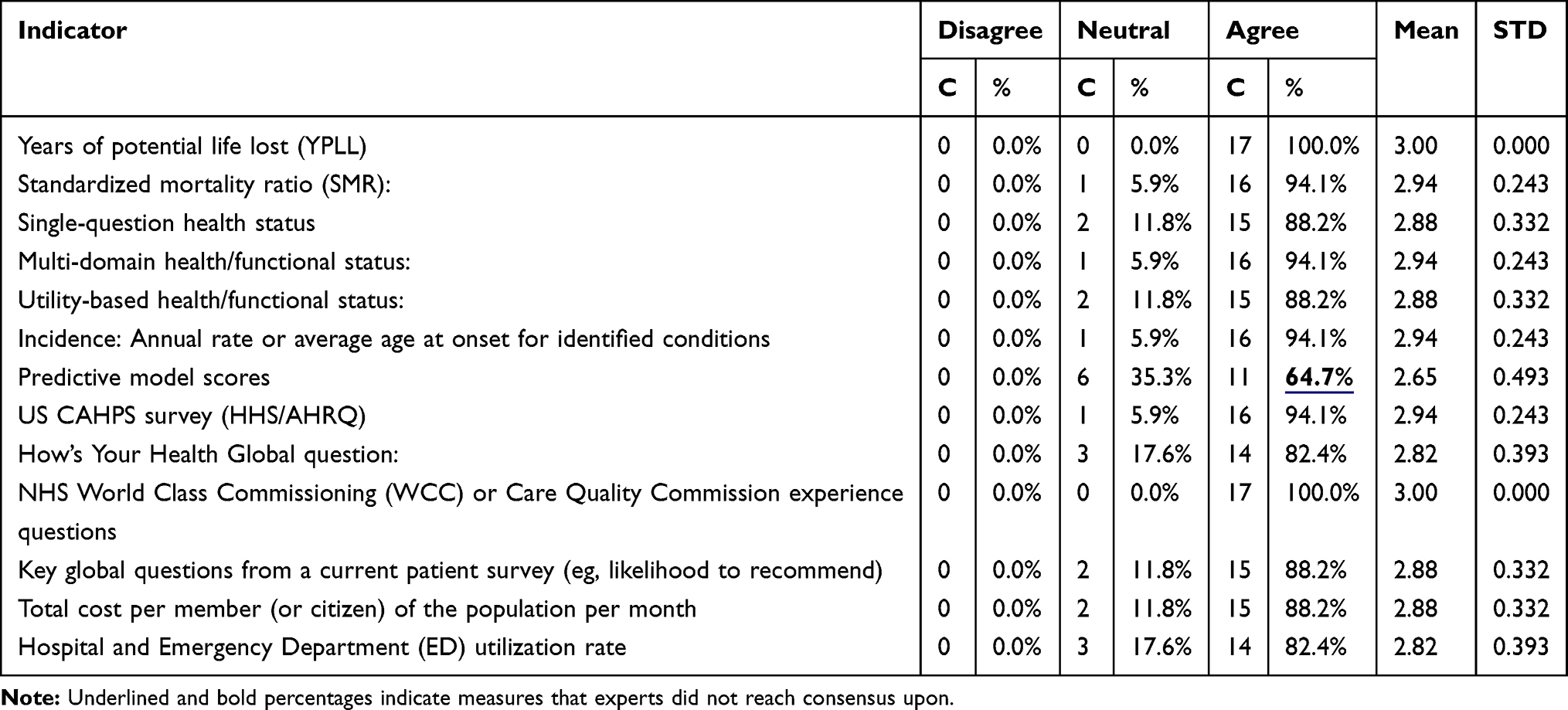 |
Table 3 Round Two Measures Which Did Not Reach Experts Consensus |
The final set of measures collected after the experts’ consensus reached 80% and above (Table 4).
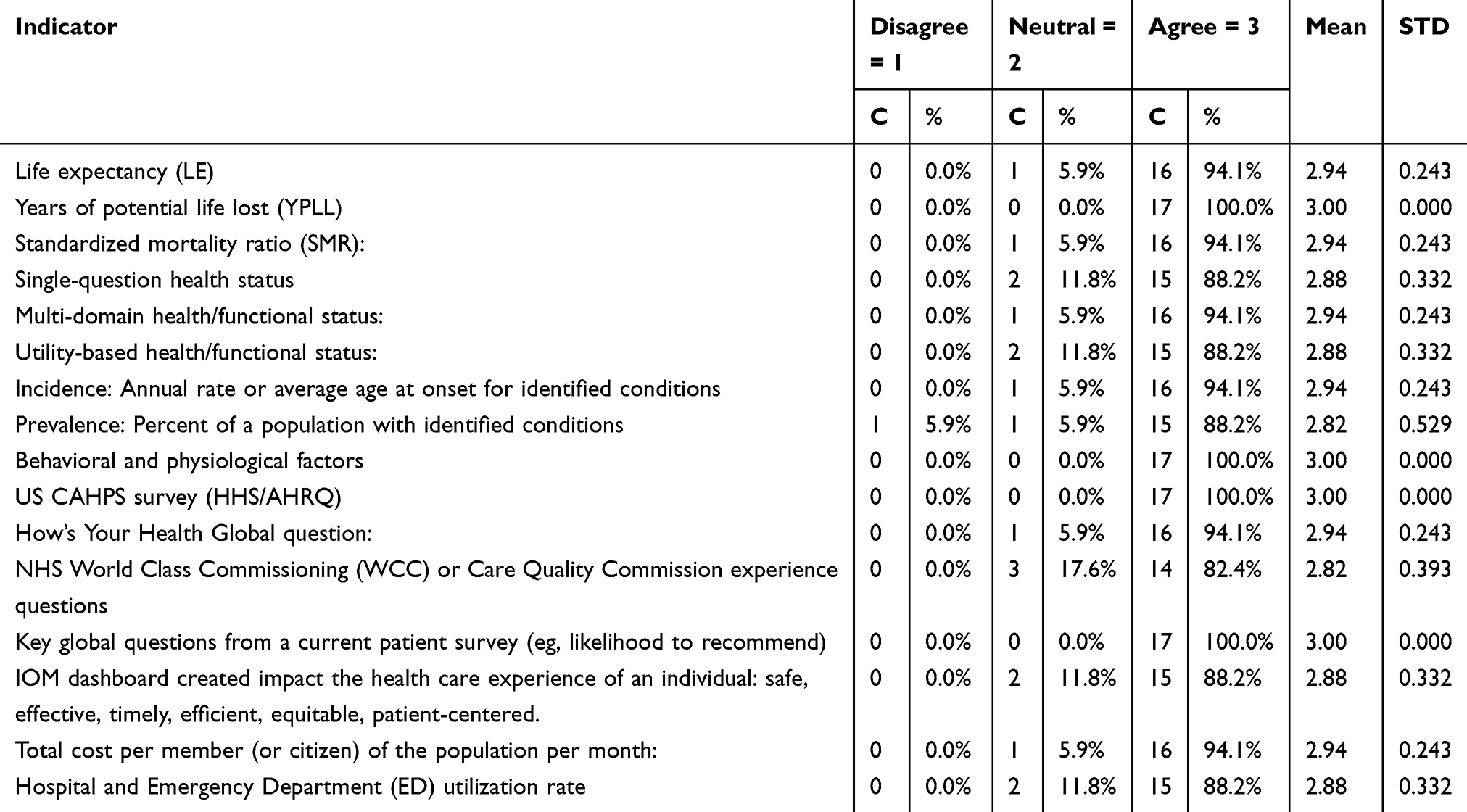 |
Table 4 The Final Set of Measures Reached Consensus by the Experts |
Discussion
This study aimed to adopt the Triple Aim model measures and reach a consensus among the experts in healthcare system on the applicability of the said measures in the context of the Saudi health system. After analysis of Round 2, a total of 16 measures reached the experts’ consensus, whereas one remaining measure is purely medical and only physicians may agree on such measure. The study illustrated that the Triple Aim model is highly applicable to different systems worldwide, which is in agreement with other studies in other countries, such as Germany and Canada.
The study faced certain challenges in terms of the clarity of the statements as perceived by the panel of experts and as explained in the previous example of timely emergency triage, which required a full explanation and clear definitions with examples of the measures. Another challenge is the time constraint against expert availability to provide responses in multiple rounds.
The advantages of the study are as follows. Responses were collected from experts from different geographical areas, specialties, and organizations in a timely manner, which is considered a big success. In addition, the Delphi approach enhanced the experts’ freedom of opinion and eliminated other effects that may induce bias or be influenced by personal judgment. Moreover, the agreement will increase the buy-in of all experts to participate and lead future transformational efforts in accordance with the Triple Aim framework of the IHI.
The limitation of this study as it was intended to include the more participants but due to their busy schedules and commitments they apologized to participate, although their participation will add more value to the study and any future study aiming to support these results should employ a larger sample.
In Canada, nine healthcare organizations have adopted the Triple Aim model, which resulted in better health for the population, improved experience of patient care, and lower costs of the system. However, such organizations noted certain difficulties in implementation. For instance, delivering the Triple Aim framework required strong governance support and leadership, as well as involvement from non-healthcare sectors, to optimize the outcomes.5
The German healthcare system found the Triple Aim framework useful for achieving the three objectives and suggested that longitudinal studies should be conducted to validate results and acquire a thorough analysis of the specific effects of the subcomponents of the general intervention.4
Conclusion
The Triple Aim framework is highly applicable across systems but requires clear operational definitions of its measures before adoption. Consideration of the three main components for execution (appropriate foundation of population management, scale management, and establishment of a learning system) will increase the chance of success.
In the current study, one measure did not reach the consensus of the experts because it was purely medical and related to comparisons of predictive model scores that can be made over time by standardizing the use of the initial population size in different risk categories (eg, healthy, at risk, uncomplicated chronic, and complex) as shown in the results. Table 5 displays the measures of the adopted framework. The researchers conclude that the Triple Aim model is applicable for the Saudi health system according to expert agreement on the applicability of such measures under the Triple Aim framework.
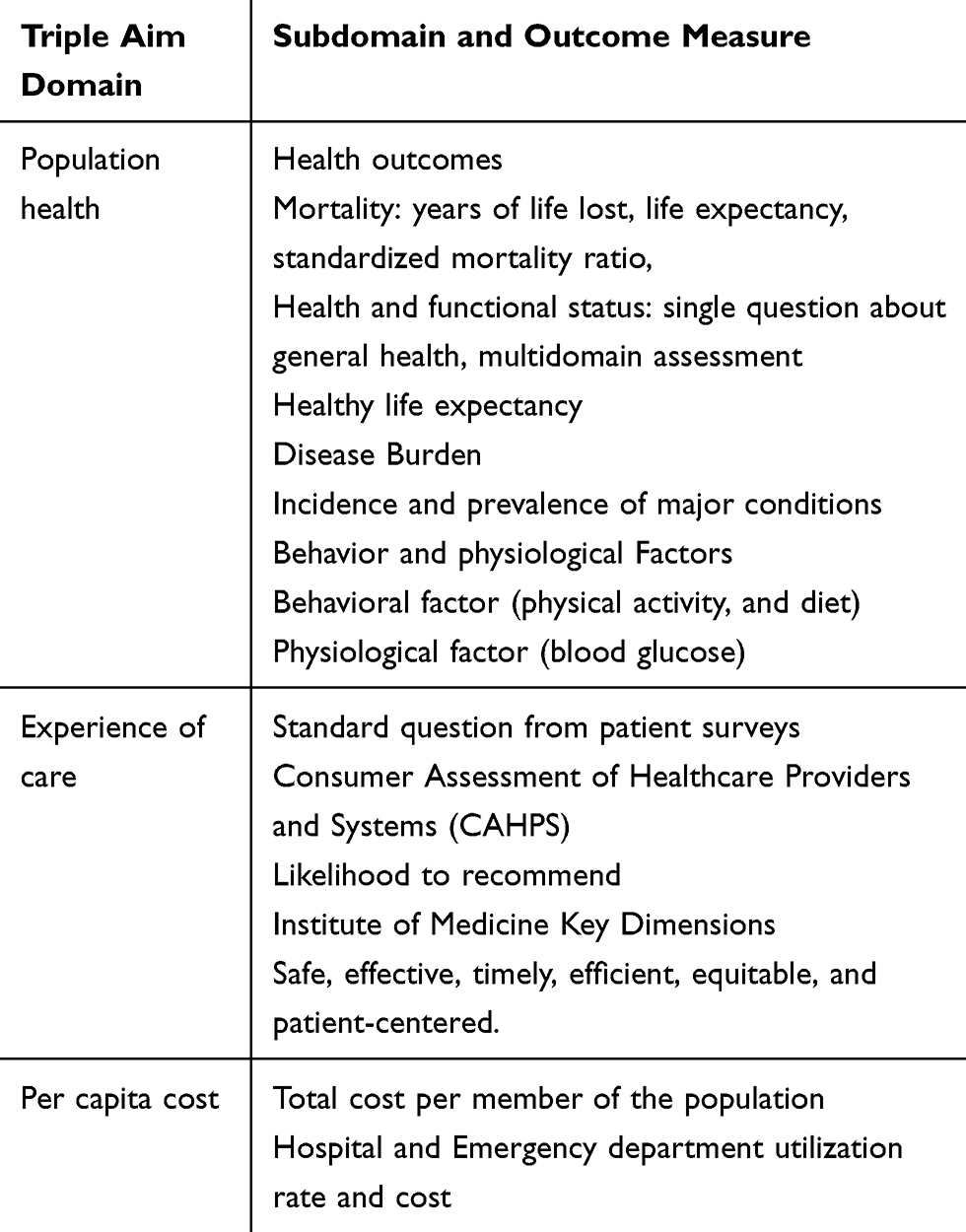 |
Table 5 Adopted Framework’s Measures |
Acknowledgments
The Authors acknowledges the support provided by the Deanship of Scientific Research through the Research Center in the College of Applied Medical Sciences at King Saud University. Also, the authors thank the Deanship of Scientific Research and RSSU at King Saud University for their technical support. In addition, the authors express appreciation for the experts who participated in the Delphi rounds.
Funding
The authors acknowledge the financial support provided by the Deanship of Scientific Research through the Research Center in the College of Applies Medical Sciences at King Saud University.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Alharbi MF. An analysis of the Saudi health-care system’s readiness to change in the context of the Saudi National Health-care Plan in Vision 2030. Int J Health Sci. 2018;12(3):83–87.
2. Berwick DM, Nolan TW, Whittington J. The triple aim: care, health, and cost. Health Aff. 2008;27(3):759–769. doi:10.1377/hlthaff.27.3.759
3. Whittington JW, Nolan K, Lewis N, et al. Pursuing the triple aim: the first 7 years. Milbank Q. 2015;93(2):263–300. doi:10.1111/1468-0009.12122
4. Hildebrandt H, Schulte T, Stunder B. Triple aim in Kinzigtal, Germany: improving population health, integrating health care and reducing costs of care – lessons for the UK? J Integrated Care. 2012;20(4):205–222. doi:10.1108/14769011211255249
5. Farmanova E, Kirvan C, Verma J, et al. Triple Aim in Canada: developing capacity to lead to better health, care and cost. Int J Qual Health Care. 2017;28(6):830–837.
6. Cheah J, Wong LM, Pang HL. Integrate now, create health: perspectives from Singapore. Int J Integr Care. 2010;10(p):e044–e044. doi:10.5334/ijic.533
7. McCarthy D, Klein S. The Triple Aim Journey: Improving Population Health and Patients’ Experience of Care, While Reducing Costs. 2010.
8. Agrawal S, Conway PH. Aligning emergency care with the triple aim: opportunities and future directions after healthcare reform. Healthcare. 2014;2(3):184–189. doi:10.1016/j.hjdsi.2014.05.005
9. Valentijn PP. The 3 differences between Value Based Healthcare and Triple Aim that you need to know. 2018, June 5; Available from: https://www.essenburgh.com/en/blog/the-3-differences-between-value-based-healthcare-and-triple-aim-that-you-need-to-know. Accessed October 11, 2020.
10. Rådestad M, Jirwe M, Castrén M, et al. Essential key indicators for disaster medical response suggested to be included in a national uniform protocol for documentation of major incidents: a Delphi study. Scand J Trauma Resusc Emerg Med. 2013;21(1):68. doi:10.1186/1757-7241-21-68
11. Stewart D, Gibson-Smith K, MacLure K, et al. A modified Delphi study to determine the level of consensus across the European Union on the structures, processes and desired outcomes of the management of polypharmacy in older people. PLoS One. 2017;12(11):e0188348. doi:10.1371/journal.pone.0188348
12. Gallotta B, Arturo Garza-Reyes J, Anosike A. Using the Delphi Method to Verify a Framework to Implement Sustainability Initiatives. 2018.
13. Stiefel M, C NK. A Guide to Measuring the Triple Aim: Population Health, Experience of Care, and per Capita Cost.IHI Innovation Series White Paper. Massachusetts: Institute for Healthcare Improvement;2012. Available from: www.IHI.org. Accessed October 11, 2020.
14. Jirwe M, Gerrish K, Keeney S, et al. Identifying the core components of cultural competence: findings from a Delphi study. J Clin Nurs. 2009;18(18):2622–2634. doi:10.1111/j.1365-2702.2008.02734.x
15. Mcilfatrick SJ, Keeney S. Identifying cancer nursing research priorities using the Delphi technique. J Adv Nurs. 2003;42(6):629–636. doi:10.1046/j.1365-2648.2003.02666.x
16. McKenna HP. The Delphi technique: a worthwhile research approach for nursing? J Adv Nurs. 1994;19(6):1221–1225. doi:10.1111/j.1365-2648.1994.tb01207.x
17. Donohoe H, Stellefson M, Tennant B. Advantages and limitations of the e-Delphi technique. Am J Health Educ. 2012;43(1):38–46. doi:10.1080/19325037.2012.10599216
18. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32(4):1008–1015.
19. Hallowell MR, Gambatese JA. Qualitative research: application of the delphi method to CEM research. J Constr Eng Manag. 2010;136(1):99–107.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.