Back to Journals » Clinical Ophthalmology » Volume 15
Adjunctive Green Thermal Laser Photocoagulation for Treatment of Resistant Infectious Keratitis
Authors Nasef MH ![]() , El Emam SY
, El Emam SY ![]() , Sharaf AF, Allam WA
, Sharaf AF, Allam WA
Received 26 March 2021
Accepted for publication 2 June 2021
Published 14 June 2021 Volume 2021:15 Pages 2447—2453
DOI https://doi.org/10.2147/OPTH.S312674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Mohamed H Nasef, Sharif Y El Emam, Amr F Sharaf, Waleed A Allam
Ophthalmology Department, Faculty of Medicine, Tanta University, Tanta, Egypt
Correspondence: Mohamed H Nasef
Ophthalmology Department, Faculty of Medicine, Tanta University, Tanta, Egypt
Tel +201002826555
Email [email protected]
Purpose: To investigate the safety and efficacy of green thermal laser as an adjunctive therapy for the treatment of resistant infectious keratitis (IK) in the Delta region of Egypt.
Methods: A retrospective case series of 150 patients, within a 4 year duration, with resistant IK, who failed to respond to specific medical treatment alone for 7 days, were included. They all received green thermal laser photocoagulation treatment to the cornea as an adjunctive to medical treatment.
Results: Forty-eight women and 102 men were included in this study with a mean age of 46.2 ± 7.7 years. Common risk factors associated with IK included trauma by material of plant origin and contact lens wear. The mean duration of healing was 2.87 ± 0.7 weeks. A single session of green thermal laser application was adequate in 138 IK cases (92%), while 12 cases (8%) required an additional session a week later. Supplementary amniotic membrane transplantation (AMT) was required in 26 cases (17.3%). Two patients (1.3%) required tectonic keratoplasty for corneal perforation. The final corrected distance visual acuity (CDVA) was counting fingers (CF) or better in 78 patients (52%). No decrease of CDVA was reported throughout the study.
Conclusion: Green thermal laser is a safe and effective adjunctive therapy for the treatment of resistant infectious keratitis.
Keywords: laser, resistant keratitis, infectious keratitis, cornea
Introduction
Infectious keratitis (IK) is a potentially sight-threatening condition.1,2 The reported incidence greatly varies, according to the geographic location, ranging between 2.5–799 cases per 100,000 population/year.3–5 It has been previously recognized as a “silent epidemic” in the developing world,6 and recently, it has been suggested to add it to the list of neglected tropical diseases (NTD) in Ophthalmology.7 Rapid accurate diagnosis and immediate, adequate treatment are mandatory for achieving good clinical outcomes.8,9
IK can be caused by a wide variety of microorganisms, including bacteria, fungi, viruses, and parasites.10,11 The evolution of drug-resistant and high virulence organisms has become the leading cause for the occurrence of resistant IK.12 Other causes of IK include irrational use of antimicrobial therapy, limited corneal penetration of some agents, toxicity from topical preservatives, corneal disorders such as neurotrophic and exposure keratopathies, and systemic diseases such as diabetes mellitus and immunodeficiency disorders.13,14 In such cases, complications such as corneal melting, perforation, and endophthalmitis are more likely to occur despite the appropriate topical antimicrobial therapy.
These issues highlight the need for novel modalities of adjunctive therapy to supplement the standard topical antimicrobial treatment. Such modalities, used separately or in conjunction, include therapeutic corneal tissue debridement,15 amniotic membrane transplantation (AMT),16,17 subconjunctival18 and intrastromal anti-microbial injections.18,19
Photo-Activated Chromophore for Keratitis-Corneal Cross-Linking (PACK-CXL) has also been described, and is based on the antimicrobial activity of the UV light, which can directly damage the DNA and RNA of various types of microorganisms.1,20 Furthermore, photoactivated riboflavin releases reactive oxygen species which can directly affect the DNA and cell membranes of organisms.21
Another recent adjuvant modality is green thermal laser application.22 Green thermal laser has been widely used for the management of retinal diseases. It is absorbed by tissue pigments, with subsequent production of thermal damage to the target tissues due to induced temperature that rises well over 90°C.23 The use of thermal laser in corneal pathologies, such as neovascularization, has been described almost 50 years ago.24 A few recent studies have already documented the efficacy of green thermal laser as an adjunctive therapy for the management of resistant IK.22,25
In the current study, we investigated the safety and efficacy of adjunctive green thermal laser treatment for cases of resistant IK.
Patients and Methods
This retrospective study was carried out at the cornea division of the Tanta University Ophthalmology Hospital in Tanta, Egypt, a tertiary referral center, in the center of the delta region. The approval by the Institutional Review Board (IRB) and Human Research Ethics Committee at Tanta University, Faculty of Medicine, were obtained, and the study was carried out in adherence to the tenets of the Declaration of Helsinki. The patients’ data confidentiality was maintained, and all patients signed an informed consent after a full explanation of the condition and the treatment options. Similarly, the nature of the procedure and its potential complications were explained to all participants.
The medical records of patients treated at the cornea unit were reviewed, and 150 eyes of 150 patients with resistant infected corneal ulcers were included, during a 4 year period, between June 1, 2016 and May 30, 2020. We considered the infectious keratitis to be “resistant” when no signs of improvement were seen after applying the specific treatment, based on the culture and sensitivity results, for 7 days. Signs of improvement were the reduction of the density of corneal infiltration, surrounding corneal edema, hypopyon level, and epithelial defect.
Patients who were uncooperative, those with uncontrolled autoimmune or collagen diseases, those with marked corneal thinning, descemetoceles, or stromal infiltration involving more of 50% of the corneal thickness were excluded. Additionally, patients with non-infectious keratitis were excluded. A routine B scan ultrasonography was done to exclude posterior segment involvement. All the included patients received green thermal laser to the cornea as an adjunctive therapy following the initial 7 days, in which they received specific antimicrobial therapy.
At presentation, a full history was taken. Any associated risk factors such as contact lens wear and corneal trauma, especially by material of organic origin, were noted. Systemic disease affecting the corneal condition were noted. Detailed external ophthalmological examination, and laboratory investigations were performed.
Slit-lamp examination was performed. The size of the epithelial defect in both the horizontal and vertical meridians was documented (in millimeters), and averaged. The density and depth of infiltration, the surrounding corneal edema, anterior chamber reaction, and level of hypopyon were also documented. Colored slit-lamp photographs were captured for all cases, at baseline, and on follow-up visits.
Patients who were receiving any form of topical antimicrobial therapy prior to presentation were asked to stop their medications for 24 hours before corneal scraping. Scraping was then performed, after the instillation of a topical anesthetic agent, using either a heat-sterilized Kimura spatula or a sterile #15, in the operating room under sterile conditions. Epithelial debridement was not performed. The obtained specimens were subjected to both microscopic examination, and microbiological culture and sensitivity testing. The microscopic examination included fresh smear examination using potassium hydroxide (KOH) and Gram-staining. The scrapings were inoculated directly onto multiple culture media, such as blood agar, chocolate agar, Sabouraud dextrose agar, thioglycollate broth, and non-nutrient Escherichia coli agar. Suspected contact lenses and their solutions were cultured in the same way.
After obtaining the specimens, treatment was prescribed based on the clinical suspicion. Patients with the clinical diagnosis of bacterial corneal ulcers received topical moxifloxacin hydrochloride 0.5% eye drops (Vigamox®, Alcon Laboratories, Inc., Fort Worth, TX, USA) every 2 hours, while those with suspected fungal keratitis received topical fluconazole 0.2% eye drops (Diflucan®, Pfizer Inc., New York, NY, USA) hourly. After obtaining culture and sensitivity results, this initial treatment regimen was modified accordingly. All patients received supportive therapy in the form of topical cyclopentolate hydrochloride 1% eye drops (Cicloplejico®, Alcon Cusi, Barcelona, Spain), preservative-free lubricating eye drops, oral tetracycline, and vitamin C. Topical anti-glaucoma eye drops were prescribed if needed, per case.
Cases that fail to show initial improvement after one week of specific therapy, according to culture and sensitivity results, were considered resistant and included in the study. However, cases with marked corneal thinning were excluded to avoid laser-induced corneal micro-perforations.
After administration of topical benoxinate hydrochloride 0.4% eye drops (Benox®, EIPICO, Cairo, Egypt), a sterile 1 mg fluorescein sodium strip (Bio Glo™, HUB Pharmaceuticals, LLC, Rancho Cucamonga, CA, USA) was used to stain the epithelial defect. A speculum was used to help with opening the patients’ eyes, with frequent instillation of topical anesthetic drops. Stained corneal tissue was then exposed to a 532 nm frequency doubled diode-pumped solid state green laser treatment (Visulas® 532s, Carl Zeiss Meditec AG., Jena, Germany), focused on the anterior corneal surface. The laser parameters used were set to a 500 μm spot size, duration of 200 milliseconds, and the power was adjusted between 900 −1200 mW. The number of shots applied differed from one patient to another, and aimed to produce light charred burns with small cavitations over the treated area. The total area of epithelial defect was covered with confluent laser burns performed in one session. All patients were kept on the same medical treatment prescribed prior to laser therapy. Pain medications were administered when needed.
If a noticeable response was not obtained after 7 days, with persistence of the epithelial defect, a second session of laser photocoagulation was applied in the same manner, and using the same parameters.
All patients were checked daily during the first week after the procedure, then every three days till healing (complete re-epithelialization with resolution of the inflammatory signs). After complete epithelial healing, a weak steroid (fluorometholone 0.1%, FML®, EIPICO, Cairo, Egypt) was added twice daily to minimize scarring. Additional follow-up visits, up to 3 months, were scheduled when needed.
Analyses were performed by SPSS statistics for Windows, version 23.0 (IBM Corp., Armonk, NY). Quantitative data were expressed as mean ± standard deviation (SD).
Results
A total of 163 records of patients with resistant infectious keratitis were assessed for study eligibility, of which 13 were excluded for incomplete data. The study included 150 eyes of 150 patients treated at Tanta University Ophthalmology Hospital between June 1, 2016 and May 30, 2020. The study included 48 women (32%) and 102 men (68%), with a mean age of 46.2 ± 7.7 years (35–65 years). Trauma with material of organic origin (99 patients, 66%) and contact lens wear (33 patients, 22%) were the most commonly associated risk factors. Some of the other risk factors were uncontrolled diabetes mellitus, exposure keratopathy, trichiasis and entropion.
All patients presented with pain and rapid drop of vision. Out of the 150 included patients, 127 (84%) had already received one or more topical anti-microbial agent prior to presentation to our hospital. The mean diameter of ulcers was 4.33 ± 1.3 mm (3.0 to 7.0 mm) in the horizontal meridian, and 4.38 ± 0.85 mm (3.0–6.0 mm) in the vertical meridian. A hypopyon level was present in 103 cases (68.6%), and ranged in height between 1.0 and 4.0 mm, with a mean of 2.36 ± 1.0 mm (Figure 1A and D). Microbiological work-up revealed mixed bacterial and fungal infections in 71 cases (47.3%). Pure fungal and bacterial etiology in 44 (29.3%) and 35 (23.3%) cases, respectively (Table 1).
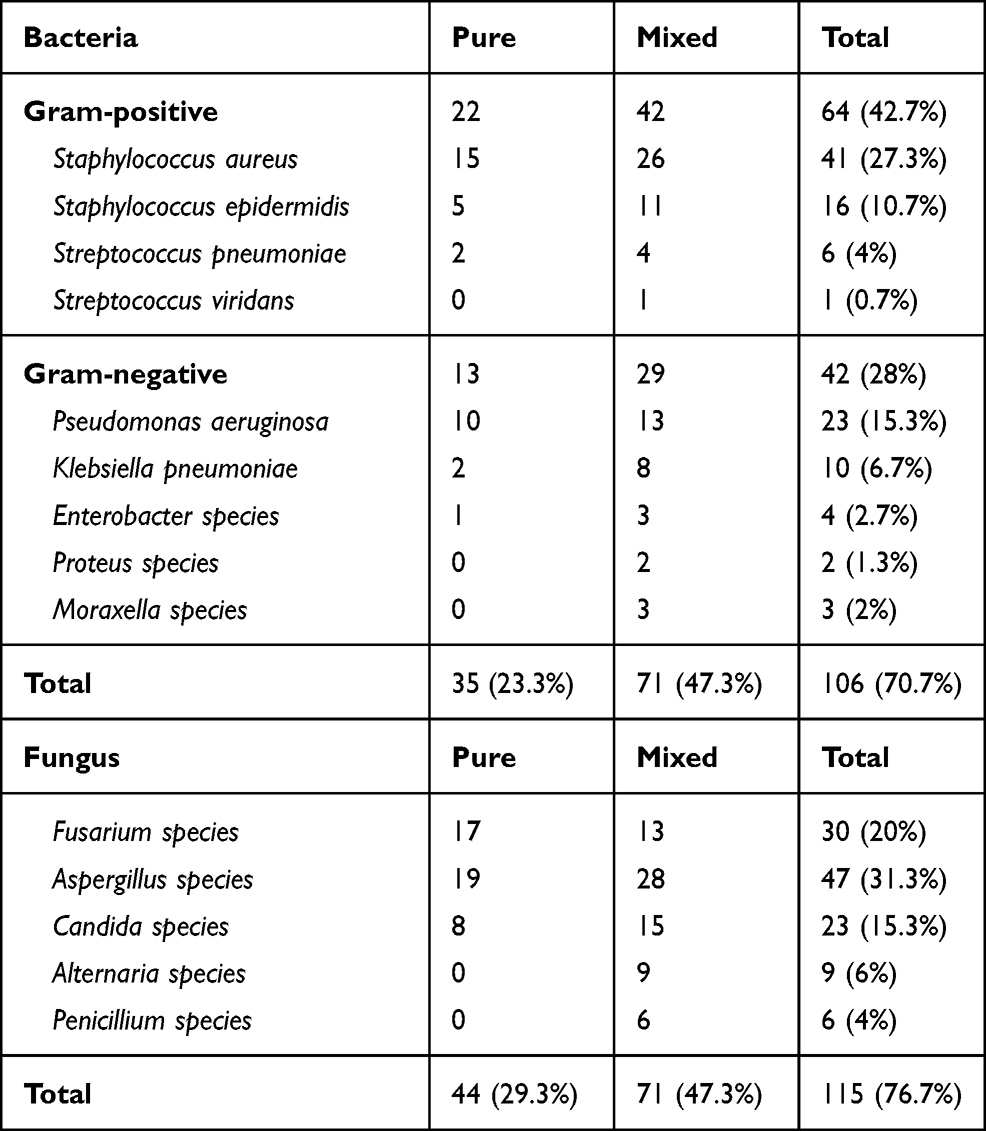 |
Table 1 Epidemiology of Microorganisms Found in Infectious Keratitis Cases |
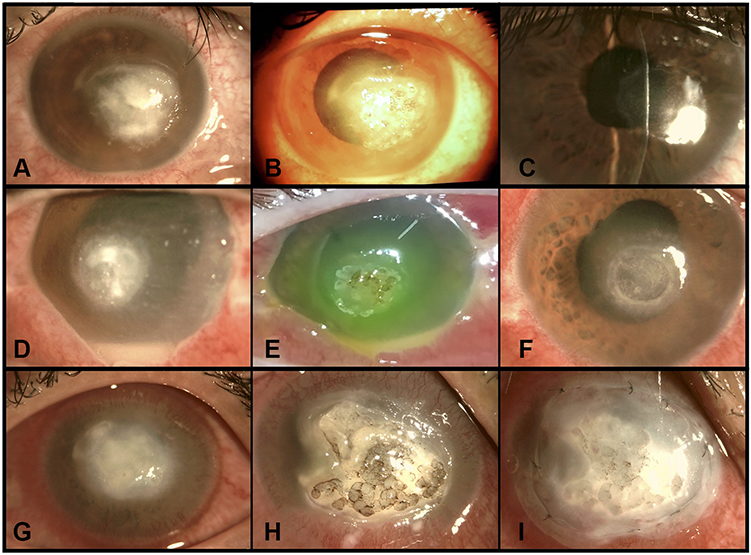 |
Figure 1 3 examples of green thermal laser application for resistant infectious keratitis (IK). Case 1 (A–C) had a bacterial IK, with a 1 mm height hypopyon level. Pre-treatment (A), post-laser (B), and after complete healing (C). Case 2 (D–F) had a fungal IK, with a 3 mm hypopyon level. Pre-treatment (D), immediately post-laser with stained cornea (E), and after complete healing (F), with residual corneal opacity. Case 3 (G–I) had mixed bacterial and fungal dense central infiltration with a flat anterior chamber (G), Post-laser (H), and after amniotic membrane transplantation (I). |
The total number of laser shots applied per session (in the 162 sessions performed) ranged from 28 to 350 pulses (178 ± 66), based on the device counter, including the missed shots due to sudden eye movements (Figure 1B, E and H). Signs of initial improvement, in the form of gradual regression of inflammatory signs and fading of corneal infiltrates, were observed in 138 patients (92%) during the first week after the procedure. Such response was not obtained in 12 cases (8%), hence, they required an additional laser session a week later, followed by amniotic membrane transplantation (AMT). Out of 150 participants, 26 (17.3%) required AMT (Figure 1G and I). The indications for AMT included laser-induced corneal micro-perforations in 3 cases (2%), progressive corneal thinning (over 50% of thickness) in 11 cases (7.3%), and as a supplementary therapy in the 12 cases who received a second “additional” laser session (8%). Tectonic corneal grafts were required in 2 cases (1.3%) due to uncontrolled inflammation with subsequent corneal macro-perforation.
Healing and complete re-epithelialization was achieved in 123 cases (82%) with the laser used as the sole adjunctive therapy (Figure 1C and F), and in 100% with the use of other adjunctive modalities. This occurred within 2.87 ± 0.7 weeks (2–6 weeks) following the laser application, with a majority (77 cases, 51.3%) within the first 2 weeks (Figure 2). No recurrences were recorded during the entire study period.
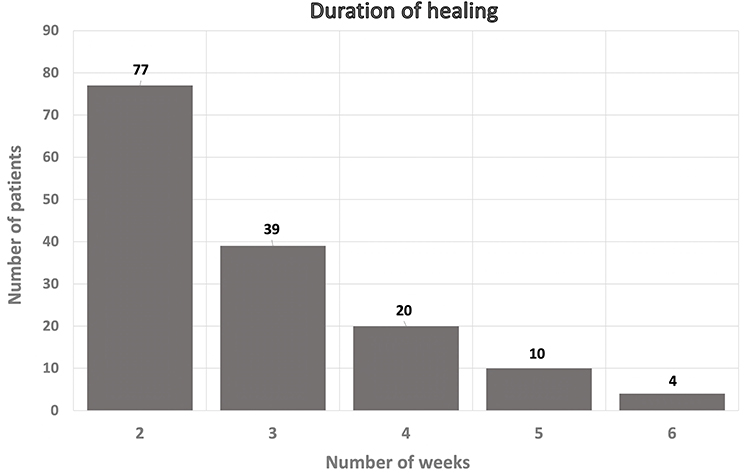 |
Figure 2 Duration till complete healing and full resolution of inflammatory signs after laser application, ranging between 2–6 weeks. The majority of cases had complete healing within the first 2 weeks (77 cases, 51.3%). |
At presentation, 112 (74.6%) patients had visual acuity of hand movement (HM), 15 (10%) patients had only light perception (LP), while 23 (15.3%) patients had acuity better than HM. After complete healing, 78 patients (52%) achieved corrected distance visual acuity (CDVA) of counting fingers (CF) or better, while 72 patients (48%) maintained their baseline vision. Loss of CDVA was not reported throughout the study (Figure 3).
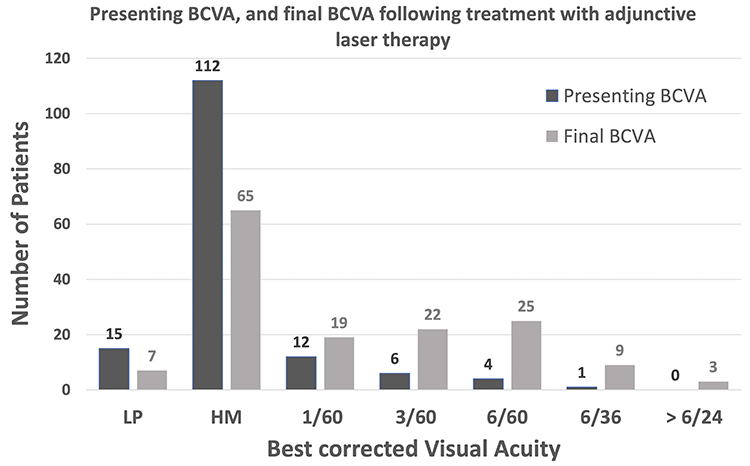 |
Figure 3 Presenting and final corrected distance visual acuity (CDVA) after adjunctive laser therapy. Before starting the treatment, 127 (84.6%) cases had a CDVA of hand movement (HM), or light perception (LP). After complete healing 78 (52%) of cases had a CDVA better than HM. |
Discussion
Resistant infectious keratitis (IK) is one of the major challenging conditions in Ophthalmology. Successful management aims at eradication of the infectious agent, halting disease progression, elimination of the associated ocular inflammation, and prevention of the potential complications. Recently, green thermal laser has been described as an adjunctive therapy for the treatment of resistant IK with promising outcomes.22 In this study, we show that adjunctive green laser therapy can be helpful in cases of IK, and fasten the healing process.
Fluorescein sodium is used as a chromophore to permit laser absorption, and to delineate the area of epithelial defect. After absorption by the corneal tissue, laser energy produces thermal damage to the infectious agent through suppression of its cellular enzymes and destruction of the cellular proteins and DNA.26 Additionally, the induced laser burns enhance the penetration of topical antimicrobial agents by means of the small pores created in the ulcer bed and the associated necrotic tissue debridement.22,27
Experimentally, Fromer et al reported successful outcomes after the use of adjunctive laser for treatment of Pseudomonas keratitis in rabbits.28 In 2013, Pellegrino and Carrasco reported excellent clinical outcomes after adjunctive laser application in 2 patients with refractory fungal keratitis.25
Khater et al conducted a prospective comparative interventional case series study on 20 eyes with resistant IK to evaluate the efficacy of adjunctive laser treatment. Ten patients were treated with laser as an adjunctive therapy. The remaining 10 patients were considered as the control group, and were treated with the specific antimicrobial drugs. All patients treated with laser achieved complete epithelial healing and resolution of stromal infiltrates within four weeks. The overall healing duration was shorter in the laser group than in the control group. In the laser group, no adverse effects were detected, and amniotic membrane transplantation (AMT) was needed in a single patient. In contrast, four cases needed an AMT due to thinning in the control group. They concluded that laser photocoagulation is useful as an adjunctive treatment for resistant infected corneal ulcers.22
In 2016, Khater et al compared laser photocoagulation to intrastromal voriconazole injection as adjunctive treatment modalities for cases of resistant mycotic corneal ulcers. The final outcome was better in the laser group regarding complete healing duration and complications.29 In another study, the same researcher compared the clinical outcome of AMT combined with either laser photocoagulation or simple tissue debridement for the treatment of resistant fungal corneal ulcers.27 He reported superior outcome in patients who received combined laser and AMT regarding treatment duration and visual outcome.
It is quite obvious that our results concur with the previously published reports. However, to the best of our knowledge, the number of cases and duration span in this study provide more comprehensive data.
In accordance with the prevalence of outdoor and agricultural activities in Egypt’s Delta region, most of our patients were males, with plant origin trauma. Fungal etiology was isolated in 115 cases (76.7%), of which 71 cases were mixed with bacteria. That may have played a significant role in resistance to standard medical treatment with subsequent need for an adjunctive therapy.
The application of an adequate number of confluent laser burns to cover the entire epithelial defect is crucial to achieve successful outcomes. Corneal micro-perforations during laser treatment were reported in 3 cases (2%). This could be attributed to laser application in the same spot, or the inadvertent movement of the patient’s eye. Additionally, 11 cases (7.3%) developed marked corneal thinning with descemetocele formation, mostly due to excess laser treatment and subsequent sloughing of necrotic tissues. AMT was performed in 26 cases (17.3%) compared to a single case (out of 10) in the study published by Khater et al.22
Our current study is limited by its retrospective nature. Loss of follow-up within rural areas is very common. The absence of a control or comparative group was a drawback. However, we tried to minimize any selection bias, and we believe, the large sample is an advantage. Comparing the treatment protocol described in this study to medical treatment only and other adjunctive therapies is an important tool to validate its safety and efficacy in future prospective studies.
In conclusion, green thermal laser is a safe and effective adjunctive therapy for the treatment of resistant infectious keratitis of fungal and/or bacterial etiologies.
Funding
No financial interests to disclose.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ting DSJ, Henein C, Said DG, Dua HS. Photoactivated chromophore for infectious keratitis - corneal cross-linking (PACK-CXL): a systematic review and meta-analysis. Ocul Surf. 2019;17(4):624–634. doi:10.1016/j.jtos.2019.08.006
2. Zhong J, Wang B, Li S, et al. Full-thickness conjunctival flap covering surgery combined with amniotic membrane transplantation for severe fungal keratitis. Exp Ther Med. 2018;15(3):2711–2718. doi:10.3892/etm.2018.5765
3. Erie JC, Nevitt MP, Hodge DO, Ballard DJ. Incidence of ulcerative keratitis in a defined population from 1950 through 1988. Arch Ophthalmol. 1993;111(12):1665–1671. doi:10.1001/archopht.1993.01090120087027
4. Upadhyay MP, Karmacharya PC, Koirala S, et al. The Bhaktapur Eye Study: ocular trauma and antibiotic prophylaxis for the prevention of corneal ulceration in Nepal. Br J Ophthalmol. 2001;85(4):388–392. doi:10.1136/bjo.85.4.388
5. Ting DSJ, Ho CS, Deshmukh R, Said DG, Dua HS. Infectious keratitis: an update on epidemiology, causative microorganisms, risk factors, and antimicrobial resistance. Eye (Lond). 2021;35(4):1084–1101. doi:10.1038/s41433-020-01339-3
6. Whitcher JP, Srinivasan M. Corneal ulceration in the developing world–a silent epidemic. Br J Ophthalmol. 1997;81(8):622–623. doi:10.1136/bjo.81.8.622
7. Ung L, Acharya NR, Agarwal T, et al. Infectious corneal ulceration: a proposal for neglected tropical disease status. Bull World Health Organ. 2019;97(12):854–856. doi:10.2471/BLT.19.232660
8. Keay L, Edwards K, Naduvilath T, et al. Microbial keratitis predisposing factors and morbidity. Ophthalmology. 2006;113(1):109–116. doi:10.1016/j.ophtha.2005.08.013
9. Khor WB, Prajna VN, Garg P, et al. The Asia Cornea Society Infectious Keratitis Study: a Prospective Multicenter Study of infectious keratitis in Asia. Am J Ophthalmol. 2018;195:161–170. doi:10.1016/j.ajo.2018.07.040
10. Bharathi MJ, Ramakrishnan R, Meenakshi R, Padmavathy S, Shivakumar C, Srinivasan M. Microbial keratitis in South India: influence of risk factors, climate, and geographical variation. Ophthalmic Epidemiol. 2007;14(2):61–69. doi:10.1080/09286580601001347
11. Dart JK, Saw VP, Kilvington S. Acanthamoeba keratitis: diagnosis and treatment update 2009. Am J Ophthalmol. 2009;148(4):487–99e2. doi:10.1016/j.ajo.2009.06.009
12. Egrilmez S, Yildirim-Theveny S. Treatment-resistant bacterial keratitis: challenges and solutions. Clin Ophthalmol. 2020;14:287–297. doi:10.2147/OPTH.S181997
13. Lalitha P, Manoharan G, Karpagam R, et al. Trends in antibiotic resistance in bacterial keratitis isolates from South India. Br J Ophthalmol. 2017;101(2):108–113. doi:10.1136/bjophthalmol-2016-308487
14. Ung L, Bispo PJM, Shanbhag SS, Gilmore MS, Chodosh J. The persistent dilemma of microbial keratitis: global burden, diagnosis, and antimicrobial resistance. Surv Ophthalmol. 2019;64(3):255–271. doi:10.1016/j.survophthal.2018.12.003
15. Sun Y, Sun Z, Chen Y, Deng G. Corneal debridement combined with intrastromal voriconazole for recalcitrant fungal keratitis. J Ophthalmol. 2018;2018:1875627. doi:10.1155/2018/1875627
16. Liu J, Sheha H, Fu Y, Liang L, Tseng SC. Update on amniotic membrane transplantation. Expert Rev Ophthalmol. 2010;5(5):645–661. doi:10.1586/eop.10.63
17. Yildiz EH, Nurozler AB, Ozkan Aksoy N, Altiparmak UE, Onat M, Karaguzel H. Amniotic membrane transplantation: indications and results. Eur J Ophthalmol. 2008;18(5):685–690. doi:10.1177/112067210801800504
18. Dev S, Rajaraman R, Raghavan A. Severe fungal keratitis treated with subconjunctival fluconazole. Am J Ophthalmol. 2006;141(4):783. author reply 83–4. doi:10.1016/j.ajo.2005.12.025
19. Prakash G, Sharma N, Goel M, Titiyal JS, Vajpayee RB. Evaluation of intrastromal injection of voriconazole as a therapeutic adjunctive for the management of deep recalcitrant fungal keratitis. Am J Ophthalmol. 2008;146(1):56–59. doi:10.1016/j.ajo.2008.02.023
20. Said DG, Elalfy MS, Gatzioufas Z, et al. Collagen cross-linking with photoactivated riboflavin (PACK-CXL) for the treatment of advanced infectious keratitis with corneal melting. Ophthalmology. 2014;121(7):1377–1382. doi:10.1016/j.ophtha.2014.01.011
21. Kumar V, Lockerbie O, Keil SD, et al. Riboflavin and UV-light based pathogen reduction: extent and consequence of DNA damage at the molecular level. Photochem Photobiol. 2004;80(1):15–21. doi:10.1562/2003-12-23-RA-036.1
22. Khater MM, Selima AA, El-Shorbagy MS. Role of argon laser as an adjunctive therapy for treatment of resistant infected corneal ulcers. Clin Ophthalmol. 2014;8:1025–1030. doi:10.2147/OPTH.S59928
23. Li J, Paulus YM. Advances in retinal laser therapy. Int J Ophthalmol Res. 2018;4(1):259–264. doi:10.17554/j.issn.2409-5680.2018.04.70
24. Cherry PM, Faulkner JD, Shaver RP, Wise JB, Witter SL. Argon laser treatment of corneal neovascularization. Ann Ophthalmol. 1973;5(8):911–920.
25. Pellegrino F, Carrasco MA. Argon laser phototherapy in the treatment of refractory fungal keratitis. Cornea. 2013;32(1):95–97. doi:10.1097/ICO.0b013e318256140e
26. Krauss JM, Puliafito CA, Steinert RF. Laser interactions with the cornea. Surv Ophthalmol. 1986;31(1):37–53. doi:10.1016/0039-6257(86)90050-0
27. Khater MM. Amniotic membrane graft with argon laser photocoagulation versus amniotic membrane graft with tissue debridement for treatment of mycotic keratitis. Semin Ophthalmol. 2017;32(3):348–352. doi:10.3109/08820538.2015.1090613
28. Fromer C, L’Esperance F. Argon laser phototherapy of pseudomonas corneal ulcers. Invest Ophthalmol. 1971;10(1):1–8.
29. Khater MM, El-Shorbagy MS, Selima AA. Argon laser photocoagulation versus intrastromal voriconazole injection in treatment of mycotic keratitis. Int J Ophthalmol. 2016;9(2):225–229. doi:10.18240/ijo.2016.02.07
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.