Back to Journals » Patient Preference and Adherence » Volume 14
Adherence to Dietary Advice and Oral Hygiene Practices Among Orthodontic Patients
Authors Aljohani SR ![]() , Alsaggaf DH
, Alsaggaf DH ![]()
Received 14 August 2020
Accepted for publication 6 October 2020
Published 20 October 2020 Volume 2020:14 Pages 1991—2000
DOI https://doi.org/10.2147/PPA.S277034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Salha R Aljohani, Doaa H Alsaggaf
Department of Orthodontics, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Salha R Aljohani
Department of Orthodontics, Faculty of Dentistry, King Abdulaziz University, Alsulemaneya, PO Box 80209, Jeddah 21589, Saudi Arabia
Tel +966 504684941
Fax +966 12 692 1262
Email [email protected]
Introduction: Adherence to dietary advice and proper oral hygiene practices during orthodontic treatment are critical to maintaining good oral health and achieving successful treatment results. Thus, understanding patients’ habits and practices before, during, and after orthodontic treatment is needed to ensure better oral health-related behavior among these patients.
Purpose: To investigate sugar-related dietary habits, visits to dental hygienists and dentists, and oral hygiene practices among patients during orthodontic treatment and after treatment compared to patients before treatment.
Methods: A cross-sectional self-administered survey collected data from 375 patients (aged 10 years and older) from the Orthodontic Department at King Abdulaziz University Dental Hospital, Jeddah, Saudi Arabia. Patients were grouped according to their history of receiving orthodontic treatment into: patients before orthodontic treatment, patients during treatment, and patients after treatment. The survey assessed sugar-related dietary habits, frequency of visits to hygienists and dentists, and oral hygiene practices.
Results: Patients during orthodontic treatment and those after treatment were less likely to eat sticky food compared to patients before treatment (OR=0.4, 95% CI=0.2– 0.9 and OR=0.5, 95% CI=0.3– 0.9, respectively). No significant differences were found in the odds of dental visits among the groups. Compared to patients before orthodontic treatment, patients during treatment and patients after treatment had higher odds of tooth brushing twice or more per day (OR=4.8, 95% CI=1.7– 14.3, and OR=4.0, 95% CI=1.2– 13.6, respectively) and were more likely to brush for an adequate time (OR=2.6, 95% CI=1.6– 4.4 and OR=1.9, 95% CI=1.0– 3.5, respectively). Moreover, the likelihood of flossing once daily was higher in patients during treatment and in patients after treatment relative to those before treatment. However, only patients during orthodontic treatment used interdental brushes more than patients before treatment.
Conclusion: Patients’ oral health-related behavior seems to improve during and after orthodontic treatment. The findings of this study suggest that orthodontists can play a role in improving oral hygiene practices among their patients. More reinforcement of dietary instructions and periodic dental and hygiene visits is needed during orthodontic follow-up appointments.
Keywords: oral health, orthodontic appliances, diet, dental hygienist, dentist, toothbrushing
Introduction
The orthodontic practice has attracted many patients who choose to have orthodontic treatment to improve their dental esthetics and function. Its popularity can also be related to positive effects of orthodontic treatment on patients’ self-regard and social interaction.1 It has been shown that malocclusion can negatively affect patients’ oral health-related quality of life, especially the psychological aspects.2 By addressing malocclusion, orthodontic treatment can enhance individuals’ dental function and esthetics as well as their social wellbeing and quality of life.
Orthodontic treatment may impact oral hygiene, given that orthodontic appliances tend to retain food debris and plaque and pose a great challenge when cleaned.3 Adherence to oral hygiene practices, particularly during orthodontic treatment, is critical for maintaining good oral health. Poor oral hygiene can lead to permanent damage to dental tissues ranging from white spot lesions to dental caries.4 Moreover, recent research has shown an increase in dental plaque after placement of fixed orthodontic appliances.5 Failure to remove dental plaque during orthodontic treatment can be detrimental to periodontal health and may lead to the development of gingivitis and periodontitis.6,7 The impact of periodontal health on general health is significant and cannot be neglected. In recent years, there has been an increasing amount of literature on the links between periodontitis and coronary heart disease.8,9 Breakthroughs in biomarker research found an association between periodontitis and increased serum levels of various inflammatory biomarkers.10–12 In order to maintain good oral and periodontal health, orthodontic patients are required to practice optimal oral hygiene measures such as brushing their teeth at least twice a day and using additional tools including interdental aids and mouthwash.13 Therefore, maintaining an adequate level of oral hygiene during orthodontic treatment requires commitment from the patient to practice good oral hygiene measures and to develop skills that demand time, effort, and motivation.
Orthodontic treatment may also have an influence on patients’ ways of eating. Patients may change their dietary habits and turn to softer food, as eating with orthodontic appliances is uncomfortable for them.14–17 In addition, orthodontic patients are instructed to minimize their consumption of sugary and sticky food since the risk of caries and white spot lesions is associated with increased consumption of sugar.18–22
Patient adherence to oral hygiene and dietary instructions during orthodontic treatment is as important a compliance factor as regular visits and maintenance of appliances since these are all critical for obtaining successful clinical results.23 Hence, patient selection, education, and motivation are essential steps that must be undertaken before commencing orthodontic treatment. Furthermore, oral hygiene advice and periodic follow-up by dental professionals are important for achieving the required level of oral health awareness and maintaining patients’ motivation.
Understanding orthodontic patients’ oral hygiene practices, dietary habits and dental visits is useful in guiding orthodontists and dentists to ensure optimal oral health-related behaviors among these patients. Therefore, the purpose of this study is to investigate the differences in sugar-related dietary habits, visits to dental hygienists and dentists, and oral hygiene practices among patients during orthodontic treatment, and patients after treatment, compared to patients before the start of orthodontic treatment.
Methods
This cross-sectional study was approved by the Research Ethics Committee of the Faculty of Dentistry at King Abdulaziz University, Jeddah, Saudi Arabia (approval # 017–01-19) and was carried out in accordance with the principles of the Declaration of Helsinki. A comprehensive electronic survey was designed to understand the dietary habits and oral health-related behaviors among orthodontic patients. Survey questions were thoroughly reviewed by a panel consisting of two orthodontists and two dentists to ensure readability and validity of the questions. Any unfavorable ambiguous question was rephrased or removed.
Patients, aged 10 years and older, registered in the patients' list of the Orthodontic Department at King Abdulaziz University Dental Hospital were invited to participate in the study. The patients’ list includes patients screened in preparation for orthodontic treatment, patients currently undergoing orthodontic treatment, as well as patients who finished their orthodontic treatment within the past 5 years. The survey was sent electronically to patients’ registered phone numbers. Study objectives were clearly communicated in the survey invitation and patients were informed that their contribution is voluntary and anonymous. Parents or guardians were invited to fill the survey for their young children. Completing the survey was considered a consent to participate in the study. Sample size estimation was done using G*Power 3.1.9.2. Considering a previous study by Petrauskiene et al24 we estimated that at least 368 subjects are required to achieve a power =0.9, at alpha= 0.05, to detect an OR=1.8 between the groups. Data collection was conducted between March and July 2019. The survey was sent to 800 patients. Of those, 375 patients completed the questionnaire.
The questionnaire initially asked patients whether they have ever received orthodontic treatment. Based on their response to this question, participants were divided into three groups: patients before the start of orthodontic treatment (G1), patients during orthodontic treatment (G2), and patients who finished orthodontic treatment (G3). Participants who never had orthodontic treatment and were not interested in receiving treatment were excluded from the study. The outcome measures were sugar-related dietary habits, attendance to dental hygiene and dental visits, and oral hygiene practices. Sugar-related dietary habits were evaluated by two questions: “how frequently do you consume sugar?” and “how frequent do you eat sticky food?”. Responses were rated on a 5-point Likert scale ranging from “never” to “always”. Frequency of visits to the dental hygienist was also assessed on the same Likert scale. Due to small frequencies, responses were grouped into “never/rarely”, “sometimes”, and “usually/always”. Dental visits were evaluated by asking participants “How often do you visit your dentist?”. Responses were either “when I have a dental problem”, “once a year”, or “twice a year”. Oral hygiene practices were assessed by measuring tooth brushing frequency (responses were “irregularly”, “once a day”, or “twice or more a day”), and duration (“≤1minute” or “≥2 minutes”). We also evaluated the use of auxiliary oral hygiene measures including the use of mouthwash (responses ranged from “never” to “always”), the use of the dental floss and interdental brushes (both measured on a scale ranging from “never” to “twice or more/day”). The survey also incorporated questions about demographics, namely, gender, age group, education, marital status and employment status. (Detailed questionnaire in Appendix 1). Reliability of the survey questions was evaluated using weighted Cohen’s kappa by requesting 10 individuals to answer the questionnaire two times with a two-week interval. Intrarater reliability of questions ranged from 0.82 to 0.9 indicating very good agreement.
Statistical analyses were carried out using IBM SPSS Statistics for Macintosh, Version 25.0 (IBM Corp, Armonk, NY). Frequency distribution of study variables was computed. Chi-square tests were used to assess the differences in demographics, dietary habits, dental hygienist and dental visits, as well as oral hygiene practices among the three study groups. Multivariate logistic regression analyses (multinomial and binary logistic regression models) were used to predict the adjusted odds of each outcome variable among patients during orthodontic treatment (G2), and those after orthodontic treatment (G3) compared to patients before orthodontic treatment (G1) while adjusting for demographic variables. Statistical significance was tested at alpha= 0.05.
Results
A total of 375 patients (G1 =108, G2= 165, and G3= 102) participated in the study. The majority of the participants were females (73.1%), while 26.9% were males. Approximately one-third of G2 patients were males, compared to 29.6% of patients in G1 and only 14.7% of those in G3 (P=0.004). Table 1 summarizes the demographic characteristics of patients in the three groups. Generally, there were statistically significant differences in the distribution of demographic characteristics among the three study groups. Patients in G3 were significantly older than G1 and G2 patients (P<0.001). Significant differences in the educational level of the participants were also found with G3 patients being more likely to have higher educational attainment compared to G1 and G2 participants (P<0.001). Most of the participants were single. G2 patients were most likely to be single (86.1%) compared to 79.6% of G1 patients, and 59.8% of patients in G3 (P<0.001). Furthermore, G1 and G2 had more students and less employed participants, compared to G3 (P=0.001).
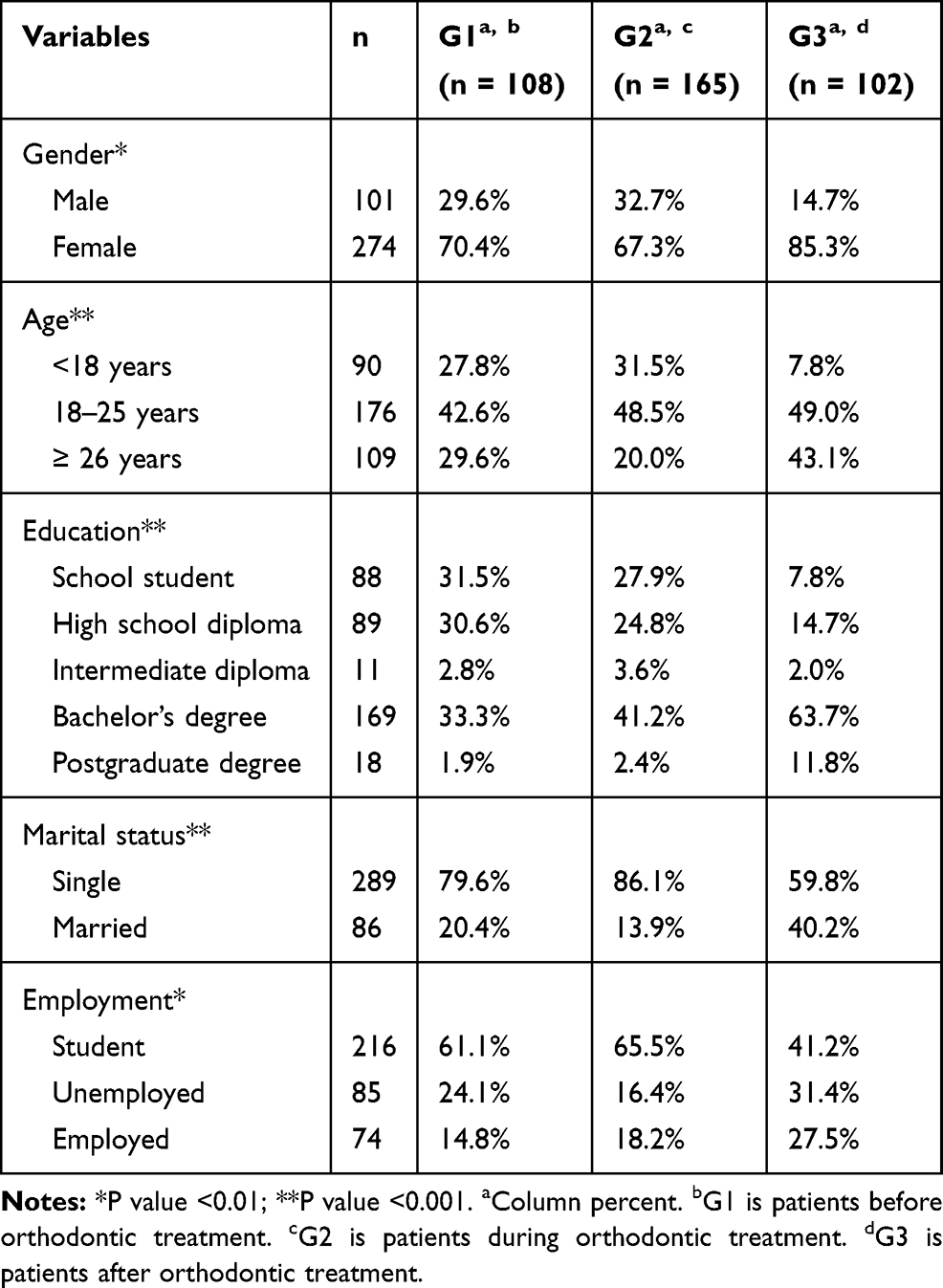 |
Table 1 Demographic Characteristics of Study Participants (N= 375) |
Comparisons of sugar-related dietary habits, dental hygienist visits, and dental visits among the study groups are presented in Table 2. There were no significant differences in the frequency of sugar consumption, or the frequency of eating sticky food among the three groups (P=0.9 and P=0.07, respectively). Approximately 16% of all participants reported visiting the dental hygienist usually or always, and the frequency of dental hygiene visits varied significantly among the groups (P=0.005). Most of the participants reported visiting a dentist only when they have a problem. Although G2 participants were less likely to visit the dentist twice a year, there were no significant differences in dental attendance among the three groups (P=0.4).
 |
Table 2 Comparison of Dietary Habits, Hygienist Visits, and Dental Visits Among Study Participants (N= 375) |
Table 3 presents results from multinomial logistic regression models predicting dietary habits and attendance to hygiene and dental visits among study participants. After controlling for demographic confounders, the odds of consuming sugar in G3, and consuming sugar sometimes in G2 were higher relative to G1. However, these associations were not statistically significant (model 1). The frequency of sticky food consumption differed significantly among the three groups. G3 patients were 50% less likely to eat sticky food sometimes than never or rarely, compared to patients in G1 (OR= 0.5, 95% CI=0.3–0.9). Moreover, compared to G1 patients, patients in G2 were 60% less likely to eat sticky food usually or always (OR= 0.4, 95% CI=0.2–0.9) (model 2). Model 3 shows the adjusted odds of hygienist visits in G2 and G3 patients, relative to G1. G3 patients were 70% less likely to visit the hygienist sometimes than never or rarely when compared to G1. Both G2 and G3 had higher, yet not statistically significant, odds of visiting the hygienist usually to always compared to G1. Dental attendance in G2 patients did not differ significantly from that of G1 patients. While G3 patients had higher odds of visiting a dentist relative to G1 patients, the association was not statistically significant (OR= 1.1, 95% CI=0.4–2.7 and OR= 2.3, 95% CI=1.0–5.5, for dental visits once/year and twice/year, respectively).
 |
Table 3 Adjusted Odds Ratios for Dietary Habits, Hygienist Visits, and Dental Visits Among Study Participants (N=375)a |
A comparison of oral hygiene practices among participants in the three groups is shown in Table 4. About 78% of all participants reported brushing twice a day or more, with 87.3% of G2 patients brushing twice or more daily compared to 70.4% and 71.6% of G1 and G3 patients, respectively (P<0.001). Patients in G2 were also more likely brush for 2 minutes or more (P=0.001). Significant differences were found in the use of mouthwash (P=0.004) and interdental brushes (P<0.001) among the three groups. Nevertheless, no statistically significant differences were found in dental floss use (P=0.08).
 |
Table 4 Comparison of Oral Hygiene Practices Among Study Participants (N=375) |
Adjusted odds of oral hygiene practices in G2 and G3 in relation to G1 are presented in Table 5. Generally, G2 and G3 patients had better tooth brushing practices relative to G1 patients. Patients in G2 had 4.8 times the odds of brushing their teeth 2 times or more per day compared to G1 patients. Moreover, G3 patients had significantly higher odds of brushing their teeth once a day and twice or more per day compared to G1 (OR=5.4, 95% CI=1.4–20.7 for brushing once/day, and OR= 4.0, 95% CI=1.2–13.6 for brushing twice or more/day). Additionally, the odds of brushing for 2 minutes or more were, respectively, 2.6 and 1.9 times greater among G2 and G3 patients relative to patients in G1 (model 6). Regarding the use of adjunctive oral hygiene measures, G2 patients had higher, yet not significant, odds of using mouthwash sometimes and usually/always in relation to G1. There were no significant differences in mouthwash use between G3 patients compared to G1 (model 7). The odds of using the dental floss once a day were greater among G2 and G3 patients compared to G1 (OR=2.6, 95% CI=1.2–5.7 and OR= 2.5, 95% CI=1.1–6.1, for G2 and G3, respectively). Nevertheless, the odds of flossing twice or more a day did not differ significantly between G2 and G3 relative to G1. Model 9 shows the adjusted odds of interdental brush use among participants. Compared to G1 patients, G2 patients had higher odds of using interdental brushes. The use of interdental brushes in G3 patients nevertheless did not differ significantly than that in G1 patients.
 |
Table 5 Adjusted Odds Ratios for Oral Hygiene Practices Among Study Participants (N=375)a |
Discussion
Oral hygiene practices are considered the most constant adherence factor among orthodontic patients.25 On the one hand, their adherence to oral hygiene and dietary advice is crucial for the success of their orthodontic treatment. On the other hand, the lack of adherence might lead to dental and periodontal damage. Thus, this study was conducted to examine the differences in sugar-related dietary habits, visits to dental hygienists and dentists, and oral hygiene practices among patients during and after orthodontic treatment compared to patients before the start of treatment. The findings of the current study indicated that patients under active treatment and even those after treatment had better oral hygiene practices and consumed sticky food less frequently compared to patients before treatment.
The average age of active orthodontic patients in this study was older (68.5% >18 years) compared to those in previous studies, which investigated younger participants.26–28 The increased number of responses among adults could be due to the method used for survey invitation, which was sent to patients’ registered phone numbers. In this study, the majority of the participants were females (73.1%), with males comprising 26.9% of the sample. This distribution of gender is consistent with the literature and with the distribution of patients who attend orthodontic practice and seek orthodontic treatment.24,26,27,29,30 This might be because females are more concerned about esthetics than males and have a higher demand for orthodontic treatment.31,32 However, some studies reported different patterns of gender distribution, with more males undergoing orthodontic treatment than females.33,34
Diet is an important component of oral health as the kind of food trapped between brackets affects the type of plaque that can build up. Increased sugar intake can be a risk factor for caries and white spot lesions.35 In addition, sticky food is more likely to get stuck between brackets for a longer time. Thus, patients are advised by orthodontists to avoid eating sticky food and reduce their sugar consumption. The present study found a high level of sugar consumption among all patients (52.1–56.5%). Moreover, although not statistically significant, sugar consumption was higher in patients during and after treatment compared to controls. Nadar et al reported a similar finding with only 50% of patients avoiding sugar.36 However, a previous study reported a lower sugar consumption among patients during orthodontic treatment (14%).37 Although sugar consumption did not vary significantly among the groups, patients under active treatment and those after treatment were significantly less likely to consume sticky food compared to patients before treatment.
Orthodontic treatment may cause dietary changes since some patients may opt to eat less frequently due to the constant need to brush their teeth to eliminate the food trapped in their appliances.17 In addition, their diet can be influenced by instructions from the orthodontists to avoid sweets as well as hard and sticky food. Thus, they are likely to adhere to a soft diet to maintain the appliances. However, patients may fail to follow their orthodontist’s advice on sugary and sticky food as their effects on teeth are not immediate. In addition, some may still prefer to consume these types of foods and overcome the risks by simply brushing their teeth more frequently. Changing dietary habits during orthodontic treatment is related to age in that it is more significant among adults (>18), who are more aware of consequences than younger patients.38 The latter are less likely to consider their orthodontist’s advice and change their dietary habits.39,40 Patients may also find it difficult to follow their orthodontist’s advice completely and change their dietary habits as they find the advice unrealistic.40,41 The findings of this and previous studies highlight the importance of dealing with patients’ expectations as well as reinforcing dietary advice through informed consent and constant reminders during follow-up visits.
The results of this study indicated higher odds of frequent visits to hygienists among the patients during and after orthodontic treatment. However, after controlling for demographics, the odds of these patients visiting a hygienist usually or always were not significantly different than in controls. Furthermore, patients after treatment were significantly less likely to visit a hygienist sometimes. Previous studies indicated more frequent visits to dental hygienists by orthodontic patients.24,42 In contrast, Atassi and Awartani reported a low frequency of visits to hygienists among orthodontic patients, though there was no control group in their study.37 The frequency of dental visits in this study also did not differ significantly between the groups. Petrauskiene et al reported better dental attendance among patients that underwent orthodontic treatment. However, their study focused mainly on adolescents.24
The most important step in the mechanical removal of dental plaque is brushing teeth at least twice a day for a minimum of two minutes. Proper brushing is vital for ensuring dental and gingival health. In fact, brushing frequency is correlated with gingival enlargement.34 In this study, patients under active orthodontic treatment (G2) and those after treatment (G3) were significantly more likely to brush their teeth twice per day or more. These patients also had higher odds of brushing their teeth for two minutes or more in comparison to the control group (G1). Many studies observed a high percentage (>90%) of orthodontic patients brushing their teeth at least twice a day.27–29,43 In comparison, other studies reported reduced adherence to toothbrushing (<65%).26,30,33,34,37 These varying findings could be attributed to several reasons, such as differences in demographic factors or oral hygiene advice protocols implemented in the different countries and hospitals investigated in these studies.
The use of dental floss is associated with better gingival health in orthodontic patients.44 However, only 33.3% of active orthodontic patients in this study reported using the dental floss once a day or more. Atassi and Awartani described that, among Saudi orthodontic patients, the use of dental floss was as low as 6%.37 Furthermore, Martignon et al indicated less frequent dental floss use among orthodontic patients compared to the reference group.43 These findings can be explained by the fact that dental floss cannot be easily used in the presence of fixed orthodontic appliances. Thus, patients might be reluctant to use it while undergoing orthodontic treatment.
Slightly more than half of active orthodontic patients in this study used an interdental brush at least once daily. Previous studies, meanwhile, reported low utilization of interdental brushes (7–23%) among orthodontic patients.28,30,33,37 Collectively, the findings showed that the use of interdental tools, such as dental floss and interdental brushes, was significantly higher among the patients under active orthodontic treatment (G2) compared to the control group (G1). Similar findings were described by Petrauskiene et al.24 In contrast, many other studies indicated lower utilization of interdental tools among patients.28,30,37,42,44–46
During orthodontic treatment, ideal oral hygiene may not be achieved simply by the mechanical removal of dental plaque. Daily rinsing with fluoridated mouthwash can significantly improve dental health and reduce white spot lesions.47–49 In the current study, patients during treatment had higher odds of using mouthwash. However, this was not a significant finding compared to the control group. Petrauskiene et al reported a statistically significant increase in mouthwash use among orthodontic patients compared to controls.24 In contrast, other studies found lower adherence to the use of mouthwash.28,30,36,42,50 A possible explanation for this finding might be that the use of mouthwash was not reinforced as well as the use of interdental tools.
Comparing active orthodontic patients (G2) and deboned orthodontic patients (G3) to the control group (G1) revealed interesting data. Improvement in oral hygiene practices during orthodontic treatment can be attributed to continuous monitoring and the oral hygiene instructions that are given during monthly follow-up visits. Orthodontic residents are trained to give all their patients comprehensive oral hygiene instructions together with dietary advice on sugary and sticky food consumption when starting orthodontic treatment and at every follow-up appointment. Another possible explanation for this improvement in oral hygiene practices during orthodontic treatment is the retentive nature of orthodontic appliances, which require more frequent cleaning. Improved oral hygiene practices were observed among patients even after orthodontic treatment as patients seemed to develop good oral hygiene habits and skills, which they picked up during orthodontic treatment and retained after its completion. Hence, patients’ increased awareness through the long course of orthodontic treatment may be considered an additional benefit of such a treatment.
To the best of our knowledge, this study is the first to evaluate dietary habits and oral hygiene measures among patients after orthodontic treatment. Previous studies also did not control for demographic confounders when comparing oral health-related behavior among orthodontic patients. Nevertheless, this study has some limitations. The data were collected using a self-administered questionnaire, so patient responses might have been affected by social desirability and recall issues. In addition, the findings of this study might not be generalizable to patients in populations with different characteristics. Further longitudinal studies following patients before, during and after orthodontic treatment are necessary to understand the influence of orthodontic treatment on individuals’ oral health-related behavior.
Conclusion
The findings of this study suggest that oral health-related behaviors seem to improve during and after orthodontic treatment. Patients during orthodontic treatment had better oral hygiene practices and were less likely to consume sticky food frequently compared to those who had yet to start treatment. The present study also provides evidence on patients after orthodontic treatment. These patients appear to adhere to some of the good oral hygiene practices. Nevertheless, sugar consumption and visits to dental hygienists and dentists did not vary significantly between the groups. With these findings, we can conclude that orthodontists may play a role in improving oral hygiene practices among their patients. However, additional efforts by orthodontists are required to reinforce dietary instructions and routine dental visits before the start of orthodontic treatment and during follow-up visits to maintain good oral health.
Abbreviations
OR, odds ratios; CI, confidence intervals.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Grewal H, Sapawat P, Modi P, Aggarwal S. Psychological impact of orthodontic treatment on quality of life – a longitudinal study. Int Orthod. 2019;17(2):269–276. doi:10.1016/j.ortho.2019.03.009
2. Masood Y, Masood M, Zainul NNB, Araby NBAA, Hussain SF, Newton T. Impact of malocclusion on oral health related quality of life in young people. Health Qual Life Outcomes. 2013;11(25):1–6.
3. Arici S, Alkan A, Arici N. Comparison of different toothbrushing protocols in poor-toothbrushing orthodontic patients. Eur J Orthod. 2007;29(5):488–492. doi:10.1093/ejo/cjm038
4. Zachrisson BU, Zachrisson S. Caries incidence and oral hygiene during orthodontic treatment. Eur J Oral Sci. 1971;79(4):394–401. doi:10.1111/j.1600-0722.1971.tb02028.x
5. Thornberg MJ, Riolo CS, Bayirli B, Riolo ML, Van Tubergen EA, Kulbersh R. Periodontal pathogen levels in adolescents before, during, and after fixed orthodontic appliance therapy. Am J Orthod Dentofacial Orthop. 2009;135(1):95–98. doi:10.1016/j.ajodo.2007.02.057
6. Zachrisson S, Zachrisson BU. Gingival condition associated with orthodontic treatment. Angle Orthod. 1972;42(1):26–34.
7. Lara-Carrillo E, Montiel-Bastida NM, Sanchez-Perez L, Alanis-Tavira J. Effect of orthodontic treatment on saliva, plaque and the levels of Streptococcus mutans and Lactobacillus. Medicina Oral Patología Oral y Cirugia Bucal. 2010;15(6):e924–e929. doi:10.4317/medoral.15.e924
8. Holmlund A, Holm G, Lind L. Number of teeth as a predictor of cardiovascular mortality in a cohort of 7674 subjects followed for 12 years. J Periodontol. 2010;81(6):870–876. doi:10.1902/jop.2010.090680
9. Vedin O, Hagström E, Budaj A, et al. Tooth loss is independently associated with poor outcomes in stable coronary heart disease. Eur J Prev Cardiol. 2016;23(8):839–846. doi:10.1177/2047487315621978
10. Isola G, Alibrandi A, Currò M, et al. Evaluation of salivary and serum asymmetric dimethylarginine (ADMA) levels in patients with periodontal and cardiovascular disease as subclinical marker of cardiovascular risk. J Periodontol. 2020;91(8):1076–1084. doi:10.1002/JPER.19-0446
11. Isola G, Polizzi A, Santonocito S, Alibrandi A, Ferlito S. Expression of salivary and serum malondialdehyde and lipid profile of patients with periodontitis and coronary heart disease. Int J Mol Sci. 2019;20(23):6061. doi:10.3390/ijms20236061
12. Isola G, Polizzi A, Iorio-Siciliano V, Alibrandi A, Ramaglia L, Leonardi R. Effectiveness of a nutraceutical agent in the non-surgical periodontal therapy: a randomized, controlled clinical trial. Clin Oral Investig. 2020;1–11.
13. British Orthodontic Society. Patient information leaflet: how to keep your teeth and gum healthy. 2019. https://view.publitas.com/british-orthodontic-society/food-and-drinkmarch2019/page/1.
14. Bernabé E, Sheiham A, de Oliveira CM. Impacts on daily performances related to wearing orthodontic appliances: a study on brazilian adolescents. Angle Orthod. 2008;78(3):482–486. doi:10.2319/050207-212.1
15. Utomi I Challenges and motivating factors of treatment among orthodontic patients. 2007.
16. Johal A, Al Jawad FA, Marcenes W, Croft N. Does orthodontic treatment harm children’s diets? J Dent. 2013;41(11):949–954. doi:10.1016/j.jdent.2013.08.025
17. Al Jawad AF, Cunningham SJ, Croft N, Johal A. A qualitative study of the early effects of fixed orthodontic treatment on dietary intake and behaviour in adolescent patients. Eur J Orthod. 2012;34(4):432–436. doi:10.1093/ejo/cjr032
18. British Orthodontic Society. Patient information leaflet: teeth and brace-friendly food and drink. 2019. https://view.publitas.com/british-orthodontic-society/oralhealthmarch2019/page/1.
19. Moynihan P, Petersen PE. Diet, nutrition and the prevention of dental diseases. Public Health Nutr. 2004;7(1a):201–226. doi:10.1079/PHN2003589
20. Duggal M, Van Loveren C. Dental considerations for dietary counselling. Int Dent J. 2001;51(S6):408–412. doi:10.1111/j.1875-595X.2001.tb00588.x
21. Marshall TA. Chairside diet assessment of caries risk. J Am Dent Assoc. 2009;140(6):670–674. doi:10.14219/jada.archive.2009.0252
22. Sudjalim T, Woods M, Manton D. Prevention of white spot lesions in orthodontic practice: a contemporary review. Aust Dent J. 2006;51(4):284–289. doi:10.1111/j.1834-7819.2006.tb00445.x
23. Tervonen -M-M, Pirttiniemi P, Lahti S. Development of a measure for orthodontists to evaluate patient compliance. Am J Orthod Dentofacial Orthop. 2011;139(6):791–796. doi:10.1016/j.ajodo.2009.10.045
24. Petrauskiene S, Wanczewska N, Slabsinskiene E, Zemgulyte G. Self-reported changes in oral hygiene habits among adolescents receiving orthodontic treatment. Dent J. 2019;7(4):96–107. doi:10.3390/dj7040096
25. Al Shammary N, Asimakopoulou K, McDonald F, Newton JT, Scambler S. How is adult patient adherence recorded in orthodontists’ clinical notes? A mixed-method case-note study. Patient Prefer Adherence. 2017;11:1807–1814. doi:10.2147/PPA.S141943
26. Sawai DS, Singh P, Tushar T, Dogra M, Sultana R, Khan S. Perception, awareness, and practice among patients seeking orthodontic treatment toward maintenance of periodontal health and factors affecting the same among patients visiting dental clinics in Patna. J Family Med Prim Care. 2019;8(11):3695–3699. doi:10.4103/jfmpc.jfmpc_773_19
27. Al-harbi AA, Alkhulayfi AS, Alharbi AT, Al-harbi M, Al-harbi AS, Al-harbi NS. Knowledge of patients about association between orthodontic treatment and periodontal diseases. Int J Oral Care Res. 2018;6:43–46.
28. Baheti MJ, Toshniwal NG. Survey on oral hygiene protocols among orthodontic correction-seeking individuals. J Educ Ethics Dent. 2015;5(1):8–13. doi:10.4103/0974-7761.178020
29. Alhaija AES, Al-Saif EM, Taani DQ. Periodontal health knowledge and awareness among subjects with fixed orthodontic appliance. Dental Press J Orthod. 2018;23(5):
30. Pandey V, Chandra S, Kumar HD, Gupta A, Bhandari PP, Rathod P. Impact of dental neglect score on oral health among patients receiving fixed orthodontic treatment: a cross-sectional study. J Int Soc Prev Community Dent. 2016;6(2):120–124. doi:10.4103/2231-0762.178752
31. Holmes A. The subjective need and demand for orthodontic treatment. Br J Orthod. 1992;19(4):287–297. doi:10.1179/bjo.19.4.287
32. Lagorsse A, Gebeile-Chauty S. Does gender make a difference in orthodontics? A literature review. Orthod Fr. 2018;89(2):157–168.
33. Shah K, Shenava S, Kulshrestha R, Hawaldar C. Evaluation of oral hygiene and perception of patients undergoing orthodontic treatment attending OPD at Terna Dental College, Mumbai, Maharashtra. Int Dent J Stud Res. 2018;6:81–84.
34. Eid HA, Assiri HAM, Kandyala R, Togoo RA, Turakhia VS. Gingival enlargement in different age groups during fixed orthodontic treatment. J Int Oral Health. 2014;6(1):1–4.
35. Khalaf K. Factors affecting the formation, severity and location of white spot lesions during orthodontic treatment with fixed appliances. J Oral Maxillofac Surg. 2014;5(1):1–10. doi:10.5037/jomr.2014.5104
36. Nadar S, Dinesh SS. A questionnaire study about oral hygiene awareness among orthodontic patients. Int J Orthod Rehabil. 2016;7(3):97–100.
37. Atassi F, Awartani F. Oral hygiene status among orthodontic patients. J Contemp Dent Pract. 2010;11(4):1–10.
38. Negrutiu BM, Todor BI, Moca A, Vaida LL, Pusta CJ. Dietary habits and weight loss in orthodontic patients. Hum Vet Med. 2019;11(2):57–60.
39. Azaripour A, Willershausen I, Hassan M, Ebenezer S, Willershausen B. Oral hygiene and dietary habits in adolescents with fixed orthodontic appliances: a Cross-sectional Study. J Contemp Dent Pract. 2016;17(3):179–183. doi:10.5005/jp-journals-10024-1824
40. Perry J, Johnson I, Popat H, Morgan MZ, Gill P. Adolescent perceptions of orthodontic treatment risks and risk information: a qualitative study. J Dent. 2018;74:61–70. doi:10.1016/j.jdent.2018.04.011
41. Wickström A. “One step at a time”: analysing young patients’ video diaries in an ethnographic tracing of fixed appliances. Child Soc. 2017;31(3):183–193. doi:10.1111/chso.12179
42. Krupińska-Nanys M, Zarzecka J. An assessment of oral hygiene in 7–14-year-old children undergoing orthodontic treatment. J Int Oral Health. 2015;7(1):6–11.
43. Martignon S, Ekstrand K, Lemos M, Lozano M, Higuera C. Plaque, caries level and oral hygiene habits in young patients receiving orthodontic treatment. Community Dent Health. 2010;27(3):133–138.
44. Zanatta FB, Moreira CHC, Rösing CK. Association between dental floss use and gingival conditions in orthodontic patients. Am J Orthod Dentofacial Orthop. 2011;140(6):812–821. doi:10.1016/j.ajodo.2011.06.028
45. Abuaffan A, Elamin L. Oral hygiene performance among a sample of sudanese orthodontic patients. Pyrex J Dent Oral Hyg. 2015;1(1):1–8.
46. Lee J, Abdullah A, Yahya N. Oral hygiene practices among fixed orthodontic patients in a university dental setting. Int J Oral Dent Health. 2016;2(2):027–030. doi:10.23937/2469-5734/1510027
47. Baehni P, Takeuchi Y. Anti‐plaque agents in the prevention of biofilm-associated oral diseases. Oral Dis. 2003;9:23–29. doi:10.1034/j.1601-0825.9.s1.5.x
48. Geiger AM, Gorelick L, Gwinnett AJ, Benson BJ. Reducing white spot lesions in orthodontic populations with fluoride rinsing. Am J Orthod Dentofacial Orthop. 1992;101(5):403–407. doi:10.1016/0889-5406(92)70112-N
49. Benson P, Shah A, Millett D, Dyer F, Parkin N, Vine R. Fluorides, orthodontics and demineralization: a systematic review. J Orthod. 2005;32(2):102–114. doi:10.1179/146531205225021033
50. Anuwongnukroh N, Dechkunakorn S, Kanpiputana R. Oral hygiene behavior during fixed orthodontic treatment. Dentistry. 2017;7(10):1–5.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.