Back to Journals » Patient Preference and Adherence » Volume 20
Adherence to Antihypertensive Medication and Its Associated Factors Among Patients with Hypertension Attending a Tertiary Hospital in Mogadishu, Somalia: A Cross-Sectional Study
Authors Shukri OM ![]() , Maani NA
, Maani NA ![]() , Adam MH
, Adam MH ![]() , Hussein AA
, Hussein AA ![]() , Noushad M
, Noushad M ![]() , Ahmed SA
, Ahmed SA ![]() , Mohamoud JH
, Mohamoud JH ![]() , Elmi OS
, Elmi OS ![]()
Received 7 March 2026
Accepted for publication 17 June 2026
Published 29 June 2026 Volume 2026:20 607701
DOI https://doi.org/10.2147/PPA.S607701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Omar Mohamed Shukri,1 Nadia Abdirahim Maani,1 Mohamed Hussein Adam,2 Anisa Abdullahi Hussein,3 Mohammed Noushad,4 Said Abdirahman Ahmed,5 Jamal Hassan Mohamoud,2 Omar Salad Elmi6
1Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 2Department of Public Health, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 3Department of Public Health Emergency, State Ministry of Health, Jowhar, Hirshabelle, Somalia; 4College of Dentistry, Dar Al Uloom University, Riyadh, Saudi Arabia; 5Department of Cardiology, Mogadishu Somalia Turkish Training and Research Hospital, Mogadishu, Somalia; 6School of Population and Global Health, Faculty of Medicine and Dentistry, University of Melbourne, Melbourne, Australia
Correspondence: Mohamed Hussein Adam, Email [email protected]
Background: Hypertension is the leading modifiable risk factor for cardiovascular disease and premature mortality worldwide. In Somalia, the national hypertension control rate is estimated at only 10%, yet antihypertensive medication adherence remains unstudied. This study determined the prevalence of medication adherence and its independent predictors among hypertensive outpatients in Mogadishu.
Methods: A hospital-based cross-sectional study was conducted between January and April 2024 at Mogadishu Somali-Turkey Training and Research Hospital. In total, 373 adult hypertensive patients on antihypertensive treatment for at least six months were recruited by simple random sampling. Adherence was assessed using the validated 8-item Morisky Medication Adherence Scale (MMAS-8), a self-reported instrument; scores of 6– 8 were classified as high or moderate adherence (adherent) and scores below 6 as low adherence (non-adherent). Multivariable binary logistic regression was used to identify independent predictors (p < 0.05).
Results: Of 373 participants (54.2% male; 45.8% aged ≥ 65 years), 63.5% demonstrated high or moderate adherence and 36.5% exhibited low adherence. Multivariable logistic regression identified four independent predictors of adherence. T2DM (AOR = 0.458; 95% CI: 0.279– 0.752; p = 0.002) and high-salt diet consumption (AOR = 0.460; 95% CI: 0.271– 0.780; p = 0.004) were independently associated with lower odds of adherence. Ischemic heart disease (IHD) was associated with 2.15 times higher odds of adherence (AOR = 2.151; 95% CI: 1.214– 3.811; p = 0.009). Divorced marital status was also associated with higher odds of adherence compared with married status (AOR = 3.077; 95% CI: 1.211– 7.817; p = 0.018).
Conclusion: More than one-third of patients exhibited low adherence. T2DM and IHD showed opposing associations with adherence, reflecting the contrasting motivational dynamics of these comorbidities. High-salt dietary intake and divorced marital status were additional independent predictors. These findings, interpreted within the context of the observational design and self-reported measurement, underscore the need for patient-centred, integrated interventions addressing comorbidity burden and dietary behaviour to improve antihypertensive adherence in Somalia. Future prospective research using objective adherence measures is recommended.
Keywords: hypertension, medication adherence, antihypertensive therapy, MMAS-8, predictors, Somalia, cross-sectional study
Introduction
Hypertension is the leading modifiable risk factor for cardiovascular disease, stroke, chronic kidney disease, and premature mortality worldwide.1,2 The global prevalence of hypertension has risen substantially over the past three decades, with the number of people living with hypertension aged 30 to 79 years nearly doubling between 1990 and 2019, from 648 million to 1.28 billion, with the greatest burden concentrated in low- and middle-income countries.3 Despite the availability of effective antihypertensive medications, blood pressure control rates remain inadequate globally, and poor medication adherence is recognised as the primary driver of this gap.4,5
Non-adherence to antihypertensive therapy encompasses failure to initiate medication, deviation from prescribed regimens, and early discontinuation of long-term treatment.4 It is associated with increased risk of cardiovascular events, hospitalisation, and death.5,6 Factors identified in the literature as predictors of non-adherence include advanced age, sex, comorbid conditions such as type 2 diabetes mellitus (T2DM) and chronic kidney disease (CKD), polypharmacy, smoking, and unhealthy dietary behaviours including high-salt intake.7–9 Critically, these factors do not operate independently; behavioural, health system, and treatment-related determinants interact dynamically, and their relative importance varies considerably by setting. Evidence from fragile, resource-limited health systems; where health system failures compound patient-level barriers, remains scarce, limiting the applicability of adherence frameworks developed in high-income contexts.
In Somalia, hypertension represents a major and growing public health challenge. Recent data estimate the national prevalence of hypertension at approximately 40%, exceeding the global average, with a hypertension control rate of only 10%.10 These figures reflect decades of civil conflict that have dismantled medical infrastructure and left the health system severely fragmented. Somalia’s healthcare system remains heavily privatized and poorly regulated,11 with only 18.5% of health facilities having undergone any accreditation.12 Several structural features of this system are particularly relevant to medication adherence: the fragmented care landscape disrupts continuity of prescriptions; out-of-pocket medication costs incentivise supply self-regulation based on affordability rather than clinical need; pharmacy benefit programmes are virtually absent; and community-level adherence support structures remain underdeveloped.
Despite this substantial burden, prior research in Somalia has focused almost exclusively on hypertension prevalence, risk factors, and knowledge, attitudes, and practices (KAP), with no published study examining adherence to antihypertensive medication or its determinants.10,13–15 This evidence gap limits the design of targeted, contextually appropriate interventions. The present study addresses that gap by pursuing two specific objectives: (1) to determine the prevalence of antihypertensive medication adherence among hypertensive outpatients attending a major tertiary hospital in Mogadishu, Somalia; and (2) to identify the independent clinical, behavioural, and sociodemographic predictors of medication adherence in this population. The findings are intended to inform targeted interventions to improve medication adherence and blood pressure control in this high-burden, resource-limited setting.
Methods
Study Design and Setting
A hospital-based cross-sectional study was conducted between January and April 2024 at Mogadishu Somali-Turkey Training and Research Hospital. This public-private partnership hospital, operated in collaboration with the Turkish and Somali governments, serves as the primary tertiary referral, training, and research centre in Mogadishu and provided the patient volume necessary for this investigation.
Study Population and Eligibility Criteria
Adults aged 18 years or above with a confirmed diagnosis of hypertension, attending outpatient clinics, who had received antihypertensive treatment for at least six months with a minimum of two recorded clinic visits, were conscious and alert, and provided written informed consent were eligible for inclusion. Individuals under 18 years, those who were not conscious or alert, pregnant or breastfeeding women, patients with cognitive impairment or mental health conditions, those who had recently initiated antihypertensive therapy (less than six months), and those who declined to consent were excluded.
Sample Size and Sampling Method
The sample size was calculated using the Cochran formula, assuming a 95% confidence level, a 5% margin of error, and a reference adherence prevalence of 61.8%,16 yielding a minimum of 363 participants. After adding a 10% non-response allowance, the adjusted target was 404. A total of 373 participants were enrolled; although below the adjusted target, this exceeded the minimum required sample of 363, with the shortfall attributable to the limited number of eligible patients available during the study period. The achieved sample was therefore considered adequate for the study objectives. Simple random sampling was employed. The outpatient clinic attendance register served as the sampling frame; confirmed eligible patients were assigned sequential identification numbers and selected using a computer-based random number generator, ensuring each had an equal and independent probability of selection.
Data Collection
Data were collected using a semi-structured questionnaire covering sociodemographic, clinical, and behavioural characteristics. The questionnaire was translated into Somali and back-translated into English by two independent bilingual professional translators to ensure linguistic validity; discrepancies between versions were resolved by consensus.
Medication adherence was measured using the 8-item Morisky Medication Adherence Scale (MMAS-8),17 a widely validated tool for assessing adherence to prescribed medications. The instrument was administered under a non-transferable academic licensing agreement granted by the copyright holder, Dr. Donald E. Morisky (License No. 2881–6032-1100-7852-8584). As no pre-existing validated Somali version of the MMAS-8 was available at the time of the study, the instrument was translated into Somali following the same forward-and-back-translation procedure described above, with discrepancies resolved by consensus to ensure conceptual and linguistic equivalence. The original validated MMAS-8 scoring procedure was strictly followed as specified by the copyright holder.17 The internal consistency of the MMAS-8 in the current study sample was evaluated using Cronbach’s alpha (α = 0.78) confirming acceptable reliability. Items 1 to 7 were dichotomous (yes/no) and item 8 used a five-point Likert-scale response format.
Operational Definitions
Hypertension was defined as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg.18,19 For the purposes of binary logistic regression, MMAS-8 scores were dichotomised: participants scoring 6–8 were classified as adherent (high or moderate adherence) and those scoring below 6 as non-adherent (low adherence). This threshold is consistent with commonly applied adherence criteria corresponding to approximately 80% or greater medication-taking coverage, as referenced in the chronic disease adherence literature.20 Uncontrolled blood pressure was defined as systolic BP ≥140 mmHg or diastolic BP ≥90 mmHg.21
Statistical Analysis
Data were analysed using IBM SPSS version 27 (IBM Corp., Armonk, NY, USA). Descriptive statistics (frequencies and percentages) were computed for all variables. Bivariable analysis using Pearson chi-square tests was performed to assess associations between independent variables and medication adherence. Variables with a p-value below 0.25 in bivariable analysis, together with those considered clinically plausible based on prior literature (including variables with p-values approaching the threshold, such as CKD and sex), were entered simultaneously into a multivariable binary logistic regression model to identify independent predictors of adherence, following the approach recommended by Hosmer et al22 Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) are reported, with statistical significance defined at p < 0.05. Multicollinearity among independent variables was examined using variance inflation factors (VIF); all VIF values were below 3.0, indicating no problematic collinearity. Model fit was evaluated using the Hosmer–Lemeshow goodness-of-fit test (χ2 = 6.73, df = 8, p = 0.472), which confirmed adequate model fit.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of SIMAD University, Mogadishu, Somalia (Ref. No.: 2023/SU-IRB/FMHS/P058) and from the Human Research Ethics Committee at Mogadishu Somali-Turkey Recep Tayyip Erdogan Training and Research Hospital. Written informed consent was obtained from all participants, who were assured of confidentiality and their right to withdraw at any time without consequence.
Results
Sociodemographic and Clinical Characteristics of Participants
A total of 373 adult hypertensive outpatients were enrolled. Of these, 202 (54.2%) were male, and the majority were aged 45 years or above (171 (45.8%) aged ≥65 years; 163 (43.7%) aged 45–64 years). Most participants were married (75.3%), unemployed (70.5%), and had no formal education (55.2%). Nearly three-quarters (71.8%) had been diagnosed with hypertension for more than five years. The most common comorbidity was T2DM, present in 170 participants (45.6%). Sociodemographic and clinical characteristics are presented in Tables 1 and 2, respectively.
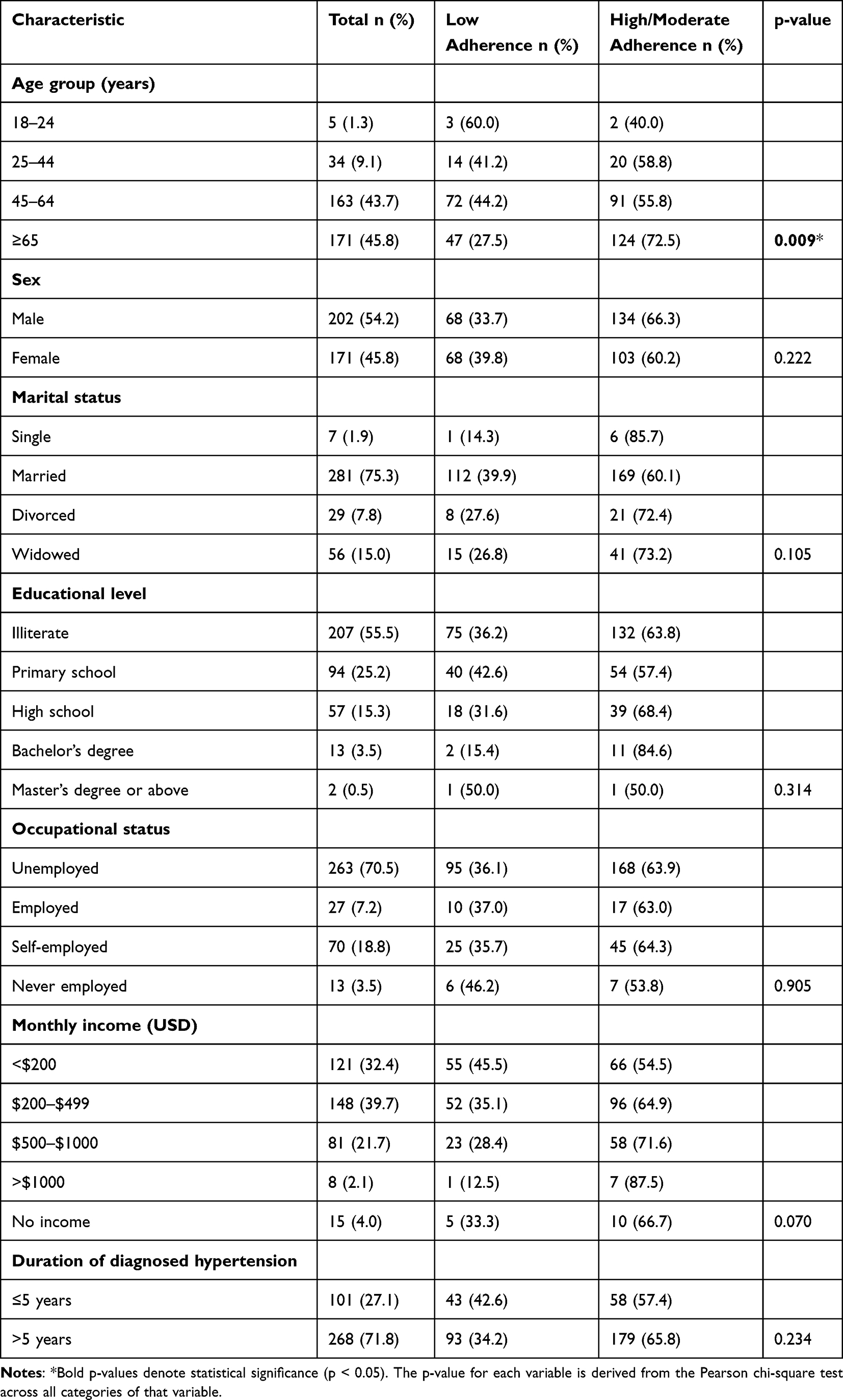 |
Table 1 Bivariable Analysis of Sociodemographic Characteristics and Antihypertensive Medication Adherence, Mogadishu Somali-Turkey Training and Research Hospital (n = 373) |
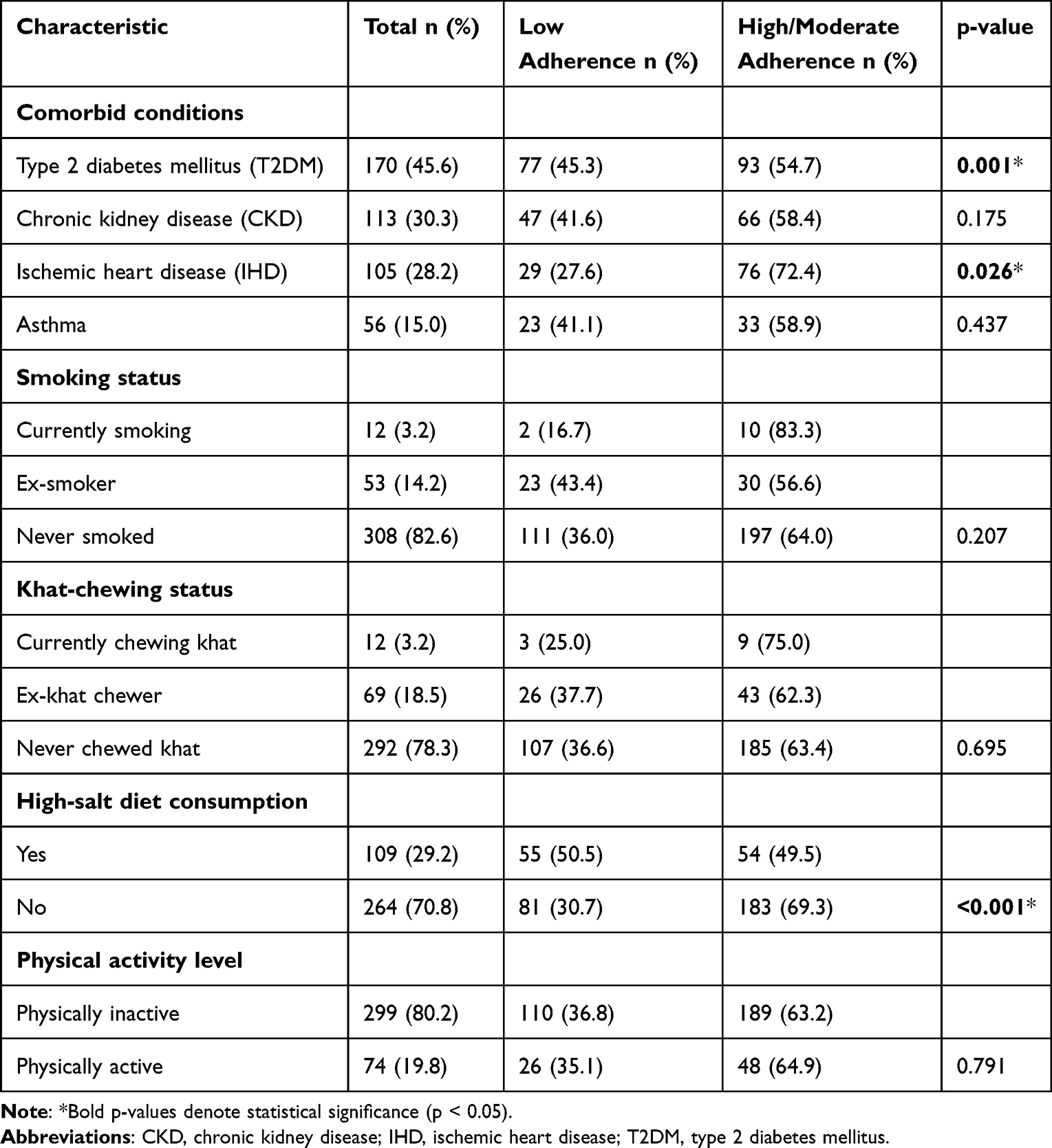 |
Table 2 Bivariable Analysis of Clinical Comorbidities and Lifestyle Factors in Relation to Antihypertensive Medication Adherence (n = 373) |
Prevalence of Antihypertensive Medication Adherence
Of the 373 participants, 237 (63.5%) were classified as having high or moderate adherence to antihypertensive medication, while 136 (36.5%) were classified as having low adherence, based on MMAS-8 scores. High adherence (score = 8) was observed in 74 participants (19.8%), moderate adherence (score ≥6 to <8) in 163 (43.7%), and low adherence (score <6) in 136 (36.5%). For regression analysis, high and moderate adherence categories were combined into a single “adherent” group (score ≥6), consistent with the standard MMAS-8 dichotomisation approach.17 The adherence distribution is presented in Figure 1.
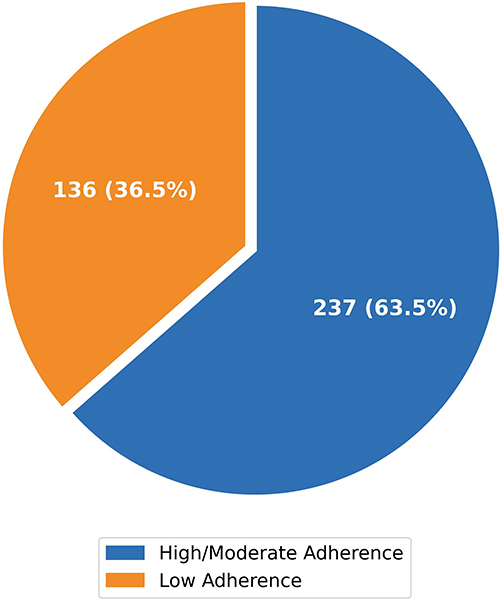 |
Figure 1 Distribution of antihypertensive medication adherence levels among hypertensive outpatients, Mogadishu Somali-Turkey Training and Research Hospital, 2024 (n = 373). |
Bivariable Analysis
Among sociodemographic variables, age was the only significant factor associated with adherence (p = 0.009), with the highest adherence observed in participants aged ≥65 years (72.5%). Sex, marital status, educational level, occupational status, monthly income, and duration of hypertension were not significantly associated with adherence in bivariable analysis (all p > 0.05), although monthly income showed a borderline trend (p = 0.070). Full results are presented in Table 1.
Among clinical and lifestyle variables, T2DM (p = 0.001), IHD (p = 0.026), and high-salt diet consumption (p < 0.001) were significantly associated with adherence. Participants with T2DM had lower adherence (54.7%) compared with those without (70.9%), while participants with IHD had higher adherence (72.4%) than those without (60.1%). Participants reporting a high-salt diet had lower adherence (49.5%) than those who did not (69.3%). CKD, asthma, smoking status, khat-chewing, and physical activity were not significantly associated with adherence in bivariable analysis. Results are presented in Table 2.
Multivariable Logistic Regression Analysis
All variables with p < 0.25 in bivariable analysis were entered into the multivariable logistic regression model (n = 10 variables). After adjustment, four variables were independently and significantly associated with high/moderate medication adherence (Table 3). Age 45–64 years, female sex, and CKD did not retain statistical significance after adjustment, indicating that their bivariable associations were largely explained by other variables in the model.
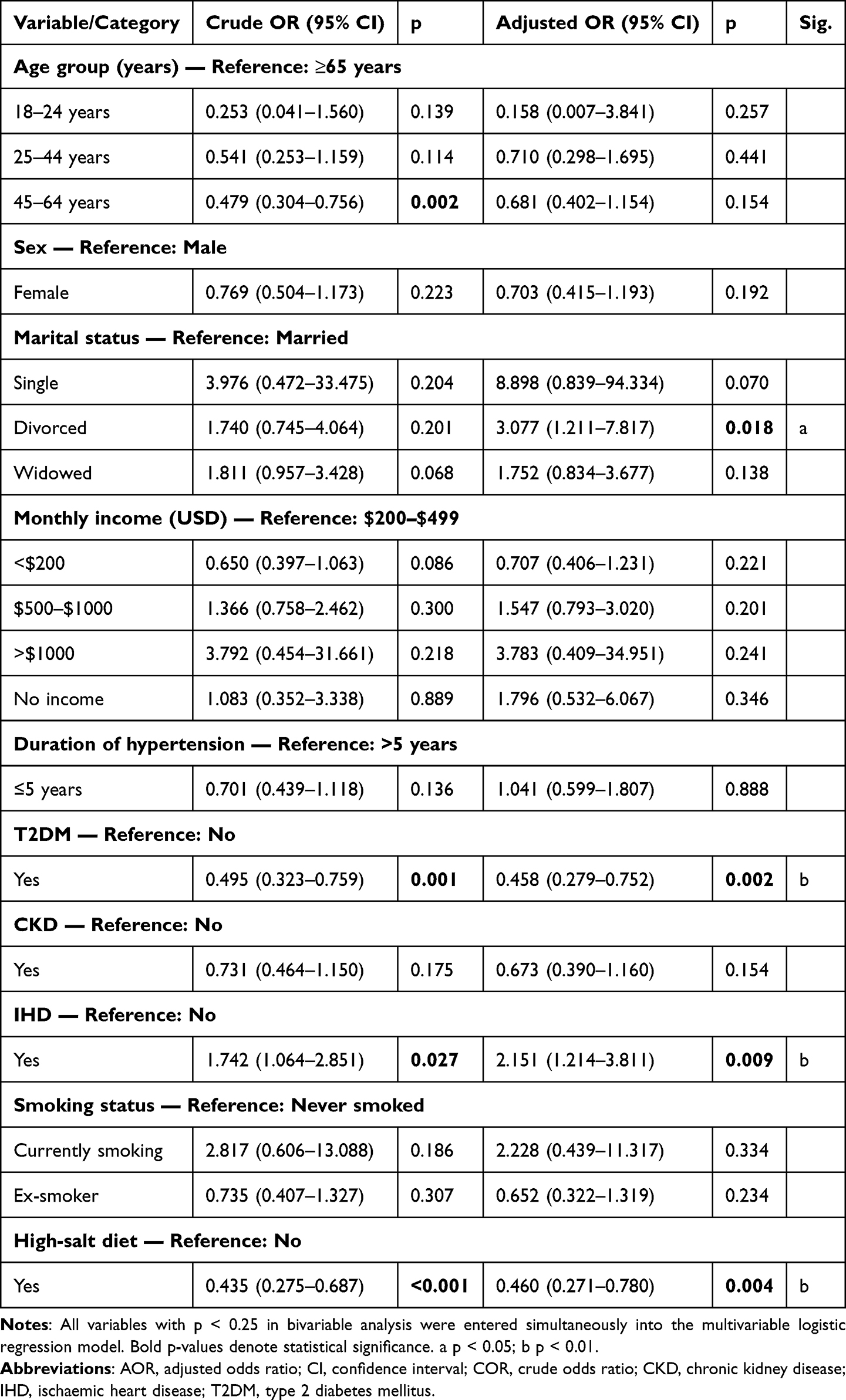 |
Table 3 Multivariable Logistic Regression Analysis of Factors Associated with Antihypertensive Medication Adherence (n = 373) |
Participants with T2DM had 54.2% lower odds of adherence compared with those without (AOR = 0.458; 95% CI: 0.279–0.752; p = 0.002). Participants reporting high-salt diet consumption had 54.0% lower odds of adherence compared with those who did not (AOR = 0.460; 95% CI: 0.271–0.780; p = 0.004). Participants with IHD were 2.15 times more likely to demonstrate adherence than those without IHD (AOR = 2.151; 95% CI: 1.214–3.811; p = 0.009). Divorced participants had higher odds of adherence compared with married participants (AOR = 3.077; 95% CI: 1.211–7.817; p = 0.018); however, this finding should be interpreted with caution given the small number of divorced participants (n = 29) and the correspondingly wide confidence interval. Full results are presented in Table 3.
Discussion
Previous research on hypertension in Somalia has focused predominantly on prevalence, risk factors, and knowledge, attitudes, and practices (KAP), with no prior investigation of antihypertensive medication adherence.10,13–15,23 This study addresses that important gap, and found that nearly two-thirds of participants demonstrated adequate adherence; a level that, while encouraging relative to the national hypertension control rate of 10%,10 still leaves more than one-third of patients at risk of treatment failure and its cardiovascular consequences.
The adherence prevalence observed here is broadly consistent with comparable sub-Saharan African settings, including Ethiopia (61.8%)16 and Eritrea (64.6%),23 suggesting that the challenge of sustaining adherence may be shared across countries with similar socioeconomic and health system constraints. Markedly lower rates reported in Uganda (17%) and Gambia (27%),24,25 underscore the regional variability of adherence behaviours, likely reflecting differences in study design, measurement tools, categorisation thresholds, and facility type. The study setting; a well-resourced, internationally supported referral hospital, may itself contribute to the relatively favourable adherence rates observed, as patients attending tertiary facilities typically receive more structured follow-up, specialist oversight, and institutional support for medication access than those managed in primary or community-based settings. These structural advantages should be considered when interpreting and generalising these findings.
Multivariable logistic regression identified four independent predictors of adherence: T2DM and high-salt diet consumption were each associated with lower adherence, while IHD and divorced marital status were each associated with higher adherence. Notably, age group 45–64 years, female sex, and CKD, which each showed associations in bivariable analysis, did not retain significance after full adjustment, indicating that their apparent effects were largely explained by other variables in the model. After adjustment for clinical comorbidities and lifestyle factors, the demographic characteristics examined, including age group, sex, educational level, and income, did not independently predict adherence in this multivariable model. This does not imply that demographic factors are unimportant, but rather that their influence in this setting may be mediated through clinical and behavioural pathways.
The independent association of T2DM with lower adherence reflects a well-recognised challenge in concurrent chronic disease management. When hypertension and T2DM co-exist, patients are typically prescribed multiple agents across both conditions, creating a complex pill burden that increases the risk of adherence fatigue and regimen simplification.26,27 While some studies from higher-income settings report that patients with diabetes maintain stronger adherence due to heightened cardiovascular risk awareness,28 the pattern observed here is more consistent with evidence from low-resource contexts where integrated chronic disease management infrastructure is limited or absent.24 In Somalia, patients managing both conditions simultaneously face compounding burdens, multiple prescribers, fragmented pharmacy access, and out-of-pocket costs, that make sustained adherence particularly difficult.
Patients with IHD demonstrated significantly higher adherence than those without, a finding consistent with the disease severity hypothesis of medication behaviour.29 While patients with IHD, like those with T2DM, often receive polypharmacy regimens (including antiplatelet agents, statins, and beta-blockers alongside antihypertensives), the key distinction lies in the perceived immediacy and salience of risk. A diagnosis of IHD, particularly one preceded by an acute cardiac event, creates a powerful and durable motivational cue for adherence: patients are acutely aware that lapses may carry life-threatening consequences. By contrast, T2DM patients managing a largely asymptomatic condition may be more vulnerable to adherence fatigue over time when faced with a complex regimen.27,30 Additionally, IHD patients in this setting receive specialist follow-up more consistently as part of secondary prevention protocols, reinforcing adherence through regular clinical review. The clinical encounter surrounding an acute cardiovascular diagnosis therefore represents an important teachable moment that should be systematically leveraged to reinforce adherence to all prescribed medications.
The association between divorced marital status and higher adherence, relative to married participants, is a statistically significant but unexpected finding that must be interpreted with considerable caution. The divorced subgroup comprised only 29 participants, yielding wide confidence intervals that reflect substantial imprecision in this estimate, and the possibility of a chance finding cannot be excluded. While marriage is frequently cited as protective for chronic disease management through spousal support,31–33 one plausible explanation is that individuals managing their health independently following marital dissolution may develop stronger personal health routines. However, residual confounding by unmeasured variables, including living arrangements, financial circumstances, healthcare-seeking behaviour, and social networks, cannot be adequately addressed with the available data. The Somali cultural context further complicates interpretation, as the social and economic circumstances of divorced individuals in Somalia differ substantially from those described in Western literature.34 This finding should be regarded as hypothesis-generating only, and dedicated research exploring social support, household structure, and adherence in Somali populations is warranted before any clinical inferences are drawn.
The association between habitual high-salt dietary intake and lower adherence is consistent with international evidence,35,36 and is best understood as a marker of broader health behaviour clustering rather than a direct causal pathway. Patients who habitually consume excess sodium may hold health beliefs that downplay the role of pharmacotherapy in blood pressure control, perceiving dietary habits as normative and medications as supplementary.37 In Somalia, high-salt intake is embedded in cultural food practices and is not easily modified through standard clinical advice alone. The co-occurrence of poor dietary habits and low medication adherence points to the importance of addressing both behaviours simultaneously through culturally tailored nutritional counselling integrated into routine hypertension visits.
The absence of independent associations for age, sex, CKD, educational level, occupational status, monthly income, and duration of hypertension after full adjustment is consistent with evidence from other fragile health system settings, suggesting that access constraints and treatment burden may outweigh sociodemographic characteristics as practical barriers in these contexts.8,38,39 Clinicians should therefore not rely on demographic risk profiling alone to identify patients most in need of adherence support.
These findings carry direct implications for hypertension care in Somalia. Adherence risk stratification should be embedded in routine clinic visits, with particular attention to patients managing concurrent T2DM and those reporting dietary risk behaviours. Given the opposing adherence associations of T2DM (lower adherence) and IHD (higher adherence), clinical management should differentiate between these patient groups: for patients with T2DM, active adherence counselling and simplified, reconciled dosing regimens may mitigate polypharmacy burden; for IHD patients, the high adherence motivation should be maintained and extended to all prescribed medications through reinforcement counselling. Culturally adapted dietary counselling, integrated into routine visits, is also warranted. Addressing the structural drivers of non-adherence in Somalia, including out-of-pocket medication costs, fragmented prescribing, and limited continuity of care, requires health system-level responses beyond the clinical encounter.
This study has several limitations. The cross-sectional design precludes causal inference, and single-facility recruitment at a major tertiary referral hospital limits generalisability to patients attending primary or community-level facilities across Somalia. Adherence was measured by self-report using the MMAS-8, which is subject to social desirability bias; this may lead to overestimation of true adherence, and findings should be interpreted accordingly. The small number of participants in certain subgroups reduces the precision of the corresponding estimates and increases the risk of chance findings. The study did not include objective adherence measures (such as pill counts or pharmacy refill records) or data on polypharmacy burden, health literacy, or patient-provider communication quality. Future studies should employ prospective multi-site designs, objective adherence measures, and examine these additional determinants to build a more complete picture of adherence determinants in Somalia.
Conclusion
Suboptimal adherence to antihypertensive medication remains a significant clinical challenge in Mogadishu, with more than one-third of patients failing to meet the adherence threshold. In this multivariable analysis, T2DM and IHD showed opposing associations with adherence reflecting the contrasting motivational dynamics of these comorbidities, while high-salt dietary intake was independently associated with lower adherence, and divorced marital status with higher adherence. The latter finding is based on a small subgroup and should be interpreted with caution. These results, observed within the limitations of a cross-sectional, single-site, self-reported adherence study, indicate that adherence determinants in this setting encompass clinical and behavioural dimensions. Patient-centred hypertension management strategies should address concurrent comorbidity burden, particularly the co-management of hypertension and T2DM, and promote healthy dietary behaviours through culturally appropriate counselling. Acute cardiovascular diagnoses should be leveraged as structured opportunities to reinforce long-term medication adherence. Addressing the structural drivers of non-adherence within the Somali health system is essential to achieving meaningful improvements in blood pressure control. Future prospective, multi-site research with objective adherence measures is needed to extend these findings.
Abbreviations
AOR, adjusted odds ratio; BP, blood pressure; CI, confidence interval; COR, crude odds ratio; CKD, chronic kidney disease; IHD, ischemic heart disease; MMAS-8, Morisky Medication Adherence Scale-8; SBP, systolic blood pressure; DBP, diastolic blood pressure; SPSS, Statistical Package for Social Sciences; T2DM, type 2 diabetes mellitus; VIF, variance inflation factor; WHO, World Health Organization.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board (IRB) of SIMAD University, Mogadishu, Somalia (Ref. No.: 2023/SU-IRB/FMHS/P058). Separate ethical approval from the Human Research Ethics Committee at Mogadishu Somalia-Turkey Recep Tayyip Erdogan Training and Research Hospital was also obtained. Written informed consent was received from all individual participants involved in the study. Participants were informed about the study objectives, their right to confidentiality, and their right to withdraw consent at any time without repercussions.
Acknowledgments
The authors express their gratitude to all participants and hospital staff involved in the conduct of this study, as well as to the Ethics and Research Committee at SIMAD University and Mogadishu Somali-Turkey Training and Research Hospital. MMAS® 2006 used with permission www.adherence.cc.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
All authors have declared that this study did not receive any funding or grants from any authority or institution.
Disclosure
All authors have declared that there are no conflicts of interest associated with this study.
References
1. Burnier M, Egan BM. Adherence in hypertension. Circ Res. 2019;124(7):1124–12. PubMed PMID: 30920917. doi:10.1161/CIRCRESAHA.118.313220
2. Abbafati C, Abbas KM, Abbasi-Kangevari M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1223. PubMed PMID: 33069327. doi:10.1016/S0140-6736(20)30752-2
3. Zhou B, Carrillo-Larco RM, Danaei G, et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957. PubMed PMID: 34450083. doi:10.1016/S0140-6736(21)01330-1
4. Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365(9455):217–223. PubMed PMID: 15652604. doi:10.1016/s0140-6736(05)17741-1
5. Haley W, Shawl F, Charles Sternbergh W, et al. Non-adherence to antihypertensive guidelines in patients with asymptomatic carotid stenosis. J Stroke Cerebrovasc Dis. 2021;30(8):105918. PubMed PMID: 34148021. doi:10.1016/J.JSTROKECEREBROVASDIS.2021.105918
6. Curtin SC. Stroke death rates among adults ages 45-64 by region and race and hispanic origin: United States, 2002-2022. NCHS Data Brief. 2024;505. PubMed PMID: 39302269. doi:10.15620/CDC/158326
7. Abbas H, Kurdi M, de Vries F, et al. Factors associated with antihypertensive medication non-adherence: a cross-sectional study among Lebanese hypertensive adults. Patient Prefer Adherence. 2020;14:663. PubMed PMID: 32280203. doi:10.2147/PPA.S238751
8. Mebrahtu G, Moleki MM, Achila OO, Seyoum Y, Adnoy ET, Ovberedjo M. Antihypertensive medication adherence and associated factors: a cross-sectional analysis of patients attending a national referral hospital in Asmara, Eritrea. Patient Prefer Adherence. 2021;15:2619. PubMed PMID: 34848951. doi:10.2147/PPA.S319987
9. Lawson AJ, Hameed MA, Brown R, et al. Nonadherence to antihypertensive medications is related to pill burden in apparent treatment-resistant hypertensive individuals. J Hypertens. 2020;38(6):1165–1173. PubMed PMID: 32141970. doi:10.1097/HJH.0000000000002398
10. Farih OA, Ali AO, Abokor AH, Ali MA, Egge AAA, Muse AH. Prevalance and determinants of hypertension among adults in Somalia using Somalia demographic health survey data, SDHS 2020. Curr Probl Cardiol. 2024;49(11):102783. PubMed PMID: 39127429. doi:10.1016/J.CPCARDIOL.2024.102783
11. Mediterranean WHOrganizationRO for the E. Understanding the private health sector: in Somalia [Internet]. 2024. Available from: https://iris.who.int/handle/10665/377333.
12. Osman NH, Abdi AM, Jimale AM, et al. Healthcare facility accreditation status and associated factors in Somalia: evidence from the 2022–2023 harmonized health facility assessment. BMC Health Serv Res. 2026;26(1):581. PubMed PMID: 41845417. doi:10.1186/S12913-026-14377-6
13. Mohamud MFY. Clinico-epidemiological profile and risk factors of hypertensive crisis among patients attended at a tertiary care hospital in Somalia. Sci Rep. 2023;13(1):447. PubMed PMID: 36624249. doi:10.1038/S41598-023-27683-4
14. Ahmed SH, Meyer HE, Kjøllesdal MK, et al. The prevalence of selected risk factors for non-communicable diseases in Hargeisa, Somaliland: a cross-sectional study. BMC Public Health. 2019;19(1):878. PubMed PMID: 31272414. doi:10.1186/S12889-019-7101-X
15. Mohamud MFY, Turfan S, Mohamed HH, et al. Exploring the prevalence, clinical spectrum, and determinants of uncontrolled hypertension in the emergency department: insights from a hospital-based study in Somalia. Curr Probl Cardiol. 2024;49(7):102589. PubMed PMID: 38701996. doi:10.1016/j.cpcardiol.2024.102589
16. Asgedom SW, Atey TM, Desse TA. Antihypertensive medication adherence and associated factors among adult hypertensive patients at Jimma University specialized hospital, southwest Ethiopia. BMC Res Notes. 2018;11(1):27. PubMed PMID: 29335003. doi:10.1186/S13104-018-3139-6
17. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348. PubMed PMID: 18453793. doi:10.1111/J.1751-7176.2008.07572.X
18. Unger T, Borghi C, Charchar F, et al. 2020 international society of hypertension global hypertension practice guidelines. Hypertension. 2020;75(6):1334–1357. PubMed PMID: 32370572. doi:10.1161/HYPERTENSIONAHA.120.15026;WGROUP:STRING:PUBLICATION
19. Prevalence of raised blood pressure (SBP≥140 OR DBP≥90) [Internet]. Available from: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/2386.
20. Gardezi SKM, Aitken WW, Jilani MH. The impact of non-adherence to antihypertensive drug therapy. Healthcare. 2023;11(22):2979. doi:10.3390/HEALTHCARE11222979/S1
21. Makukule A, Modjadji P, Thovhogi N, Mokgalaboni K, Kengne AP. Uncontrolled hypertension, treatment, and predictors among hypertensive out-patients attending primary health facilities in Johannesburg, South Africa. Healthcare. 2023;11(20):2783. PubMed PMID: 37893857. doi:10.3390/HEALTHCARE11202783
22. Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression: Third Edition. 2013:1–510. doi:10.1002/9781118548387
23. Hareri H, Gedefaw M, Simeng B. Assessment of prevalence and associated factors of adherence to anti-hypertensive agents among adults on follow up in Adama Referal hospital, East Shoa, Ethiopia-cross sectional study. Int J Curr Microbiol App Sci. 2014;3(1):760.
24. Mugwano I, Kaddumukasa M, Mugenyi L, et al. Poor drug adherence and lack of awareness of hypertension among hypertensive stroke patients in Kampala, Uganda: a cross sectional study. BMC Res Notes. 2016;9(1):3. PubMed PMID: 26725042. doi:10.1186/S13104-015-1830-4
25. Van Der Sande MAB, Milligan PJM, Nyan OA, et al. Blood pressure patterns and cardiovascular risk factors in rural and urban gambian communities. J Hum Hypertens. 2000;14(8):489–496. PubMed PMID: 10962516. doi:10.1038/SJ.JHH.1001050
26. An J, Nichol MB. Multiple medication adherence and its effect on clinical outcomes among patients with comorbid type 2 diabetes and hypertension. Med Care. 2013;51(10):879–887. PubMed PMID: 23929398. doi:10.1097/MLR.0B013E31829FA8ED
27. Tiv M, Viel JF, Mauny F, et al. Medication adherence in type 2 diabetes: the ENTRED study 2007, a French population-based study. PLoS One. 2012;7(3):e32412. PubMed PMID: 22403654. doi:10.1371/JOURNAL.PONE.0032412
28. Al-Maskari A, Al-Maamari Q, Al-Abdali M, Al-Shaaibi H, Nadar SK. Adherence to medications in patients with ischaemic heart disease in Oman. Sultan Qaboos Univ Med J. 2024;24(1):109. PubMed PMID: 38434452. doi:10.18295/SQUMJ.7.2023.045
29. Polonsky WH, Henry RR. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence. 2016;10:1299. PubMed PMID: 27524885. doi:10.2147/PPA.S106821
30. García-Pérez LE, Álvarez M, Dilla T, Gil-Guillén V, Orozco-Beltrán D. Adherence to therapies in patients with type 2 diabetes. Diab Ther. 2013;4(2):175. PubMed PMID: 23990497. doi:10.1007/S13300-013-0034-Y
31. Molloy GJ, Hamer M, Randall G, Chida Y. Marital status and cardiac rehabilitation attendance: a meta-analysis. Eur J Cardiovasc Prev Rehabil. 2008;15(5):557–561. PubMed PMID: 18800004. doi:10.1097/HJR.0B013E3283063929
32. Franks MM, Wehrspann E, August KJ, Rook KS, Parris Stephens MA. Chronic disease management in older couples: spousal support versus control strategies. In: Couple Relationships in the Middle and Later Years: Their Nature, Complexity, and Role in Health and Illness. 2016:303–323. doi:10.1037/14897-016
33. August KJ, Sorkin DH. Marital status and gender differences in managing a chronic illness: the function of health-related social control. Soc Sci Med. 2010;71(10):1831. PubMed PMID: 20889249. doi:10.1016/J.SOCSCIMED.2010.08.022
34. Omar YS. The state of marriage in somalia, djibouti, and comoros. Gulf Studies. 2024;17:217–261. doi:10.1007/978-981-97-7620-7_4/TABLES/2
35. Dietary salt intake and hypertension in an urban south Indian population--[CURES - 53] - PubMed [Internet]. Available from: https://pubmed.ncbi.nlm.nih.gov/17879493/.
36. Shim JS, Heo JE, Kim HC. Factors associated with dietary adherence to the guidelines for prevention and treatment of hypertension among Korean adults with and without hypertension. Clin Hypertens. 2020;26(1):5. PubMed PMID: 32190348. doi:10.1186/S40885-020-00138-Y
37. Grillo A, Salvi L, Coruzzi P, Salvi P, Parati G. Sodium Intake and Hypertension. Nutrients. 2019;11(9):1970. PubMed PMID: 31438636. doi:10.3390/NU11091970
38. Lor M, Koleck TA, Bakken S, Yoon S, Dunn Navarra AM. Association between health literacy and medication adherence among hispanics with hypertension. J Racial Ethn Health Disparities. 2019;6(3):517–524. PubMed PMID: 30607576. doi:10.1007/S40615-018-00550-Z
39. Wan J, Wu Y, Ma Y, Tao X, Wang A. Predictors of poor medication adherence of older people with hypertension. Nurs Open. 2022;9(2):1370. PubMed PMID: 35094495. doi:10.1002/NOP2.1183
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence and Blood Pressure Control Among Hypertensive Outpatients Attending a Tertiary Cardiovascular Hospital in Tanzania: A Cross-Sectional Study
Pallangyo P, Komba M, Mkojera ZS, Kisenge PR, Bhalia S, Mayala H, Kifai E, Richard MK, Khanbhai K, Wibonela S, Millinga J, Yeyeye R, Njau NF, Odemary TK, Janabi M
Integrated Blood Pressure Control 2022, 15:97-112
Published Date: 10 August 2022
A Critical Review of Medication Adherence in Hypertension: Barriers and Facilitators Clinicians Should Consider
Hamrahian SM, Maarouf OH, Fülöp T
Patient Preference and Adherence 2022, 16:2749-2757
Published Date: 7 October 2022
Interventions Incorporating Therapeutic Alliance to Improve Medication Adherence in Black Patients with Diabetes, Hypertension and Kidney Disease: A Systematic Review
Desta R, Blumrosen C, Laferriere HE, Saluja A, Bruce MA, Elasy TA, Griffith DM, Norris KC, Cavanaugh KL, Umeukeje EM
Patient Preference and Adherence 2022, 16:3095-3110
Published Date: 14 November 2022
Patient Pill Organization Strategies and Adherence Measured in a Cross-Sectional Study of Hypertension
Genelin MP, Helmkamp LJ, Steiner JF, Maertens JA, Hanratty R, Vupputuri S, Havranek EP, Dickinson LM, Blair IV, Daugherty SL
Patient Preference and Adherence 2023, 17:817-826
Published Date: 23 March 2023
A Systematic Review of the Hill-Bone Compliance to Blood Pressure Therapy Scale
Commodore-Mensah Y, Delva S, Ogungbe O, Smulcer LA, Rives S, Dennison Himmelfarb CR, Kim MT, Bone L, Levine D, Hill MN
Patient Preference and Adherence 2023, 17:2401-2420
Published Date: 28 September 2023