Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Add-On Therapy with DPP-4 Inhibitors May Improve Renal Function Decline in α-Glucosidase Inhibitor and Metformin Users: A Retrospective Observational Study
Authors Osonoi T, Saito M, Koda N, Douguchi S, Nakano T, Ofuchi K, Katoh M ![]()
Received 22 July 2020
Accepted for publication 2 September 2020
Published 5 October 2020 Volume 2020:13 Pages 3497—3506
DOI https://doi.org/10.2147/DMSO.S273405
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Takeshi Osonoi, Miyoko Saito, Naoya Koda, Satako Douguchi, Takako Nakano, Kensuke Ofuchi, Makoto Katoh
Naka Kinen Clinic, Ibaraki, Japan
Correspondence: Makoto Katoh
Naka Kinen Clinic, 745-5 Nakadai, Naka-Shi, Ibaraki 311-0113, Japan
Tel +81-29-353-2800
Fax +81-29-295-5400
Email [email protected]
Purpose: We retrospectively evaluated the long-term effect of dipeptidyl peptidase (DPP)-4 inhibitors on estimated glomerular filtration rate (eGFR) slopes, and then evaluated the beneficial interaction between DPP-4 inhibitor initiation and baseline use of α-glucosidase inhibitor and/or metformin in patients with diabetic kidney disease.
Patients and Methods: Altogether, 1512 patients with type 2 diabetes were receiving DPP-4 inhibitor therapy over 1 year and were followed up for a maximum of 2 years before and after 7 years of treatment. The decline in renal function was estimated as the slope of the individual linear regression line of eGFR over 2-year follow-up. Prescription data on medications before and after DPP-4 inhibitor treatment were examined.
Results: The mean length of DPP-4 inhibitor treatment was 5.3 ± 2.6 years. The baseline mean eGFR slope (mL/min/1.73m2/year) was − 2.24 ± 6.05. After DPP-4 inhibitor treatment, mean eGFR slope was significantly improved (− 1.53 ± 6.36, P < 0.01) in patients with type 2 diabetes. This effect appeared more pronounced for baseline use of α-glucosidase inhibitor and/or metformin in patients with diabetic kidney disease. These non-users showed a trend towards attenuation or no effects.
Conclusion: In the present study, patients treated with DPP-4 inhibitors had a significantly slower annual loss of kidney function. The benefit appears pronounced in α-glucosidase inhibitor and metformin users with advanced renal dysfunction. These results suggest that the beneficial effects of DPP-4 inhibitors on kidney function may have occurred in the presence of an α-glucosidase inhibitor and/or metformin.
Keywords: DPP-4 inhibitor, α-glucosidase inhibitor, metformin, eGFR slope, type 2 diabetes
Introduction
Patients with type 2 diabetes mellitus are at increased risk for macrovascular and microvascular complications,1 with type 2 diabetes being the leading cause of chronic kidney disease (CKD) development.2 Patients with CKD have higher mortality and adverse cardiovascular (CV) event rates.3 It has been also known that the increases in albuminuria and glomerular filtration rate (GFR) decline are associated with a considerably increased risk of CV disease.4
When used as monotherapy, the commonly used oral glucose-lowering agents in type 2 diabetes: Dipeptidyl peptidase (DPP)-4 inhibitors, have a low risk of hypoglycemia and generally neutral effects on body weight. In addition, DPP-4 inhibitors are tolerable in patients with CKD. However, their efficacy in diabetic complication prevention, especially diabetic kidney disease (DKD), is not well established. Physiologically, DPP-4 is most expressed in the kidneys among all organs,5,6 and some preclinical studies have suggested that DPP-4 inhibitors have some pleiotropic effects, which might be beneficial to the kidney.6–9 However, in clinical trials, the renal protective effects of DPP-4 inhibitors were inconsistent.
Recently, a meta-analysis of the three major DPP-4 inhibitor cardiovascular outcomes trials (CVOTs) suggested that baseline metformin use may have a moderating effect on cardiovascular outcomes in DPP-4 inhibitor use.10 DPP-4 inhibitors prevent the degradation of active glucagon-like peptide-1 (GLP-1),8 and metformin11,12 or α-glucosidase inhibitors13,14 increase circulating GLP-1 levels in clinical studies. Therefore, it is plausible that these drugs could interact synergistically. Nevertheless, it is unknown whether metformin or α-glucosidase inhibitor use may be a beneficial effect on renal function with DPP-4 inhibitor use. Moreover, a majority of these studies only contained short-term follow-up data15–18 and included only one DPP-4 inhibitor drug; thus, they were unable to evaluate the effects according to drug class.
Therefore, we considered it important to examine the long-term effect of DPP-4 inhibitor therapy on estimated GFR (eGFR) slope in daily clinical practice. Moreover, we evaluated the beneficial interaction between DPP-4 inhibitor initiation and baseline use of α-glucosidase inhibitor and/or metformin in patients with DKD.
Patients and Methods
Study Design
We screened 2942 patients with type 2 diabetes who had been taking DPP-4 inhibitors between January 2008 and October 2019 and performed a retrospective observational study of 1512 patients who received DPP-4 inhibitor therapy for at least 1 year and were followed up for a maximum of 2 years before and after 7 years of treatment. We evaluated the changes in eGFR, urinary albumin-to-creatinine ratio (UACR), glycated hemoglobin (HbA1c), body mass index (BMI), blood pressure, and heart rate from baseline to the end of treatment. The study protocol was reviewed and approved by the ethics review committee of the Naka Kinen Clinic. The registration number at the University Hospital Medical Information Network for this study is UMIN000038801. Patient informed consent was obtained in the form of opt-out on the web-site of Naka Kinen Clinic. Those who rejected were excluded. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and the ethical guidelines for medical and health research involving human subjects.
Subjects
The eligibility criteria were as follows: 1) age of 20 years or older, 2) patients identified as having type 2 diabetes, 3) patients who were on DPP-4 inhibitor therapy for more than 1 year, 4) patients who had their eGFR measured at least 1 year before and after DPP-4 inhibitor treatment. The exclusion criteria were as follows: 1) previous or concomitant type 1 diabetes mellitus, 2) patients who were considered ineligible by the principal investigator or investigator for other reasons.
Endpoints
The primary endpoints of this study were changes in eGFR slope and UACR after DPP-4 inhibitor treatment. We calculated eGFR using the age, body weight, gender, and serum creatinine, and the UACR in spot urine samples was calculated from urinary albumin and creatinine (Cr) levels. We calculated the annual eGFR slope as the individual linear regression line of eGFR over 2-year follow-up, and a linear line with at least 3 point data served for detection. The number of eGFR measurements in the baseline period was 3.7 ± 3.0 times/year, and that in the follow-up period was 4.1 ± 3.5 times/year. Patients were classified based on their eGFR categories (G1: >90 mL/min/1.73 m2, G2: <90 and >60 mL/min/1.73 m2, G3a: <60 and >45 mL/min/1.73 m2, G3b: <45 and >30 mL/min/1.73 m2, G4: <30 and >15 mL/min/1.73 m2, or G5: <15 mL/min/1.73 m2) or their UACR categories (normoalbuminuria: <30 mg/gCr, microalbuminuria: >30 and <300 mg/gCr, and macroalbuminuria: >300 mg/gCr) according to the Kidney Disease Improving Global Outcomes (KDIGO) classification who were not on dialysis.19 The secondary endpoints were the statistical interaction between DPP-4 inhibitor initiation and baseline use of α-glucosidase inhibitor and/or metformin in DKD patients, and mean changes in HbA1c, BMI, systolic (SBP) and diastolic blood pressure (DBP), and heart rate before and after 1 year of treatment with DPP-4 inhibitors.
Statistical Analysis
Data in all tables and figures are presented as the arithmetic mean ± standard deviation (SD), except the UACR data, which are presented as the geometric mean with a 95% confidence interval (CI). For the annual eGFR slope, paired t-tests were used to analyze differences between pre- and post-treatment. A comparison between the mean value 1 year before and after treatment for UACR, HbA1c, body weight, SBP and DBP, and heart rate, was performed using a paired t-test. A two-sided P value <0.05 was considered statistically significant, and the two-sided 95% CI was also calculated. Analyses were conducted with Prism 8.3 software.
Results
Patient Disposition and Baseline Characteristics
The patient dispositions are shown in Figure 1. Of the 2942 patients screened, 1512 completed the study, including 495 patients with CKD (defined as an eGFR <60 mL/min/1.73 m2). There were 966 males (63.9%) and 546 females (36.1%), with a mean age of 66.6 ± 10.7 years, mean BMI of 22.9 ± 3.1 kg/m2, mean HbA1c of 7.2 ± 1.0% (55.6 ± 11.4 mmol/mol), mean eGFR of 67.5 ± 19.2 mL/min/1.73 m2, mean UACR of 18.8 (4.7–75.6) mg/gCr, mean SBP of 131.9 ± 16.2 mmHg, mean DBP of 74.4 ± 11.2 mmHg, and mean heart rate of 79.7 ± 13.7 beats/min. Patients with eGFR stage G1 were younger (a mean age of 57.8 years) than that with stage G2 to G5 (mean ages of >65 years), and higher mean HbA1c (7.6%) than that with stage G2 to G5 (range of mean HbA1c from 6.9% to 7.2%).
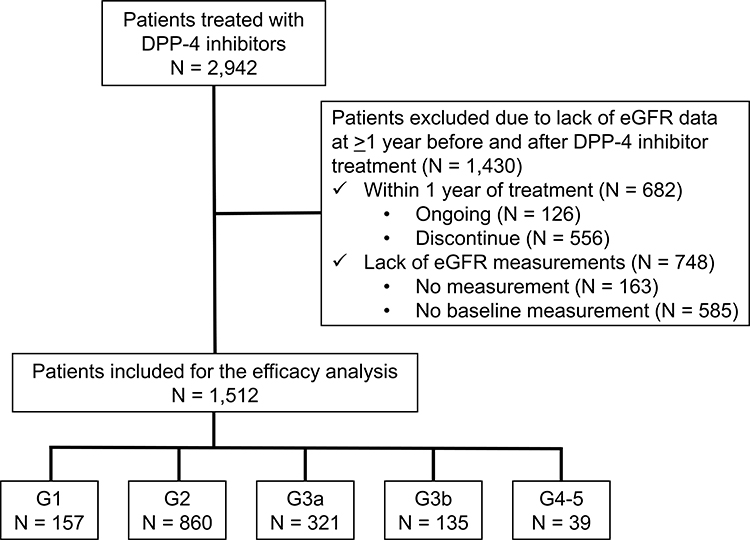 |
Figure 1 Patient disposition. |
The mean length of DPP-4 inhibitor treatment was 5.3 ± 2.6 years. Eight DPP-4 inhibitors were used alogliptin (44.7%), sitagliptin (42.2%), teneligliptin (5.0%), anagliptin (4.4%), linagliptin (1.5%), vildagliptin (1.5%), saxagliptin (0.5%), and trelagliptin (0.3%). The number of prescriptions per patient before and 1 year after the initiation of DPP-4 inhibitor therapy ranged from 1.9 ± 1.0 to 2.5 ± 1.0. From baseline to 1 year after the initiation of treatment, the use of an α-glucosidase inhibitor (from 76.3% to 69.6%), biguanide (61.7% to 56.3%), insulin (18.3% to 14.6%), thiazolidine (13.1% to 4.4%), glinide (11.2% to 1.2%), and sulfonylureas (10.4% to 2.1%) declined, whereas the use of a sodium-glucose cotransporter 2 (SGLT2) inhibitor (0.9% to 1.4%) increased. Moreover, the treatment of 1.1% of patients were switched from a GLP-1 receptor agonist to a different therapy.
Changes in eGFR Slope for Each Patient Using the Linear Regression Coefficient and Analyzed by Baseline GFR Categories and Treatment Drugs
The time-course of eGFR at the period for a maximum of 2 years before and after 7 years of treatment with DPP-4 inhibitors is shown in Figure 2A. Renal function decline was estimated as the slope of the individual linear regression line of eGFR over 2-year follow-up. The baseline eGFR slope was −2.24 ± 6.05 mL/min/1.73 m2/year, and DPP-4 inhibitor treatment significantly improved the eGFR slope to −1.53 ± 6.36 mL/min/1.73 m2/year (P < 0.01). Patients were classified into 5 categories based on their eGFR, and their eGFR slopes were determined. The decline in the mean eGFR at stages G2 to G5 was slightly slower following the DPP-4 inhibitor treatment compared with before treatment initiation, but patients with eGFR stage G1were associated with accelerated eGFR decline (Figure 2B). The eGFR slopes at stages G1 to G5 before and after DPP-4 inhibitor treatment are shown in Figure 3. DPP-4 inhibitor therapy significantly improved the eGFR slope at stages G2 to G3b and tended to improve the slope (P = 0.05) at stage G4–5, but the slope at stage G1 was significantly steeper (P < 0.05).
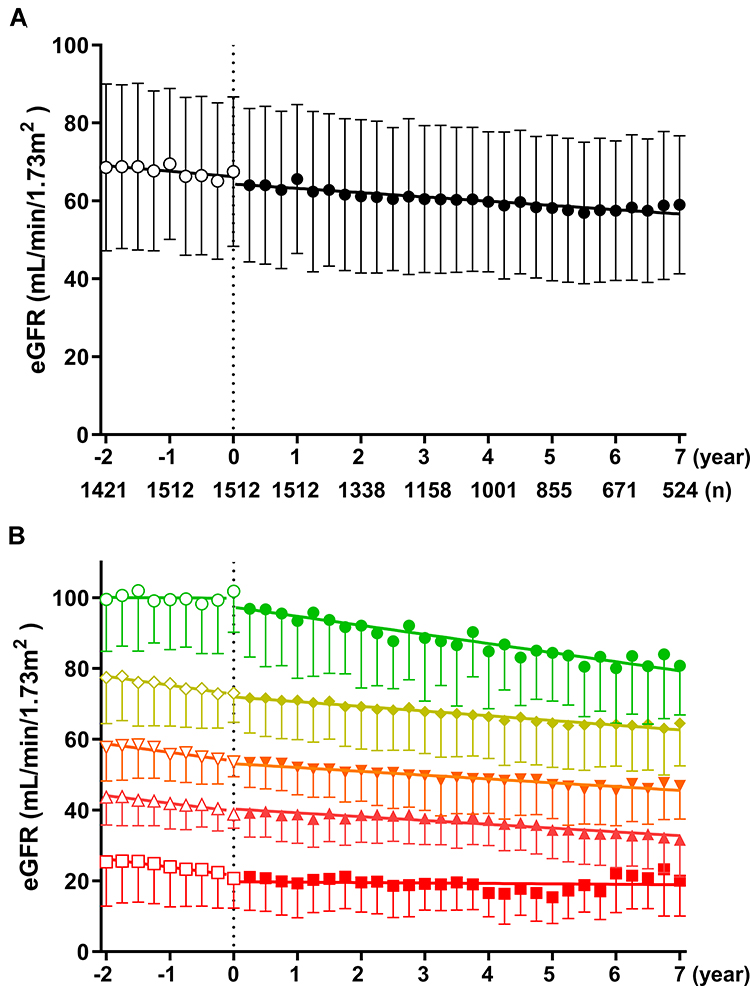 |
Figure 2 Effect of DPP-4 inhibitors on decline in eGFR in all patients (A) and patients with stages G1 to G5 chronic kidney disease (B). (A) Open and closed circles represent data from pre- and post-treatment with DPP-4 inhibitors, respectively. (B) Open and closed symbols represent data from pre- and post-treatment with DPP-4 inhibitors, respectively. Circle, G1; rhombus, G2; inverted triangle, G3a; triangle, G3b; square, G4–5. Data are the mean ± SD. |
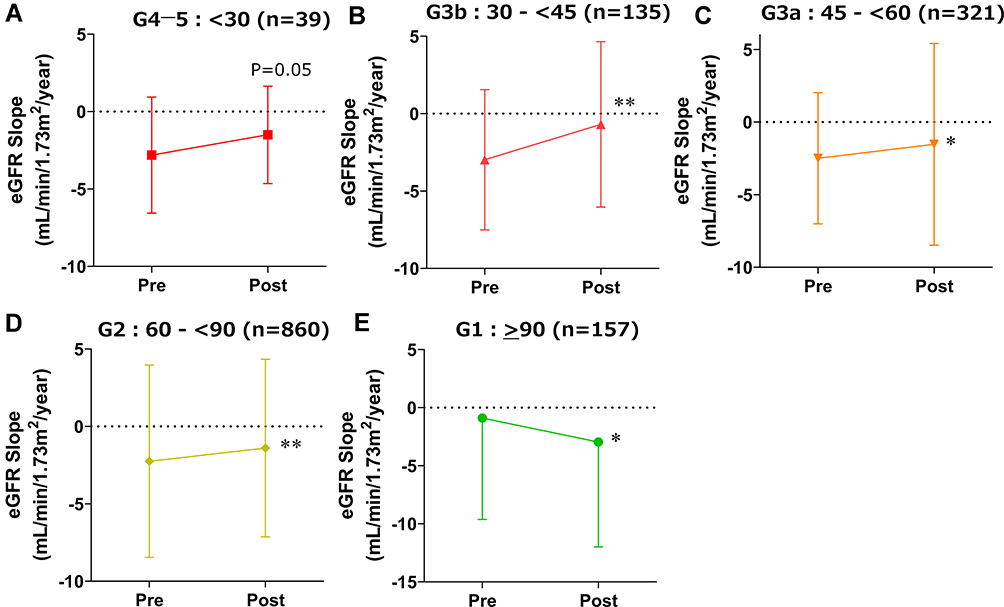 |
Figure 3 Effect of DPP-4 inhibitors on eGFR slope in patients with stages G4–5 (A), G3b (B), G3a (C), G2 (D), and G1 (E). Data are the mean ± SD. *P < 0.05, **P < 0.01 vs pre-value by paired t-test. |
Most of the patients with CKD (78.2%) were receiving either an α-glucosidase inhibitor or metformin from 1 year before to 1 year after the initiation of the DPP-4 inhibitor treatment. We evaluated the effect of DPP-4 inhibitors on eGFR slope with or without an α-glucosidase inhibitor and/or metformin (Table 1). eGFR slopes with both an α-glucosidase inhibitor and metformin were significantly improved after DPP-4 inhibitor administration compared with the pretreatment period; however, no improvement was seen in those without these treatments (Table 1).
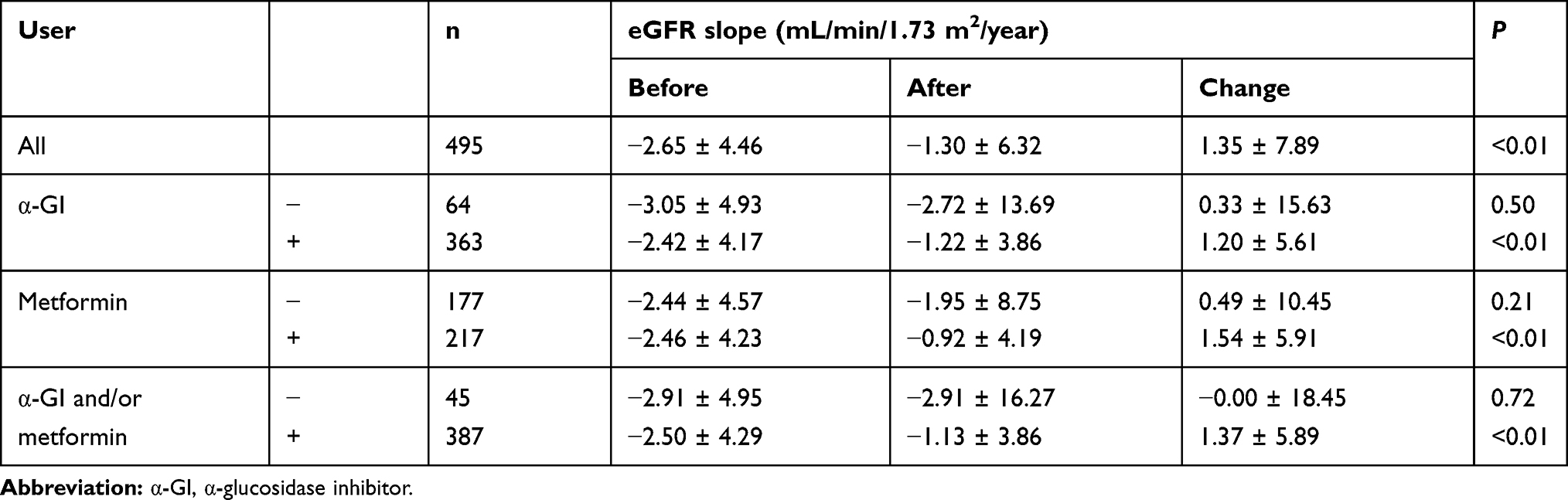 |
Table 1 Effect of DPP-4 Inhibitors on eGFR Slope with or without an α-Glucosidase Inhibitor and/or Metformin |
From 1 year before to 1 year after the initiation of the DPP-4 inhibitor treatment, 40.8% of the patients with CKD were receiving an angiotensin II receptor blocker. Regardless of the presence (from −2.66 ± 4.49 to −1.27 ± 4.11 mL/min/1.73 m2/year, P < 0.01, n = 202) or absence (from −2.53 ± 4.42 to −0.89 ± 8.57 mL/min/1.73 m2/year, P < 0.05, n = 180) of an angiotensin II receptor blocker, DPP-4 inhibitor therapy significantly improved the eGFR slope. However, given that only six patients (1.2%) with CKD were receiving an SGLT2 inhibitor, differences in eGFR slope between with and without SGLT2 inhibitor were not clear.
Changes in UACR
Changes in UACR determined by the analysis of baseline UACR categories before and after DPP-4 inhibitor treatment are shown in Figure 4A and B. From the comparison of the means before and 1 year after the initiation of DPP-4 inhibitor therapy, UACR was significantly reduced (from 20.9 [95% CI: 5.6–78.2] to 20.1 [5.2–77.6] mg/gCr, P < 0.05) (Figure 4B), and its effect was sustained for at least 7 years of treatment (Figure 4A). When analyzed according to baseline albuminuria, UACR was reduced; however, it did not differ significantly for any UACR categories in comparison to that before treatment (normoalbuminuria: <30 mg/gCr, microalbuminuria: >30 and <300 mg/gCr, and macroalbuminuria: >300 mg/gCr) (Figure 4B).
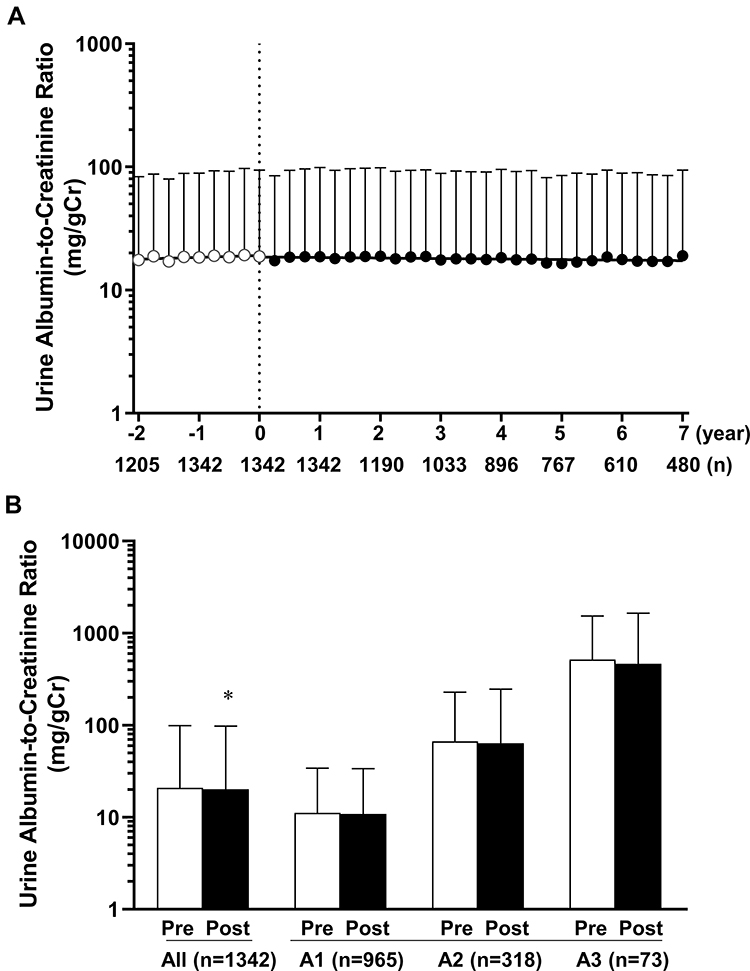 |
Figure 4 The time-course of UACR before and after the treatment with DPP-4 inhibitors in all patients (A) and effect of DPP-4 inhibitors on UACR by comparison of the means of administration before and after 1 year in all patients and those with stages A1 to A3 (B). Data are the geometric mean with a 95% CI. *P < 0.05 vs pre-value by paired t-test. UACR, urinary albumin-to-creatinine ratio. |
Changes in HbA1c, BMI, Blood Pressure, and Heart Rate
When the means before and after 1 year of treatment were compared, DPP-4 inhibitor therapy significantly decreased HbA1c (from 7.2 ± 0.9 [54.8 ± 9.4] to 6.9 ± 0.8% [51.7 ± 9.0 mmol/mol], P < 0.01), BMI (from 23.0 ± 3.1 to 22.9 ± 3.1 kg/m2, P < 0.01), SBP (from 131.7 ± 12.8 to 130.9 ± 12.6 mmHg, P < 0.01), DBP (from 74.3 ± 9.7 to 74.1 ± 9.4 mmHg, P = 0.07) and significantly increased heart rate (from 79.6 ± 11.5 to 80.6 ± 11.3 beats/min, P < 0.01). Moreover, these effects were sustained for at least 7 years of treatment, except for blood pressure (Figure 5).
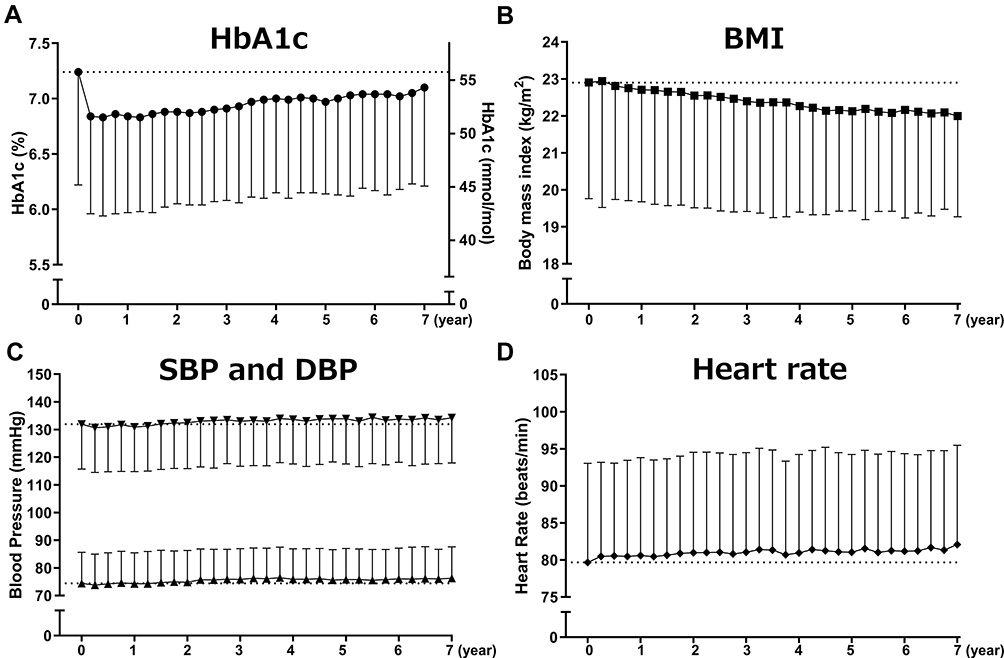 |
Figure 5 Effect of DPP-4 inhibitors on HbA1c (A), body weight (B), systolic and diastolic blood pressure (C), and heart rate (D) in patients with type 2 diabetes. Data are the mean ± SD. |
Discussion
This clinical study demonstrated for the first time that the long-term administration of DPP-4 inhibitor improves the annual rate of kidney function decline, as assessed by eGFR slopes in patients with type 2 diabetes and CKD. In addition, we found that add-on DPP-4 inhibitor therapy has been the preferred to α-glucosidase inhibitor and/or metformin users. We interpret these findings to suggest that the effect of add-on DPP-4 inhibitor therapy may contribute to the amelioration of DKD development and progression.
In this study, DPP-4 inhibitor therapy significantly improved the eGFR slope at stages G2, which may prevent or delay the onset of CKD. However, further research is necessary to demonstrate the clear renal protection benefits, while DPP-4 inhibitor therapy in patients with stage G1 was significantly steeper. Hyperfiltration is a typical feature of type 2 diabetic patients, and hyperglycemia is clearly involved in this hemodynamic abnormality.20 In older patients with type 2 diabetes, hyperfiltration can be masked by this age-related decline in GFR.20 Therefore, since DPP-4 inhibitor therapy has shown a further reduction of HbA1c in relatively younger patients with stage G1, it suggests that DPP-4 inhibitor therapy may correct hyperfiltration.
It has been shown in DPP-4 inhibitor CVOTs that the long-term administration of DPP-4 inhibitors appear to have a neutral effect on cardiovascular outcomes compared with placebo.21–24 A consensus report, by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), recommends metformin as first-line therapy.25 However, in the three major DPP-4 inhibitor CVOTs, baseline metformin nonusers were 20–30% of the total population, and prevalent users of metformin experienced a trend toward reduction of CV events with DPP-4 inhibitors, while baseline nonusers showed a trend towards harm.10 These results suggest that baseline metformin use may be a moderator of the effect of DPP-4 inhibitors on CV outcomes. Furthermore, in the sitagliptin CVOT, the mean eGFR reduction over 4 years from baseline was no significant differences between the sitagliptin and the placebo group for each eGFR stage, because the sitagliptin CVOT participants with reduced baseline kidney function were less likely to be taking metformin.26 The present study has shown that add-on DPP-4 inhibitor therapy significantly improved the eGFR slope in metformin users. Therefore, DPP-4 inhibitor therapy may not only prevent CV events but may equally reduce the risk for renal events with concurrent metformin use.
Moreover, we have demonstrated that baseline α-glucosidase inhibitor and/or metformin use induces a potential moderating effect on renal function with DPP-4 inhibitor initiation. α-Glucosidase inhibitor and metformin have been each shown to increase GLP-1 secretion through different mechanisms.11–14 In addition, add-on therapy with anagliptin in type 2 diabetes patients treated with miglitol and metformin for 52 weeks enhanced postprandial concentrations of active GLP-1 level.27 Thus, the combination of DPP-4 inhibitors and α-glucosidase inhibitor and/or metformin would be expected to provide an additive or synergistic effect via increased GLP-1 levels. Furthermore, the prescription of the main dose of metformin (750 mg/day) in this study has been through 250 mg tablets administered three times per day with meals as well as α-glucosidase inhibitors. Therefore, multidisciplinary therapy including the quality of drug therapy and medication management may contribute to at least a partial prevention of DKD development and progression.
A previous report in Japan found that DPP-4 inhibitors were most frequently (50–60%) prescribed to drug-naive patients as the first-line treatment.28 Ease of use in patients with renal impairment and frequency of administration were the most influential factors in choosing a DPP-4 inhibitor.28 In the present study, the number of prescriptions per patient as initial therapy of DPP-4 inhibitors were 9.9%. The use of metformin in accordance with ADA/EASD guidelines could derive beneficial effects of DPP-4 inhibitors as a result.
The renin-angiotensin system (RAS) blockade with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers are widely used and are known to induce a slowing in DKD progression.29,30 In this study, the observed benefits of DPP-4 inhibitors were consistent regardless of the baseline use of RAS blockade. Thus, these results imply that the DPP-4 inhibitor may be recommended to be routinely offered to patients with type 2 diabetes and CKD.
DPP-4 inhibitors marginally decreased the change in geometric mean UACR after 1 year of treatment compared with baseline. Previous studies suggested that DPP4 inhibitors may delay the progression of albuminuria.15–18 In any case, given that albuminuria is a pivotal marker in predicting the risk for end-stage renal disease, it is likely that this effect of DPP-4 inhibitors may contribute, at least in part, to the prevention of DKD progression.
The present study had several limitations. First, since it was a retrospective cohort study with no control group, it is difficult to demonstrate causation. However, the eGFR slope was compared with a follow-up of maximum 2 years before and after 7 years of treatment with DPP-4 inhibitors. The results of this study suggested that the effects of DPP-4 inhibitors in clinical practice may conform to the characteristics. Second, our methods of estimating eGFR slopes did not consider non-linear and time-varying patterns of eGFR decline. However, a study showed that slopes were linear for 83% of individuals with diabetes and normal kidney function.31 Third, it was not powered for analyses of the individual renal outcomes. Moreover, patients with mean eGFR of 67.5 mL/min/1.73 m2 were followed up for 5.3 ± 2.6 years, and therefore, we cannot extrapolate to longer-term effects in routine clinical practice. Furthermore, the label states that metformin is contraindicated at an eGFR <30 mL/min/1.73 m2. However, there may be a potential slowing in the reduction of the eGFR with DPP-4 inhibitors in patients with a low baseline eGFR. Further studies are needed to determine the renal outcomes in a prospective cohort study.
Conclusion
The long-term administration of DPP-4 inhibitor resulted in a significantly slower annual loss of kidney function, which was determined using eGFR slopes in patients with type 2 diabetes and CKD. In addition, DPP-4 inhibitor add-on therapy has been the preferred to α-glucosidase inhibitor and/or metformin users. These findings suggest that the effect of DPP-4 inhibitor add-on therapy may contribute to the amelioration of DKD development and progression.
Acknowledgments
We would like to thank all the physicians and staff members of the Naka Kinen Clinic.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
T.O. received personal fees from Abbott, AbbVie GK, Astellas Pharma, AstraZeneca, Bayer Yakuhin, Bristol-Myers Squibb, Daiichi Sankyo, Eli Lilly, Japan Tobacco, Kowa Pharmaceutical, Kyowa Hakko Kirin, Mitsubishi Tanabe Pharma, MSD, Novo Nordisk Pharma, Novartis Pharma, Ono Pharmaceutical, Poxel SA, Sanofi, Sanwa Kagaku Kenkyusho, Sumitomo Dainippon Pharma, Takeda Pharmaceutical, and Terumo, outside the submitted work and reports no other potential conflicts of interest for this work. The other authors report no conflicts of interest for this work.
References
1. Stamler J, Vaccaro O, Neaton JD, et al. Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the multiple risk factor intervention trial. Diabetes Care. 1993;16:434–444. doi:10.2337/diacare.16.2.434
2. Koye DN, Shaw JE, Reid CM, et al. Incidence of chronic kidney disease among people with diabetes: a systematic review of observational studies. Diabet Med. 2017;34:887–901. doi:10.1111/dme.13324
3. Hostetter TH. Chronic kidney disease predicts cardiovascular disease. N Engl J Med. 2004;351:1344–1346. doi:10.1056/NEJMe048211
4. van der Velde M, Matsushita K, Coresh J, et al. Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative meta-analysis of high-risk population cohorts. Kidney Int. 2011;79:1341–1352.
5. Mentlein R. Dipeptidyl-peptidase IV (CD26)–role in the inactivation of regulatory peptides. Regul Pept. 1999;85:9–24. doi:10.1016/S0167-0115(99)00089-0
6. Kanasaki K, Shi S, Kanasaki M, et al. Linagliptin-mediated DPP-4 inhibition ameliorates kidney fibrosis in streptozotocin-induced diabetic mice by inhibiting endothelial-to-mesenchymal transition in a therapeutic regimen. Diabetes. 2014;63:2120–2131. doi:10.2337/db13-1029
7. Kirino Y, Sato Y, Kamimoto T, et al. Interrelationship of dipeptidyl peptidase IV (DPP4) with the development of diabetes, dyslipidaemia and nephropathy: a streptozotocin-induced model using wild-type and DPP4-deficient rats. J Endocrinol. 2009;200:53–61. doi:10.1677/JOE-08-0424
8. Mulvihill EE, Drucker DJ. Pharmacology, physiology, and mechanisms of action of dipeptidyl peptidase-4 inhibitors. Endocr Rev. 2014;35:992–1019. doi:10.1210/er.2014-1035
9. Muskiet MH, Smits MM, Morsink LM, et al. The gut-renal axis: do incretin-based agents confer renoprotection in diabetes? Nat Rev Nephrol. 2014;10:88–103. doi:10.1038/nrneph.2013.272
10. Crowley MJ, Williams JW
11. Kårhus ML, Brønden A, Sonne DP, et al. Evidence connecting old, new and neglected glucose-lowering drugs to bile acid-induced GLP-1 secretion: a review. Diabetes Obes Metab. 2017;19:1214–1222. doi:10.1111/dom.12946
12. Bahne E, Hansen M, Brønden A, et al. Involvement of glucagon-like peptide-1 in the glucose-lowering effect of metformin. Diabetes Obes Metab. 2016;18:955–961. doi:10.1111/dom.12697
13. Lee A, Patrick P, Wishart J, et al. The effects of miglitol on glucagon-like peptide-1 secretion and appetite sensations in obese type 2 diabetics. Diabetes Obes Metab. 2002;4:329–335. doi:10.1046/j.1463-1326.2002.00219.x
14. Aoki K, Miyazaki T, Nagakura J, et al. Effects of pre-meal versus post-meal administration of miglitol on plasma glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide levels in healthy men. Endocr J. 2010;57:673–677. doi:10.1507/endocrj.K10E-064
15. Hattori S. Sitagliptin reduces albuminuria in patients with type 2 diabetes. Endocr J. 2011;58:69–73. doi:10.1507/endocrj.K10E-382
16. Groop P-H, Cooper ME, Perkovic V, et al. Dipeptidyl peptidase-4 inhibition with linagliptin and effects on hyperglycaemia and albuminuria in patients with type 2 diabetes and renal dysfunction: rationale and design of the MARLINA-T2D™ trial. Diab Vasc Dis Res. 2015;12:455–462. doi:10.1177/1479164115579002
17. Mori H, Okada Y, Arao T, et al. Sitagliptin improves albuminuria in patients with type 2 diabetes mellitus. J Diabetes Invest. 2014;5:313–319. doi:10.1111/jdi.12142
18. Goldshtein I, Karasik A, Melzer-Cohen C, et al. Urinary albumin excretion with sitagliptin compared to sulfonylurea as add on to metformin in type 2 diabetes patients with albuminuria: A real-world evidence study. J Diabetes Complications. 2016;30:1354–1359. doi:10.1016/j.jdiacomp.2016.05.012
19. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3:1–150.
20. Trevisan R, Dodesini AR. The hyperfiltering kidney in diabetes. Nephron. 2017;136:277–280. doi:10.1159/000448183
21. White WB, Cannon CP, Heller SR, et al. EXAMINE Investigators. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med. 2013;369:1327–1335. doi:10.1056/NEJMoa1305889
22. Scirica BM, Bhatt DL, Braunwald E, et al. SAVOR-TIMI 53 Steering Committee and Investigators. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013;369:1317–1326. doi:10.1056/NEJMoa1307684
23. Green JB, Bethel MA, Armstrong PW, et al. TECOS Study Group. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;373:232–242. doi:10.1056/NEJMoa1501352
24. Rosenstock J, Kahn SE, Johansen OE, et al. CAROLINA Investigators. Effect of linagliptin vs glimepiride on major adverse cardiovascular outcomes in patients with type 2 diabetes: the CAROLINA Randomized Clinical Trial. JAMA. 2019;322:1155–1166. doi:10.1001/jama.2019.13772
25. Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41:2669–2701. doi:10.2337/dci18-0033
26. Cornel JH, Bakris GL, Stevens SR, et al. TECOS Study Group. Effect of sitagliptin on kidney function and respective cardiovascular outcomes in type 2 diabetes: outcomes from TECOS. Diabetes Care. 2016;39:2304–2310. doi:10.2337/dc16-1415
27. Osonoi T, Saito M, Hariya N, et al. Add-on therapy with anagliptin in Japanese patients with type-2 diabetes mellitus treated with metformin and miglitol can maintain higher concentrations of biologically active GLP-1/total GIP and a lower concentration of leptin. Peptides. 2016;86:118–125. doi:10.1016/j.peptides.2016.10.011
28. Murayama H, Imai K, Odawara M. Factors influencing the prescribing preferences of physicians for drug-naive patients with type 2 diabetes mellitus in the real-world setting in Japan: insight from a web survey. Diabetes Ther. 2018;9:1185–1199. doi:10.1007/s13300-018-0431-3
29. Kitada M, Kanasaki K, Koya D. Clinical therapeutic strategies for early stage of diabetic kidney disease. World J Diabetes. 2014;5:342–356. doi:10.4239/wjd.v5.i3.342
30. Vejakama P, Ingsathit A, McKay GJ, et al. Treatment effects of renin-angiotensin aldosterone system blockade on kidney failure and mortality in chronic kidney disease patients. BMC Nephrol. 2017;18:342. doi:10.1186/s12882-017-0753-9.
31. Skupien J, Warram JH, Smiles AM, et al. The early decline in renal function in patients with type 1 diabetes and proteinuria predicts the risk of end-stage renal disease. Kidney Int. 2012;82:589–597. doi:10.1038/ki.2012.189
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.