Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 18
Adapting the Chairside: Pediatric Dental Management for Children with Neurodevelopmental Disorders – A Scoping Review
Authors Swastiantari PAP, Primarti RS ![]() , Ahmad M I, Andisetyanto P, Pratidina NB
, Ahmad M I, Andisetyanto P, Pratidina NB
Received 12 March 2026
Accepted for publication 30 May 2026
Published 15 June 2026 Volume 2026:18 605432
DOI https://doi.org/10.2147/CCIDE.S605432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Renan Dal Fabbro
Putu Ayu Pradnya Swastiantari, Risti Saptarini Primarti, Iwan Ahmad M, Prima Andisetyanto, Naninda Berliana Pratidina
Department of Pediatric Dentistry, Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Risti Saptarini Primarti, Department of Pediatric Dentistry, Universitas Padjadjaran, Bandung, West Java, Indonesia, Email [email protected]
Background: Children with neurodevelopmental disorders (NDD), especially autism spectrum disorder (ASD), are commonly characterized by sensory sensitivities, communication differences, and anxiety during dental treatment. These factors can reduce cooperation and prevent completion of care. This scoping review mapped recent evidence on non-pharmacological chairside strategies used to support pediatric dental management for children with NDD.
Methods: This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. A systematic literature search was conducted in PubMed, Scopus, ScienceDirect, and SpringerLink for publications from 2020 to 2026. The search focused on non-pharmacological chairside behaviour management strategies for children aged 0– 18 years with neurodevelopmental disorders in pediatric dental settings. Predefined keywords and the Population, Concept, and Context (PCC) framework were used to guide the search.
Results: Six studies from Malaysia, California, China, Italy, Turkey, and Brazil were included. Most studies focused on autism spectrum disorder, with limited representation of other neurodevelopmental profiles. Five chairside strategy domains were mapped: Tell-Show-Do-based behavior guidance, desensitization often supported by video or point-of-view modeling, structured visual pedagogy, sensory-adapted dental environments, and protective stabilization or passive immobilization. Reported outcomes were heterogeneous and included cooperation ratings, procedural tolerance, observed distress, and physiological markers.
Conclusion: Non-pharmacological chairside strategies for children with NDD show potential, particularly structured preparation, visual supports, and sensory-adapted environments. However, the evidence remains limited and methodologically heterogeneous. Standardized child-centered outcome sets and broader inclusion of non-ASD NDD subgroups are needed.
Keywords: neurodevelopmental disorders, behaviour guidance, desensitization, sensory-adapted environment
Introduction
Neurodevelopmental disorders (NDD), particularly autism spectrum disorder (ASD), are increasingly encountered in pediatric dentistry. These conditions are commonly associated with sensory over-responsivity, communication differences, and difficulty tolerating changes in routine. Such features can amplify dental anxiety and distress in the operatory, reduce cooperation, and contribute to delayed or incomplete care.1–3 Children with disabilities also face persistent barriers to oral health services. These barriers include limited availability of trained providers, environmental challenges within clinics, and the complexity of delivering care when cooperation is reduced.4
At chairside, behavioral challenges in ASD and other NDD profiles are often triggered by predictable aspects of dental care. These include bright lights, sounds from suction or handpieces, unfamiliar smells, physical proximity, and intraoral touch. Difficulties in understanding unfamiliar instructions or coping with uncertainty can further increase distress.1–3 These factors may lead to avoidance, resistance to change, or behavioral escalation. They may also increase appointment duration, reduce procedural quality, and raise safety concerns for both the child and the dental team.1–3 Consequently, pediatric dentists commonly use non-pharmacological chairside behavior guidance and clinic adaptations to support cooperation and reduce distress before considering pharmacological approaches.
Recent evidence has highlighted several clusters of non-pharmacological strategies used to improve tolerance and cooperation in autistic children. System-level or pathway-based behavioral support programs may include visual supports, structured exposure, caregiver preparation, and consistent dental routines. These approaches have been associated with improved collaboration over time and reduced reliance on general anesthesia for some treatments.3 Preparation-focused strategies, such as systematic desensitization, modeling, and stepwise rehearsal, are frequently described as practical methods to increase acceptance of dental examinations and procedures.1,2 Structured visual and staged behavioral approaches have also been applied to improve compliance with examination steps and cooperation, with measurable improvements using cooperation scales in clinical settings.5
In addition to communication and preparation strategies, adaptations to the physical environment have gained empirical attention. In a large randomized crossover trial involving autistic children, a sensory-adapted dental environment (SADE) significantly reduced physiological stress and observed behavioral distress compared with a regular dental environment during routine dental cleaning. This finding supports the clinical utility of environmental modification as a scalable chairside strategy.6 Complementary clinical evidence also maps how chairside behavior guidance techniques are used in special care pediatric settings. These techniques include Tell-Show-Do (TSD)-based bundles and, in selected cases, protective stabilization, while emphasizing the need for careful monitoring and individualized decision-making.7
Although the number of publications is increasing, the evidence remains scattered across intervention types, settings, and outcome measures. Recent syntheses have highlighted substantial heterogeneity in how studies define and assess success. Outcomes range from cooperation ratings and procedural tolerance to behavioral distress and physiological markers.2 This variation limits comparability across strategies and complicates translation into a unified chairside decision framework. In addition, the literature continues to be dominated by ASD, with limited mapping of non-ASD NDD profiles and fewer studies emphasizing standardized, child-centered outcomes.2,4
Therefore, a scoping review is justified to delineate recent evidence on non-pharmacological chairside management strategies for children with NDD in pediatric dental settings. This review also summarizes how outcomes are measured and identifies research gaps that may inform future clinical protocols and research priorities.
Methods
This scoping review was conducted in accordance with the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines. A Population-Concept-Context (PCC) framework was developed to guide the search process and define the inclusion and exclusion criteria (Table 1). The literature search targeted publications from 2020 to 2026 and was performed across four databases: PubMed, Scopus, ScienceDirect, and SpringerLink. Searches were conducted using predefined keywords and database-specific index terms where applicable (Table 2). For databases that do not use MeSH, namely ScienceDirect and SpringerLink, keyword-based searching was applied and adapted to each platform’s syntax.
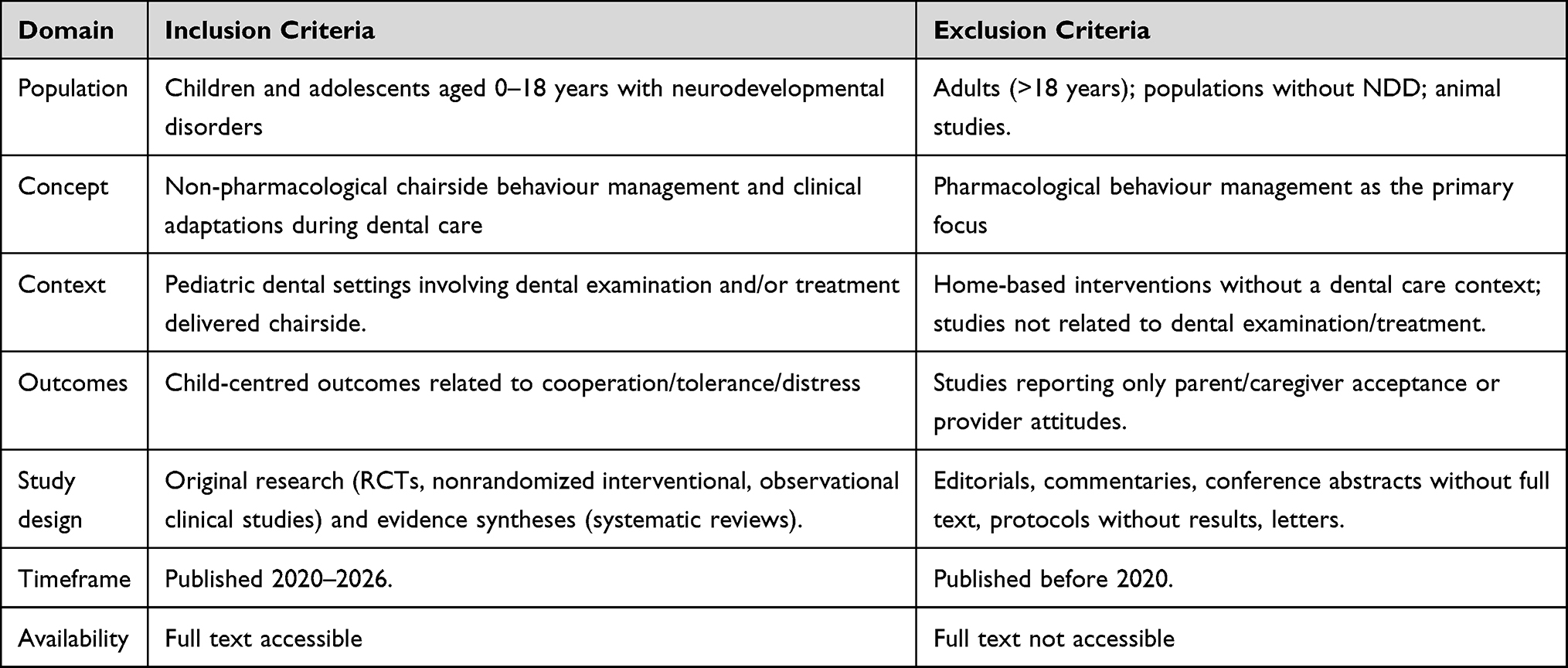 |
Table 1 Inclusion and Exclusion Criteria (PCC-Based) |
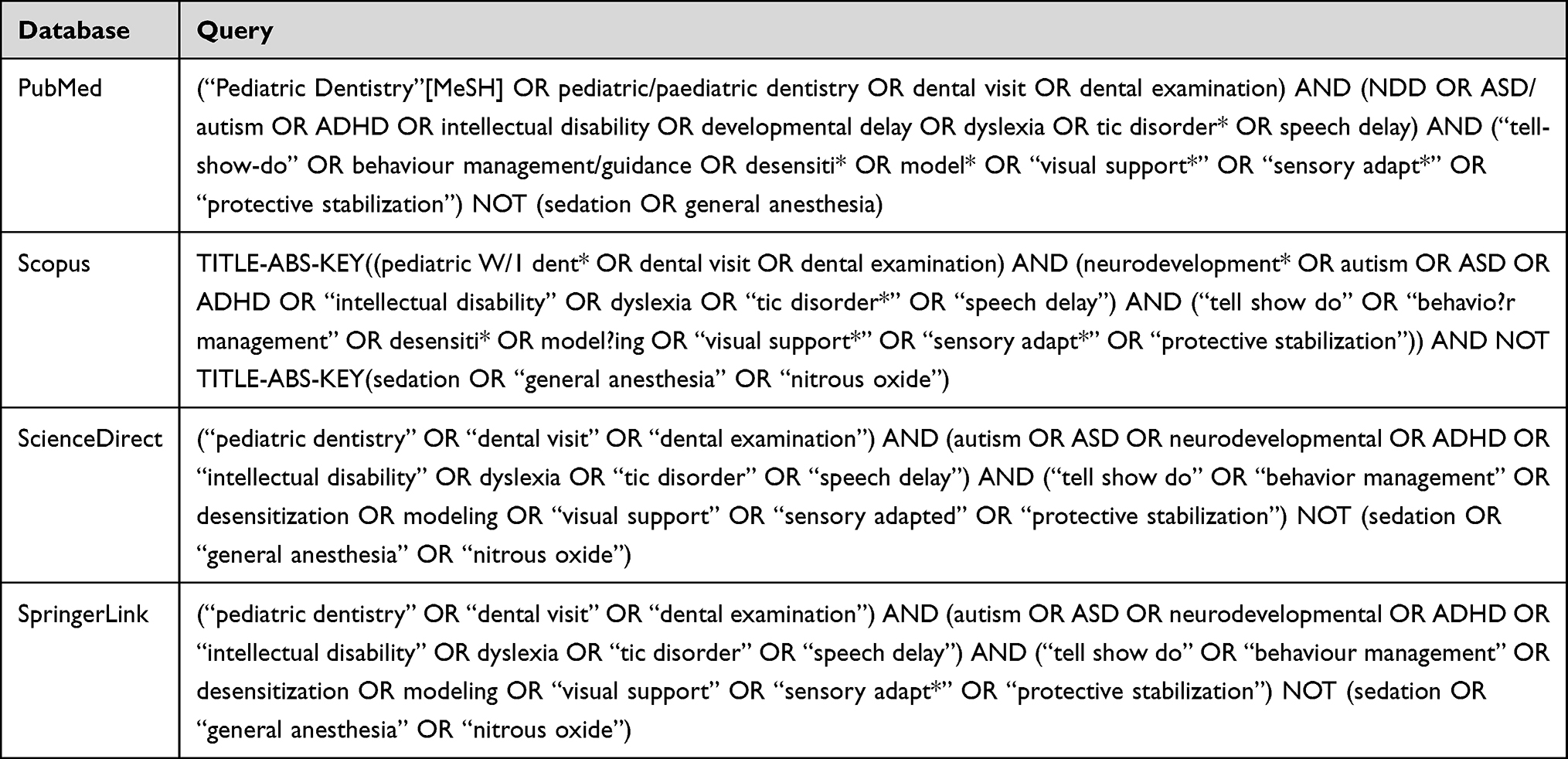 |
Table 2 Keywords |
This scoping review aimed to map non-pharmacological chairside pediatric dental management strategies for children (0–18 years) with neurodevelopmental disorders (NDD) in pediatric dental settings. The initial stage involved identifying records from the four databases using the predefined search strategy. A total of 248 records were retrieved; one duplicate was removed, leaving 247 records for title and abstract screening. Subsequently, potentially relevant articles were subjected to full-text evaluation, resulting in 17 articles assessed for eligibility. After full-text screening against the inclusion and exclusion criteria, six studies met the eligibility criteria and were included in the final evidence map. The overall selection and screening process is illustrated in the PRISMA-ScR flow diagram (Figure 1).8
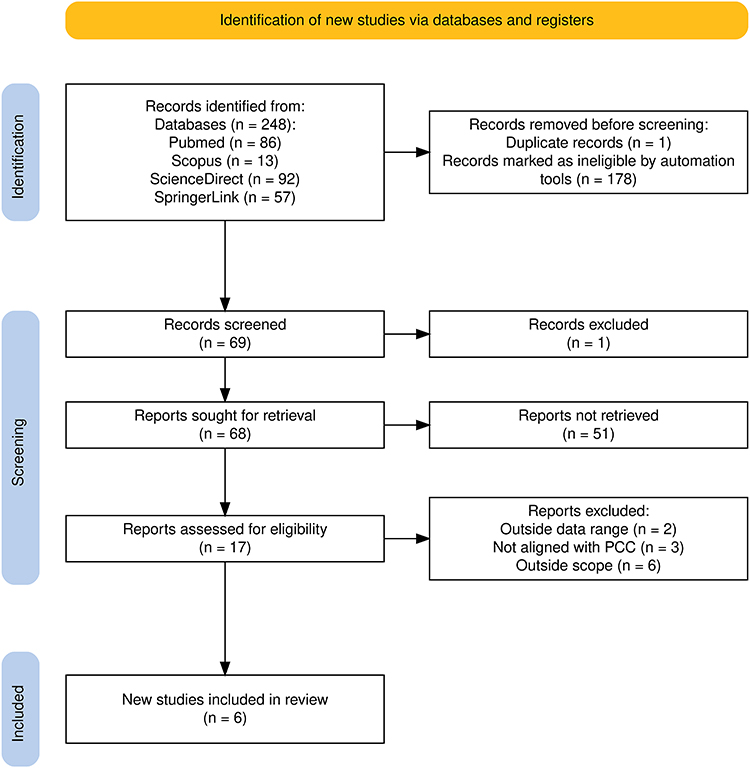 |
Figure 1 Prisma-ScR flow diagram. |
Result
This scoping review focused on studies published within a recent publication window from 2020 to 2026. Six studies met the eligibility criteria. The included studies represented diverse research designs, including two randomized crossover trials, two interventional clinical studies, one retrospective chart review, and one systematic review (Table 3). Most of the included evidence focused on children with autism spectrum disorder (ASD), whereas other neurodevelopmental disorder (NDD) profiles were infrequently represented. Non-pharmacological chairside management strategies were grouped into five domains: Tell-Show-Do-based behavior guidance, commonly used with positive reinforcement or distraction; systematic desensitization or graded exposure, often supported by video or point-of-view modeling; structured visual pedagogy, including Tell-Show-Feel-Do with staged practice; sensory-adapted dental environments; and protective stabilization or passive immobilization used in selected clinical circumstances.
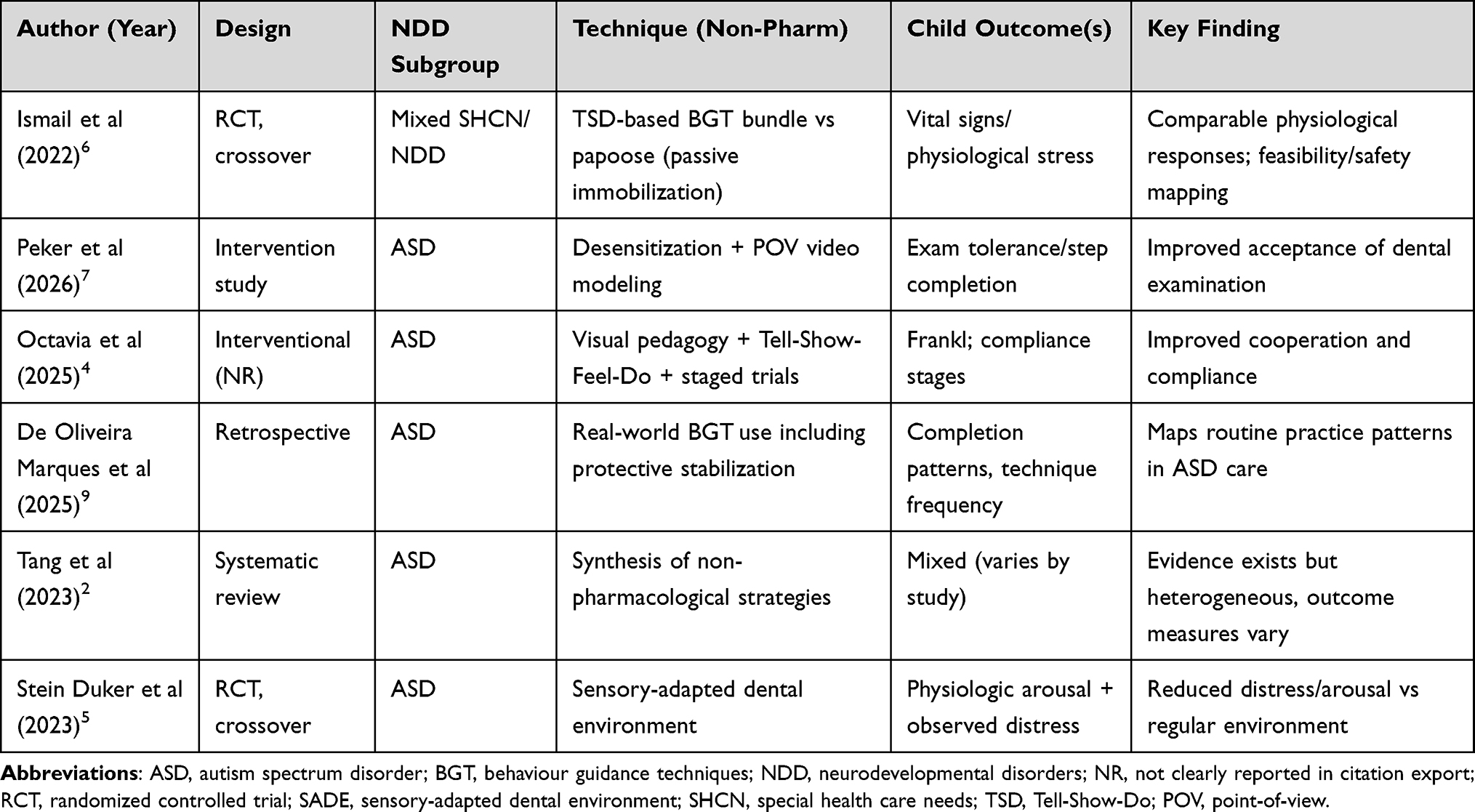 |
Table 3 Included Study Characteristics (n=6) |
Outcome reporting was heterogeneous across studies. Reported outcomes included cooperation scores, procedural tolerance or steps completed, observed behavioral distress, and physiological measures of arousal.
Discussion
This scoping review mapped recent evidence (2020–2026) on non-pharmacological chairside management for children with NDD in pediatric dental settings. This timeframe was intentionally selected to capture contemporary clinical approaches that increasingly emphasize sensory-adapted dental environments, structured preparation, visual pedagogy, caregiver involvement, and individualized behavior guidance strategies. Within this recent evidence base, the literature was limited, predominantly focused on ASD, and highly heterogeneous in terms of interventions and outcome measures.2,4–7 Structured preparation, including desensitization and modeling; structured visual pedagogy, including Tell-Show-Feel-Do and staged practice; sensory-adapted dental environments; and baseline behavior guidance bundles, such as Tell-Show-Do with reinforcement or distraction, were the most commonly described techniques across the six included studies. Protective stabilization was also discussed or employed in selected circumstances during treatment.2,4–7 These findings are consistent with the broader disability oral health literature, which emphasizes that children with disabilities continue to face access and system-level barriers. Therefore, this review highlights the clinical need for scalable chairside adaptations that may reduce distress and facilitate treatment completion.3 However, because the search was restricted to recent publications, earlier foundational studies may not have been captured. Thus, the findings should be interpreted as a mapping of recent evidence rather than a comprehensive historical synthesis of all available literature.
Tell-Show-Do-based behavior guidance remains a practical foundation for chairside management, particularly when combined with distraction and positive reinforcement to enhance predictability and perceived control.6 In the randomized crossover trial conducted by Ismail et al, no statistically significant differences in physiological measures, including blood pressure, heart rate, and oxygen saturation, were observed between a basic behavior guidance bundle and passive immobilization using papoose boards in children with special health care needs, most of whom had ASD.6 This trial has two clinically relevant implications. First, core behavior guidance bundles are commonly implemented as baseline strategies in SHCN/NDD care. Second, physiological monitoring may help contextualize safety concerns when more restrictive approaches are used in selected cases.6,7 However, physiological stability represents only one aspect of the child’s experience. Decision-making should also consider functional cooperation, distress, comfort, and adverse events whenever possible.6
Preparation-based strategies may be especially important in ASD because sensory unpredictability and unfamiliar routines can lead to avoidance and agitation during dental treatment.2,4 Across the included evidence, graded exposure, desensitization, and modeling were described as approaches that may reduce novelty and increase procedural tolerance.2,4,7 The structured visual model reported in the Indonesian study operationalized this concept through multiple visits using a successive approach. The intervention included Tell-Show-Feel-Do, visual pedagogy, audiovisual modeling, in vivo modeling, and behavioral trials.4 The study reported statistically significant improvements in compliance with examination steps and cooperation, as measured by the Frankl Behavior Scale.4 This approach has clinical utility because it describes a replicable multicomponent trajectory that resembles real-world step-up acclimatization in pediatric dental care rather than a single-session intervention.4
Pathway-based behavioral support models may also facilitate the integration of dental visits into routine ASD care over the long term. Pastore et al assessed a person-directed behavioral support pathway that included visual prompts, caregiver education, longer sessions, and intensive follow-up. Collaboration improved across the first year and remained greater in the supported group, with a considerable proportion of interventions completed without general anesthesia.1 Although this approach is resource-intensive, it supports a clinically useful concept. Repeated positive exposure with consistent structure may decrease the need for advanced management and improve access to routine preventive and restorative care.1
Environmental adaptation is another high-yield strategy because it can reduce sensory overload without requiring complex behavioral training. The randomized crossover trial by Stein Duker et al found significantly lower physiological stress, measured by electrodermal activity, and lower video-coded behavioral distress in a sensory-adapted dental environment than in a standard environment during dental cleanings in autistic children.5 Moderators such as age, IQ, and expressive communication influenced intervention success. This suggests that a one-size-fits-all sensory adaptation may not be equally effective across the ASD spectrum.5 For clinical practice, these findings support a tiered model. Core sensory adaptations, such as modifications to lighting, sound, and tactile stimuli, can be implemented broadly, while additional support should be tailored to the child’s profile and response.5
Outcome heterogeneity was identified as a major challenge because it limits comparability and slows translation into standardized chairside protocols.2 The systematic review by Tang et al emphasized that studies used different tools to assess anxiety, cooperation, and uncooperative behaviors. Many studies also focused on sensory-adapted environments as a strategy to increase cooperation during procedural and preventive examinations.2 Across the included studies, outcomes included cooperation scales, such as the Frankl scale, procedural tolerance or step completion, observed distress coding, and physiological markers, including vital signs or electrodermal activity.4–7 Although each outcome domain is important, the absence of a shared outcome set limits the ability to answer clinically relevant comparative questions. For example, it remains difficult to determine which approach is best suited for a particular child profile or what constitutes clinically meaningful improvement in routine care completion.2 Future studies should consider a minimum child-centered outcome package that includes cooperation rating, procedural completion or tolerance, distress measures, and adverse events. This would allow interventions to remain pragmatic while improving comparability across studies.2,5
This review also highlights an ASD-dominant evidence based, with limited representation of other NDD profiles, such as tic disorders, dyslexia, and speech-language delay, in recent chairside management research.2,4,5,7,9 This imbalance is clinically important because non-ASD NDD presentations may be associated with specific chairside challenges, including involuntary movements or vocalizations, receptive language limitations, and executive function difficulties.3 Moreover, disability access literature indicates that barriers may arise not only from the child’s characteristics but also from system design and clinic readiness.3 Therefore, future research should include diverse NDD diagnoses and care contexts, such as community clinics, hospital dentistry, and school-based programs, to support equitable and generalizable chairside frameworks.3
The available evidence suggests that non-pharmacological chairside management in NDD may be most useful when implemented as a stepwise, patient-centered approach.2,4–7 First, clinicians can establish standard communication using Tell-Show-Do or Tell-Show-Feel-Do, short instructions, and visual supports, followed by positive reinforcement and structured sequencing.4,6 Second, for children with high avoidance or low tolerance, structured preparation through graded exposure or desensitization combined with modeling may improve tolerance of examinations and preventive care over repeated visits.1,4,7 Third, sensory adaptation of the dental environment provides a concrete clinic-level strategy to reduce physiological stress and observed distress during routine care, particularly for children with sensory over-responsivity.5 Fourth, when protective stabilization or immobilization is considered necessary, available evidence suggests physiological stability in controlled settings. However, reporting of child-centered distress, adverse events, and decision criteria remains limited, highlighting an important research and reporting gap.6
This scoping review intentionally focused on non-pharmacological, child-centered outcomes and was limited to studies published between 2020 and 2026. Only six eligible studies met the inclusion criteria. Therefore, earlier foundational studies and caregiver/provider acceptability literature that may inform feasibility and ethics may not have been captured.2,3 As a result, the findings should be interpreted as a mapping of recent evidence rather than a comprehensive historical synthesis of the field. Furthermore, the supporting evidence was heterogeneous in design and outcome measures, making quantitative synthesis impossible.2,5 Nevertheless, this review provides a systematic overview of recent chairside approach clusters, highlights measurement gaps, and identifies priorities for future work.1–5,7
Future research should represent the full range of NDD profiles beyond ASD. Studies should also standardize intervention reporting, including components, dose, delivery setting, and fidelity. In addition, future studies should use a child-centered outcome set that includes cooperation, tolerance or completion, distress, and adverse events.2,3,5 Pragmatic trials comparing commonly used clusters, such as structured visual pedagogy, SADE, and graded exposure protocols, across settings would be especially valuable for supporting implementable clinical guidance.2,3,5
Conclusion
The findings of this scoping review suggest that structured, child-centered chairside adaptations may support dental care for children with neurodevelopmental disorders, particularly autism spectrum disorder. Non-pharmacological approaches that improve predictability and reduce sensory and communication barriers, such as Tell-Show-Do-based behavior guidance, graded exposure or desensitization supported by modeling, structured visual pedagogy, and sensory-adapted dental environments, show potential to improve procedural tolerance and reduce distress during routine dental visits. However, given the limited number of eligible studies and the heterogeneity of interventions, study designs, and outcome measures, these findings should be interpreted cautiously.
The available evidence indicates the importance of stepwise and individualized care planning. Strategies should be selected according to the child’s sensory profile, communication needs, baseline tolerance, and clinical context, while prioritizing comfort, safety, and a positive dental experience. Practical and scalable approaches, particularly structured preparation and environmental or sensory modifications, may be useful for reducing repeated distress and improving visit completion. Future studies should expand beyond ASD to include underrepresented neurodevelopmental profiles, report intervention components and dose more clearly, and adopt standardized child-centered outcome measures. Further well-designed studies are needed to strengthen clinical translation and support evidence-informed pediatric dental practice.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pastore I, Bedin E, Marzari G, et al. Behavioral guidance for improving dental care in autistic spectrum disorders. Front Psychiatry. 2023;14:1272638. doi:10.3389/fpsyt.2023.1272638
2. Tang SJ, Wei HL, Li CY, et al. Management strategies of dental anxiety and uncooperative behaviors in children with autism spectrum disorder. BMC Pediatr. 2023;23:612. doi:10.1186/s12887-023-04439-7
3. Alwadi MA, AlJameel AH, Baker SR, et al. Access to oral health care services for children with disabilities: a mixed methods systematic review. BMC Oral Health. 2024;24:1002. doi:10.1186/s12903-024-04767-9
4. Octavia A, Sitthisettapong T, Kettaratad-Pruksapong M, Dewanto I. Structured-visual model for dental examination in autism spectrum disorder children: cooperation and compliance. Int Dent J. 2025;75(3):2182–8. doi:10.1016/j.identj.2024.12.015
5. Stein Duker LI, Como DH, Jolette C, et al. Sensory adaptations to improve physiological and behavioral distress during dental visits in autistic children: a randomized crossover trial. JAMA Network Open. 2023;6(6):e2316346. doi:10.1001/jamanetworkopen.2023.16346
6. Ismail N, Md Isa KA, Wan Mokhtar I. A randomized crossover trial of behaviour guidance techniques on children with special health care needs during dental treatment: the physiological variations. Children. 2022;9:1526. doi:10.3390/children9101526
7. Peker I, Bagci N, Akdag F, Demirtas S, Akin Bulbul I, Atabek D. A combined approach: point-of-view video modeling and systematic desensitization for preparing children with autism spectrum disorders for dental examinations. Res Autism Spectr Disord. 2026;131:202808.
8. Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: an R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimized digital transparency and. Open Synth Campbell Sys Rev. 2022;18:e1230. doi:10.1002/cl2.1230
9. de Oliveira Marques V, Kort-Kamp LM, de Souza MAN, Portela MB, de Araújo Castro GFB. Oral health and behavioral management of children with autistic spectrum disorder: a 30-year retrospective study. J Autism Develop Disord. 2025;55(1):250–257. doi:10.1007/s10803-023-06209-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.