Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Acute unstable complex radial head and neck fractures fixed with a mini T-shaped plate in a 20-year-old man: a case report
Authors Yu W ![]() , Hu J, Zhang X, Zhu X, Xu Y, Yi J, Liu Y
, Hu J, Zhang X, Zhu X, Xu Y, Yi J, Liu Y
Received 2 March 2016
Accepted for publication 11 April 2016
Published 26 May 2016 Volume 2016:12 Pages 825—830
DOI https://doi.org/10.2147/TCRM.S107640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Weiguang Yu,1,* Jun Hu,1,* Xinchao Zhang,2 Xingfei Zhu,2 Yinfeng Xu,1 Jianhua Yi,1 Yunjiang Liu1
1Department of Orthopedics, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, 2Department of Orthopedics, Jinshan Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Abstract: Acute unstable complex radial head and neck fractures in adults are seldom reported in the literature. Early recognition and appropriate management are essential to prevent long-term consequences of the loss of elbow function, forearm rotation, and chronic pain. Here, we describe an unusual case of a 20-year-old man who exhibited acute unstable complex fractures of the head and neck of the right radius without other injuries or comorbidity. An open reduction and mini T-shaped plate fixation were performed within 3 hours after injury, and the results were satisfactory. A long plaster fixation was continued for 3 weeks. A gradual mobilization was started after the removal of the plaster under the supervision of a physiotherapist. At the 12-month follow-up, no complications associated with the use of the mini T-shaped plate were noted, and the Mayo Elbow Performance Score was 97 (excellent). To our knowledge, acute unstable complex radial head and neck fractures in adults can be successfully treated with a mini T-shaped plate reconstruction technique.
Keywords: unstable complex fractures, mini T-shaped plate, radial head, internal fixation, radial head replacement
Introduction
Acute unstable complex radial head and neck fractures are rare in adults. Several different treatments have been described in the literature including the excision of fragments or radial head, the use of 2.7 mm interfragmentary screws, radial head replacement (RHR), and open reduction and internal fixation (ORIF) with a Kirschner wire.1–3 The radial head stabilizing the radius during rotation of the forearm is responsible for transmitting most of the axial load across the elbow joint. Although excision of fragments or radial head fails to significantly alter elbow biomechanics in an otherwise intact elbow, radial head resection possibly results in valgus instability, degenerative changes, or early osteoarthritis of the ulnohumeral joint.4 Preservation of the radial head via ORIF is currently recommended in order to restore alignment and stability of the elbow.5 The use of 2.7 mm interfragmentary screws is an ideal treatment option (superior bending stiffness), but it may fail to reach the requirements of rigid fixation.6 As for RHR, it may cause more severe joint damage, subsequent joint degeneration, or reoperation.4 In addition, ORIF with a Kirschner wire, with advantages of low profile and requiring less exposure, does not provide rigid internal fixation; the Kirschner wire was left protruding through the skin, which led to osteomyelitis and avascular necrosis of the radial head.7 Businger et al8 evaluated the value of an “on-table” reconstruction technique in isolated comminuted radial head fractures without ulnar instability and concluded that comminuted radial head fractures can have a good functional outcome. In this article, we report ORIF with a mini T-shaped plate as an operative procedure for this injury and evaluate the value of the mini T-shaped plate.
Case report
A 20-year-old, right-handed man sustained acute unstable complex fractures of the head and neck of the right radius following a traffic accident, consisting of a radial head fracture and medial displacement, radial neck fracture, and a rupture of the lateral ligament complex. On admission, closed elbow trauma was observed, in which severe soft tissue swelling was noted but the neurovascular status was normal. An apparent restriction was noted in the flexion–extension arc of the elbow. The initial radiographs revealed complete fracture-dislocation of the head and neck of the radius, with a large fragment of the radial head lateral to the shaft of the radius and posterior to the elbow joint (Figure 1). On the basis of the above findings, an open procedure was required for the patient.
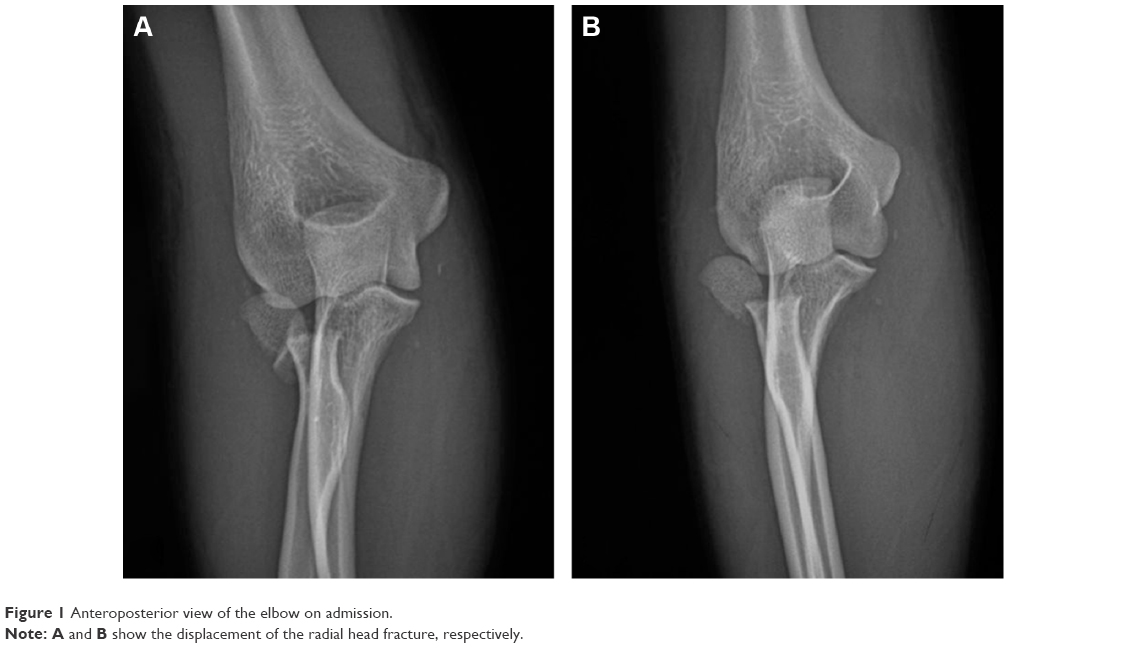 | Figure 1 Anteroposterior view of the elbow on admission. |
In the operating room, an open reduction and mini T-shaped plate internal fixation was performed under general anesthesia. An arthrotomy of the elbow joint was performed through a posterolateral approach. This surgical technique (the exposure process of the radial head) was done in accordance to that described by Shmueli et al.9 After making a longitudinal incision in the capsule of the elbow joint, damage to the lateral ligament complex was observed, and two large radial head fragments were found to be dissociative. Some small fragments in the elbow joint were removed. The articular surface of the radial head was lustrous but not integral. After extracting the radial head manually, a reconstruction of the articular surface of the radial head was performed in vitro. After refreshing the fracture site, these fragments were fixed with a mini T-shaped plate and screws (Synthes [Shanghai] Medical Trading Co., Ltd, Guangzhou, People’s Republic of China) (Figure 2), and then the damaged periosteum was interruptedly sutured using absorbable sutures. Finally, one small hole was drilled at the epicondyle. Nonabsorbable sutures were passed through this and through the lateral ligament complex (radial collateral ligament and annular ligament) to fix the ligament securely to the bone. Medial dislocation of the radial head was successfully eliminated. As the reconstructed radial head appeared to be properly aligned on fluoroscopy, a long plaster fixation in the neutral forearm position and 90° of elbow flexion were applied. The postoperative radiographs of the elbow showed that the fixation device was stable and nondisplaced (Figure 3). After 12 hours, the neurovascular status was rechecked, and the patient was strictly instructed to keep the limb elevated.
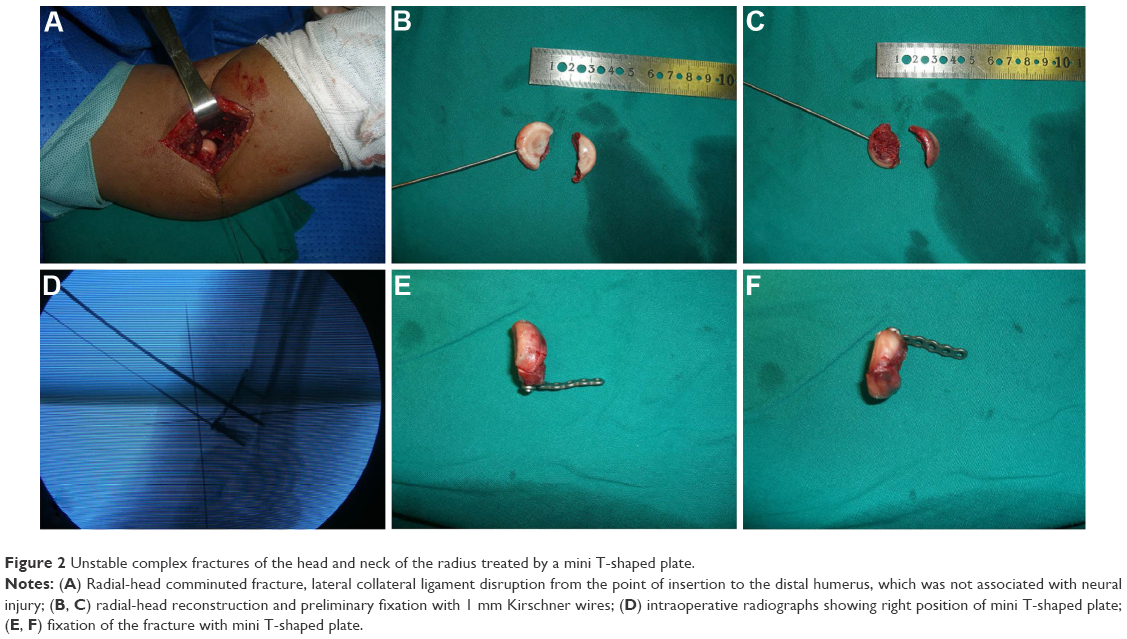 | Figure 2 Unstable complex fractures of the head and neck of the radius treated by a mini T-shaped plate. |
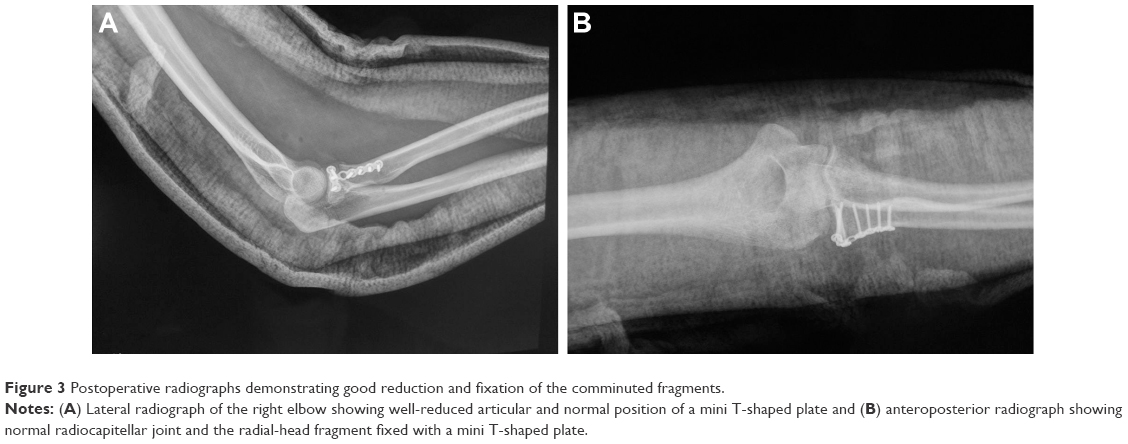 | Figure 3 Postoperative radiographs demonstrating good reduction and fixation of the comminuted fragments. |
Three weeks later, the reconstructed radial head appeared by fluoroscopy to be in its proper location on fluoroscopy. No obvious rotation or separation was observed. Then, the plaster fixation was removed and an attempt was made to start early active exercises for flexion–extension and pronation–supination. Weight bearing was not allowed until the first clinical and radiological follow-up after 1.5 months. After 3 months, full loading was performed.
Bone union occurred without osteonecrosis or heterotopic ossification. Additionally, a radiograph taken 6 months after surgery revealed no avascular necrosis, collapse, or deformity of the radial head. After the metalwork was removed at 1 year (Figure 4), no comment was made regarding the complications associated with the use of the internal fixator, and the patient was symptom-free with full range of motion in the elbow joint. The carrying angle was 12°. The Mayo Elbow Performance Score was 97 (excellent) (Figure 5). This study was reviewed and approved by the review board of the First Affiliated Hospital, Sun Yat-sen University, and an exemption for informed consent was obtained from this Investigational Ethical Review Board.
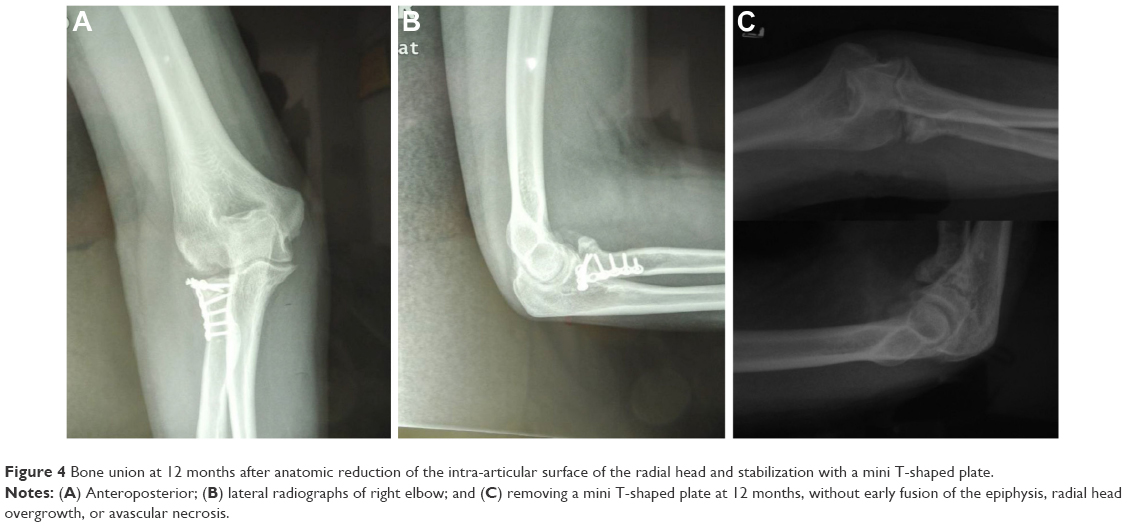 | Figure 4 Bone union at 12 months after anatomic reduction of the intra-articular surface of the radial head and stabilization with a mini T-shaped plate. |
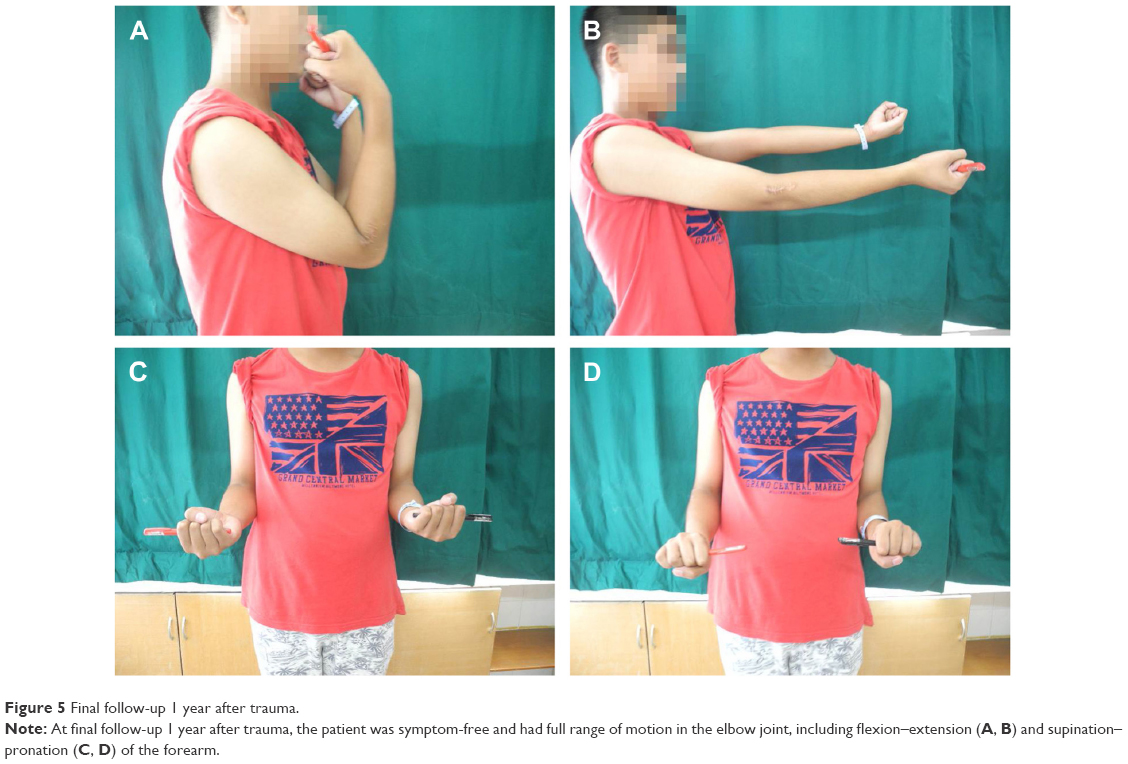 | Figure 5 Final follow-up 1 year after trauma. |
Discussion
In general, unstable radial head fractures commonly occur as part of a complex injury pattern, have fragments that are detached and mobile with little or no soft tissue attachments, and are associated with osseous and ligamentous injuries to the elbow or forearm.10 Acute unstable complex fractures of the radial head and neck in skeletally mature individuals with damage to the lateral ligament complex are rare, with only a few cases having been reported. However, to our knowledge, no report has described an injury consisting of complex fractures with obvious radial head–neck displacement and simultaneous medial dislocation of the radial head.
Given the number, size, and displacement of fragments, a viable option for initial or secondary treatment is RHR or ORIF.11,12 Based on the injury pattern observed in our case and the fact that biomechanical measurement proves that mini-plate could maintain an enhanced fixation and withstand rotational forces,13 a mini T-shaped plate fixation may be more appropriate for such fracture dislocations compared with RHR. This is consistent with previous reports.6,8,13 Duckworth et al7 demonstrated a high removal or revision rate after RHR for acute unstable complex fractures. Birkedal et al14 reported that six patients who received RHR had a clinically significant decrease in elbow flexion. Charalambous et al15 believed that RHR may potentially be associated with loosening and the early appearance of osteoarthritic changes in the capitellum and elbow joint. Additionally, some other studies described the results of a loose, spacer arthroplasty type of RHR for the treatment of acute unstable complex radial head and neck fractures.8,16–18 However, Heim et al19 demonstrated that fractures in six out of eleven patients with mini T-shaped plate fixation for comminuted radial head fractures failed to heal. The reason is likely associated with early full weight-bearing or evaluation of isolated Mason type 3 fractures. Chen et al20 reported that for unstable and comminuted radial head fractures, the satisfactory rate and complication rate of mini T-shaped plate fixation were 65.2% and 47.9%, respectively. This may be explained by the fact that decreasing age was associated with decreasing fracture complexity. Shore et al21 believed that RHR was indicated for displaced comminuted radial head fractures that could not be managed reliably with mini T-shaped plate fixation and had an associated elbow dislocation. In short, the management of comminuted radial head fractures with associated ligament disruption remains controversial.8 Although mini T-shaped plate fixation is performed based on a small amount of defective bone and stable comminuted fractures of the radial head, the concept is not to reconstruct the anatomic shape of the radial head but rather to maintain the length of the radius and the integrity of the articular surface of the radial head and to repair the ligaments and damaged periosteum. Nevertheless, mini T-shaped plate fixation of displaced comminuted radial head fractures with more small fragments may be associated with elbow instability, in which RHR may have a better performance. Watters et al22 reported that RHR afforded the ability to obtain elbow stability with comparable overall outcomes (disabilities of the arm, shoulder, and hand and Broberg–Morrey scores, range of motion) when compared to mini T-shaped plate fixation.
Conclusion
In special cases, if a radial head is irreparable, RHR is useful to restore elbow and forearm stability. If the reduction has relative stability, mini T-shaped plate fixation can result in satisfactory joint mobility and provide a good functional outcome and could be an option.
Acknowledgment
The authors thank Dr Jianhua Yi, The First Affiliated Hospital of Sun Yat-sen University, who provided generous support for the operation.
Disclosure
The authors report no conflicts of interest in this work.
References
Agashe MV, Samant A, Aroojis AJ. Convergent radioulnar translocation with radial head fracture in a child: a case report and review of the literature. J Orthop Trauma. 2012;26(4):E36–E39. | ||
Li Y-A, Chang M-C, Chen T-S. Extreme comminuted fracture of the radial head fixed with multiple Kirschner wires: case report. J Trauma. 2009;67(4):E124–E128. | ||
Tay D, Mahadev A. An unexpected outcome following radial head excision for Jeffrey Type II fracture–dislocation of the proximal radius in a child. Ann Acad Med Singapore. 2010;39(9):742–744. | ||
Duckworth AD, Watson BS, Will EM, et al. Radial head and neck fractures: functional results and predictors of outcome. J Trauma. 2011;71(3):643–648. | ||
Smith AM, Morrey BF, Steinmann SP. Low profile fixation of radial head and neck fractures: surgical technique and clinical experience. J Orthop Trauma. 2007;21(10):718–724. | ||
Navali AM, Sadigi A. Displaced fracture of the neck of the radius with complete 180 degrees rotation of the radial head during closed reduction. J Hand Surg Br. 2006;31B(6):689–691. | ||
Duckworth AD, Wickramasinghe NR, Clement ND, et al. Radial head replacement for acute complex fractures: what are the rate and risks factors for revision or removal? Clin Orthop Relat Res. 2014;472(7):2136–2143. | ||
Businger A, Ruedi TP, Sommer C. On-table reconstruction of comminuted fractures of the radial head. Injury. 2010;41(6):583–588. | ||
Shmueli G, Herold HZ. Compression screwing of displaced fractures of the head of the radius. J Bone Joint Surg Br. 1981;63B(4):535–538. | ||
Duckworth AD, McQueen MM, Ring D. Fractures of the radial head. Bone Joint J. 2013;95B(2):151–159. | ||
Leigh WB, Ball CM. Radial head reconstruction versus replacement in the treatment of terrible triad injuries of the elbow. J Shoulder Elbow Surg. 2012;21(10):1336–1341. | ||
Burkhart KJ, Nowak TE, Kim YJ, Rommens PM, Muller LP. Anatomic fit of six different radial head plates: comparison of precontoured low-profile radial head plates. J Hand Surg Am. 2011;36A(4):617–624. | ||
Burkhart KJ, Mueller LP, Krezdorn D, et al. Stability of radial head and neck fractures: a biomechanical study of six fixation constructs with consideration of three locking plates. J Hand Surg Am. 2007;32A(10):1569–1575. | ||
Birkedal JP, Deal DN, Ruch DS. Loss of flexion after radial head replacement. J Shoulder Elbow Surg. 2004;13(2):208–213. | ||
Charalambous CP, Stanley JK, Siddique I, Powell E, Ramamurthy C, Gagey O. Radial head fracture in the medial collateral ligament deficient elbow; biomechanical comparison of fixation, replacement and excision in human cadavers. Injury. 2006;37(9):849–853. | ||
Ring D. Radial head fracture: open reduction-internal fixation or prosthetic replacement. J Shoulder Elbow Surg. 2011;20(2):S107–S112. | ||
Moro JK, Werier J, MacDermid JC, Patterson SD, King GJW. Arthroplasty with a metal radial head for unreconstructible fractures of the radial head. J Bone Joint Surg Am. 2001;83A(8):1201–1211. | ||
Delclaux S, Lebon J, Faraud A, et al. Complications of radial head prostheses. Int Orthop. 2015;39(5):907–913. | ||
Heim U. Surgical treatment of radial head fracture. Z Unfallchir Versicherungsmed. 1992;85(1):3–11. | ||
Chen X, Wang SC, Cao LH, Yang GQ, Li M, Su JC. Comparison between radial head replacement and open reduction and internal fixation in clinical treatment of unstable, multi-fragmented radial head fractures. Int Orthop. 2011;35(7):1071–1076. | ||
Shore BJ, Mozzon JB, MacDermid JC, Faber KJ, King GJW. Chronic posttraumatic elbow disorders treated with metallic radial head arthroplasty. J Bone Joint Surg Am. 2008;90A(2):271–280. | ||
Watters TS, Garrigues GE, Ring D, Ruch DS. Fixation versus replacement of radial head in terrible triad: is there a difference in elbow stability and prognosis? Clin Orthop Relat Res. 2014;472(7):2128–2135. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.