Back to Journals » Clinical Ophthalmology » Volume 16
Acquisition Time for Swept-Source Optical Biometry Plus Corneal Power Measurement During Cataract Evaluation
Authors Ruiz-Mesa R ![]() , Ruiz-Santos M, Blanch-Ruiz J, Jiménez-Nieto A
, Ruiz-Santos M, Blanch-Ruiz J, Jiménez-Nieto A
Received 30 November 2021
Accepted for publication 26 January 2022
Published 5 March 2022 Volume 2022:16 Pages 661—668
DOI https://doi.org/10.2147/OPTH.S351845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ramón Ruiz-Mesa, Maria Ruiz-Santos, Julia Blanch-Ruiz, Ana Jiménez-Nieto
Cataract and Refractive Surgery Department, Oftalvist Jerez de la Frontera, Jerez de la Frontera, Spain
Correspondence: Ramón Ruiz-Mesa, Oftalvist Jerez de la Frontera, Avenida Puerta del Sur S/N, Jerez de la Frontera, Cádiz, 11408, Spain, Email [email protected]
Purpose: To compare the acquisition time necessary to obtain the optical biometry plus corneal power measurement using the IOLMaster 700 with central topography with that found using the standard IOLMaster 700 in combination with two corneal topographers, when acquiring biometry measurements during cataract evaluation.
Methods: This prospective, observational, controlled study included 96 eyes of 96 cataract patients. Acquisition times were registered for different conditions: time required for one complete measurement with IOLMaster 700 with central topography, time required for one complete measurement with standard IOLMaster 700 (without central topography), time required for one complete measurement with standard IOLMaster 700 plus time required for one complete measurement with Cassini, and time required for one complete measurement with standard IOLMaster 700 plus time required for one complete measurement with Pentacam HR. In addition, the agreement between keratometry (K), total keratometry (TK) and equivalent K reading (EKR) parameters using the three devices was performed.
Results: The post hoc Tukey’s test revealed that there were statistically significant differences for all pairwise comparisons (p < 0.001) except for the acquisition times of the IOLMaster with central topography and the standard IOLMaster 700 (p = 0.501). The acquisition time by the IOLMaster 700 with central topography takes approximately three less times than the use of a corneal topographer combined with a biometer. The agreement of K1, K2, TK1, TK2, EKR1 and EKR2 measurements between the three devices revealed statistically significant differences for all possible comparisons (p < 0.001) except for the comparison between the IOLMaster 700 and the Cassini for all parameters (p > 0.05).
Conclusion: We consider that this is an efficient procedure that improves clinical flow. We also conclude that K readings obtained with the three devices cannot be used interchangeably since there are clinically relevant differences that may affect cataract surgery outcomes.
Keywords: IOLMaster 700, optical biometer, cataract, Scheimpflug imaging, color LED
Introduction
The measurement of different corneal parameters, such as posterior keratometry (K), has become increasingly important in cataract surgery since it can be advantageous for some patients who may benefit from more accurate information about their total corneal power (astigmatic or post-laser excimer refractive surgery eyes among others). Standard K provides only information from the anterior corneal surface, but the posterior surface and the corneal thickness also contribute to the total corneal power. Then, adding this information when calculating intraocular lens (IOL) power would enhance surgical outcome accuracy. However, if this valuable information is not considered, surgeons may report significant postoperative over- or under-correction outcomes,1,2 thus critical in premium lens power calculation such as for multifocal toric IOL. Although some nomograms extrapolate mathematically total corneal astigmatism from the anterior cornea, it is expected that real data may benefit the clinical outcomes post-surgery. In addition, surgeons need to use an optical biometer to measure required parameters for IOL calculation (ie, K, axial length, anterior chamber depth, etc.) and a secondary device that merely estimates the impact of posterior corneal astigmatism.3 This may increase inaccuracies in managing preoperative data and the time required for examinations in patients to be submitted to cataract surgery.
The IOLMaster 700 (Carl Zeiss Meditec AG, Jena, Germany), a well-known optical biometer based on swept-source optical coherence tomography (SS-OCT),4 can measure both anterior and posterior astigmatism, providing clinicians the total corneal power. This device directly measures anterior and posterior corneal curvature using a combination of telecentric 3-zone K and SS-OCT, called Total Keratometry (TK). Different clinical studies have assessed the use of this device, comparing standard K with TK using different IOL formulas and after corneal refractive surgery3,5–13 showing good refractive outcomes by using TK. However, only two studies have analyzed TK and compared to total corneal astigmatism by other devices, being in this case, a Scheimpflug camera.9,13 The time required to acquire preoperative measurements such as optical biometry warrants attention since it impacts efficient clinical flow and can affect the patient experience.14 Efficient procedures, accurate and fast, should be considered in routine cataract surgery practice.
The purpose of the present study was to compare the acquisition time necessary to obtain the optical biometry plus corneal power measurement using the IOLMaster 700 with central topography with that found using the standard IOLMaster 700 in combination with two corneal topographers: the Pentacam HR Scheimpflug camera (Oculus, Wetzlar, Germany) and the Cassini color LED (Cassini Technologies B.V, Den Haag, The Netherlands). In addition, the study assessed the corneal power measurements with the three devices analyzing the agreement for K1, K2, TK1, TK2, equivalent K reading 1 (EKR1), and EKR2.
Materials and Methods
Patients
This prospective, observational, controlled study included 100 eyes of 100 cataract patients. The study was conducted in accordance with the tenets of the Helsinki Declaration and was approved by the Ethics Committee CEIM Hospital Clínico San Carlos (Spain). This study was registered at clinicaltrials.gov with the following number NCT04875247. Proper informed consent for participating in the study was acquired for every patient enrolled. All patients were examined at the Oftalvist Jerez de la Frontera, Cádiz, Spain. Exclusion criteria considered previous corneal surgery, keratoconus, corneal scar or pterygium. Refraction, visual acuity, and standard ophthalmological examination with slit-lamp examination and fundoscopy were performed before the measurements as standard clinical routine procedure for cataract surgery. Considering the similarity of parameters between both eyes of the same patient15 only the right eye was included in the study.
Devices
The IOLMaster 700 is an SS-OCT optical biometer that calculates K1 and K2 using telecentric keratometry. The 3-zone telecentric keratometry in combination with the SS-OCT enables the device to obtain central anterior and total corneal power maps, as well as total corneal power (TK). TK considers anterior and posterior corneal curvature and corneal thickness providing the following values: TK1 and TK2. The Pentacam HR is based on the Scheimpflug principle. The Pentacam uses a monochromatic blue light-emitting diode with a wavelength of 475 nm and a Scheimpflug camera that that revolves around the optical axes of the eye creating a three-dimensional model of the anterior segment. Elevation data from Scheimpflug images are used to calculate the anterior and posterior corneal curvature. The Cassini analyses the specular reflection of 679 colored LEDs (red, yellow, and green) and 7 blue “anchor” LEDs. It uses the location of each reflected spot to generate anterior corneal topographic maps and uses the 7 additional infrared LEDs based on the second Purkinje image to measure the corneal posterior surface. Both devices provide the EKR1 and 2 values.
Examination
A skilled operator did all measurements in the same session. Each patient was positioned correctly on the chin rest and forehead. Measurement for the three devices evaluated was done in random order. All devices were calibrated daily to check the quality of the measurements following the manufacturer’s recommendations. Acquisition times were registered for different conditions: 1) time required for one complete measurement with IOLMaster 700 with central topography, 2) time required for one complete measurement with standard IOLMaster 700 (without central topography), 3) time required for one complete measurement with standard IOLMaster 700 plus time required for one complete measurement with Cassini, and 4) time required for one complete measurement with standard IOLMaster 700 plus time required for one complete measurement with Pentacam. Note that one complete measurement considers the time when the patient’s chin touches the device, the measurement carried out by the examiner, and when the patient leans back.
Statistical Analysis
Statistical analysis was carried out using SPSS software (22.0 version, IBM Corp., Armonk, New York, USA). All the measurements are shown as the mean ± standard deviation (SD). The analysis of the normality distribution was checked by means of the Shapiro–Wilk test. Statistically significant differences between the measurements taken with the three devices were evaluated with repeated measures analysis of variance (rANOVA). The Tukey procedure was used as a post hoc test for comparisons between data groups when the rANOVA revealed significant differences between measurements. The p value was considered statistically significant when <0.05.
Bland and Altman method were done to assess the agreement between devices.16,17 The average and the difference between the measurements (K1, K2, TK1, TK2, EKR1, and EK2) for all possible pairwise comparisons for the three devices were calculated. Different values were depicted in the plot: average difference, confidence interval 95% (CI) of the average difference, and 95% limits of agreement (LoA). The LoA was calculated as mean difference ± 1.96 SD.
Results
Ninety-six eyes of 96 patients (40 males and 56 females) with a mean age of 66.43 ± 9.34 years were analysed. Four patients were excluded from the study since not all the parameters were fully obtained. Only the right eye in each patient was evaluated. All patients were evaluated using all the devices. Data was completely registered for each eye in the database for the analysis. The mean spherical equivalent of the eyes was −1.12 ± 5.01 D (mean ± SD) and ranged from +10.63 to −28.50 D.
Table 1 shows the acquisition times (mean ± SD and range) for the different situations previously described. The rANOVA test revealed that there were statistical differences when the acquisition times were compared between the four situations (p < 0.001). The post hoc Tukey’s test revealed that there were statistically significant differences for all pairwise comparisons (p < 0.001) except for the acquisition times of the IOLMaster with central topography and the standard IOLMaster 700 (p = 0.501).
 |
Table 1 Mean Acquisition Time for the Different Devices |
Figure 1 shows the different Bland-Altman plots (mean difference vs average) for the three possible comparisons between devices: IOLMaster 700 vs Cassini, IOLMaster 700 vs Pentacam HR and Cassini vs Pentacam HR for K1 and K2. Figure 2 shows the same plots for TK1, TK2, EKR1 and EKR2. Table 2 shows the mean difference ± SD, the 95% CI, the 95% LoA, and the p values obtained for all comparisons. The post hoc Tukey’s test revealed statistically significant differences for all possible comparisons (p < 0.001) except for the comparison between the IOLMaster 700 and the Cassini for all parameters (p > 0.05). The lowest mean differences were found for the comparison between the IOLMaster 700 and Cassini (−0.02 and 0.01 D).
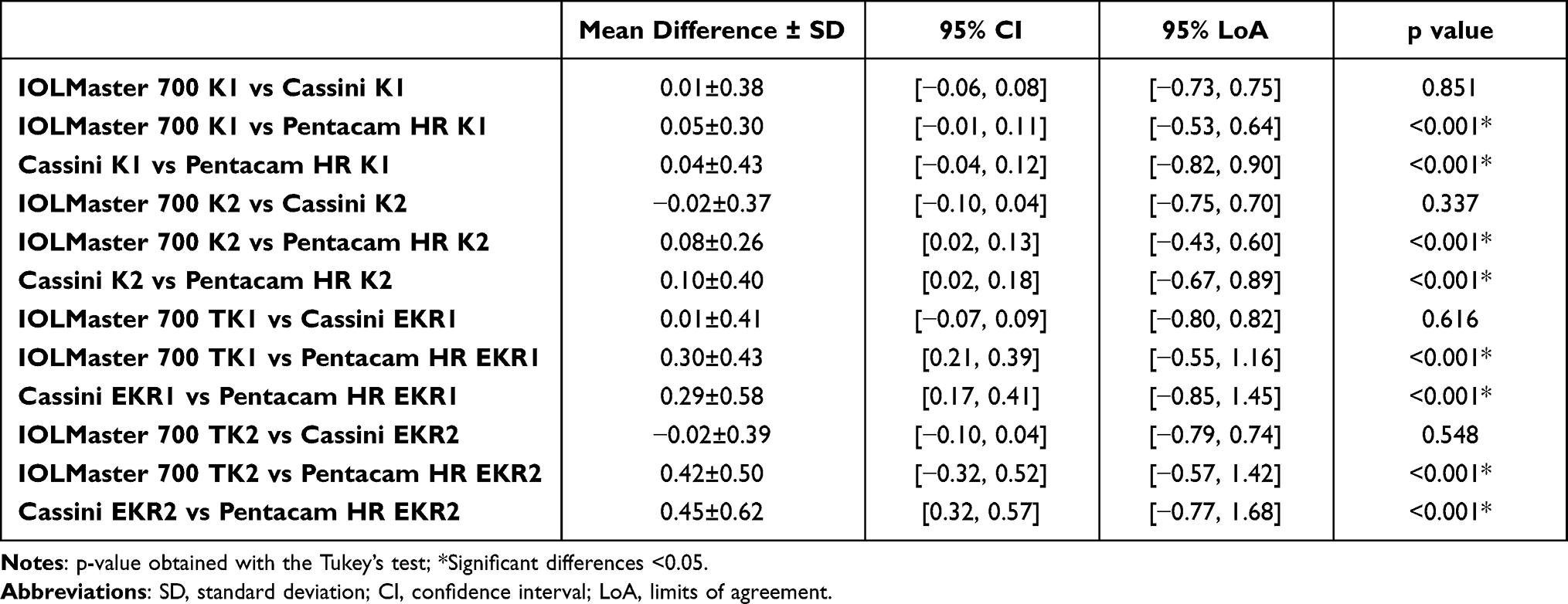 |
Table 2 Agreement of K1, K2, TK1, TK2, EKR1 and EKR2 (Diopters) Measurements Between the Three Devices |
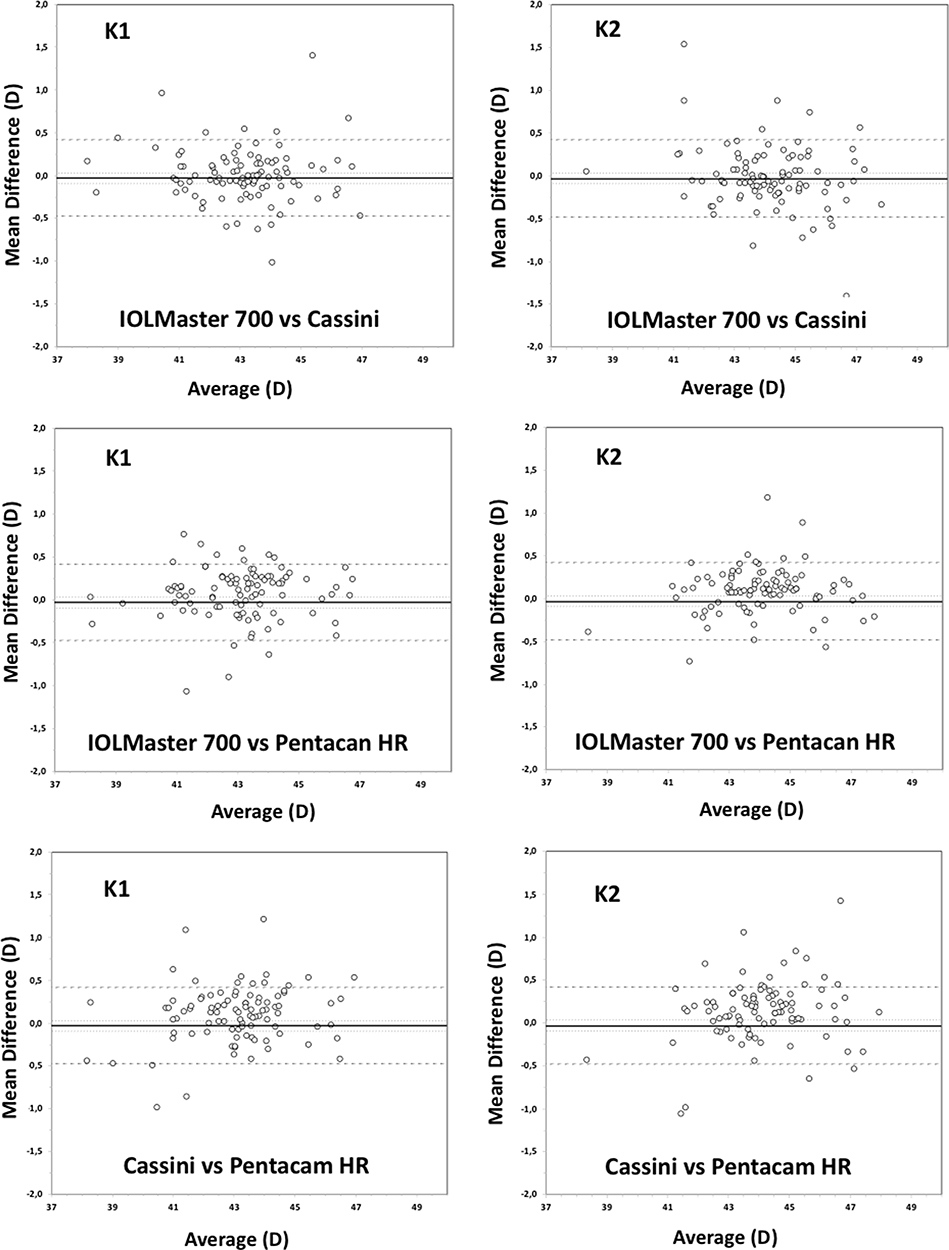 |
Figure 1 Bland-Altman plots obtained showing the mean difference versus average for the comparison between the different devices for K1 and K2. Mean (continuous line), lower and upper limits of agreement (±1.96SD, standard deviation, peripheral dotted lines) and lower and upper confidence intervals (95%) are depicted. |
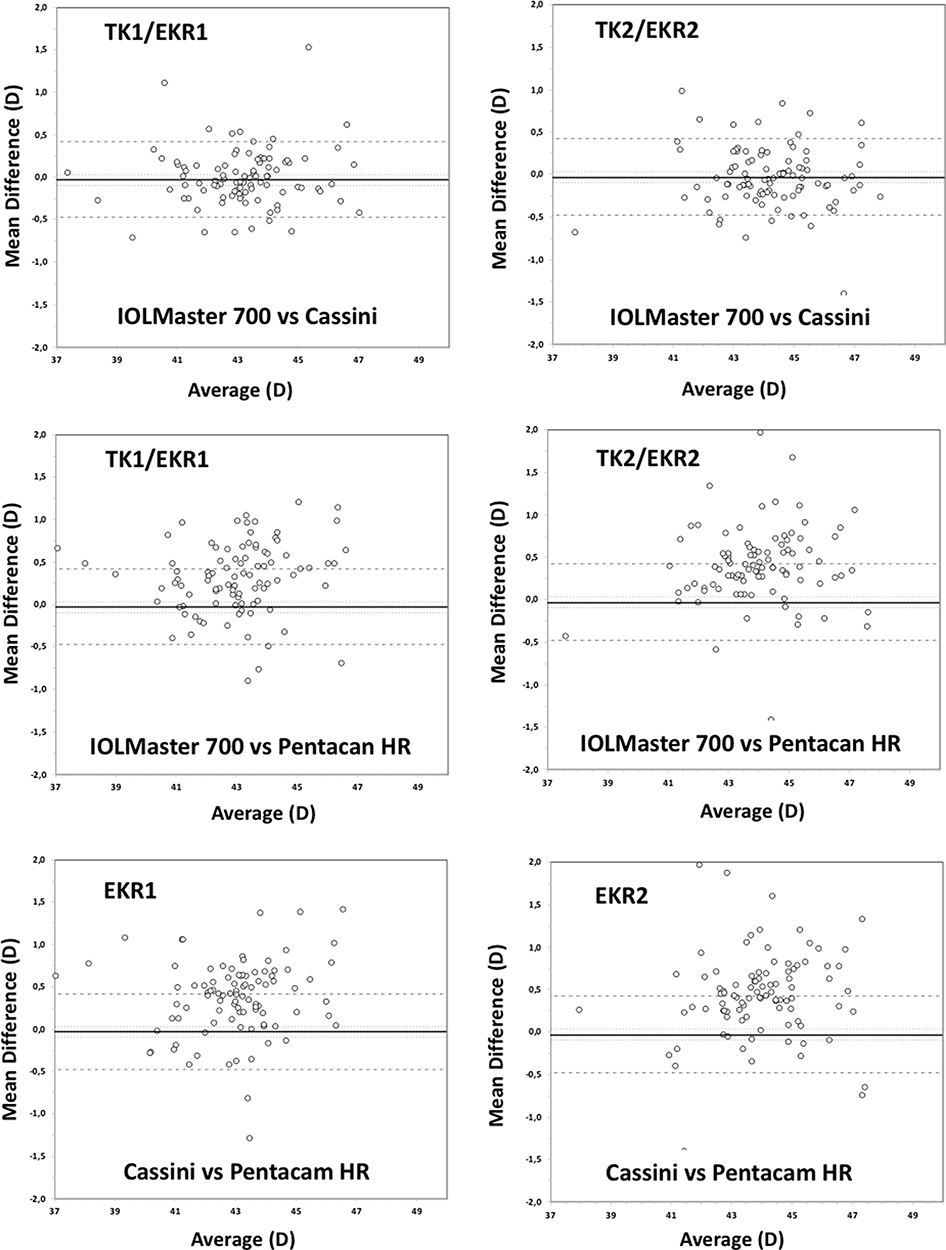 |
Figure 2 Bland-Altman plots obtained showing the mean difference versus average for the comparison between the different devices for TK1, TK2, EKR1 and EKR2. Mean (continuous line), lower and upper limits of agreement (±1.96SD, standard deviation, peripheral dotted lines) and lower and upper confidence intervals (95%) are depicted. |
Discussion
Optical biometry is an essential procedure for preoperative planning in patients to be submitted to cataract surgery. Accurate measurements are fundamental to obtaining good refractive outcomes in general and in patients implanted with premium IOLs. It should also be considered that the time needed to obtain the preoperative measurements may affect the clinical flow. Then, both accurate and fast measurements should be considered to obtain excellent outcomes, without refractive surprises, and to improve daily clinical flow.
The IOLMaster 700 can provide a full biometric measurement of the eye plus the anterior and posterior corneal curvature. The present study shows that this device requires less time for acquiring measurements than standard IOLMaster 700 combined with a topographer (Cassini or Pentacam HR). Table 1 shows the mean acquisition times, where the mean value for this procedure takes about 20 seconds versus about three times more when the standard IOLMaster 700 is used in combination with the topographers (about 60 seconds, p < 0.001). These values pointed out the reduction in time required to obtain biometric parameters necessary for cataract surgery. A recent study published by Passi et al14 compared the efficiency of the SS-OCT IOLMaster 700 biometer with the Lenstar LS900 when acquiring biometric measurements during cataract evaluation. These authors analyzed 64 eyes of 32 patients on the same day using both optical biometers measuring the total image acquisition time per patient in order to compare both devices. They found that the average acquisition time to carry out a biometric measurement in both eyes was significantly shorter for the IOLMaster700 compare with the Lenstar LS900: 44.5 ± 12.4 versus 168.8 ± 67.2 seconds (p < 0.001). It was about 73% less for the IOLMaster 700. These results broadly agree with our values considering that the acquisition time in our study was registered for optical biometric measurement in one eye only. Passi et al14 considered that the time required to obtain this measurement deserves attention since it has the potential to impact clinical flow and patient experience. These authors confirmed that their results suggest that the IOLMaster 700 may be more efficient that the LS900 for biometry measurement during routine cataract evaluation. Our results show that there the use of the IOLMaster 700 with CT is more efficient than using this optical biometer without CT combined with corneal topographers.
In relation to comparison of the agreement between the topographic values obtained with the different devices, our results revealed that the values were statistically significantly different between them for all parameters and comparisons (p < 0.001) except for the comparison between the IOLMaster 700 and the Cassini (all parameters, p > 0.05, Table 2). Note that despite the significant differences, the mean values obtained for K1 and K2 for the three devices were small (<0.10D), being, therefore, clinically irrelevant. However, the LoAs (defined as the mean ±1.96 SD) for both parameters and the three comparisons showed values larger than 0.50D; then, we should consider that these devices cannot be used as interchangeable. These outcomes can be seen from Figure 1, which shows the different Bland-Altman plots for the three possible comparisons between devices: IOLMaster 700 vs Cassini, IOLMaster 700 vs Pentacam HR and Cassini vs Pentacam HR for K1 and K2. It shows the mean (continuous line), the lower and upper LoA (peripheral dotted lines) and the lower and upper CI (95%). Ozyol and Ozyol18 assessed the agreement between the IOLMaster 700 and the Pentacam HR in a sample of 62 eyes (62 healthy patients) and concluded that the mean keratometry should not be considered interchangeable. They found a mean difference of −0.20 ± 0.09 D with a LoA varying from −0.02 to −0.38 D (P < 0.001). Tañá-Rivero et al19 assessed the agreement of the IOLMaster 700 with the Pentacam AXL and found no statistically significant differences for K1 and K2 between the devices. Mean difference values were 0.09 and 0.14D for K1 and K2, respectively. The 95% LoA varied from −0.43 to 0.60D and −0.19 to 0.47D, for K1 and K2, respectively. Our results are similar to those reported by these authors and consider that LoA are wide and may have an important impact, especially when calculating a premium IOL such as a toric lens. Hidalgo et al20 compared the Pentacam HR and the Cassini in 20 eyes of 20 healthy volunteers and showed a 0.38 D of higher difference in keratometry (P < 0.05).
Mean values for TK1/TK2 and EKR1/EKR2 for the comparison between the Pentacam HR and the other two devices are slightly large (ranging from 0.29 to 0.45D). In addition, the LoA in these cases were width (about 1.50–2.00D). Figure 2 shows the Bland-Altman plots for four values and Table 2 shows the mean difference ± SD, the 95% CI, the 95% LoA, and the p values obtained for all comparisons. Then, these values should be kept in mind due to the possible clinical impact. We consider that the possible differences obtained between the different devices could come from the different technologies used in each one and the posterior data processing applied. Also, the area of analysis used for the calculations is different (2.5-mm for the IOLMaster 700 and 3-mm for the Pentacam HR and Cassini).
Wang et al21 recently compared the CT from the IOLMaster 700 with predicate topographic maps from a Placido disk-dual Scheimpflug tomographer in detection of irregularities that could influence the decision-making to implant premium IOLs such as a toric, multifocal or extended depth-of-focus. These authors analysed 105 eyes comparing the CT and the topographic maps and reported a similar shape in 68.6% to 89.5% of cases, and comparable map symmetries were reported in 60.0% to 83.8%. They indicated that the peripheral corneal steeping or flattening was the primary finding that was visible in the topographic maps but not in the CT. They concluded that both provided similar overall shape and comparable symmetries in most cases. Specifically, they concluded that the same decision was made whether to recommend a premium IOL based on CT and predicate topographic maps in 75% to 97% of cases.
Our study has some limitations, including the number of eyes including in the study and the use of only two corneal topographers. Future study should consider a large sample of eyes, the use of more commercial corneal topographers available in the market and the analysis of different IOL formulas using K readings from the different devices.
Conclusion
Our study shows that the acquisition time by the IOLMaster 700 with central topography takes approximately three less times than the use of a corneal topographer combined with a biometer. We consider that this is an efficient procedure that improves clinical flow. We also conclude that K readings obtained with the three devices cannot be used interchangeably since there are clinically relevant differences that may affect cataract surgery outcomes.
Data Sharing Statement
Data are not available for sharing.
Acknowledgments
We thank the collaboration of Paula Rodríguez and Gabriel Sanjuan in this study.
Funding
This study has been funded by an IIT Grant from Carl Zeiss (ESP-000101). Carl Zeiss did not have any role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38(12):2080–2087. doi:10.1016/j.jcrs.2012.08.036
2. Savini G, Naeser K. An analysis of the factors influencing the residual refractive astigmatism after cataract surgery with toric intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56(2):827–835. doi:10.1167/iovs.14-15903
3. LaHood BR, Goggin M. Measurement of posterior corneal astigmatism by the IOLMaster 700. J Refract Surg. 2018;34(5):331–336. doi:10.3928/1081597X-20180214-02
4. Montés-Micó R, Pastor-Pascual F, Ruiz-Mesa R, Tañá-Rivero P. Ocular biometry with swept-source optical coherence tomography. J Cataract Refract Surg. 2021;47(6):802–814. doi:10.1097/j.jcrs.0000000000000551
5. Wang L, Spektor T, de Souza RG, Koch DD. Evaluation of total keratometry and its accuracy for intraocular lens power calculation in eyes after corneal refractive surgery. J Cataract Refract Surg. 2019;45(10):1416–1421. doi:10.1016/j.jcrs.2019.05.020
6. Fabian E, Wehner W. Prediction accuracy of total keratometry compared to standard keratometry using different intraocular lens power formulas. J Refract Surg. 2019;35(6):362–368. doi:10.3928/1081597X-20190422-02
7. Srivannaboon S, Chirapapaisan C. Comparison of refractive outcomes using conventional keratometry or total keratometry for IOL power calculation in cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2019;257(12):2677–2682. doi:10.1007/s00417-019-04443-7
8. Kern C, El Kaissi L, Kortuem K, et al. Comparing refractive outcomes of a standard industry toric IOL calculator using anterior corneal astigmatism and total corneal refractive power. Graefes Arch Clin Exp Ophthalmol. 2020;258(2):345–350. doi:10.1007/s00417-019-04570-1
9. Shajari M, Sonntag R, Ramsauer M, et al. Evaluation of total corneal power measurements with a new optical biometer. J Cataract Refract Surg. 2020;46(5):675–681. doi:10.1097/j.jcrs.0000000000000136
10. Yeo TK, Heng WJ, Pek D, Wong J, Fam HB. Accuracy of intraocular lens formulas using total keratometry in eyes with previous myopic laser refractive surgery. Eye. 2020;35(6):1705–1711. doi:10.1038/s41433-020-01159-5
11. Lawless M, Jiang JY, Hodge C, Sutton G, Roberts TV, Barrett G. Total keratometry in intraocular lens power calculations in eyes with previous laser refractive surgery. Clin Exp Ophthalmol. 2020;48(6):749–756. doi:10.1111/ceo.13760
12. Levron A, El Chehab H, Agard E, Chudzinski R, Billant J, Dot C. Impact of measured total keratometry versus anterior keratometry on the refractive outcomes of the AT TORBI 709-MP toric intraocular lens. Graefes Arch Clin Exp Ophthalmol. 2021;259(5):1199–1207. doi:10.1007/s00417-020-05046-3
13. Savini G, Taroni L, Schiano-Lomoriello D, Hoffer KJ. Repeatability of total Keratometry and standard Keratometry by the IOLMaster 700 and comparison to total corneal astigmatism by Scheimpflug imaging. Eye. 2021;35(1):307–315. doi:10.1038/s41433-020-01245-8
14. Passi SF, Thompson AC, Gupta PK. Comparison of agreement and efficiency of a swept source-optical coherence tomography device and an optical low-coherence reflectometry device for biometry measurements during cataract evaluation. Clin Ophthalmol. 2018;12:2245–2251. doi:10.2147/OPTH.S182898
15. McAlinden C, Khadka J, Pesudovs K. Statistical methods for conducting agreement (comparison of clinical tests) and precision (repeatability or reproducibility) studies in optometry and ophthalmology. Ophthalmic Physiol Opt. 2011;31(4):330–338. doi:10.1111/j.1475-1313.2011.00851.x
16. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135–160. doi:10.1177/096228029900800204
17. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. doi:10.1016/S0140-6736(86)90837-8
18. Ozyol P, Ozyol E. Agreement between swept-source optical biometry and Scheimpflug-based topography measurements of anterior segment parameters. Am J Ophthalmol. 2016;169:73–78. doi:10.1016/j.ajo.2016.06.020
19. Tañá-Rivero P, Aguilar-Córcoles S, Tello-Elordi C, Pastor-Pascual F, Montés-Micó R. Agreement between 2 swept-source OCT biometers and a Scheimpflug partial coherence interferometer. J Cataract Refract Surg. 2021;47(4):488–495. doi:10.1097/j.jcrs.0000000000000483
20. Hidalgo IR, Rozema JJ, Dhubhghaill SN, Zakaria N, Koppen C, Tassignon MJ. Repeatability and inter-device agreement for three different methods of keratometry: Placido, Scheimpflug, and color LED corneal topography. J Refract Surg. 2015;31(3):176–181. doi:10.3928/1081597X-20150224-01
21. Wang L, Canedo ALC, Wang Y, Xie KC, Koch DD. Comparison of central topographic maps from a swept-source OCT biometer and a Placido disk-dual Scheimpflug tomographer. J Cataract Refract Surg. 2021;47(4):482–487. doi:10.1097/j.jcrs.0000000000000459
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.