Back to Journals » Risk Management and Healthcare Policy » Volume 13
Accurate Detection of Non-Cavitated Proximal Caries in Posterior Permanent Teeth: An in vivo Study
Received 29 May 2020
Accepted for publication 31 July 2020
Published 4 September 2020 Volume 2020:13 Pages 1431—1436
DOI https://doi.org/10.2147/RMHP.S264939
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Raghad Alammar,1 Durre Sadaf2,3
1Qassim University, College of Dentistry, Buraidah, Alqassim, Saudi Arabia; 2Conservative Dentistry Department, Qassim University, College of Dentistry, Buraidah, Alqassim, Saudi Arabia; 3University of Oxford, Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences, Oxford, UK
Correspondence: Raghad Alammar Tel +966 583573888
Email [email protected]
Purpose: This study aimed to compare the sensitivity and specificity of DIAGNOdent versus bitewing radiographs in detecting non-cavitated proximal caries.
Patients and Methods: This observational prospective study included 120 proximal surfaces, without obvious cavitation, on permanent mandibular and maxillary posterior teeth in patients over 16 years old. The DIAGNOdent test was performed, and digital bitewing radiographs were obtained; these were compared with a standard reference method, which comprised a clinical assessment of the proximal surfaces following the application of an orthodontic separator between the teeth for 7 days. Each test was performed by a different investigator blinded to the assessment results of the other examiners.
Results: The DIAGNOdent device exhibited a higher sensitivity in detecting enamel proximal caries (95%) than digital bitewing radiographs (64%), and the specificity of DIAGNOdent (89%) was greater than that of bitewing radiographs (77%). Regarding the detection of dentin caries, the sensitivities of DIAGNOdent and bitewing radiographs were similar (both 62%); however, the specificity of DIAGNOdent was higher (98% versus 88%). The results of the Kruskal–Wallis test revealed a significant difference in DIAGNOdent scores across the three diagnoses (sound tooth surfaces, enamel caries, dentin caries) (p-value < 0.001).
Conclusion: The diagnostic accuracy of DIAGNOdent in detecting enamel caries is significantly higher than that of digital bitewing radiography. The routine use of DIAGNOdent can facilitate an accurate diagnosis of early carious lesions and inform the implementation of preventive treatment.
Keywords: bitewing, dental caries, dentition, permanent, radiography
Introduction
Dentists most often rely on visual, tactile, and radiographic methods to detect dental caries.1 Carious lesions on proximal surfaces are formed cervical to the contact area, which makes their visualization challenging because of obstruction by the adjacent tooth. Therefore, carious lesions on proximal surfaces frequently remain undetected until they have extended well into the dentin.2 Therefore, the early detection of proximal caries is important, as any further progression of the lesion can be arrested by applying effective preventive measures.2
Bitewing radiographs are often unable to detect initial enamel lesions, and lesions have usually penetrated into the dentin by the time they are diagnosed.3 Furthermore, bitewing radiographs are unable to differentiate between lesions that are demineralized and not yet cavitated, and lesions that are truly cavitated; this may result in over-treatment, as non-cavitated lesions may be remineralized and do not require a restoration.4,5 Another problem associated with bitewing radiographs is that a proximal radiolucency does not always reflect a carious lesion; it may instead be a “cervical burn out,” which is a cervical radiolucency produced because of the decreased x-ray attenuation of the cementum. Therefore, it is essential to take a series of bitewing radiographs, usually at yearly intervals, to evaluate the progression of a lesion.2 Radiation exposure is another concern with radiography.6
In terms of clinical detection, the use of a probe is not only unreliable for detecting fissure caries, as it can become locked into the fissure, but it also damages teeth by creating an iatrogenic cavitation in the lesion that would otherwise have the potential to remineralize.7 Additionally, a previous study, which assessed the ability of clinical probing to diagnose caries in 100 extracted teeth with stained fissures, reported a low sensitivity (22%) for this detection method.8
Modern advancements in caries detection have resulted in improved specificity and sensitivity, compared to visual examination. DIAGNOdent (Kavo, Biberach/Riß, Germany) employs a red pulsed light (655 nm wavelength) to illuminate the tooth and detects the emitted fluorescent light from bacterial products, which differs with tooth demineralization.7 A numerical value is then provided, which corresponds to the intensity of the fluorescent light; this guides the decision of whether to perform preventive therapy or restorative treatment.7,9 Despite the potential of DIAGNOdent to aid in the clinical diagnosis of early proximal caries, prior literature providing direct comparisons with digital bitewing radiographs, in terms of sensitivity and specificity, is scarce. Therefore, the objective of this study was to determine the sensitivity and specificity of DIAGNOdent versus bitewing radiographs in the detection of non-cavitated proximal caries.
Patients and Methods
The protocol for this prospective observational study was reviewed and approved by the Qassim University Dental Research Center Ethics Committee, No. F-2018-3019. The study was conducted in accordance with the declaration of Helsinki. As the study was an observational, non-interventional, non-randomized study, it was exempt from trial registration. A convenience sampling technique was used for patient selection. Altogether, 120 proximal surfaces without obvious cavitation, on permanent mandibular and maxillary posterior teeth, were identified in 30 female patients over 16 years old who attended a university dental clinic in Saudi Arabia. The procedures and aims of the study were explained to potential participants, and informed consent was obtained.
Inclusion and Exclusion Criteria
Patients were included if they had permanent molars without restorations, hypoplasia, and cavitation on the proximal and occlusal surfaces. Exclusion criteria comprised patients (1) undergoing orthodontic treatment; (2) with a temporomandibular joint disorder; (3) with severe periodontitis or gingivitis; (4) who were pregnant; and (5) with cavitated teeth (including cases with a loss of the marginal ridge due to cavitation) or symptoms of pulpitis.
Three examiners were trained (by a dentist) to use the DIAGNOdent device, obtain bitewing radiographs, and perform visual-tactile inspection to detect non-cavitated proximal caries. Each examiner performed an independent assessment and was blinded to the assessment results of the other examiners. For the first 10 samples, three observers recorded their observation from each of the diagnostic tests: DIAGNOdent, bitewing radiographs, and clinical examination. Cohn’s kappa (k) test was performed to assess these outcomes; the inter-observer reliability for DIAGNOdent, bitewing radiographs, and clinical examinations were 0.82, 0.89, and 0.95, respectively.
DIAGNOdent Examination
The selected proximal surfaces were cleaned with a slow rotating bristle brush and dental floss. A laser fluorescence device, a DIAGNOdent pen (Kavo, Biberach/Riß, Germany) with a proximal tip (Probe tip 1), was used according to the manufacturer’s instructions. The DIAGNOdent device was first calibrated against a ceramic reference, for which the fluorescence value was known. After the standard calibration, the fluorescence value of a sound spot was recorded (zero value) and subsequently subtracted from the values assessed on the tooth surface.10 After a standardized drying time of 5 s using compressed air, the tip of the DIAGNOdent device was placed apical to the contact area and then moved to the marginal ridge, first from the buccal side and then from the lingual/palatal side; the peak value was recorded.11,12 The measurement was repeated three times on the side that had a higher peak value.11 The average of the three peak values from the same side was calculated. This value was recorded and subjected to the statistical analysis.13
Examination of the Bitewing Radiograph
Once the DIAGNOdent recordings of the teeth were completed, another examiner took digital bitewing radiographs under standardized conditions (ie, using an intraoral sensor with a bitewing sensor holder, and a paralleling long cone technique). A Heliodent DS intra-oral-x-ray unit with Sidexis intraoral sensors aligned perpendicular to a Rinn sensor holder (Sirona Company, Bensheim, Germany) at 60 kVp and 7mA was used. The sensor was exposed for 0.30 seconds.
The scoring system suggested by Marthaler was used.14 The frequency distribution of surfaces with a radiolucency in the outer half of the enamel indicated that scores of 1 or 2 (radiolucency in the outer and inner half of the enamel, respectively) should be combined into one group. Thus, the proximal surfaces were scored as follows: 0 = no radiolucency; 1 = radiolucency in the enamel; 2 = radiolucency in the outer half of the dentin; and 3 = radiolucency in the inner half of the dentin.12
Clinical Examination
The reference standard method (visual-tactile inspection) was performed by a third examiner 1 week after obtaining the DIAGNOdent device measurement and digital bitewing radiograph. The reference standard assessment required the temporary separation of proximal surfaces using orthodontic separators, which were placed between the selected contact points for 7 days.
After cleaning the separated proximal surfaces, an examination was conducted with a dental mirror and a World Health Organization periodontal probe. Proximal surfaces were classified as (i) sound (0 = no change in enamel translucency after air drying and absence of surface discontinuity); (ii) with a white/brown spot lesion (1 = white or brown discoloration on a wet or dried tooth, with no enamel discontinuity); or (iii) with a cavitated carious lesion (2 = loss of integrity of the surface detected visually and/or with the probe).6–15
Statistical Analysis
All data analyses were performed with the Statistical Package for Social Science software (SPSS version 24.0, IBM Corp., Armonk, NY, USA). The Kruskal–Wallis test was used to compare differences in the DIAGNOdent readings and bitewing radiographs among the three groups: sound (D0), enamel caries (D1-D2), and dentin caries (D3) (Table 1). The sensitivity, specificity, accuracy, positive predictive value, negative predictive value, and 95% confidence interval (CI) were subsequently calculated for the DIAGNOdent and bitewing radiographs at the cavitation and non-cavitation thresholds, using receiver operating characteristic (ROC) analyses. The cut-off values for the DIAGNOdent were determined in a way that provided the highest sum of sensitivity and specificity at the cavitation and non-cavitation thresholds. The area under the ROC curve (AUC) was used to calculate the accuracy and p-values of the two diagnostic methods.
 |
Table 1 Caries Interpretation Scores |
Results
The current study included 120 proximal surfaces from 30 patients (mean age = 22.5 ± 5.2 years). Altogether, 45 proximal surfaces were diagnosed as sound (D0), while 62 and 13 proximal surfaces were diagnosed as having enamel caries (D1-D2) and dentin caries (D3), respectively. One-third (32.6%) of the assessed surfaces were from upper molar teeth, and approximately one-fifth were from upper premolars (20.8%) and one-fifth from lower premolars and molars (23.3%).
The results of the Kruskal–Wallis test revealed a significant difference (p-value <0.001) in DIAGNOdent scores across the three groups (D0, D1-D2, D3) (Table 2). An inspection of the groups’ mean ranks suggested that D3 had the highest DIAGNOdent scores, while D0 had the lowest. Table 3 compares the sensitivity, specificity, positive predictive value, and negative predictive value for the detection of enamel and dentin caries. In terms of enamel caries, the DIAGNOdent device showed a higher sensitivity (95%) than the bitewing radiographs (64%). Similarly, the specificity of DIAGNOdent (89%) for enamel caries was greater than that of bitewing radiographs (77%). The positive predictive value indicates the probability of a test being positive if a disease is present and was higher with DIAGNOdent (91%) than bitewing radiographs (75%). The negative predictive value, which indicates the probability of a test being negative in the absence of a disease, was also higher with DIAGNOdent (94%) than with bitewing radiographs (67%). In terms of the detection of dentin caries, the sensitivities of DIAGNOdent and bitewing radiographs were similar (both 62%); however, the specificity of DIAGNOdent was higher (98% versus 88%).
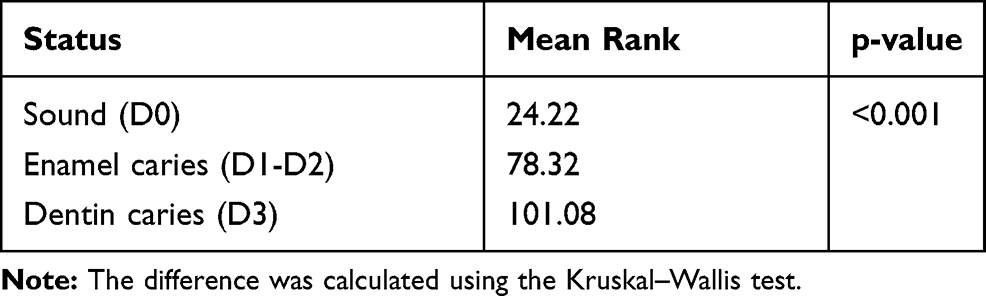 |
Table 2 Difference in DIAGNOdent Scores Across the Three Groups (D0, D1-D2, D3) |
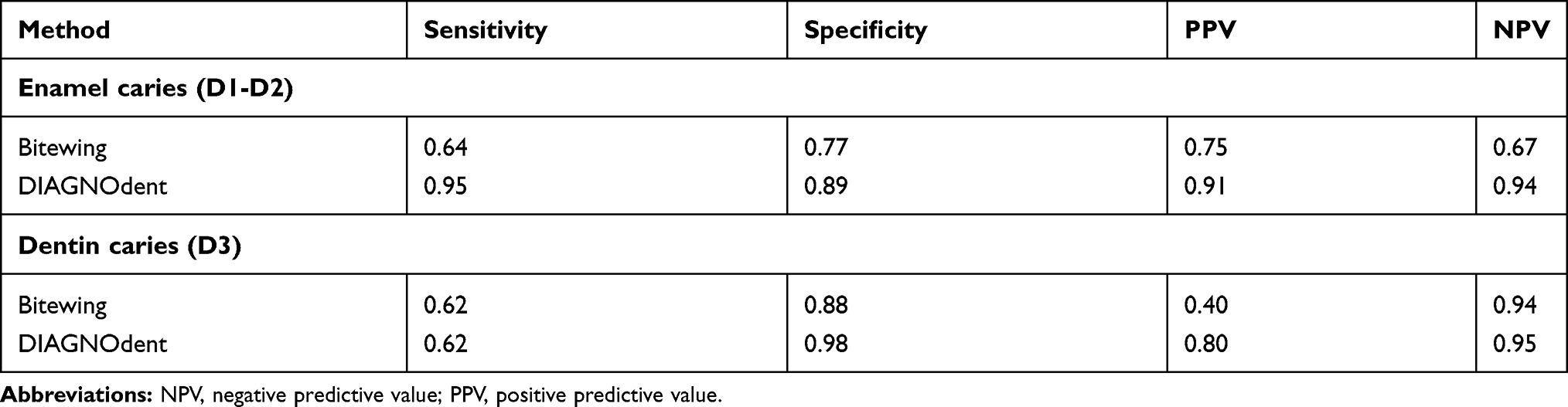 |
Table 3 Comparison of Sensitivity, Specificity, Positive Predictive Value, and Negative Predictive Value Between Bitewing Radiographic and DIAGNOdent Device Methods |
Figure 1 shows the ROC curve of the diagnostic performance of the DIAGNOdent device (blue line) and bitewing radiographs (green line) for enamel caries. The curve of the DIAGNOdent device was further to the left, thus indicating a higher accuracy. The area under the DIAGNOdent curve (0.807) was significantly greater than that for the bitewing radiograph curve (0.716; p-value <0.001). Figure 2 shows the ROC curve of the diagnostic performance of the DIAGNOdent device (blue line) and bitewing radiographs (green line) for dentin caries. The curve of the DIAGNOdent device was further to the left, thus indicating a higher accuracy. The area under the DIAGNOdent curve (0.879) was significantly greater than that for the bitewing radiograph curve (0.836; p-value <0.001).
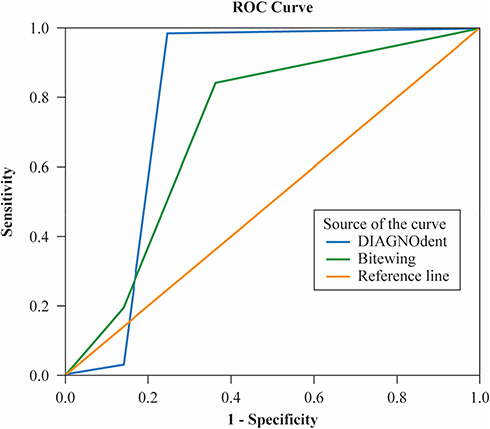 |
Figure 1 The receiver operating characteristic (ROC) curve of the diagnostic performance of the DIAGNOdent device (blue line) and bitewing radiographs (green line) in enamel caries (D1-D2). |
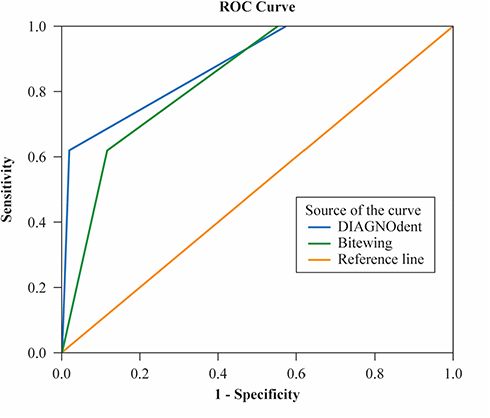 |
Figure 2 The receiver operating characteristic (ROC) curve of the diagnostic performance of the DIAGNOdent device (blue line) and bitewing radiographs (green line) in dentin caries (D3). |
Discussion
This study aimed to compare the diagnostic accuracy of DIAGNOdent with bitewing radiographs in detecting proximal caries. We recruited patients attending a dental hospital; therefore, the cut-off value identified in the current study is more generalizable to the population of patients attending dental care settings. Notably, this cut-off value is the same as that identified by Lussi et al,13 in an in vitro study evaluating 150 proximal surfaces on 75 permanent teeth using DIAGNOdent and bitewing radiographs. Their reference standard for caries was histological assessment.
The distribution of the diagnoses showed that approximately half of the cases had enamel caries, while only 10.8% were defined as having dentin caries. This was most likely because of the exclusion of teeth with obvious cavitation from the study. The sensitivity of a test is the probability that the test is positive, given a patient has the condition. The DIAGNOdent device had a higher sensitivity than bitewing radiographs for the detection of enamel caries (D1-D2). Nevertheless, previous studies have only reported a better performance for the DIAGNOdent device when used to detect occlusal dentin caries in primary teeth; this has been attributed to the mechanism of the device, which measures the fluorescence from the organic contents in carious lesions.16,17
DIAGNOdent also exhibited a higher sensitivity than bitewing radiographs in the detection of proximal caries on permanent teeth, and this was consistent with the results of Menem et al.18 This highlights the importance of DIAGNOdent in detecting early enamel lesions, and the potential role it has in informing the decision to employ preventive measures to arrest lesion progression. This is in contrast to bitewing radiographs, which are mainly effective for the detection of caries that have already reached the dentin.3
In terms of dentin caries (D3), both DIAGNOdent and bitewing radiographs had a similar sensitivity (62%). This was in contrast to the study conducted by Menem et al18 which reported a higher sensitivity for DIAGNOdent (100%); this may have been because of the combination of enamel and dentin caries (D1-D3) into a single category. Furthermore, only one examiner performed all three diagnostic tests in the study conducted by Menem et al,18 and this may have resulted in a bias toward a higher sensitivity with DIAGNOdent. In the present study, each of the three examiners performed independent assessments and were blinded to the assessments of the other examiners. The similar sensitivity between DIAGNOdent and bitewing radiographs in the diagnosis of dentin caries could also be attributed to the low percentage of dentin caries (10.8%) in the sample, as a diagnosis could often be made clinically without the need for additional diagnostic aids.
The specificity of a test is the probability that its result is negative, given the absence of the condition. The specificity of DIAGNOdent was greater than that of bitewing radiographs. In contrast, previous in vivo studies have reported a similar specificity for DIAGNOdent and bitewing radiographs when used for caries detection in primary teeth.11,12 Proximal carious lesions are usually detected by clinical inspection in combination with radiography, and it has been well-documented that radiography is the more sensitive of the two diagnostic methods.4 However, there remains a concern among both the public and dental profession toward the unavoidable hazards of ionizing radiation. DIAGNOdent may serve as an adjunct to conventional caries detection methods, especially in the diagnosis of early carious lesions and monitoring of caries progression and regression, and decrease the frequency of required radiographic examinations.
Limitations of the Study
A potential limitation of the current study was the low percentage of dentin caries (10.8%) in the sample, which could often be diagnosed clinically without the need for additional diagnostic aids. Nevertheless, the overall results indicated that DIAGNOdent had a better sensitivity and specificity than bitewing radiographs; therefore, it can be used as an alternative diagnostic method for the early detection of proximal caries in permanent teeth and continuous monitoring of lesions at regular intervals, with the added advantage of a lack of exposure to harmful radiation.
Conclusion
This study demonstrated that the diagnostic accuracy of DIAGNOdent is significantly higher than that of digital bitewing radiographs in detecting proximal enamel caries. Therefore, DIAGNOdent may serve as an adjunct to conventional caries detection methods, especially in the diagnosis of early carious lesions, and decrease the frequency of required radiographic examinations.
Abbreviations
AUC, area under the ROC curve; CI, confidence interval; ROC, receiver operating characteristic.
Disclosure
The authors report no conflicts of interest in this work. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
1. Bader JD, Shugars DA, Bonito AJ. A systematic review of the performance of methods for identifying carious lesions. J Public Health Dent. 2002;62(4):201–213. doi:10.1111/j.1752-7325.2002.tb03446.x.
2. Kidd E, Smith B, Watson T. Pickard’s Manual of Operative Dentistry.
3. Jacobsen J, Hansen B, Wenzel A, Hintze H. Relationship between histological and radiographic caries lesion depth measured in images from four digital radiography systems. Caries Res. 2004;38(1):34–38. doi:10.1159/000073918
4. Wenzel A. Radiographic display of carious lesions and cavitation in approximal surfaces: advantages and drawbacks of conventional and advanced modalities. Acta Odontol Scand. 2014;72(4):251–264. doi:10.3109/00016357.2014.888757
5. Baelum V, Hintze H, Wenzel A, Danielsen B, Nyvad B. Implications of caries diagnostic strategies for clinical management decisions. Community Dent Oral Epidemiol. 2012;40(3):257–266. doi:10.1111/j.1600-0528.2011.00655.x
6. Novaes TF, Matos R, Braga MM. Performance of a pen-type laser fluorescence device and conventional methods in detecting approximal caries lesions in primary teeth–in vivo study. Caries Res. 2009;43(1):36–42. doi:10.1159/000189705
7. Devlin H. Operative Dentistry: A Practical Guide to Recent Innovations. Heidelberg: Springer-Verlag Berlin; 2006.
8. Penning C, van Amerongen JP, Seef RE, Ten Cate JM. Validity of probing for fissure caries diagnosis. Caries Res. 1992;26(6):445–449. doi:10.1159/000261485
9. Bamzahim M, Shi XQ, Angmar-Månsson B. Secondary caries detection by DIAGNOdent and radiography: a comparative in vitro study. Acta Odontol Scand. 2004;62(1):61–64. doi:10.1080/00016350310008526
10. Rodrigues JA, Hug I, Lussi A. The influence of zero value subtraction on the performance of a new laser fluorescence device for approximal caries detection. Lasers Med Sci. 2009;24(3):301–306. doi:10.1007/s10103-008-0549-z
11. Chen J, Qin M, Ma W, Ge L. A clinical study of a laser fluorescence device for the detection of approximal caries in primary molars. Int J Paediatr Dent. 2012;22(2):132–138. doi:10.1111/j.1365-263X.2011.01180.x
12. Novaes T, Matos R, Raggio D, Imparato J, Braga M, Mendes F. Influence of the discomfort reported by children on the performance of approximal caries detection methods. Caries Res. 2012;44(5):465–471. doi:10.1159/000320266
13. Lussi A, Hack A, Hug I, Heckenberger H, Megert B, Stich H. Detection of approximal caries with a new laser fluorescence device. Caries Res. 2006;40(2):97–103. doi:10.1159/000091054
14. Marthaler T. A standardized system of recording dental conditions. Helv Odontol Acta. 1966;10:1–18.
15. Akbari M, Ahrari F, Hoseini ZH, Movagharipour F. Assessing the performance of the laser fluorescence technique in detecting proximal caries cavities. J Mashhad Dent Sch. 2013;37(3):185–200.
16. Braga M, Nicolau J, Rodrigues CR, Imparato JC, Mendes FM. Laser fluorescence device does not perform well in detection of early caries lesions in primary teeth: an in vitro study. Oral Health Prev Dent. 2008;6(2):165–169.
17. Alwas-Danowska HM, Plasschaert AJ, Suliborski S, Verdonschot EH. Reliability and validity issues of laser fluorescence measurements in occlusal caries diagnosis. J Dent. 2002;30(4):129–134. doi:10.1016/S0300-5712(02)00015-5
18. Menem R, Barngkgei I, Beiruti N, Al Haffar I, Joury E. The diagnostic accuracy of a laser fluorescence device and digital radiography in detecting approximal caries lesions in posterior permanent teeth: an in vivo study. Lasers Med Sci. 2017;32(3):621–628. doi:10.1007/s10103-017-2157-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.