Back to Journals » Clinical Ophthalmology » Volume 13
Accuracy, speed and repeatability of the voice assisted subjective refractor (VASR)
Authors Kabat AG ![]() , Lievens CW
, Lievens CW ![]() , Newman CM, Weber J
, Newman CM, Weber J ![]()
Received 24 April 2019
Accepted for publication 13 August 2019
Published 12 September 2019 Volume 2019:13 Pages 1807—1813
DOI https://doi.org/10.2147/OPTH.S213294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alan G Kabat,1 Christopher W Lievens,2 Christina M Newman,2 Jacob Weber2
1Pennsylvania College of Optometry, Salus University, Elkins Park, PA, USA; 2Southern College of Optometry, Memphis, TN, USA
Correspondence: Alan G Kabat
Pennsylvania College of Optometry, Salus University, 8360 Old York Road, Elkins Park, PA 19027, USA
Tel +1 954 553 1061
Fax +1 856 433 8439
Email [email protected]
Purpose: To compare the accuracy, speed and repeatability of the voice assisted subjective refractor (VASR) to traditional refractive methods.
Methods: Fifty healthy adult subjects were examined by autorefractor, followed by subjective phoropter refinement. Subjects were then evaluated using the VASR (Vmax Vision) to obtain an objective and subjective result. Three total assessments were performed for each subject using each of the methods described. Corrected visual acuity was recorded for each eye after each procedure. The total time was measured for both the traditional and VASR refraction.
Results: A comparison of the results obtained by traditional refraction and VASR revealed no statistically significant difference from the mean in equivalent sphere measurements (P=0.1383), and the datasets were highly correlated (r=0.993). The data comparisons for cylinder power and axis were similar (cylinder: P=0.6377, r=0.864) (axis: P=0.6991, r=0.738). VASR, on average, required 71 additional seconds to complete when compared to traditional phoropter refraction. In terms of repeatability, the average difference noted upon repeat of equivalent sphere power was 0.01 D for the phoropter (P=0.98) and 0.10 D for the VASR (P=0.23). For sphere power, the average difference was 0.02 D for the phoropter (P=0.55) and 0.07 D for the VASR (P=0.58). For cylinder power, the average difference was 0.02 D for the phoropter (P=0.11) and 0.03 D for the VASR (P=0.39). For all refractive methods, the differences between measurements amounted to ≤0.10 diopters, which is neither clinically nor statistically significant.
Conclusion: Refractive error results obtained with the VASR were not statistically different from those achieved using traditional phoropter methods. Time elapsed for the VASR was slightly longer than a more traditional refractive sequence. The VASR demonstrated clinically and statistically significant repeatability of measurement, consistent with traditional refraction.
Keywords: autorefractor, subjective refraction, wavefront aberrometry, point-spread function, VASR
Introduction
Automated refraction has been conceptualized by researchers of visual science since prior to World War II. Collins1 first described the Electronic Refractionometer in 1937, a system that employed infrared light to execute an objective assessment of refractive error, “the accuracy of which is neither dependent on the mental reactions of the patient or the perception of the operator.”2 The first functional, commercially available autorefractor did not appear until the 1970s, however. This device was developed by Safir, and marketed by Bausch & Lomb as the Ophthalmetron.3,4 Other early systems included the Dioptron (Coherent Radiation) and the 6600 Autorefractor (Acuity Systems, Inc.). As Collins had envisioned, all three of these devices utilized infrared light, although each relied on a different principle of examination to conduct an objective refraction in a manner previously acquired only by manual retinoscopy.5–7
The first fully subjective refracting system was developed by Humphrey8 in 1976, and was marketed as the Humphrey Vision Analyzer (HVA).9 This system had the capability to perform not only a spherocylindrical distance refraction, but near point evaluation and binocular testing as well. To its detriment, however, the HVA required its own refracting lane long enough to accommodate the exam chair, desk console, operator’s chair and an office desk size projection system along with a 30 cm diameter concave mirror situated 3 m from the patient.10 Additionally, the HVA had a steep learning curve, and required that the operator has a detailed working knowledge of refractive principles and spectacle correction.
Modern autorefractors use a variety of strategies (eg, infrared videorefraction, LED-driven imaging using the Scheiner principle, wavefront aberrometry) to obtain objective assessments of refractive error. Subjective capabilities have also been added to many of these units to allow for refinement of the objective measurements. Several of these instruments can measure visual acuity before and after refraction, and sphere, cylinder and axis can be adjusted in accordance with patient responses to various targets presented. The ultimate goal of these technological advances has always focused on providing faster, more accurate results while maintaining the smallest possible footprint within the eye care practitioner’s office. Moreover, the operation of these devices has been simplified to the point that a technician with very little training can produce reliable and repeatable results.
The voice assisted subjective refractor, a/k/a VASR (Vmax Vision, Maitland, FL, USA) is a unique digital refracting platform that utilizes wavefront aberrometry and point-spread function (PSF) technology combined with computer-generated artificial intelligence to conduct a complete objective and subjective refraction (Figure 1). It has been described as a “voice-guided self-refraction instrument”; the VASR prompts the patient through the subjective exam, and the patient responds to these prompts by means of a handheld remote. A technician monitors the process and validates visual acuity measurements, allowing the testing to proceed. The machine’s footprint is approximately 12ʺ×18ʺ, and a technician can be trained to confidently operate the device in a matter of just 2–3 hrs, according to the manufacturer. The utility of such an instrument lies in its ability to provide rapid, reliable and repeatable results without the direct, physical oversight of a physician. This clinical study compared the measurements obtained with the VASR by an inexperienced technician – in our case, a 2nd-year optometry student – to traditional phoropter refraction conducted by an experienced optometric clinician.
 |
Figure 1 The voice assisted subjective refractor, a/k/a VASR unit. |
Materials and methods
This study followed the tenets of the Helsinki Declaration and was approved by the Institutional Review Board at Southern College of Optometry (Memphis, TN, USA). Subjects were recruited from a large optometric facility and included professional students as well as college employees. Inclusion criteria were as follows: ≥18 years of age, current spectacle or soft contact lens wearer, and best-corrected monocular distance visual acuity of 20/25 or better in each eye. There was no restriction on the magnitude of refractive error. Exclusion criteria consisted of: use of rigid gas-permeable contact lenses, history of refractive surgery, and a known diagnosis of ocular disease that would affect refractive measurements (eg, corneal degenerations, disease or defects; retinal abnormalities; media or lens opacities). All participants provided written informed consent before commencing the study. A total of 50 healthy subjects aged 22–55 (mean 28 years) were examined by a masked investigator (AK, CL, CN) using the TonoRef™ II autorefractor (Nidek; Fremont, CA, USA) to obtain the objective measurement, followed by subjective refinement through the phoropter (monocular subjective refraction with binocular balance). Subjects were then evaluated by a different investigator (JW) using the VASR to obtain an objective and subjective refraction result. Phoropter values were measured in 0.25 diopter steps for both sphere and cylinder components, while VASR data were calculated to the nearest 0.01 diopter for sphere and cylinder. Final corrected visual acuity was recorded for each eye after each procedure using standard Snellen targets. The total time was measured via stopwatch for both the traditional refraction and the VASR refraction. This process of evaluation by autorefractor, subjective phoropter refraction and VASR refraction was repeated twice: once later on the same day as the initial evaluation, and again on a subsequent visit to validate the repeatability of the measurements.
Results
Fifty individuals participated in the study, however, one subject was excluded from analysis due to inadequate responsiveness during subjective testing. Sphere, cylinder and axis values from the right and left eyes were recorded for each procedure (ie, autorefraction, manifest refraction and VASR refraction), and equivalent sphere power was then calculated. Elapsed time for each individual procedure was also recorded, as well as the final-corrected visual acuity. To eliminate confusion, unilateral measurements (OD only) were analyzed with regard to refractive values.
Equivalent sphere power for the manifest refraction ranged from +1.13 to −12.75 (95% CI = −1.63 to −3.63), with a median of −2.50. For VASR, values ranged from +1.08 to −14.39 (95% CI = −1.26 to −3.46), with a median of −2.69. In this regard, a high correlation (R=0.99) was noted between the manifest and VASR (Figure 2). The datasets for both refractive methods displayed a negative skew (manifest = −1.23, VASR = −1.46), which is to be anticipated in this particular population; most of the subjects were graduate students, who tend to have a higher prevalence of myopia (Figure 3).11,12 Platykurtosis was also observed (manifest = 1.79, VASR = 2.85). Because of these factors, non-parametric analyses were performed using the Wilcoxon test.
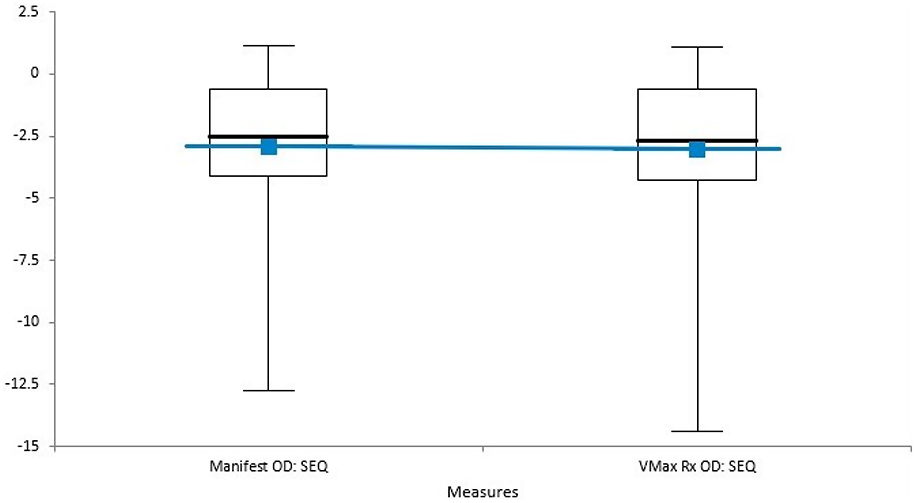 |
Figure 2 Box plot of results (Manifest vs VASR). |
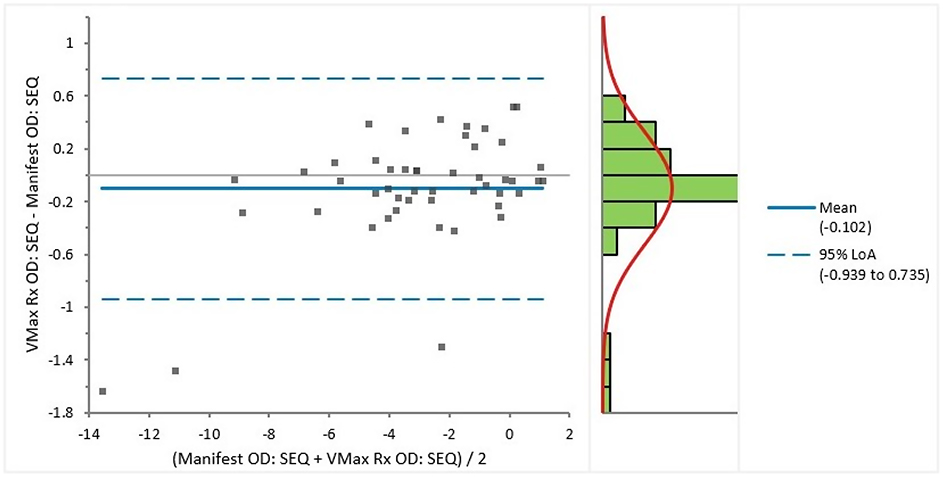 |
Figure 3 Difference plot. |
No statistically significant difference from the mean was noted for equivalent sphere values between manifest and VASR refractions (P=0.14). A high correlation was likewise noted for cylinder power (R=0.86, P=0.64) and axis (R=0.74, P=0.70). Corrected visual acuity measurements were similar for both groups; 16% of subjects had better acuity with VASR (≥1 line Snellen), while just 4% of subjects had worse acuity with VASR (≥1 line Snellen). 80% of subjects experienced a difference of <1 line of Snellen between techniques.
In terms of elapsed time, manifest refraction averaged 5 mins, 38 s (range = 3:00–9:00), including autorefraction and subjective refinement with cross-cylinder testing and binocular balance. The VASR averaged 6 mins, 47 s (range = 4:35–11:03) to complete both eyes, including objective wavefront analysis and subjective PSF refinement. Measurement of final-corrected visual acuity was included in the time calculations.
To determine the repeatability of the procedures, a total of three refractive assessments were obtained for each subject. The first trial (T1) was conducted at a morning visit. The second (T2) was performed in the afternoon on same day but at least 6 hrs after T1, while the third (T3) was conducted on a separate day, at least 24 hrs but no more than 1 week after T2. Datasets for these trials were then assessed by ANOVA. The average differences noted upon repeat testing of spherical power were 0.02 D for the autorefractor (P=0.62), 0.02 D for the manifest refraction (P=0.55) and 0.07 D for VASR (P=0.58). The average differences noted upon repeat testing of cylinder power were 0.01 D for the autorefractor (P=0.49), 0.02 D for manifest refraction (P=0.11) and 0.03 D for VASR (P=0.39) (Figures 4 and 5). The average differences noted upon repeat testing of spherical equivalent power were 0.03 D for the autorefractor (P=0.43), 0.01 D for manifest refraction (P=0.98) and 0.10 D for VASR (P=0.23).
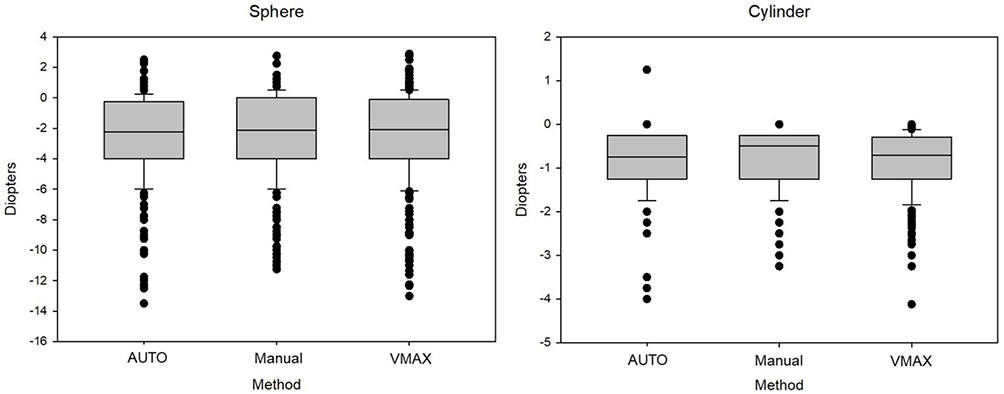 |
Figure 4 Repeatability of sphere and cylinder power. |
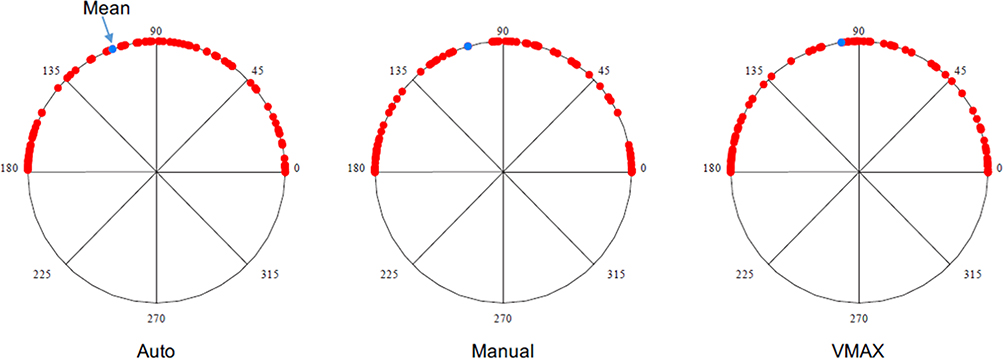 |
Figure 5 Distribution of axis orientation. |
Discussion
Overall, the outcomes obtained with the VASR proved to be reliable and efficient with regard to accuracy, speed and repeatability. In the determination of spherocylindrical refractive error, the VASR results were not statistically different from those achieved using traditional phoropter methods by an experienced optometrist. Final, corrected visual acuity was similar between groups, and the differences noted between methods were not clinically significant.
The elapsed time for the VASR sequence was found to be slightly greater than for the traditional phoropter refraction, averaging 71 s longer. To this point, however, several considerations must be made. First, refraction time can vary greatly from patient to patient, and there is no normative value for this sequence of testing. In most cases with a cooperative individual, an experienced clinician can perform a complete objective and subjective refraction in roughly 5–10 mins. By means of comparison to other instruments, an evaluation of the Topcon (Tokyo, Japan) BV-1000 Automated Subjective Refraction System with a similar cohort revealed a mean test time of 9:45±0.11 mins.13 In our study, the VASR beat this time by nearly 3 mins. Second, it must be noted that the VASR – like most autorefractors – is designed to be operated by a technician rather than the optometrist or ophthalmologist. If this duty is delegated to office staff, then the small difference in time becomes negligible in comparison to the overall reduction in face-to-face time between doctor and patient.
Finally, the VASR was found to be highly repeatable with regard to the measurement of sphere power, cylinder power and spherocylindrical power. For all refractive methods – autorefractor, manifest refraction and VASR – the differences between measurements amounted to ≤0.10 diopters, which is neither clinically nor statistically significant.
The results of this study as displayed clearly demonstrate the accuracy, speed and repeatability of the VASR when compared to traditional refractive methods. The strengths of the study include a robust cohort of subjects, consistency of the operator performing VASR to eliminate testing bias, and testing on different days and at different times in order to account for fatigue. Variability was well-controlled by utilizing the same examination rooms and equipment for all subjects, with standardized lighting and acuity charts. However, this study is not without its limitations. The selected cohort consisted primarily of young, healthy individuals, a good majority of whom were familiar with the refractive process by virtue of being optometry students. This could possibly have biased the phoropter refraction results, causing them to be faster than might be anticipated in a similar age-matched population.
Additionally, the exclusion of subjects with ocular disease allowed for a less complicated and likely faster refractive assessment, both for the traditional manifest as well as the VASR. By that same process, however, we are unable to comment on the accuracy or repeatability of VASR in patients whose vision might be compromised due to such disorders like cataract or macular degeneration. A forerunner of VASR, the PSF Refractor (Vmax Vision) has previously been assessed by Trattler in keratoconus patients.14 That study of 14 patients (28 eyes) concluded that the PSF autorefractor
produces a more reliable and accurate refraction outcome in visually challenged patients such as keratoconus and cataracts. It is easier for the patient and provides the best corrected visual acuity when compared to a phoropter.14
It also bears mentioning that while the traditional manifest refraction in our study included binocular balancing, the VASR does not permit or facilitate any such binocularity. Some view this as a drawback of the VASR; others however have implied that such testing is unnecessary when utilizing a PSF system for refraction. The goal of the binocular balance is to equalize the accommodative response for the two eyes. The procedure is deemed necessary (in those with normal accommodative capacity and equivalent visual acuity in both eyes) because occlusion of the untested eye during monocular refraction can itself stimulate accommodation, and by Hering’s law of equal innervation, this results in accommodation by the unoccluded eye as well.15 Hence, the binocular balance can be used as a means of determining the appropriate sphere power for each eye while preventing the clinician from “over-minusing” the patient during traditional phoropter refraction. The PSF target is different from standard Snellen optotypes, however, in that it is far more sensitive to defocus. Subjects tested with this system can perceive small changes from the optimal refraction much more clearly. The “smaller and darker” effect that can result with over-minusing behind the phoropter is perceived as blur by the same subject when viewing a PSF target. Geffen and Brujic16 in a study of 30 patients, assessed the results of subjective phoropter refraction with binocular balancing as compared to monocular refraction without binocular balance using the PSF Refractor. Their study concluded that, in 70% of patients, the spherical equivalent obtained with the PSF device was within 0.13 D of the phoropter refraction, and more than 0.25 D different in just 3%. PSF refraction results were equal to or better than those obtained with the phoropter binocular method in 93.5% of patients.16 This suggests that the inability to perform binocular testing with VASR may not be a detriment at all.
Another potential limitation of the study design involved the use of only the right eye data in the analysis. While this was considered a necessary element in order to maintain consistency of the data, the authors unknowingly introduced a potential bias by following this protocol. Since the right eye was consistently tested before the left, there may have been some “learning” by the subjects with regard to the Vmax. This could have potentially extended the testing time for the right eye as compared to the left eye. Randomization of testing with regard to the right and left eye might have yielded additional or different findings.
Finally, it was the authors’ decision to use Snellen visual acuity measurement for this study in an effort to make the results as clinically relevant to the practicing clinician as possible. However, it should be noted that the VASR can also be programmed to measure visual acuity using ETDRS (i.e. LogMAR) as well as Lea or Allen symbols. These alternative strategies may be helpful for future studies evaluating different populations, and may potentially provide greater accuracy.
Acknowledgments
Financial support for this study was provided in the form of an educational grant by Vmax Vision, Inc. The company did not play any role in manuscript preparation, study design, or the decision to publish. This data set and its conclusions were originally presented as two posters at the Association for Research in Vision and Ophthalmology (ARVO) Annual Meeting 2018. The posters’ abstracts were published in Investigative Ophthalmology and Visual Science, July 2018, Vol.59, 1283–1284; https://iovs.arvojournals.org/article.aspx?articleid=2689763; https://iovs.arvojournals.org/article.aspx?articleid=2689764.
Disclosure
Dr Kabat reports grants, personal fees, non-financial support from Vmax Vision, Inc., during the conduct of the study, personal fees, non-financial support from Bruder Healthcare Company, Inc., personal fees, non-financial support from Jobson Healthcare Information, personal fees from Kala Pharmaceuticals, Lacrivera, Ocusoft, Inc., National Vision Administrators, LLC, Quidel, Sight Sciences, Sun Pharmaceuticals, Takeda Pharmaceutical Company (formerly Shire), personal fees, non-financial support from Avellino Labs, grants, personal fees from Bio-Tissue, Inc., personal fees, non-financial support from EyeGate Pharma, personal fees from TearScience, grants from Thermi, personal fees from BlephEx, outside the submitted work. Dr Kabat is a consultant for Vmax Vision. Dr Lievens reports grants from Southern College of Optometry, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Collins G. The electronic refractionometer. Br J Physiol Optics. 1937;11:30–42.
2. Collins G. The electronic refractionometer. Aust J Optom. 1939;22:122–132.
3. Knoll HA, Mohrman R. The ophthalmetron, principles and operation. Am J Optom Arch Am Acad Optom. 1972;49:122–128. doi:10.1097/00006324-197202000-00006
4. Floyd RP, Garcia G. The ophthalmetron: a clinical trial of accuracy. Arch Ophthalmol. 1974;92:10–14. doi:10.1001/archopht.1974.01010010014004
5. Sloan PG, Poise KA. Preliminary clinical evaluation of the Dioptron. Am J Optom Physiol Opt. 1974;51(3):189–197. doi:10.1097/00006324-197403000-00004
6. Polse DA, Kerr KE. An automatic objective optometer. Description and clinical evaluation. Arch Ophthalmol. 1975;93:225–231. doi:10.1001/archopht.1975.01010020233013
7. Pappas CJ, Anderson DR, Briese FW. Clinical evaluation of the 6600 Autorefractor. Arch Ophthalmol. 1978;96:993–996. doi:10.1001/archopht.1978.03910050517001
8. Humphrey WE. Automatic retinoscopy: the humphrey vision analyzer. Optician. 1977;173:17–27.
9. Elmstrom G. Humphrey vision analyzer. J Am Optom Assoc. 1976;47:973–974.
10. Efron N. Instrument review: the humphrey vision analyser. Aust J Optom. 1981;64:149–153.
11. Al-Rashidi SH, Albahouth AA, Althwini WA, et al. Prevalence refractive errors among Medical Students of Qassim University, Saudi Arabia: cross-sectional descriptive study. Open Access Maced J Med Sci. 2018;6:940–943. doi:10.3889/oamjms.2018.221
12. Mountjoy E, Davies NM, Plotnikov D, et al. Education and myopia: assessing the direction of causality by mendelian randomisation. BMJ. 2018;361:k2022. doi:10.1136/bmj.k2022
13. Dave T, Fukuma Y. Clinical evaluation of the Topcon BV-1000 automated subjective refraction system. Optom Vis Sci. 2004;81:323–333.
14. Trattler WB. Comparative evaluation of subjective point-spread function refraction results with subjective phoropter results on keratoconus patients.
15. Momeni-Moghaddam H, Goss DA. Comparison of four different binocular balancing techniques. Clin Exp Optom. 2014;97:422–425. doi:10.1111/cxo.2014.97.issue-5
16. Geffen D, Brujic M. Is binocular balancing with subjective refraction a thing of the past? Poster presented at Optometry’s Meeting (American Optometric Association), June 27, 2015. Seattle, WA.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.