Back to Journals » Patient Preference and Adherence » Volume 13
Accountability in patient adherence
Authors Oussedik E, Cline A ![]() , Su JJ, Masicampo EJ, Kammrath LK, Ip E, Feldman SR
, Su JJ, Masicampo EJ, Kammrath LK, Ip E, Feldman SR ![]()
Received 23 April 2019
Accepted for publication 27 August 2019
Published 4 September 2019 Volume 2019:13 Pages 1511—1517
DOI https://doi.org/10.2147/PPA.S213113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Elias Oussedik1,2, Abigail Cline1, Jennifer J Su1, EJ Masicampo3, Lara K Kammrath3, Edward Ip4, Steven R Feldman1,5,6
1Center for Dermatology Research, Department of Dermatology, Wake Forest School of Medicine, Winston-Salem, NC, USA; 2Faculty of Medicine, McGill University, Montreal, QC, Canada; 3Department of Psychology, Wake Forest University, Winston-Salem, NC, USA; 4Department of Pathology, Wake Forest School of Medicine, Winston-Salem, NC, USA; 5Department of Public Health Sciences, Wake Forest School of Medicine, Winston-Salem, NC, USA; 6Department of Dermatology, University of Southern Denmark, Odense, Denmark
Correspondence: Abigail Cline
Center for Dermatology Resarch, Department of Dermatology, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157-1071, USA
Tel +1 336 716 7740
Fax +1 336 716 7732
Email [email protected]
Background: The accountability inherent in the social interaction between a patient and healthcare provider affects patients’ motivation to adhere to treatment. To characterize the role of accountability as a tool to improve self-efficacy and self-management and thereby promote patients’ adherence to treatment, a measure of accountability is needed.
Aims: To develop and test the validity, reliability, and sensitivity of a new outcome measure designed to assess accountability.
Methods: The accountability measurement tool was developed from the literature, expert consultation, and focus groups. A focus group and three pilot studies were performed both in clinic and through an online crowdsourcing platform. Principal Component Analysis evaluated constructs, and Cronbach’s alpha measured internal consistency. Validity was established using convergent and divergent correlations to other validated scales.
Results: A total of 292 participants took part in this study. The 12-item accountability scale demonstrated very good internal consistency (Cronbach’s α=0.92). Components of the accountability measurement tool correlated with predicted validated measures, including the Treatment Self-Regulation Questionnaire. Divergent validity was established with no significant difference noted between age, sex, race, and education level.
Conclusion: Future use of this questionnaire will allow for the assessment of the interaction between accountability and adherence to treatment and lead to the development of new interventions to promote better adherence.
Keywords: accountability, adherence, self-determination theory, self-efficacy, patient behavior
Introduction
Nonadherence is a significant medical problem that can lead to increased morbidity, mortality, and excessive health care expenditures.1 While researchers and practitioners have had a long-standing interest in adherence, the effectiveness of interventions has been limited. New approaches are needed, and socially-centered interventions may prove valuable.
The accountability derived from the expectation of a social interaction between the patient and the healthcare provider may affect patients’ motivation to adhere to treatment. Accountability is a novel psycho-behavioral theoretical construct that is missing from health behavior models.2 Accountability refers to the implicit or explicit expectation that an individual may be called upon to account for his or her actions or inactions.3 Accountability requires social presence— which can be by telephone, by email, or in person—the latter of which is considered the most influential.4–6 From weekly addiction meetings to piano lessons; the anticipation of an expected social interaction encourages adherence. Similarly, medication adherence increases around the time of office visits.7 Despite accountability being present in multiple spheres of human behavior, the importance of accountability has been largely missed in existing health behavior models. To better understand the role accountability in adherence, a measure of the accountability construct is needed.
Herein, we report on the development of the accountability model, the generation of sample items, and the face and construct validity of the Accountability Measurement Tool (AMT). The objective of this study was to produce a validated accountability measurement that can be incorporated into health behavior models, research, clinical care, product development and can better define how accountability may best be used to increase patient adherence.8–10
Methods
Development of the accountability measurement tool
This study and the protocols used in the study were approved by the Institutional Review Board of Wake Forest Baptist Health. Informed consent was provided by all participants either in person or through an online portal.
Guided by the Self-Determination Theory and Bandura’s theory of self-efficacy, a prototype set of 18 questions relevant to accountability related to health behavior was developed and grouped into three theoretical domains: controlled accountability, autonomous accountability, and general accountability.2,11 To be able to detect small changes, each item was scored on a 5-point Likert scale (from 1, strongly disagree to 5, strongly agree).
The first phase consisted of focus group discussions of the prototype scale. Participants were eligible if they were dealing with a chronic disease as defined by the US National Center for Health Sciences, a working knowledge of English, and prescribed at least one medication for the past month and expected to continue for another month.12 Three separate focus groups of 6–8 participants with an equal mix of men and women tested the original set of 18 questions. The focus group involved of four parts: (1) open discussion, during which participants discussed definitions and aspects of accountability; (2) question by question review, during which participants read the accountability questions developed by a panel of experts; (3) filling the gaps, during which subjects discussed what areas of accountability need to be included; and (4) filling in the questionnaire on paper, during which subjects filled in the AMT along with other validated measures, including the Brief Fear of Negative Evaluation Scale (BFNE) and the Treatment Self-Regulation Questionnaire (TSRQ). The BFNE is a self-report questionnaire which assesses fear and worry about receiving negative evaluation from others. Participants indicate how characteristic each of the 12 statements is of them on a 1–5 Likert-type scale. The TSRQ is a self-report questionnaire which assesses domain-specific types of motivation or regulation. Participants indicate how true each of the 15 statements is on a Likert-type scale ranging from 1=“Not at all true” to 7=“Very true”.
In the second phase, three pilot studies were conducted for data collection. Data collected from all participants were analyzed to improve the accountability questionnaire. In addition to completing the three questionnaires (the AMT, BFNE, and TSRQ), basic demographic questions were also collected.
Phase three was instrument modification. Following the completion of each pilot study, the accountability questionnaire was slightly modified with either the addition or deletion of items depending on statistical analysis. During the third pilot study, a 12-item accountability measurement tool was finalized.
Phase four was instrument validation. The finalized 12-item AMT was administered. Demographics data, including race, ethnicity, sex, and education level was collected. Respondents were asked the length of time they had been with their medical provider, if they ever had a disagreement with their provider, and whether they were overall satisfied with their provider. Along with the AMT, respondents in this phase took the BFNE, the TSRQ, the Satisfaction with Life Scale, and the Emotional Regulation Questionnaire to assess convergent and divergent validity.13,14 A subset of 15 respondents completed the AMT a second time 4 weeks after the initial administration.
All study procedures were subject to ethical approval by the Wake Forest University School of Medicine Institutional Review Board (Winston-Salem, NC, USA).
Setting
All focus group participants were recruited in ambulatory clinic. Participants in the pilot studies and validation were recruited either through ambulatory clinic or through Amazon’s Mechanical Turk (MTurk), an online crowdsourcing platform. MTurk is a validated tool in conducting research in social sciences and allows for representation as diverse as traditional samples.15 The use of an online crowdsourcing platform allowed for the recruitment of a larger sample in a shorter time frame. Inclusion criteria were as follows: subjects with a chronic disease as defined by the US National Center for Health Statistics, a working knowledge of English, a prescription for at least one medication, subjects with a regular health provider who they had seen at least twice during the past two years, and age 18 years or older.12
Statistical analysis
We calculated descriptive statistics for the participant demographics and the accountability measurement tool. An exploratory factor analysis of 18 items identified items we retained for the final questionnaire. Scree plot and eigenvalues items were evaluated by their factor loadings and by their item-to-total correlations. Items with high factor loadings (>0.50) and at least a moderate correlation (>0.50) with the total scale were retained. Cronbach’s α estimated the internal consistency of each scale, and mean inter-item correlations were calculated to further demonstrate internal consistency. Cronbach’s α values of 0.7–0.8 are considered satisfactory.16 Item analysis assessed inter-item and corrected item-total correlations for indications of incongruence or redundancy of items. Values for Cronbach’s α were examined if certain items were deleted.
After we selected the final items for the AMT, we used bivariate correlation analyses and Student t-tests to assess its validity. Construct validity can be inferred from predicted associations between the scale (AMT) and other variables. These include predicted associations (convergent validity) and predicted lack of association (divergent validity). We predicted that the AMT autonomous accountability score would associate with TSRQ autonomous motivation score, that the AMT controlled accountability score would associate with the TSRQ external motivation score, and that overall satisfaction with medical provider would associate with accountability. We also predicted that the AMT would associate with age, education level, sex, Satisfaction with Life Scale, and Emotional Regulation Scale. All t-tests were two-sided, and p-values less than 0.05 were considered significant.
To evaluate the AMT’s test-retest reliability, we calculated the intraclass correlation coefficient for two administrations of the AMT to a subset of 15 respondents within a 4-week period.
Results
Participant characteristics
A total of 292 participated in the study (Table 1), 27 were recruited through clinic and 265 were recruited through MTurk. There were few differences between the groups given paper-and-pencil (n=27) and web-based (n=265) surveys. The subsample completing the paper-and-pencil survey had an older mean age (56 vs 29, p<0.0001); however, both groups were majority female and Caucasian. Neither the total AMT scores (40 vs 46), the BFNE score (23 vs 21), nor the total TSRQ score (65 vs 65) differed across administration modalities (p>0.5).
 |
Table 1 Patient demographics |
Item reduction and reliability
Determination of poorly-worded or redundant items by focus groups and examination of poor Cronbach’s α values led to the removal of six items from the original 18-item set.
The scree plot from the factor analysis demonstrated that two factors had eigenvalues>1. The eigenvalue 6.39 accounted for 53.3% of the variance and the eigenvalue 1.12 accounted for 9.35% of the variance. The two main factors were autonomous accountability (6 items) and controlled accountability (6 items) (Table 2). Communalities ranged from 0.45 to 0.75.
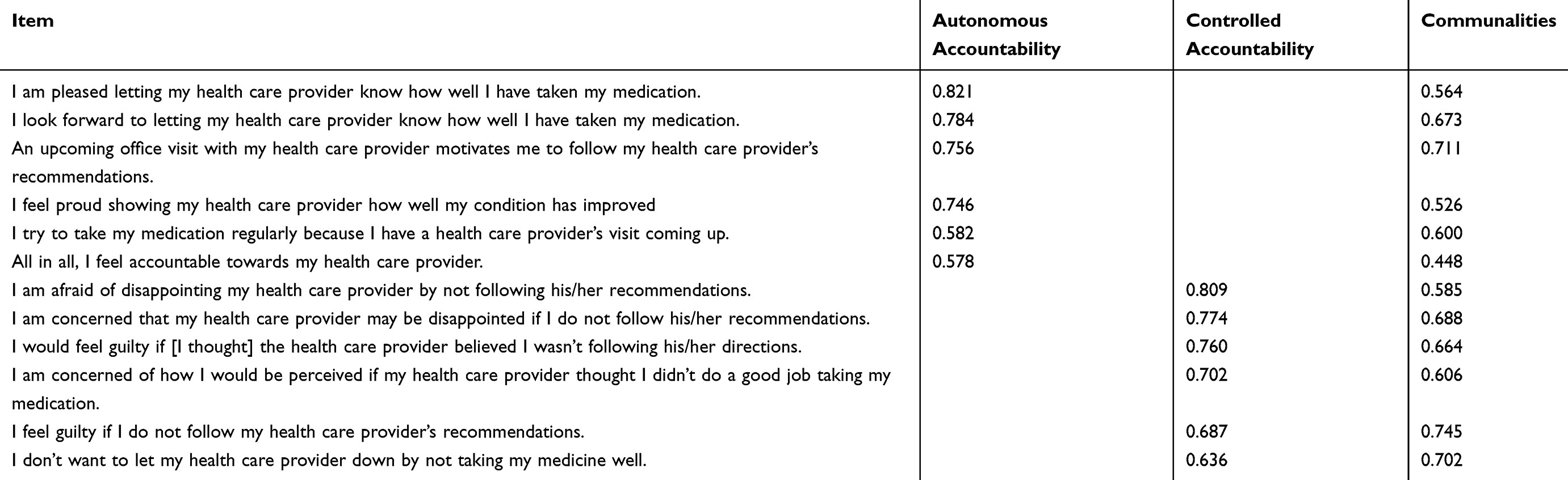 |
Table 2 Main factors and communalities for the accountability measurement tool |
Cronbach’s α coefficient for the resulting 12-item scale was 0.92, reflecting a high degree of internal consistency. The α coefficients for the autonomous and controlled accountability subscales were also excellent (α=0.87 and 0.88). Review of item-to-total correlations demonstrated a range from 0.57 to 0.75 (Table 3).
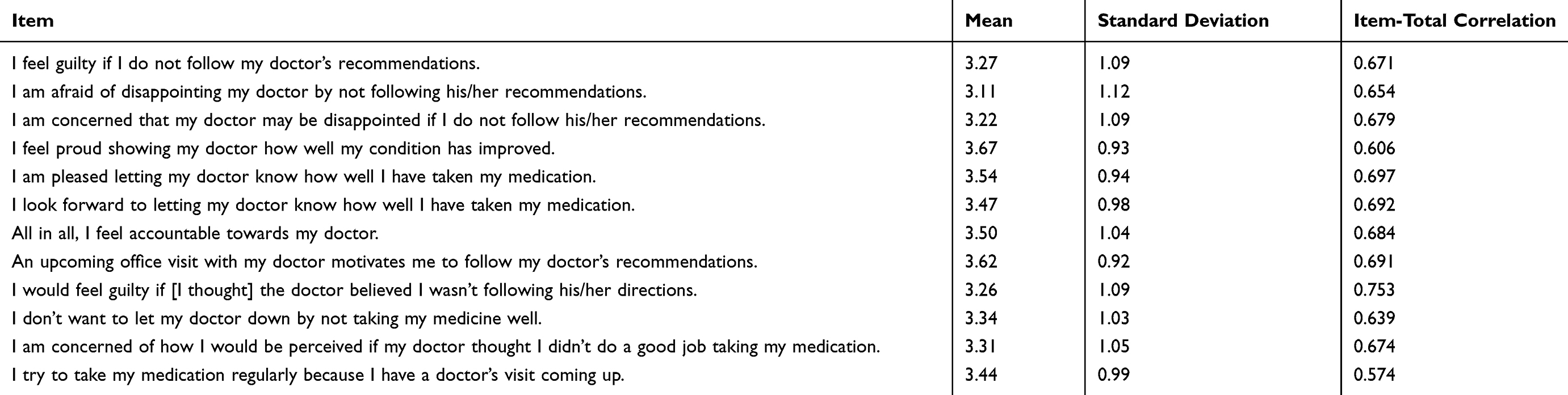 |
Table 3 Means, standard deviations, and correlations for the accountability measurement tool |
The test-retest administrations for the AMT total score was high, as calculated by parametric method (Pearson correlation r=0.91, p<0.01) and nonparametric method (Spearman’s Rho r=0.79, p<0.01). The component accountability measurement scores were also high for the test-retest: internal accountability (Pearson correlation r=0.89, p<0.01 and Spearman’s Rho r=0.84, p<0.01), external accountability (Pearson correlation r=0.74, p<0.01 and Spearman’s Rho r=0.70, p<0.01), and general accountability (Pearson correlation r=0.83, p<0.01 and Spearman’s Rho r=0.61, p<0.05).
Construct validity
Using the 12-item AMT measure, the relationship between accountability and the fear of negative evaluation was examined using Pearson’s correlation coefficient. There was slight positive correlation between total accountability and BFNE (r=0.31) and controlled accountability and BFNE (r=0.34) (Table 4).
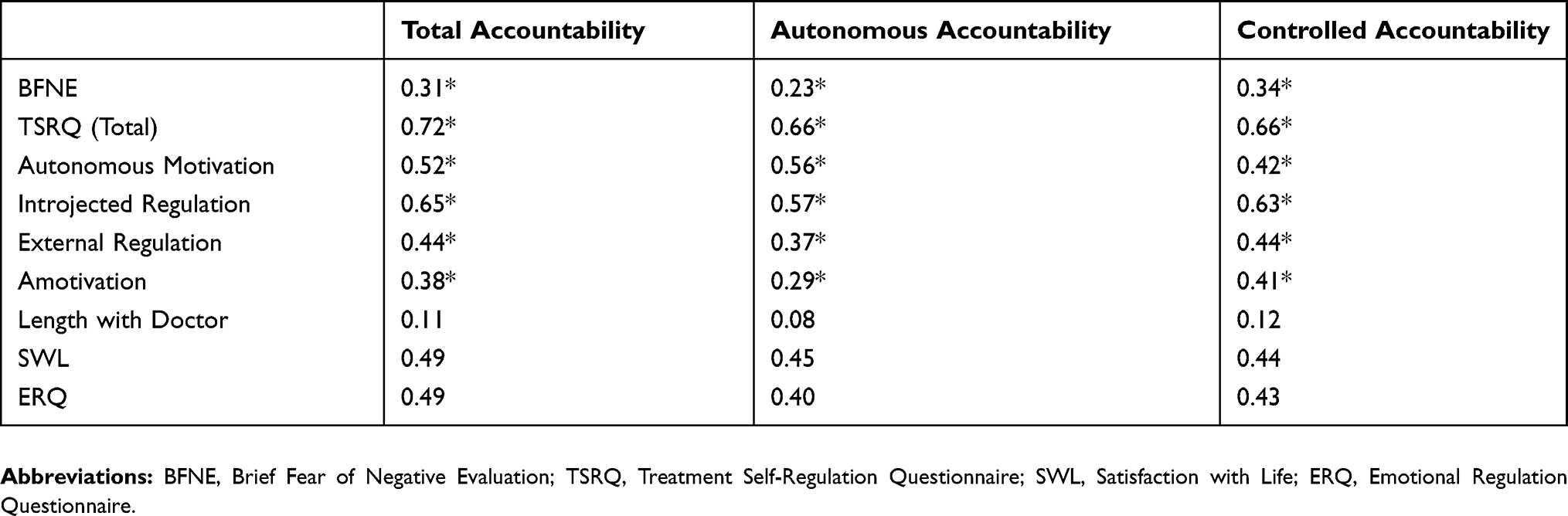 |
Table 4 Correlations between the AMT and other validated scales |
Regarding the TSRQ, autonomous motivation correlated with total accountability (r=0.52), autonomous accountability (r=0.56), and controlled accountability (r=0.42). Introjected motivation positively correlated with total accountability (r =0.65), autonomous accountability (r=0.57), and controlled accountability (r=0.63). External motivation correlated most strongly with total and controlled accountability (r=0.44). Amotivation correlated most strongly with controlled accountability (r=0.41) (Table 4). Reported length with provider did not correlate with total accountability or any of its factors. Reported satisfaction with medical provider did influence accountability. Respondents reporting satisfaction with their provider had higher total accountability compared to those who reported dissatisfaction (41.6 vs 33.0, p<0.005).
Non-significant associations between the AMT and age (r=−0.08), education (r=−0.17), and race (r=−0.23) support divergent validity. T-test revealed no difference of AMT scores between men and women (p=0.3). However, total accountability did positively correlate with the Satisfaction with Life Scale (r=0.49) and the Emotional Regulation Questionnaire (r=0.49) (Table 4).
Discussion
Statistical analysis of the tool revealed two constructs: autonomous and controlled accountability. The 18-item prototype was hypothesized to contain an additional construct (general accountability) based on the TSRQ, a theoretically derived scale designed to assess the different forms of motivation within the Self-Determination Theory (SDT).17 However, factor analysis suggested the removal of this construct, likely due to general accountability containing aspects of both autonomous and controlled accountability. As expected, autonomous motivation most strongly correlated with autonomous accountability. Introjected and external motivation, forms of extrinsic motivation, most strongly correlated with controlled accountability. Although amotivation suggests neither type of motivation, it weakly correlated with all accountability constructs, suggesting that motivation is not the only driving factor.
The association between patient satisfaction with his/her physician and accountability supports the notion that SDT, a heath behavior theory, can incorporate aspects of accountability into healthcare.2 The correlation between accountability and fear of negative evaluation is consistent with the SDT which suggests that accountability can be considered a spectrum from a paternalistic use of duress to comply with instructions (controlled accountability) to patients’ autonomous internal desire to please a respected health care provider (autonomous accountability).2
In order to further refine autonomous and controlled accountability, we analyzed personal factors including sex, age, level of education, and race. Interestingly, we found no significant association between any of these factors and accountability. This suggests accountability is a novel characteristic independent from demographics.
Although participants were recruited in two different settings, the only significant difference between the paper-based and web-based samples was age. This difference was not surprisingly as MTurk workers tend to be around 30 years old, college-educated, and white.18
Several limitations of the present study should be considered. First, the sample was a convenient sample of respondents who self-selected for participation in the study. Therefore, factor analysis was limited. Second, we only used the BFNE, the TSRQ, Satisfaction with Life Scale, and Emotional Regulation Scale to assess the reliability and validity of the AMT. We cannot know whether other scales, such as the self-efficacy scale, might have yielded different results. Third, the sample of participants from the test-retest administration was small.
Despite these limitations, the AMT has demonstrated reliability and validity. Furthermore, the test-retest analysis demonstrates excellent temporal stability. Accountability has been a missing concept of adherence research. A validated accountability scale would allow for the formation of testable hypotheses and interventions to address patient adherence. Future research should examine the multi-dimensional and complex relationships between patient accountability, adherence, and behaviors when managing chronic disease.
Conclusion
We developed and validated a 12-item tool to quickly, easily, and objectively measure accountability. The tool may prove valuable for assessing the impact of interventions designed to improve adherence by increasing patients’ sense of being held accountable. Future research issues to consider include how accountability can affect short-term adherence, how short-term adherence may affect long-term use, and how accountability might be used over the long term. Future research should aim for larger samples of known chronic disease states and sociodemographic diversity to evaluate the reliability and the generalizability of the AMT.
Acknowledgment
We are indebted to the statistical assistance of the Wake Forest Clinical and Translational Science Institute (WF CTSI), which is supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through grant award number UL1TR001420. We would also like to thank Gregory Bartos, BS and David Arnold, BS for data collection and manuscript preparation.
Disclosure
Dr. Feldman is a speaker for Taro, a consultant and speaker for Galderma, Abbvie, Celgene, Abbott Labs, Lilly, Janssen, Novartis Pharmaceuticals and Leo Pharma Inc., has received grants from Galderma, Janssen, Abbott Labs, Abbvie, Celgene, Taro, Sanofi, Celgene, Novartis Pharmaceuticals, Qurient, Pfizer Inc. and Anacor, a consultant for Advance Medical, Caremark, Gerson Lehrman Group, Guidepoint Global, Kikaku, Lilly, Merck & Co Inc, Mylan, Pfizer Inc, Qurient, Sanofi, Sienna, Sun Pharma, Suncare Research, Valeant, and Xenoport, is the founder, chief technology officer and holds stock in Causa Research, holds stock and is majority owner in Medical Quality Enhancement Corporation, and receives royalties from UpToDate, Informa and Xlibris; he reports no other conflicts of interest in this work. Abigail Cline, Lara Kammrath, EJ Masicampo, Elias Oussedik, Jennifer J Su, and Edward Ip have no conflicts of interest to disclose.
References
1. Irvine J, Baker B, Smith J, et al. Poor adherence to placebo or amiodarone therapy predicts mortality: results from the CAMIAT study. Psychosom Med. 1999;61(4):566–575.
2. Oussedik E, Foy CG, Masicampo EJ, Kammrath LK, Anderson RE, Feldman SR. Accountability: a missing construct in models of adherence behavior and in clinical practice. Patient Prefer Adherence. 2017;11:1285–1294. doi:10.2147/PPA.S135895
3. Lerner JS, Tetlock PE. Accounting for the effects of accountability. Psychol Bull. 1999;125(2):255–275.
4. Yentzer BA, Wood AA, Sagransky MJ, et al. An internet-based survey and improvement of acne treatment outcomes. Arch Dermatol. 2011;147(10):1223–1224. doi:10.1001/archdermatol.2011.277
5. Davis SA, Lin HC, Yu CH, Balkrishnan R, Feldman SR. Underuse of early follow-up visits: a missed opportunity to improve patients’ adherence. J Drugs Dermatol. 2014;13(7):833–836.
6. Laffer MS, Feldman SR. Improving medication adherence through technology: analyzing the managing meds video challenge. Skin Res Technol. 2014;20(1):62–66. doi:10.1111/srt.12084
7. Feldman SR, Camacho FT, Krejci-Manwaring J, Carroll CL, Balkrishnan R. Adherence to topical therapy increases around the time of office visits. J Am Acad Dermatol. 2007;57(1):81–83. doi:10.1016/j.jaad.2007.04.005
8. Hamilton M. Rating depressive patients. J Clin Psychiatry. 1980;41(12 Pt 2):21–24.
9. Bandura A. Guide for constructing self-efficacy scales (revised). Self-effic Beliefs Adolesc. 2006;5(1):307–337.
10. Cutrona CE, Russell D. The provisions of social relationships and adaptation to stress. Adv Pers Relat. 1987;11983(1):37–67.
11. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215.
12. McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Eng J Med. 2003;348(26):2635–2645. doi:10.1056/NEJMsa022615
13. Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. 1985;49(1):71–75. doi:10.1207/s15327752jpa4901_13
14. Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. 2003;85(2):348–362.
15. Buhrmester M, Kwang T, Gosling SD. Amazon’s mechanical Turk: a new source of inexpensive, yet high-quality, data? Perspect Psychol Sci. 2011;6(1):3–5. doi:10.1177/1745691610393980
16. Bland JM, Altman DG. Statistics notes: cronbach’s alpha. BMJ. 1997;314(7080):572. doi:10.1136/bmj.314.7080.572
17. Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ, US: Prentice-Hall, Inc; 1986.
18. Keith MG, Tay L, Harms PD. Systems perspective of Amazon Mechanical Turk for Organizational Research: review and recommendations. Front Psychol. 2017;8:1359. doi:10.3389/fpsyg.2017.01359
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.