Back to Journals » Patient Preference and Adherence » Volume 12
Access and adherence to medications for the primary and secondary prevention of atherosclerotic cardiovascular disease in Singapore: a qualitative study
Authors Koh JJK, Cheng RX ![]() , Yap YC, Haldane V
, Yap YC, Haldane V ![]() , Tan YG
, Tan YG ![]() , Teo KWQ, Srivastava A, Ong PS, Perel P
, Teo KWQ, Srivastava A, Ong PS, Perel P ![]() , Legido-Quigley H
, Legido-Quigley H
Received 4 June 2018
Accepted for publication 7 September 2018
Published 22 November 2018 Volume 2018:12 Pages 2481—2498
DOI https://doi.org/10.2147/PPA.S176256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Joel Jun Kai Koh,1,* Rui Xiang Cheng,2,* Yicheng Yap,2,* Victoria Haldane,1 Yao Guo Tan,2 Krichelle Wei Qi Teo,2 Aastha Srivastava,1 Pei Shi Ong,2 Pablo Perel,3 Helena Legido-Quigley1,3
1Saw Swee Hock School of Public Health, National University of Singapore, Singapore; 2Department of Pharmacy, National University of Singapore, Singapore; 3London School of Hygiene and Tropical Medicine, London, UK
*These authors contributed equally to this work
Background: Atherosclerotic cardiovascular disease (ASCVD) is a growing public health threat globally, and many individuals remain undiagnosed, untreated, and their condition remains uncontrolled. The key to effective ASCVD management is adherence to pharmacotherapy, and non-adherence has been associated with an increased risk of cardiovascular events and complications such as stroke, further impacting a patient’s ability to be adherent. Our qualitative study aimed to explore factors influencing medication adherence in the primary and secondary prevention of ASCVD in Singapore. We propose a synthesized framework, which expands on current understandings of the factors of medication adherence, as a frame of analysis in this study.
Methods: We conducted in-depth, semi-structured interviews with 20 patients over the age of 40 with ASCVD and/or its risk factors in Singapore. QSR Nvivo 11 was used to conduct thematic analysis using an inductive approach.
Results: Using a synthesized framework, we reported that complex medication regimens, the lack of support received during regimen changes, and the perceived seriousness of a condition could impact a patient’s medication adherence. Key findings suggest that the relationship between health care professionals and patients impacted patient acceptability of the medication regimen and consequently medication adherence. Different patient beliefs regarding diagnosis, medication, and adherence had some bearing on the ability to perceive the need to adhere to their medication. Patients also reported that they could afford medication, sometimes with the help of family members. Patients also largely reported not needing help managing their medication, considering it an individual responsibility.
Conclusion: We identified key factors which future interventions looking to improve medication adherence ought to consider. These include changing patient perceptions of health systems, diagnosis, medication, and adherence; patient-centeredness in developing interventions that facilitate adherence through building self-efficacy and stronger support networks via patient empowerment and engagement; decreasing patient co-payments on medication; and cultivating a trusting patient–provider relationship.
Keywords: atherosclerotic cardiovascular disease, medication adherence, access, qualitative research, Singapore
Introduction
Cardiovascular disease (CVD), including atherosclerotic cardiovascular disease (ASCVD) such as ischemic heart disease, stroke, and peripheral vascular disease, are leading causes of mortality worldwide.1 The recent Global Burden of Disease study estimates 422.7 million prevalent cases of CVD, with CVD being accountable for one third of all deaths.2 The World Heart Federation estimates there will be over 23 million deaths from CVD by 2030 and that many CVD cases are preventable by addressing behavioral risk factors.3 Further, evidence has shown that Asian countries face higher age-adjusted mortality from CVD.4 In 2016, 39.5% of total deaths in Singapore were due to CVD.5
ASCVD risk factors such as hyperlipidemia, hypertension, and/or prior ASCVD contribute to future ASCVD risk, which necessitates primary and secondary cardiovascular prevention.6–8 A key component of secondary CVD prevention is the use of pharmacotherapy, which has been shown to mitigate the risk of developing ASCVD and associated complications.7,9 Medication adherence is crucial to the effectiveness of pharmacotherapy for CVD;10–12 however, evidence shows that patient non-adherence to medications for chronic conditions such as ASCVD is common.12,13 Such non-adherence to medication has been associated with the occurrence of cardiovascular events among patients with CVD,14 as well as increasing the risk of complications such as stroke, which could further impact a patient’s ability to be adherent.10,15
Several studies have illustrated issues associated with medication non-adherence, such as poor patient outcomes and the burden it places on the health care system.16,17 Several factors have been found to underpin issues associated with medication non-adherence such as, the type of medication prescribed,18,19 low socioeconomic status,14 treatment complexity,20 marital status,19 treatment side effects,21 and health system factors.15,22 Given these challenges, there has been a call for interventions to support medication adherence that consider the patient’s role within the context of the health system.16 As such, there is a need for innovative ways to better enable patients to take their medications, particularly in health systems like Singapore, where coverage and health system usage are high and the effectiveness of a treatment is largely dependent on medication adherence.14
Mobile health (mHealth) interventions for CVD prevention have shown promising results in promoting medication adherence for stroke,23 hypertension,24 and heart failure.25,26
This paper focuses on Singapore, where, given high rates of mobile phone use,27,28 mHealth interventions have the potential to be successful in promoting medication adherence. The current study is the development phase of a proposed mHealth intervention to support patient adherence to ASCVD and hypertension medication among a diverse, elderly Singaporean population. Integral to the development of this intervention is the need for an understanding of the various factors contributing to the experience of medication (non-)adherence among patients with ASCVD. Thus, our qualitative study aimed to explore factors influencing medication adherence in the primary and secondary prevention of ASCVD in Singapore by delving into the experience of patients.
Conceptual framework
In this paper, our approach to conceptualizing medication adherence has been informed by the WHO’s five dimensions of adherence, as well as Levesque’s conceptualization of patient-centered access.6,29
Based on a review of the literature, the dimensions describe the various factors impacting on adherence, ranging from the personal to system level factors. The WHO dimensions do not operate as separate factors, but rather interplay with each other to impact patient adherence to medication. However, while these dimensions are useful, a more detailed description of each concept within a dimension is needed to provide a comprehensive understanding of the factors influencing patients’ adherence to treatment. For example, health system factors such as the lack of health care financing need to consider socioeconomic factors such as the patient’s ability to pay for health care in light of other expenses in order to truly understand its impact on a patient’s adherence. Thus, we found that an important element not sufficiently highlighted in the current WHO framework is access, which has been shown to impact a patient’s adherence to treatment.30 Access is particularly important as it helps us see how the dimensions of health system, patient, and socioeconomic factors truly interplay with each other to impact a patient’s adherence to treatment.
Levesque et al define access as “the opportunity to reach and obtain appropriate health care services in situations of perceived need for care”.29 The authors conceive access as both the accessibility of services to realize such an opportunity, as well as the ability of patients to interact with such accessibility.
Accessibility is conceptualized in five dimensions, approachability, acceptability, availability, affordability, and appropriateness. Correspondingly, there are five abilities that enable the patient to engage with accessibility including ability to perceive, seek, reach, pay, and engage, respectively.
To better understand the many factors acting upon patients, we have integrated the two frameworks (WHO framework of adherence and Levesque’s framework for health care access) to form the conceptual basis of this paper. Integrating these frameworks allows for exploration of nuance in the dimensions of adherence conceived by the WHO, and greater consideration of the role of access in patient adherence. Although Levesque et al conceived the framework in the context of health system access, in this paper, we used their framework more narrowly to explore medication access and its impact on medication adherence. While traditionally medication access refers to the process of physically obtaining medication,31,32 we used Levesque et al’s understanding of health system access to frame medication access as the interaction of accessibility and ability (Figure 1).
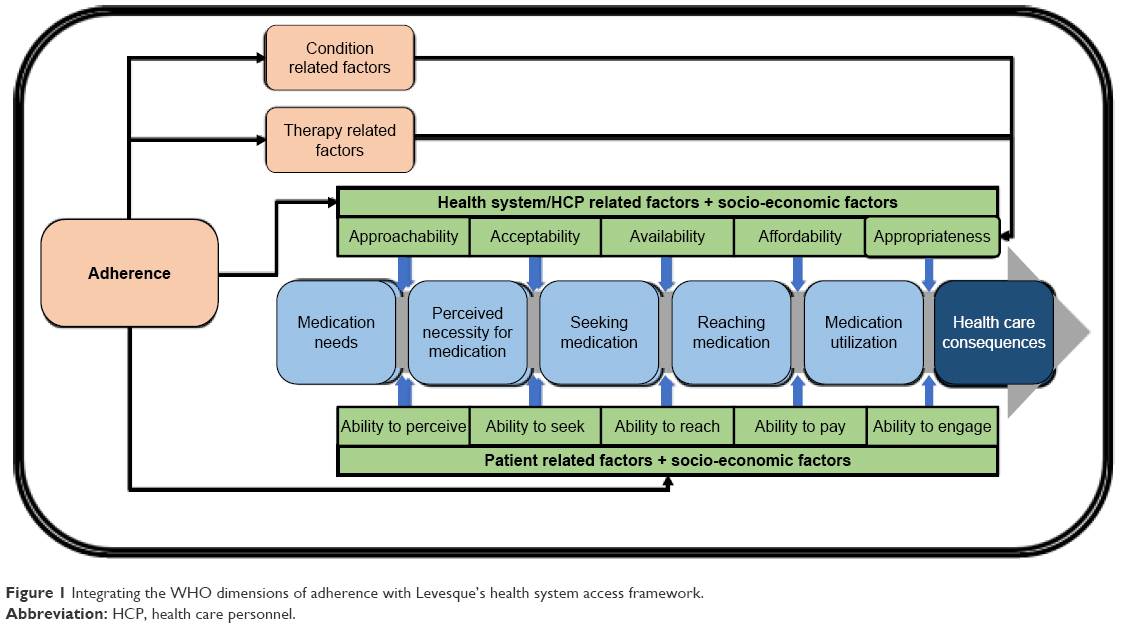 | Figure 1 Integrating the WHO dimensions of adherence with Levesque’s health system access framework. |
This synthesized framework was conceptualized with a mix of inductive approaches from thematic analysis of the data and deductive approaches based on our aim to explore factors which have bearing on access and adherence. Such a framework is important to understand the interface of health system, social, economic, and patient related factors, as well as to foster a deeper understanding of the complex relationship between health system and patient in enabling medication adherence. Such an understanding not only allows for greater granularity in exploring factors related to medication adherence but also accounts for patients’ perspectives, which has been lacking in the conception of previous adherence interventions and models of understanding health behaviour.14,16 For example, the health belief model which has traditionally been a cornerstone to help health systems predict why people take action, to screen, prevent, and manage their illnesses, has tended to focus on patient beliefs as the key to encouraging better self management of illnesses.33 However such a view overlooks two key points. Firstly, it overlooks how structures such as social financing, health financing, or socioeconomic factors might impact how beliefs are conceived. Secondly, it makes an implicit assumption that health beliefs manifest into practice, which might not be the case and points to the clear need for an understanding of access to develop a more nuanced approach. Insights derived from this framework can inform the development of comprehensive adherence interventions, such as the proposed mHealth intervention.
Methods
Sampling
The study took place in Singapore, and we used purposive sampling from an existing patient list to recruit those aged 40 years and above with established ASCVD, or at least one risk factor for ASCVD (Box 1 includes complete inclusion and exclusion criteria).
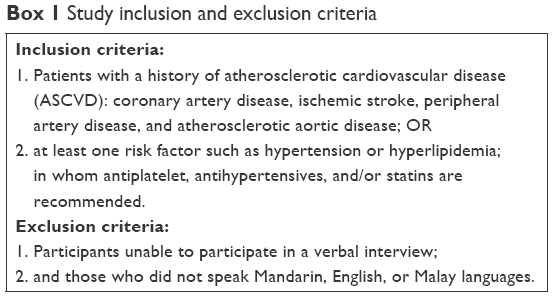 | Box 1 Study inclusion and exclusion criteria |
In-depth interviews
Trained staff and students from the National University of Singapore conducted semi-structured in-depth interviews in the participant’s preferred language (by staff fluent in that language). Interviewer training included description of research protocol, qualitative methods, and research ethics in practice.
The interview guide was developed as part of the larger txt2heart collaboration (an international collaboration evaluating the effectiveness of mHealth for secondary prevention), which we then adapted to the Singapore context and covered topics including patients’ sociodemographic characteristics, health care access, medication adherence, mobile phone technology usage (ownership, access, and utilization), and interest in mHealth (Table 1).
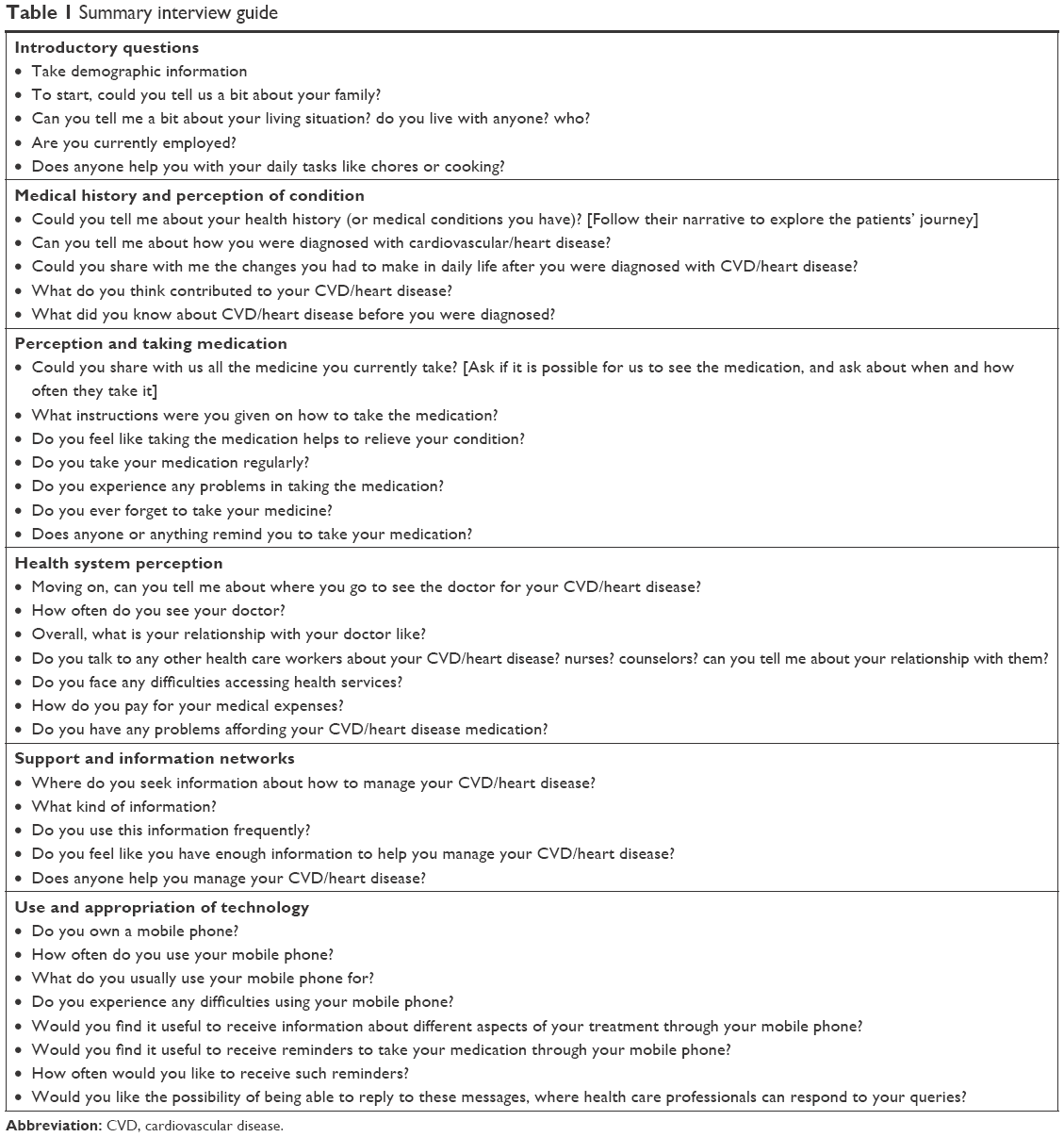 | Table 1 Summary interview guide |
Analysis
This study was grounded within interpretative approaches, in which interviews are believed to provide access to accounts of how respondents perceive, understand, and talk about the world. Two research team members coded interviews using QSR Nvivo 11 Software, applying inductive approaches, thematic analysis, and techniques from the constant comparative method, where line-by-line analysis of early interviews is used on subsequent interviews to test preliminary assumptions.34 Interviews were recorded and transcribed in full. Reviewers agreed on identified codes and themes. To maintain confidentiality, all names reported are pseudonyms and identifying data have been excluded.
Participants
Twenty participants agreed to participate in the in-depth interviews. Out of the 20 participants interviewed, 19 agreed to audio recording, and one participant declined. For the latter, detailed field notes and an extensive memo were taken for inclusion in data analysis.
Ethical approval
Ethical approval for the study was obtained from the National University of Singapore Institutional Review Board. Written informed consent for participation and recording was obtained before the interview started using a participant information sheet and consent form. Participants could refuse to answer any of the questions and/or discontinue their participation in the research at any time.
Results
Participant characteristics
We conducted 20 in-depth interviews with participants who met inclusion criteria, and detailed characteristics are presented in Table 2. Participants were largely of Chinese ethnicity (n=15) with fewer participants from Indian (n=4) and Malay (n=1) ethnic groups. Participants were mostly male (n=12), with eight female participants. The average age of participants was 72.5 years old. The majority of participants (n=19) reported a hypertension diagnosis, followed by hyperlipidemia (n=16), myocardial infarction/acute coronary syndrome (n=8), and stroke/transient ischemic attack (n=5).
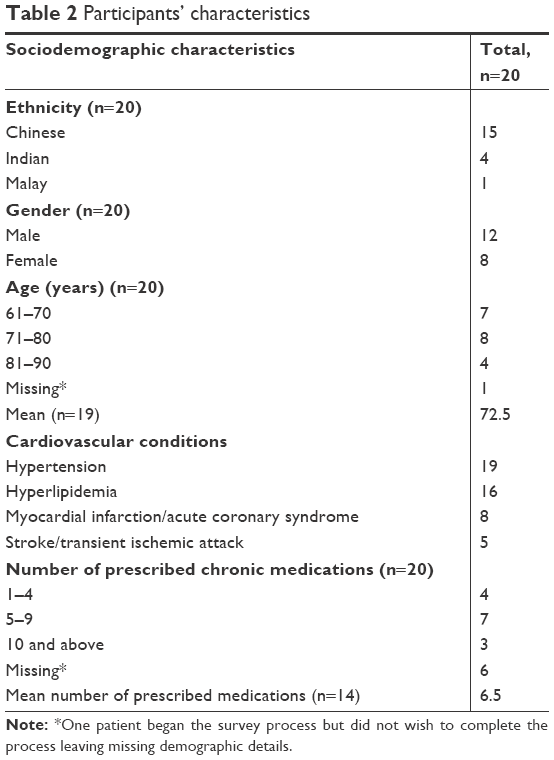 | Table 2 Participants’ characteristics |
Findings: conceptual framework
We presented our findings under themes presented in the conceptual framework (Figure 1). First, we examined condition and therapy related factors which may impact a patient’s adherence. Then we considered the impact of health system, patient, and socioeconomic factors on medication adherence through the lens of medication access using our adapted framework. These were divided into five key themes from Levesque et al’s (2013) key dimensions of access. First, “approachability” and “ability to perceive” demonstrate how patient beliefs about diagnosis, medication, and adherence impact their ability to perceive the need to adhere to their medication. Second, “acceptability” and “ability to seek” discuss how a patient’s perception of health care facilities as well as their relationship with their health care provider might influence the acceptability of medication therapy. Third, “availability” and “ability to reach” report on the different physical difficulties patients have in reaching their health care facility, compounded by factors such as the weather, transport, and health care costs. Fourth, “affordability” and “ability to pay” describes the existing health financing structures available for patients and their difficulties in financing their health care expenses in spite of these structures. Last, “appropriateness” and “ability to engage” discuss how patients adapt and engage with medication therapy, and also how they perceive it to be an individual responsibility. These findings are summarized in Table 3.
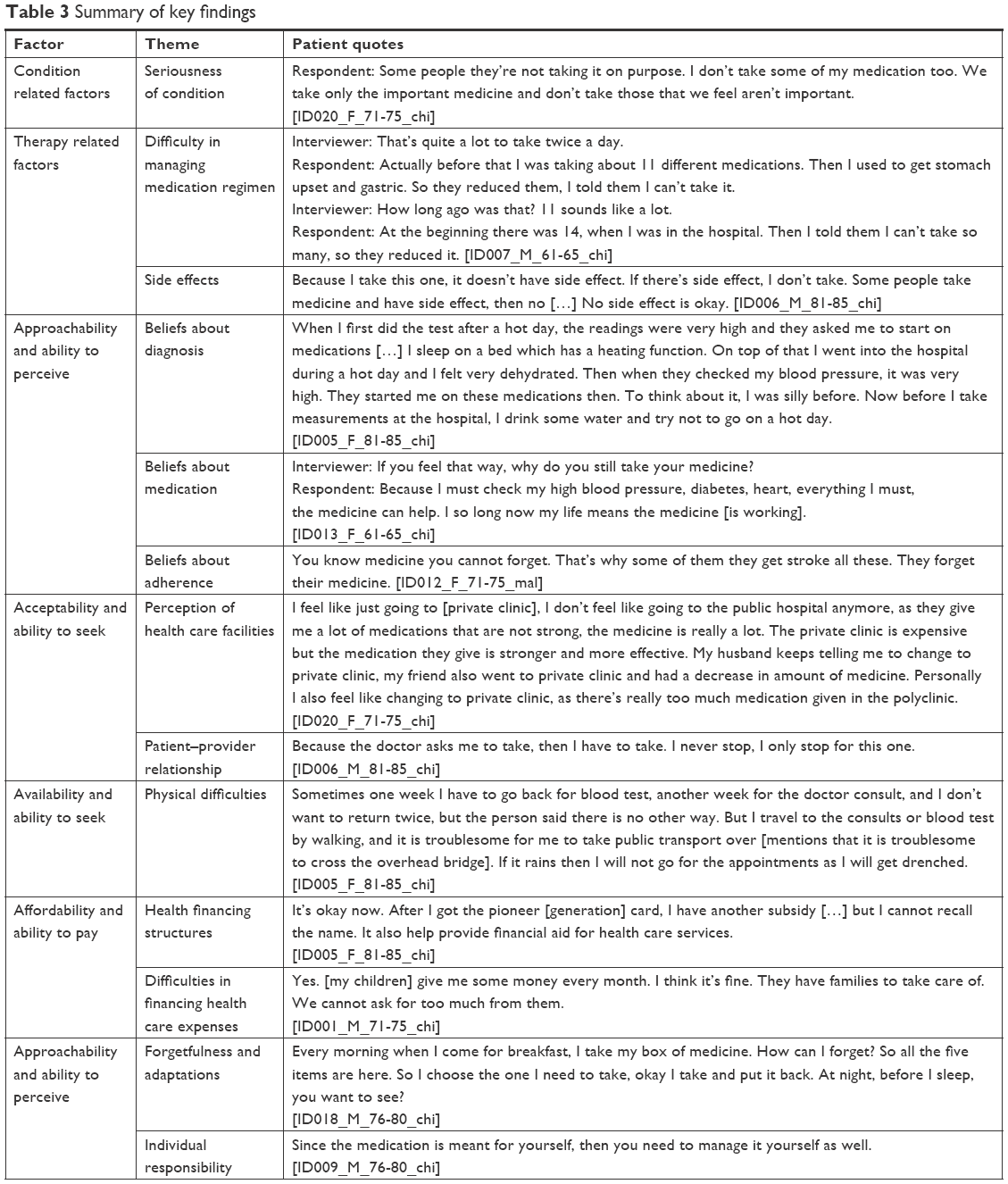 | Table 3 Summary of key findings |
Condition related factors
Condition related factors refer to the demands faced by the patient as a result of their condition and its symptoms which might impact medication adherence. In this context, the perception of the seriousness of a condition, in relation to other conditions, has an influence on a patient’s adherence to medication therapy.
Seriousness of condition
Some patients expressed that they choose which medication to take based on how serious they perceive their condition to be. When asked about the importance of taking medication, Sue shared that,
Respondent: Some people they’re not taking it on purpose. I don’t take some of my medication too. We take only the important medicine and don’t take those that we feel aren’t important. [ID020_F_71-75_chi]
Some patients reported prioritizing certain illnesses over others. In our study, patients’ perceived high cholesterol to be less serious compared to other conditions. Some patients thus chose not to take cholesterol medication, as Patsy explained,
Interviewer: So you believe in taking medications for more serious illnesses? But when it comes to minor illnesses […]?
Respondent: Like me, mine are not that serious, so sometimes I can don’t take them. Especially the cholesterol medication. Although the doctor says it’s okay to take them. What if something happens? […] So for serious illnesses, take your medication. But for minor ones, as long as you follow-up, it’s okay. [ID004_F_66-70_chi]
Thus, patient perceptions of the seriousness of ASCVD and their risk factors in relation to their other illnesses had some impact on their perceived need to adhere to the medication.
Therapy related factors
Therapy related factors describe the difficulties patients face in managing their complex medication regimens and different aspects of treatment (ie, treatment changes and side effects). In this context, it refers to the difficulty a patient faces in managing their medication regimen and the experienced side effects from prescribed medication.
Difficulty in managing medication regimen
Previous literature has demonstrated that patients with ASCVD tend to have multiple co-morbidities which require a complex medication regimen to manage effectively.9,35 For patients, this could result in polypharmacy which may impact medication adherence.20 For some patients like Heng, having to manage multiple different medications impacted their adherence:
Interviewer: That’s quite a lot to take twice a day.
Respondent: Actually before that I was taking about 11 different medications. Then I used to get stomach upset and gastric. So they reduced them, I told them I can’t take it.
Interviewer: How long ago was that? 11 sounds like a lot.
Respondent: At the beginning there was 14, when I was in the hospital. Then I told them I can’t take so many, so they reduced it. [ID007_M_61-65_chi]
However, some patients reported no problems managing a complex medication regimen, for example, Seng who despite having polypharmacy, only needed to take medication once a day:
Interviewer: Do you feel confused about so many types of medicine?
Respondent: It’s just once a day! It doesn’t really take up a lot of time. It can be done in about 5 minutes, not more than 10 minutes. I don’t ask for anything else. [ID001_M_71-75_chi]
For some patients, polypharmacy was not the only difficulty faced when having a complex medication regimen. Sue expressed that she struggled with changes made to her medication regimen, and this was compounded by the lack of support given by health care professionals to take medication:
Interviewer: Did they explain how to take the medications?
Respondent: Yes, this one eat half hour within meals, this one take only when eaten food, this one for morning. This medicine should be morning medicine, but I don’t take it anymore.
Interviewer: Why?
Respondent: This medicine at the start when he told me to stop eating it, then I forgot how to take it when it resumed, then they didn’t explain to me how to take it again. [ID020_F_71-75_chi]
Experience of side effects from prescribed medication
Several patients reported that their side effects, as a result of taking medication, impacted their motivation to adhere to their medications. For example, Tim explained,
Because I take this one, it doesn’t have side effect. If there’s side effect, I don’t take. Some people take medicine and have side effect, then no […] No side effect is okay. [ID006_M_81-85_chi]
For some patients, their willingness to bear with the side effects of a medication is dependent on their perception of the severity of their illness. Devi reported,
Interviewer: So you mentioned that you are not taking the cholesterol medication?
Respondent: Yeah. I am not taking it.
Interviewer: Why is that the case?
Respondent: As long as my readings are fine.
Interviewer: As long as the readings are okay.
Respondent: You know why? Sometimes it gives you aches in your bones. It starts to hurt. [ID011_F_61-65_ind]
Access related factors
Below we reported the results for the five access dimensions with their corresponding abilities from the perspective of the patient (Figure 1). We grouped the different factors of accessibility with their corresponding ability as seen in the framework posited earlier together, as the same theme, as we believe discussing them separately would posit them as separate points when they actually work in tandem to impact patient adherence.
Approachability and ability to perceive
Approachability and the ability to perceive refer to the ability of patients to identify the importance of adhering to their medication regimen, and having the necessary information to do so. In this context, we described how patient beliefs about diagnosis, medication, and adherence impact adherence.
Beliefs about diagnosis
Some patients had doubts that they even had conditions they were diagnosed with and given medication for.
When I first did the test after a hot day, the readings were very high and they asked me to start on medications […] I sleep on a bed which has a heating function. On top of that I went into the hospital during a hot day and I felt very dehydrated. Then when they checked my blood pressure, it was very high. They started me on these medications then. To think about it, I was silly before. Now before I take measurements at the hospital, I drink some water and try not to go on a hot day. [ID005_F_81-85_chi]
Mei believed that her high blood pressure reading was caused by the conditions in which their test was taken and was not entirely convinced that she had hypertension.
When asked if he had high blood pressure, Tim responded,
No. No diabetes, no high blood pressure. No more high blood pressure. [ID006_M_81-85_chi]
This was despite the fact that Tim had been prescribed hypertension medication.
Beliefs about medication
Some patients interviewed believed that there was value in adhering to their medication regimen and that it was the reason why they were still alive.
Interviewer: Okay that’s good. So actually do you think the medicine helps you with the condition?
Respondent: Of course it helps […] if not I may not survive till now. [ID003_F_NA_chi]
Despite this, patients such as Patsy would rather manage their condition through diet management due to the perceived side effects of medication.
Interviewer: Why don’t you take the cholesterol medication?
Respondent: Because both my niece and my elder sister are nurses. My sister told me that if I take a lot of these cholesterol medication, it will affect my kidneys. Because I have cancer, so I want to avoid taking these. I avoid oily and fatty foods. I try to control my cholesterol that way. [ID004_F_66-70_chi]
Some patients, like Tim, do not see the need to take several types of medication for one illness. In trying to justify why he had stopped taking enalapril for his blood pressure, Tim asserted that:
[this is] quite the same […] this one is for the heart, high blood pressure […] this one is quite the same, high blood pressure […]. [ID006_M_81-85_chi]
For Tim, the perception that enalapril is the “same” as other medication for his high blood pressure impacted his adherence to his medication regimen.
Beliefs about adherence
Patients interviewed had several beliefs about adherence which impacted how they perceived the need to be adherent. Firstly, some patients did not feel the need to be constantly adherent to their medication regimen, and this was dependent on how they feel and their readings. Devi perceived that there is no need to adhere to cholesterol medication if a patient’s cholesterol is only borderline and took a self-management approach to medication adherence,
Interviewer: So the doctor has been giving you the cholesterol medication but you have not been taking it? Then […] diabetes?
Respondent: That one is only a few months. They said, “oh your case is borderline” – I said, “borderline”? Then why are you giving me […]? After that, they said, “Normal, normal, but this medicine still carry on”.
Interviewer: Did you tell the doctor that you didn’t take or didn’t want to take the cholesterol medicine?
Respondent: No, as long as my reading is normal I’ll keep quiet. If it goes up I’ll tell them. If they try to increase my dosage then I will tell them I haven’t been taking it. [ID011_F_61-65_ind]
She would only disclose she had not been adherent when her reading goes beyond borderline. Dan echoes this and sometimes does not feel the need to take his cholesterol medication when he feels alright,
Okay, to be honest, blood thinner, I almost take every day. So sometimes the idea just come “Hey, I think I am okay what, so don’t need to take everyday”. You know what I mean? But mostly, blood thinner I try to take regularly. Cholesterol, sometimes I miss. [ID016_M_61-65_chi]
Secondly, several patients explained that they were adherent to their medication because they are afraid of the complications that will result from non-adherence. Ben explained that he knew being non-adherent to his medicine could lead to a stroke and was afraid of it:
Interviewer: Do you think it’s important to control your blood pressure?
Respondent: Yes, otherwise things happen.
Interviewer: What kind of things?
Respondent: Things like stroke. [ID019_M_81-85_chi]
Kim shared that she was motivated to adhere to medication as she is worried about death which could potentially result from not managing her condition:
Because I’m scared to die, it motivates me to eat my medication, without even any reminder. [ID008_F_71-75_chi]
Third, some patients felt that being non-adherent would make the whole process of seeking care and seeing a physician pointless.
I trust [doctors] so I won’t dare to not take the medication. If you don’t take the medication, then you might as well don’t see the doctor. It’ll be a waste of everyone’s time. [ID009_M_76-80_chi]
Why you want to see doctor if you don’t take the medicine? Right? If you want to see the doctor that means you want to get well and to get well, you have to eat the medicine, otherwise, how can you get well? [ID018_M_76-80_chi]
Both Steve and Teo asserted that non-adherence will not only render appointments with the physician pointless but also prevent patients from managing their condition.
Acceptability and ability to seek
Acceptability and ability to seek refer to the sociocultural factors which enable patients to have the capacity to seek and accept different aspects of the medication therapy impacting their adherence. Important facets of acceptability and the ability to seek include individual health system preferences, as well as the patient–provider relationship.
Perception of health care facilities
Some patients mentioned that the acceptability of medication therapy was impacted by perceptions of the services provided by different sectors of the health system, namely, private or public health care. For example, Sue expressed that:
I feel like just going to [private clinic], I don’t feel like going to the public hospital anymore, as they give me a lot of medication that are not strong, the medicine is really a lot. The private clinic is expensive but the medication they give is stronger and more effective. My husband keep telling me to change to private clinic, my friend also went to private clinic and had a decrease in amount of medicine. Personally I also feel like changing to private clinic, as there’s really too much medication given in the polyclinic. [ID020_F_71-75_chi]
For some patients these perceptions stem from previous experience with providers from different sectors (ie, providers in public and private health care facilities). Kim explained that,
At the polyclinic they don’t care so much how serious things are. They just ask a few questions and ask me to collect my medicine. It’s better at the hospital. Last time, my daughter likes to bring me to private hospitals. They’re very good, but too expensive, [private hospital]. Their medications are very good but very expensive. The medication is good, no problems even after my surgery. [ID008_F_71-75_chi]
Patient–provider relationship
Key to the acceptability of a medication regimen is the engagement between health care professionals and patients, and the ability of health care professionals to deliver care acceptable to the patient. Many patients described encountering multiple non-physician health care professionals during their engagement with the health system, where different tasks in the care process are shared among health care professionals such as pharmacists, nurses, and care coordinators. Many patients described their encounters with these health care professionals positively with regard to helping them adhere to their medication. For example, when asked about the help she receives in taking medication Xue said,
Yeah, yeah. My pharmacy, they tell me. The pharmacy, they help me a lot. Sometimes, I don’t know the medicine name. I don’t know until now, I don’t know the medicine name, but only I know morning, up. Night, up. “Okay, morning I must take. Night, also, I must take.” Same medicine. So I don’t know the name but the pharmacists say, “This one, half ah madam,” and then they tell me of what medicine. So sometimes I see the words. This one is half tablet, one tablet, I can see the words. [ID013_F_61-65_chi]
Some patients, such as Heng, have a care coordinator who helps them to adhere to their medication and manage their condition through medication reconciliation and counseling. Heng’s experience with his care coordinator has been very positive. When asked about whether the care coordinator has helped him, Heng responded,
Yes, it helps because it’s more personal care than a general [one] […]. [ID007_M_61-65_chi]
Beyond the personalized care that a care coordinator provides, Heng believes that some care coordinators are more knowledgeable than the doctors, and should be trusted as they have been at the clinic longer than the doctors.
Some of them have been there 5–6 years, but the doctors are maybe there for 1–2 years. Sometimes when the doctors say something, they will correct them, like if it’s not allowed or like that. [ID007_M_61-65_chi]
While trust in non-physician health care professionals is important in ensuring the acceptability of health services to ensure patients adhere to medication, the relationship between a patient and physician is also crucial in enabling medication adherence, and consequently condition management. In response to a question about whether Mei Ling takes any form of alternative medicine, she responded that:
Very little. Because my liver is not good, I’m afraid of mixing them. The doctor told me before as well, to stick to my medication, and he knows my condition well. My doctor talks to me like a friend. [ID005_F_81-85_chi]
For Mei, the relationship she has with her physician is described to be one of friendship which in turn encouraged her adherence to her medication regime. Echoing this, several patients interviewed talked about the trust they had in their doctors and the importance of a relationship with them. However, not all patients had a sole primary physician. Samuel demonstrated a desire to see the same doctor, and the preference for a doctor to “know” him, but health system changes have made this difficult.
In the polyclinic every appointment is with a different doctor. Sometimes I try to ask to see the same doctor, because the doctor knows me, but the last two years it has been a different doctor. There was a stage about 5 or 6 years ago when I used to see the same doctor, I tried to make appointments to see the same one. In order to do that, I don’t make an appointment early […]. I go and then ask on the spot. Because actually I would rather see the same doctor every time. At least he or she can recognize me. If I am booking by phone or through the App, it’s an automated system. You can get Tom, Dick or Harry. Sometimes they will give a different result or a different diagnosis or whatever. This is what I think. [ID015_M_61-65_chi]
Beyond fostering a friendly and trusting relationship, doctors are in the position to make certain types of treatment acceptable for the patient. For example Teo explained,
That one time they said I have a stroke, I have to accept the fact, I can’t run away from it and so, they begin to prescribe medicine for me. Now the interesting thing is that one of the senior doctor was talking to me, invite me to join the group to test a new drug for diluting the blood circulation. I was quite scared. Because of my reaction, the doctor told me, “Don’t worry. We are not doing any harm to you. What we are doing is actually for your own good. But we think it is good.” The way he said it was so confident so okay, I accept it. [ID018_M_76-80_chi]
For some patients, such as Siew and Patsy, this trust in physicians might not stem from “friendship” but should rather be seen as a given due to the power dynamic between doctors and patients. For example, Siew explained that:
Interviewer: Why do you follow the instruction of doctors?
Respondent: Because I know my own problem well […] so if I see a doctor and don’t trust him, then why should I go and see? [ID003_F_NA_chi]
Interviewer: Since you have said you shared a lot of things with your doctor, do you have a good relationship with your doctor?
Respondent: Yes it has to be. I will tell the doctor everything.
Interviewer: So you trust your doctor?
Respondent: Yes, I have to. Or else? You should always follow-up with your doctor after taking your medications. [ID004_F_66-70_chi]
This sense of unquestioned trust in physicians also manifested in how patients perceived the physician’s instructions.
I can’t remember what they’re [medication] for. The doctor give me, so I eat. [ID002_M_81-85_chi]
Seng even expressed that if a doctor says something then there is “no choice” but to accept medication therapy.
They said I have to take medicine for […] what is that called […] it’s high blood pressure. The doctor told me to take medicine. No choice, I started taking it and took it for a few decades already, since I was 40-something. [ID001_M_71-75_chi]
Despite this, some patients such as Patsy still choose not to adhere to medication given to her, and would rather not tell the doctor about it for fear of being scolded.
Interviewer: How about your cholesterol?
Respondent: It varies. Sometimes it’s high, sometimes it’s low. Because sometimes I don’t take the medication. You see, this cholesterol medication was given to me in March, and I still have so much left over. If I show the doctor, he/she is going to scold me. So I won’t tell the doctor. [ID004_F_66-70_chi]
Availability and ability to reach
Availability and ability to reach relates to the factors which give people the capability to reach the medication they need when they need it. These include physical access, mobility, and understanding of the health services available. Most patients were able to physically access health services; however, some pointed out that the journey to health care facilities could be difficult due to their age and other physical difficulties.
Interviewer: Do you walk there?
Respondent: No, I take transportation [bus]. It’s too far to walk. I cannot […] my legs are not well. [ID001_M_71-75_chi]
Mei noted that it is sometimes difficult for her to get to health care facilities for medical appointments due to inclement weather, and this at times discourages her from wanting to go for her appointment to see the doctor.
Sometimes one week I have to go back for blood test, another week for the doctor consult, and I don’t want to return twice, but the person said there is no other way. But I travel to the consults or blood test by walking, and it is troublesome for me to take public transport over [mentions that it is troublesome to cross the overhead bridge]. If it rains then I will not go for the appointments as I will get drenched. [ID005_F_81-85_chi]
Kim pointed out that her ability to pay for health services, and desire to not burden her children, had an impact on her ability to seek certain types of medication,
I was seeing private hospital, but my friends say that I shouldn’t burden my daughter with the fees. Initially I went to a polyclinic and they didn’t have the medicine, as it’s an expensive medicine. Then my friends brought me to Clementi polyclinic, which is a polyclinic for richer people, and they really have the medicine there. But it’s still expensive, not cheaper by a lot. [ID008_F_71-75_chi]
Affordability and ability to pay
Affordability and ability to pay refer to the structures in place which impact an individual’s economic capacity to engage with health services and obtain medication. They ensure a patient is financially able to adhere to a medication regimen prescribed, without having grave impact on daily necessities. In this context, we described the health financing structures which make medication affordable for patients, and their ability to pay for health care expenses in light of these structures.
Health financing structures
Most patients interviewed found medication prescribed for ASCVD and their risk factors to be affordable and had no issues obtaining medication. This is largely due to the availability of different schemes and subsidies initiated by the government. When asked if she felt medication was affordable Mei responded,
It’s okay now. After I got the pioneer [generation] card, I have another subsidy […] but I cannot recall the name. It also help provide financial aid for health care services. [ID005_F_81-85_chi]
Several patients interviewed had a Pioneer Generation (PG) or Community Health Assistance Scheme (CHAS), like Mei, and stated that it had helped them greatly in making their health care and medication expenditure affordable.
Difficulties in financing health care expenses
Although patients generally found that they could afford their medications, some patients shared that the subsidies from financing structures were necessary for them to pay for any of their medical expenses at all. Li said that without health care and social financing they are unable to pay for any of their health care expenses.
Interviewer: Without this [Comcare] card, how much would the expenses be?
Respondent: We wouldn’t be able to afford [health care expenses] at all. [ID014_M_71-75_chi]
Patients, such as Siva, who were not eligible for Comcare and had to co-pay for their medication also described difficulties paying out of pocket despite subsidies available.
Interviewer: Do you have Medisave for these?
Respondent: I have problems with Medisave now. They give me something like $300 every three months. The other time I went for something and now it’s all gone. So I must wait till January for them to top-up $300.
Interviewer: So you have to pay out of pocket now?
Respondent: Yes. I asked my son to help […] Subsidize is have. [ID010_M_71-75_ind]
Siva is still required to pay out of pocket for medication, and has to count on his son to help him with the expenses. Several patients mentioned that their family members helped them to manage the financial burdens of obtaining medication.
Yes. [My children] give me some money every month. I think it’s fine. They have families to take care of. We cannot ask for too much from them. [ID001_M_71-75_chi]
As with Seng, there was a sense among patients interviewed that they did not want to be an economic burden on their family members and be prioritized over other family interests.
Appropriateness and ability to engage
Appropriateness and ability to engage relate to the capacity and willingness of patients to participate in their medication regimen to meet their treatment needs. In this context, it refers to the adaptations patients make to their daily lives to mitigate forgetting their medication, and their assertion that there is an individual responsibility to engage with their medication regimen.
Forgetfulness and adaptations
For some patients, a key reason for lack of engagement with their medication plan is forgetfulness. Patients had several reasons for forgetting their medication, for example Peter reported forgetting medication after being distracted by housework.
Interviewer: Why do you forget?
Respondent: Housework, etc. Sometimes the time for medication has passed. I forget about once or twice a week. [ID002_M_81-85_chi]
Patsy forgets when she travels to her daughter’s house on the weekends to help with child care,
I tend to forget my medications in the morning on weekends. I take care of my grandchildren, I go to Woodlands where my daughter stays, and so I forget. [ID004_F_66-70_chi]
Sue claimed that she does not forget and knowingly chooses not to adhere to her medication as she finds taking it to be inconvenient.
Interviewer: Do you forget to take your medication?
Respondent: No. But if I go out, I won’t bring and eat it. It’s very troublesome to take it when I’m on the bus or MRT [tube system in Singapore]. I’ll just miss taking it. For instance, I went to Ipoh Malaysia the other day, I brought my medicine but I didn’t take it for two days, as it’s too troublesome. As we sometimes take car late in the night so it’s troublesome taking medicine, also sometimes simply forget after eating meals. [ID020_F_71-75_chi]
For patients that forget to take their medication, some reported that health care professionals are aware and do provide advice on how to re-engage with their medication regimen. For example, Peter consults his doctor about what to do when he misses a dose.
Interviewer: Have you asked the doctor if it’s okay to take the medication later?
Respondent: The doctor said it’s okay to miss a dose, and just continue the next day. [ID002_M_81-85_chi]
The doctor recommended Pasty use a pillbox to help her remember to take her medication, and it worked for her.
Respondent: The doctor recommended me to put the medicine into a pillbox as I forget to take my medication often. Putting the medicine in a pillbox simply serves as a reminder that I forget to eat.
Interviewer: How long have you used this pillbox?
Respondent: One year. It helps with my memory, so I won’t keep forgetting to take my medications. And since the medication is already packed, so I won’t forget to eat one or two medication. [ID004_F_66-70_chi]
The use of a pillbox was effective in helping several patients such as Devi remember to take their medication and preventing overdose.
Interviewer: Do you feel [the pillbox] helps?
Respondent: Yes. Sometimes you forget! “Did I take the medication or not?” and you look into it. If you look at it and it has disappeared that means you have already taken it. Also, if I am not sure then I totally avoid it because I don’t want to have an overdose. [ID011_F_61-65_ind]
Several patients were able to actively engage with their medication regimen, adapting their daily lives and creating habitual processes to ensure they adhere to medication.
I usually put the pills down here [table] during the meal, and put them up there after taking the pills. [ID001_M_71-75_chi]
Yes. I place it on the table so that I know I need to take it tomorrow morning. Once I’ve taken it, I place it back in the cupboard. [ID002_M_81-85_chi]
I place it here. In the morning, I go for my exercise. When I return home after breakfast, I will take the medications first before doing anything else. It has become a habit so I won’t forget. [ID009_M_76-80_chi]
Some patients are more innovative, Xue repurposed a toolbox to be used as a pillbox.
No, I go and shop the […] Jurong West got one shop. Then, I go see this kind of [tool] box. My friends tell me it can cut, put with the needle and the thread then I said, “Hey, can put the medicine in also what”. [ID013_F_61-65_chi]
Li felt that pillboxes did not work for him as he always lost them, he decided to pack his medication into little plastic packets so he could just open one and take all the necessary medication for the day. When asked about how he came up with this idea, Li responded that,
In the past, we used to use the pillbox. But somehow the whole box would go missing, as I was working during that time. So it’s easier to remember this way, even after I stopped working. We can go back to the box, but we already lost it so we don’t want to buy it. [ID014_M-71-75_chi]
Individual responsibility to engage
When asking Patsy if anyone helps them manage her medication, she responded that,
It’s better if I do it myself, since [the helper] doesn’t know what medication I take […]. I feel that since it’s my medication, I should take responsibility for it. [ID004_F_66-70_chi]
This sentiment was echoed by several patients interviewed, and many of them did not feel like they needed help managing their medication since it should be an individual responsibility to engage with their treatment regimen.
Since the medication is meant for yourself, then you need to manage it yourself as well. [ID009_M_76-80_chi]
Discussion
This qualitative study explored the different factors influencing medication adherence in the primary and secondary prevention of ASCVD in Singapore. To better contextualize our findings it is necessary to consider larger health system factors relevant to Singapore, primarily the ubiquity of affordable and accessible health care. Singaporeans have access to largely subsidized care offered in polyclinics (government subsidized general practice clinics), private GPs, and tertiary care facilities for primary care and chronic condition management. Further, within the primary care setting, doctors regularly prescribe a few months’ worth of medications thus enabling ease of access to medications.
Singapore has a “no free lunch” philosophy to health care financing, where subsidies and various schemes for the management of chronic conditions are widely available but Singaporeans are expected to co-pay part of the cost to ensure “shared responsibility”.36,37 A key feature of health care financing in Singapore is the use of an individual medical savings scheme administered by the state, known as Medisave, in chronic disease financing. Medisave helps individuals put aside part of their income into Medisave accounts to meet future health expenses they might have, as a way of helping Singaporeans to be individually responsible for financing their health care.37,38 In addition to Medisave, many patients interviewed cited having the PG, CHAS, and Comcare card. The PG card grants subsidies to public health care services and medication to seniors aged 65 and above in 2014. The CHAS card allows for Singaporeans in low- to middle-income households to receive subsidies for medical care in participating primary care facilities. Comcare is a social assistance scheme directed at low income Singaporeans and their families. These financing structures ensure that the majority of Singaporeans have access to relatively affordable medication, particularly for chronic diseases, such as CVD, which carry a heavy economic burden.
Participants reported condition and therapy related factors impacting their adherence. Some patients perceived ASCVD and their risk factors to be of lower priority relative to their other illnesses, which had an impact on their perceived need to adhere to the medication regimen. This is consistent with previous evidence demonstrating that a patient’s perception of a disease’s severity could have implications on their medication adherence.39 It was also found that some participants chose not to adhere to their medication due to the complexity and possible side effects of their medication regimen. Patients who were non-adherent to complex regimens tended to experience polypharmacy, which for several patients led to non-adherence. This runs parallel to previous work done in the literature and has been extensively shown to impact adherence in several contexts.12,18–21,40–47
From the perspective of access, and considering the tenets of accessibility, many patients described the acceptability of a medication regimen to be highly contingent on the patient–provider relationship as well as their perception of different health care facilities. Some patients interviewed believed that medication obtained from health care establishments in the private sector are “better”, as compared to public health care facilities. For some patients this impacted their acceptability of, and possibly their adherence to, a medication regimen. For many patients their adherence to medication was largely contingent on their trusting relationship with their health care professional. However, for some patients this trusting relationship with providers and their medication regimen was unquestionably accepted. This hinted at a possible underlying power asymmetry which underlay the trust relationship between patient and physician, and caused some patients to be non-adherent without telling their provider about it, feeling the need to hide their non-adherence. Similar work done elsewhere also demonstrated that the rapport patients have with their health care provider, has an impact on their adherence.31,43,48
Another tenet of accessibility expressed was affordability, and this could be discussed in tandem with a patient’s ability to pay. Most patients shared that medication was generally made affordable due to a number of subsidies and schemes, which decreased the amount they needed to co-pay for medication. Some patients continued to struggle to pool finances among themselves and their families to pay for medication in spite of financing structures made available within the health system. The ability to pay for care has been shown to have a direct impact on patients’ ability to manage their chronic conditions, Wee and Koh (2012) have shown that awareness, treatment, and control of CVD risk factors, such as hypertension, were poorer in Singaporean patients with low socioeconomic status.49 Furthermore, some patients also felt that their ability to seek medication they want was impacted by their ability to pay for it. Evidence in the literature has clearly shown that costly health system options, coupled with insufficient financial resources, could negatively affect a patient’s ability to seek medication.14,31,40–42,50 A patient’s ability to seek the medication they want is integral in order for the patient to adhere to medication. Other studies have also reported on non-adherence attributed to fragmented health care provision, and the corresponding need for accessible, continual, and coordinated health care services to facilitate adherence.15,22,51,52 Hence, there is a need for more innovative funding structures for patients who lack the ability to pay for health care services and medication.
For many patients their ability to perceive the need to be adherent to a medication regime, was founded on their belief of diagnosis, treatment, and adherence. Several patients did not believe that they had the risk factors of ASCVD, such as hypertension. These patients were convinced that their diagnosis of these risk factors were in fact due to the conditions in which they were tested (ie, stresses of traveling to health care institutions, or hot weather, causing high blood pressure readings) rather than actually having the condition. Many patients had the ability to perceive that it is important to adhere to a medication regimen due to either the believed efficacy of medication or the fear of potential complications resulting from unmanaged ASCVD risk factors. These findings mirror results from other studies that evaluated medication adherence among patients with CVDs.43–47 We also observed a few participants displaying “self-monitor-and-review” and “risk-benefit evaluation” behavior, similar to qualitative findings from a systematic review, in which participants took medication only when symptoms ensued.45 These behaviors illustrate a dynamic interplay of beliefs and perceptions in patients’ thought processes that can be framed under behavioral models such as the Health-Belief Model.53 In making decisions regarding adherence, “self-monitor-and-review” constitutes an interplay of perceptions regarding disease severity and therapy benefits, while “risk-benefit evaluation” goes further in accounting for perceived therapy risk (or barriers).53
While some patients, at times, forgot to take their medication, many were able to engage with their medication regimen concurring with other studies that associated forgetfulness with non-adherence.51,54,55 Most patients either used pillboxes, or developed their own everyday habits to remind them to take medication and ensure that they were able to be adherent to the medication regimen. Patients demonstrated that this willingness to engage with their medication regimen stems from the importance they place on medication adherence being an individual responsibility. Similarly, self-efficacy has been identified as a key adherence facilitator in prior studies.40,43 This willingness to engage independently, opens the door for health care providers to develop innovative approaches, such as mHealth, to help ASCVD patients manage their chronic conditions. However, these interventions will need to consider larger health system access factors pointed out earlier.
Recommendations
Based on the synthesized framework proposed earlier, our findings recommend that future interventions, such as those using mHealth, which aim to encourage medication adherence among patients who have ASCVD and its risk factors need to consider four key factors; patient perceptions; patient-centeredness; medication affordability; and the patient–provider relationship.
Patient perceptions
Interventions have to tackle patient perceptions of health systems, diagnosis, medication, adherence, and possible complications of ASCVD. Our findings point to how these perceptions impacted a patient’s ability to perceive the need to be adherent to their medication and the acceptability of medication regimens. Adherent behavior arises from a composite of perceptions; therefore strategies, including mHealth, aiming to improve adherence via changing perceptions are essential, and should be guided by behavioral models that approach the topic from multiple perspectives.53
Patient-centeredness
Our findings show that patients do engage with their medication regimen and believe that there is an individual responsibility to do so. Although self-management might risk impacting a patient’s adherence to medication therapy, our findings show that many patients adapted their everyday activities to accommodate and ensure medication adherence and took clear ownership of taking medication. This advocates a push for patient-centered care interventions which facilitate adherence through building self-efficacy and stronger support networks via patient empowerment and engagement.56,57 Elsewhere, patient-centeredness has demonstrated potential in promoting therapy appropriateness for chronic disease management, and consequently, adherence.58–60 This push for patient-centered care is supported by our findings that medication regimen complexity and side effects negatively impact a patient’s ability and willingness to be adherent, pointing to the importance of personalized care, a key component to patient-centered care. Hence, future interventions targeted at medication adherence have to be patient-centered, understanding patient concerns with regard to their medication and conditions.61
Medication affordability
Future interventions should look at decreasing patient co-payments as much as possible. While Singapore’s health care financing structures allow for patients to affordably have access to medication, our findings suggest that some patients still have difficulty pulling resources together to pay for medication. Furthermore, the evidence of the decrease of patient co-payments in order to encourage adherence has been widely reported elsewhere.62–65
Patient–provider relationship
A key theme in this study is the relationship between a patient and their provider. Our findings show that doctors are trusted and their words hold tremendous value to the patients. Many patients shared that the foundation of their adherence is their trust in the doctor, and the doctors’ words are able to make a medication regimen acceptable in the eyes of the patient. Hence, future interventions should seek to cultivate a trusting relationship between the patient and physician if adherence is to be improved, as reported elsewhere.48 We also found that non-physician health care professionals such as nurses and pharmacists played some role in a patient’s medication adherence. Although their role was less pronounced, they have important roles in encouraging medication adherence among patients.66,67 Future interventions should also look at promoting good patient–provider relationships with non-physician health care professionals.
Strengths and limitations
A key strength of this study is the application of a synthesized framework which expands our view of medication access, and broadens existing understandings of adherence factors. Applying qualitative methodology to explore participants’ perspectives through in-depth interviews allowed us to access participants’ perceptions, beliefs, and experiences, which is usually not accessible through quantitative studies.68 Moreover, this is one of the few qualitative studies, to our knowledge, that explored adherence among ASCVD patients in Singapore. Our study also included participants from different ethnic backgrounds which added to the diversity of experiences captured.
A limitation of this study is the age of our patients who were all above 60 years, as such this study was not able to capture the views and experiences of younger, middle-aged patients taking ASCVD medication. Furthermore, this study excluded patients who had physical, cognitive or mental deficiencies which prevented them from participating in the interviews. Also, patients interviewed largely claimed to be adherent to their medication, and this could be inaccurate due to it being a self-reported outcome which is prone to desirability bias. This bias might have compelled participants to report more favorably about their own adherence. Finally, further research could focus on understanding the bearing of other socioeconomic factors on medication adherence, such as education level or ethnicity.
Conclusion
This study has identified several factors influencing medication adherence toward ASCVD prevention in Singapore. We proposed a framework which expanded on existing understandings of medication access, to broaden our insight into the factors of medication adherence. We used this framework to explore the different therapy, condition, and access related factors which might impact medication adherence for patients with ASCVD or their risk factors in Singapore. We believe that this framework would be a useful tool for exploring the social and access factors which underpin interventions, such as those used in mHealth, conceived to promote adherence. On the basis of using this framework to conduct an analysis in this study, we recommend that future interventions consider patient perceptions, advocate patient-centered care, guarantee that medication is affordable for the patient, and nurture good patient–provider relationships.
As populations around the world age at an alarming rate, the need to understand what works in managing chronic disease has become increasingly important. Moving forward, future research needs to consider the relevance of existing interventions for the “next generation” of patients with ASCVD, and develop innovative interventions (developed with patients at the center) which are effective for those patients. This is particularly important for wealthier nations with good access to health care like Singapore, where the effectiveness of pharmacotherapy might be heavily contingent on improving adherence levels.14
Acknowledgment
This research was supported by Humanities and Social Sciences Seed Fund, R-608-000-137-646, and the National University Health System (NUHS) Singapore Population Health Improvement Centre (SPHERiC).
Disclosure
The authors report no conflicts of interest in this work.
References
Mendis S, Puska P, Norrving B. WHO. Global Atlas on Cardiovascular Disease Prevention and Control. Geneva: World Health Organization; 2011. | ||
Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. | ||
World Heart Federation. CVD Advocacy Toolkit: The Road to 2018. Geneva: World Heart Federation; 2016. | ||
Ohira T, Iso H. Cardiovascular disease epidemiology in Asia: an overview. Circ J. 2013;77(7):1646–1652. | ||
moh.gov.sg. Principal causes of death; 2017. Ministry of Health Singapore. Available from: https://www.moh.gov.sg/resources-statistics/singapore-health-facts/principal-causes-of-death. Accessed 12 April 2018. | ||
Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization; 2003. Available from: http://www.who.int/chp/knowledge/publications/adherence_report/en/. Accessed November 9, 2018. | ||
Perel P, Avezum A, Huffman M, et al. Reducing premature cardiovascular morbidity and mortality in people with atherosclerotic vascular disease: The World Heart Federation Roadmap for Secondary Prevention of Cardiovascular Disease. Glob Heart. 2015;10(2):99–110. | ||
Daniels SR. Prevention of atherosclerotic cardiovascular disease: what is the best approach and how early should we start? J Am Coll Cardiol. 2014;63(25 Pt A):2786–2788. | ||
Stewart J, Manmathan G, Wilkinson P. Primary prevention of cardiovascular disease: A review of contemporary guidance and literature. JRSM Cardiovasc Dis. 2017;6:2048004016687211. | ||
Wang W, Chia GS, Tan IF, et al. Independent predictors of medication adherence among Singaporean patients following an ischaemic stroke or transient ischaemic attack. J Clin Nurs. 2017;26(23–24):5016–5024. | ||
Lee GK, Wang HH, Liu KQ, Cheung Y, Morisky DE, Wong MC. Determinants of medication adherence to antihypertensive medications among a Chinese population using Morisky Medication Adherence Scale. PLoS One. 2013;8(4):e62775. | ||
Baroletti S, Dell’Orfano H. Medication adherence in cardiovascular disease. Circulation. 2010;121(12):1455–1458. | ||
Mahler C, Hermann K, Horne R, et al. Assessing reported adherence to pharmacological treatment recommendations. Translation and evaluation of the Medication Adherence Report Scale (MARS) in Germany. J Eval Clin Pract. 2010;16(3):574–579. | ||
Chowdhury R, Khan H, Heydon E, et al. Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical consequences. Eur Heart J. 2013;34(38):2940–2948. | ||
Kronish IM, Ye S. Adherence to cardiovascular medications: lessons learned and future directions. Prog Cardiovasc Dis. 2013;55(6):590–600. | ||
Bosworth HB, Granger BB, Mendys P, et al. Medication adherence: a call for action. Am Heart J. 2011;162(3):412–424. | ||
Kumbhani DJ, Steg PG, Cannon CP, et al; REduction of Atherothrombosis for Continued Health Registry Investigators. Adherence to secondary prevention medications and four-year outcomes in outpatients with atherosclerosis. Am J Med. 2013;126(8):693–700.e1. | ||
Psaty BM, Koepsell TO, Wagner EH, LoGerfo JP, Inui TS. The relative risk of incident coronary heart disease associated with recently stopping the use of beta-blockers. JAMA. 1990;263(12):1653–1657. | ||
Kulkarni SP, Alexander KP, Lytle B, Heiss G, Peterson ED. Long-term adherence with cardiovascular drug regimens. Am Heart J. 2006;151(1):185–191. | ||
Cordero A, Rodriguez Padial L, Batalla A, et al; CAPS study investigators. Optimal pharmacological treatment and adherence to medication in secondary prevention of cardiovascular events in Spain: Results from the CAPS study. Cardiovasc Ther. 2017;35(2):e12240. | ||
Garner JB. Problems of nonadherence in cardiology and proposals to improve outcomes. Am J Cardiol. 2010;105(10):1495–1501. | ||
Packard KA, Hilleman DE. Adherence to therapies for secondary prevention of cardiovascular disease: a focus on aspirin. Cardiovasc Ther. 2016;34(6):415–422. | ||
Kamal AK, Shaikh Q, Pasha O, et al. A randomized controlled behavioral intervention trial to improve medication adherence in adult stroke patients with prescription tailored Short Messaging Service (SMS)-SMS4Stroke study. BMC Neurol. 2015;15:212. | ||
Leon N, Surender R, Bobrow K, Muller J, Farmer A. Improving treatment adherence for blood pressure lowering via mobile phone SMS-messages in South Africa: a qualitative evaluation of the SMS-text Adherence SuppoRt (StAR) trial. BMC Fam Pract. 2015;16:80. | ||
Park LG, Beatty A, Stafford Z, Whooley MA. Mobile Phone Interventions for the Secondary Prevention of Cardiovascular Disease. Prog Cardiovasc Dis. 2016;58(6):639–650. | ||
Adler AJ, Martin N, Mariani J, et al. Mobile phone text messaging to improve medication adherence in secondary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2017;4:CD011851. | ||
data.gov.sg. Authority IMD. Mobile Penetration Rate. 30 March 2017. Available from: https://data.gov.sg/dataset/mobile-penetration-rate. Accessed October 11, 2018. | ||
Union IT. Measuring the Information Society Report 2017. Geneva: International Telecommunication Union; 2017. Available from: https://www.itu.int/en/ITU-D/Statistics/Pages/publications/mis2017.aspx. Accessed November 3, 2018. | ||
Levesque JF, Harris MF, Russell G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013;12:18. | ||
Sayles JN, Wong MD, Kinsler JJ, Martins D, Cunningham WE. The association of stigma with self-reported access to medical care and antiretroviral therapy adherence in persons living with HIV/AIDS. J Gen Intern Med. 2009;24(10):1101–1108. | ||
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. | ||
Sleath BL, Krishnadas R, Cho M, et al. Patient-reported barriers to glaucoma medication access, use, and adherence in southern India. Indian J Ophthalmol. 2009;57(1):63–68. | ||
Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice. Hoboken, NJ: John Wiley & Sons; 2008. | ||
Strauss AL. Qualitative Analysis for Social Scientists. Cambridge: Cambridge University Press; 1987. | ||
Benetos A, Rossignol P, Cherubini A, et al. Polypharmacy in the Aging Patient: Management of Hypertension in Octogenarians. JAMA. 2015;314(2):170–180. | ||
Lim MK. Shifting the burden of health care finance: a case study of public-private partnership in Singapore. Health Policy. 2004;69(1):83–92. | ||
Khoo HS, Lim YW, Vrijhoef HJ. Primary healthcare system and practice characteristics in Singapore. Asia Pac Fam Med. 2014;13(1):8. | ||
Singapore MoH. Medisave; 2017. Available from: https://www.moh.gov.sg/cost-financing/healthcare-schemes-subsidies/medisave. Accessed 12 April 2018. | ||
DiMatteo MR, Haskard KB, Williams SL. Health beliefs, disease severity, and patient adherence: a meta-analysis. Med Care. 2007;45(6):521–528. | ||
Odusola AO, Hendriks M, Schultsz C, et al. Perceptions of inhibitors and facilitators for adhering to hypertension treatment among insured patients in rural Nigeria: a qualitative study. BMC Health Serv Res. 2014;14:624. | ||
Garavalia L, Garavalia B, Spertus JA, Decker C. Exploring patients’ reasons for discontinuance of heart medications. J Cardiovasc Nurs. 2009;24(5):371–379. | ||
van der Laan DM, Elders PJM, Boons CCLM, Beckeringh JJ, Nijpels G, Hugtenburg JG. Factors associated with antihypertensive medication non-adherence: a systematic review. J Hum Hypertens. 2017;31(11):687–694. | ||
Holt EW, Rung AL, Leon KA, Firestein C, Krousel-Wood MA. Medication adherence in older adults: a qualitative study. Educ Gerontol. 2014;40(3):198–211. | ||
Harrison TN, Derose SF, Cheetham TC, et al. Primary nonadherence to statin therapy: patients’ perceptions. Am J Manag Care. 2013;19(4):e133–e139. | ||
Marshall IJ, Wolfe CD, McKevitt C. Lay perspectives on hypertension and drug adherence: systematic review of qualitative research. BMJ. 2012;345:e3953. | ||
Jamison J, Graffy J, Mullis R, Mant J, Sutton S. Barriers to medication adherence for the secondary prevention of stroke: a qualitative interview study in primary care. Br J Gen Pract. 2016;66(649):e568–e576. | ||
Nguyen TP, Schuiling-Veninga CC, Nguyen TB, Vu TH, Wright EP, Postma MJ. Adherence to hypertension medication: Quantitative and qualitative investigations in a rural Northern Vietnamese community. PLoS One. 2017;12(2):e0171203. | ||
Legido-Quigley H, Camacho Lopez PA, Balabanova D, et al. Patients’ knowledge, attitudes, behaviour and health care experiences on the prevention, detection, management and control of hypertension in Colombia: a qualitative study. PLoS One. 2015;10(4):e0122112. | ||
Wee LE, Koh GC. Individual and neighborhood social factors of hypertension management in a low-socioeconomic status population: a community-based case-control study in Singapore. Hypertens Res. 2012;35(3):295–303. | ||
Syed ST, Gerber BS, Sharp LK. Traveling towards disease: transportation barriers to health care access. J Community Health. 2013;38(5):976–993. | ||
O’Quin KE, Semalulu T, Orom H. Elder and caregiver solutions to improve medication adherence. Health Educ Res. 2015;30(2):323–335. | ||
Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. | ||
Viswanath K, Orleans CT, Glanz K, Rimer BK. Health Behavior and Health Education: Theory, Research, and Practice. San Francisco, CA: Jossey-Bass; 2008. | ||
Khatib R, Schwalm JD, Yusuf S, et al. Patient and healthcare provider barriers to hypertension awareness, treatment and follow up: a systematic review and meta-analysis of qualitative and quantitative studies. PLoS One. 2014;9(1):e84238. | ||
Roy NT, Sajith M, Bansode MP. Assessment of Factors Associated with Low Adherence to Pharmacotherapy in Elderly Patients. J Young Pharmacists. 2017;9(2):272–276. | ||
World Health Organization. Framework on Integrated, People-centred Health Services. Geneva: WHO; 2015. Available from: http://www.who.int/servicedeliverysafety/areas/people-centred-care/conceptual-framework.pdf. Accessed November 3, 2018. | ||
Schwamm LH, Chumbler N, Brown E, et al; American Heart Association Advocacy Coordinating Committee. Recommendations for the Implementation of Telehealth in Cardiovascular and Stroke Care: A Policy Statement From the American Heart Association. Circulation. 2017;135(7):e24–e44. | ||
Goldfarb M. A Cardiology Fellow’s Guide to Patient-Centered Care. J Am Coll Cardiol. 2017;69(23):2871–2874. | ||
Roumie CL, Greevy R, Wallston KA, et al. Patient centered primary care is associated with patient hypertension medication adherence. J Behav Med. 2011;34(4):244–253. | ||
Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70(4):351–379. | ||
Clifford S, Barber N, Elliott R, Hartley E, Horne R. Patient-centred advice is effective in improving adherence to medicines. Pharm World Sci. 2006;28(3):165–170. | ||
Gibson TB, Mark TL, Axelsen K, Baser O, Rublee DA, McGuigan KA. Impact of statin copayments on adherence and medical care utilization and expenditures. Am J Manag Care. 2006;12:SP11–SP19. | ||
Maciejewski ML, Bryson CL, Perkins M, et al. Increasing copayments and adherence to diabetes, hypertension, and hyperlipidemic medications. Am J Manag Care. 2010;16(1):e20–e34. | ||
Cole JA, Norman H, Weatherby LB, Walker AM. Drug copayment and adherence in chronic heart failure: effect on cost and outcomes. Pharmacotherapy. 2006;26(8):1157–1164. | ||
Maimaris W, Paty J, Perel P, et al. The influence of health systems on hypertension awareness, treatment, and control: a systematic literature review. PLoS Med. 2013;10(7):e1001490. | ||
Lee JK, Grace KA, Taylor AJ. Effect of a pharmacy care program on medication adherence and persistence, blood pressure, and low-density lipoprotein cholesterol: a randomized controlled trial. JAMA. 2006;296(21):2563–2571. | ||
Bakken S, Holzemer WL, Brown MA, et al. Relationships between perception of engagement with health care provider and demographic characteristics, health status, and adherence to therapeutic regimen in persons with HIV/AIDS. AIDS Patient Care STDS. 2000;14(4):189–197. | ||
Green J, Thorogood N. Qualitative Methods for Health Research. Thousand Oaks, CA: SAGE Publications; 2013. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.